






-
心肌桥(myocardial bridge,MB)是指覆盖在心外膜冠状动脉上的心肌纤维束,被心肌纤维束覆盖的冠状动脉称为壁冠状动脉(muralcoronary artery,MCA),而这一复合体统称为MB-MCA。MB-MCA被认为是一种良性的冠状动脉先天性解剖变异,可导致部分患者心肌缺血,甚至猝死[1],因此,早期准确地诊断及评价MB-MCA,有助于预防严重并发症。多层螺旋CT的空间、时间分辨力高,具有无创性,评价冠状动脉病变准确、快速,且能直观显示MB-MCA形态学特征,包括MCA的部位、心肌覆盖范围、血管狭窄程度以及MB的厚度,并同时可发现桥近、远段及MCA本身有无粥样硬化病变,因此,其在诊断MB-MCA相关冠状动脉病变上具有重要的临床应用价值。本研究拟利用640层螺旋CT冠状动脉成像对MB-MCA的形态学及相关功能改变进行量化分析,并探讨MB-MCA与冠状动脉粥样硬化的相关性。
HTML
-
收集2014年8月至2015年12月我院临床疑似冠心病的186例患者作为研究对象,其中男性96例、女性90例,年龄42~84岁,平均年龄(63±12)岁;临床表现为心前区不适或胸痛等症状。所有患者均成功行640层螺旋CT冠状动脉成像检查。扫描检查时心率为54~87次/min,平均心率为69次/min,排除房颤、图像质量不佳者。所有患者接受检查前均告知检查内容并签署了知情同意书。
-
采用日本东芝640层Aquilionone CT进行检查。检查前测量血压及心率,对静息状态下心率高于75次/min且无酒石酸美托洛尔禁忌症的患者,检查前1 h给予酒石酸美托洛尔25~50 mg,最大剂量不超过100 mg。患者取仰卧位,扫描前进行严格的屏气训练,对不能良好配合的患者使用腹压带。用美国Medra公司的双筒高压注射器经肘静脉注入对比剂碘海醇(GE,美国)(350 mgI/mL)40~60 mL,流速为4.0~5.5 mL/s,随后以相同流速注射生理盐水30 mL。采用Sure Start软件智能触发扫描,触发点定于扫描野中央层面胸主动脉,以个体化手动触发,注入药物14 s后开始扫描。管电压为120 kV,管电流为60~370 mA。机架扫描一周为0.35 s,扫描范围12~16 cm。所有扫描均采用前瞻性心电门控。
-
所有患者的原始影像数据资料均传至Vitrea FXVES 6.0后处理工作站,选择最佳的心动周期相位(多为45%或75%),运用心脏高级后处理软件包对冠状动脉各主要分支血管进行评估分析。后处理重建方法包括:容积再现(volume rendering,VR)、最大密度投影(maximum intensity projection,MIP)、多平面重组(multiplanar reformation,MPR)、曲面重建(curve planar reformation,CPR)等。由2位放射科医师采用独立盲法观察横断面、VR、MIP、MPR、CPR等图像,对每例血管进行评价和分析;至少两个平面显示冠状动脉走行于心肌内,可以肯定MB的存在;其次采用多时相重建来判定心脏收缩末期和舒张末期。根据Ferreira等[2]的研究,按照MB的心肌覆盖的厚度将MCA分为浅表型和深厚型。浅表型指MCA部分或全部被心肌包绕,厚度 < 2 mm;深厚型指MCA位于较深的心肌中,厚度≥2 mm。诊断MB-MCA的病例达成一致后,分别记录MB-MCA的所在部位、数目、MB的厚度、MCA的长度、管腔的狭窄程度以及MB-MCA近端、远端和MCA是否合并冠状动脉粥样硬化斑块;同时选择左前降支的MB-MCA,计算其收缩期到舒张期MB的厚度变化(△厚度)和直径变化(△直径)。按照Noble分级法[3]将MB-MCA收缩期狭窄分为3级:Ⅰ级,狭窄程度≤50%;Ⅱ级,50%<狭窄程度≤75%;Ⅲ级,狭窄程度>75%。采用美国心脏病学会冠状动脉的15段分段标准对冠脉MB-MCA分布进行评价。
-
采用SPSS 17.0软件对数据进行统计学分析,计量资料用均数±标准差表示;数据进行分析前先进行正态分布检验,采用合理统计方法(t检验或非参数检验);MB的功能变化指标比较采用配对t检验,MB粥样斑块的分布特征比较采用独立样本t检验,P<0.05表示差异有统计学意义。
1.1. 一般资料
1.2. 多层螺旋CT冠状动脉扫描
1.3. 图像后处理及数据分析
1.4. 统计学方法
-
186例患者中共发现56例(70段)存在MB-MCA,约占30.1%,其中45例(80.4%)为单一MCA,8例(14.3%)为2段受累,3例(5.3%)为3段受累。70段MB-MCA的位置如表 1所示。
部位 数量 平均厚度(x±s)/mm 平均长度(x±s)/mm 浅表型 深厚型 LAD2 48(68.6%) 2.68±0.68 21.42±6.42 31 17 LAD1-3 9(12.9%) 2.33±0.64 19.86±5.98 5 4 LCX 3(4.3%) 2.35±0.48 20.04±6.26 2 1 D1-2 5(7.1%) 2.14±0.38 17.23±5.23 3 2 OM 3(4.3%) 2.46±0.58 16.48±5.32 2 1 RCA 2(2.8%) 2.13±0.42 16.58±4.96 1 1 合计 70(100%) 2.32±0.51 18.48±5.24 44 26 注:表中,LAD2:左前降支2段;LAD1-3:左前降支近、中、远段;LCX:左回旋支;D1-2:第l、2对角支;OM:钝缘支;CA:右冠状动脉。 Table 1. Distribution and measured results of 70 segments of myocardial bridge-mural coronary artery in 56 patients
CPR图像示MCA走行较平直,在心肌内行走一段距离后又浅露于心肌表面,即“上下台阶”征(图 1中A)。70段MB-MCA平均MB厚度为(2.32±0.51)mm,MCA平均长度为(18.48±5.24)mm。根据MB的厚度,70段MB-MCA中浅表型44段(占62.9%),深厚型26段(占37.1%)(图 1中B、C);MB-MCA具体分布和测量结果见表 1。
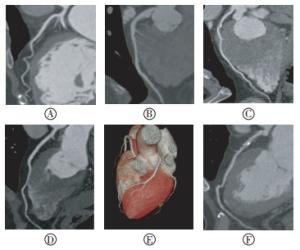
Figure 1. Multi-detector spiral CT imagings of different coronary disease patients
-
48段位于LAD2的MB-MCA剔除5段横断面血管边缘模糊的病例,最终对43段进行定量分析,详见表 2。MB的△厚度范围为1.02~1.86 mm,平均为(1.64±0.56)mm,△直径范围为0.80~2.02 mm,平均为(1.21±0.36)mm。△厚度和△直径在心脏收缩期和舒张期差异具有统计学意义(t=2.84、3.38,P均<0.05),且两者变化呈反比趋势。43段MB-MCA中,10段(23.3%)为Ⅰ级狭窄,28段(65.1%)为Ⅱ级狭窄,5段(11.6%)为Ⅲ级狭窄(图 1中D、E)。
量化指标 Dd/mm Ds/mm 差值/mm 变化率/% MB厚度 2.56±0.52 4.24±0.92 1.64±0.56 68.6 MCA直径 2.36±0.46 1.46±0.24 1.21±0.36 57.8 注:表中,MB:心肌桥;MCA:壁冠状动脉;Dd:舒张末期内径,Ds:收缩末期内径。 Table 2. Quantitative analysis of myocardial bridge-mural coronary artery of left anterior descending(x±s)
-
70段MB-MCA中共发现48段存在粥样斑块,占68.6%;其粥样斑块发生在MB-MCA近侧者42段(87.5%),远侧者6段(12.5%),两者之间的差异具有统计学意义(t=3.12,P<0.05),MCA本身未发现存在粥样斑块(图 1中B、C、F)。
2.1. 心肌桥分布及形态特征
2.2. 左前降支2段(left anterior descending,LAD2)心肌桥定量分析
2.3. MB-MCA粥样斑块分布特征
-
MB-MCA作为一种良性的解剖变异,其发病机制尚未完全明确,结构学基础表现为部分冠状动脉血管节段被心肌所覆盖。MB患者临床症状不具有特异性,许多患者长期无明显症状,但也有不少患者有心肌缺血表现。MB在人群中的发生率报道不一:尸检发现率为15%~85%[4],平均约35%;冠状动脉造影(coronary angiography,CAG)检查MB-MCA的发现率为0.6%~25%[5],多数报道小于2%,而以往多层螺旋CT研究MB-MCA的检出率为18.56%~64.2%[6-8],本研究检出率为30.1%,明显高于CAG检出率,与以往研究相符。多层螺旋CT可以直接显示位于心肌内的MCA,能准确显示心肌桥;而多层螺旋CT检出率之间的差异主要是由CT扫描仪性能(空间和时间分辨率)上的差异所致,研究发现128层或以上的CT、双源CT具有更高的检出率[6-8]。
MB-MCA好发于左前降支中段,深度多在10 mm以下,长度10~40 mm,以往研究报道其发生率为59.6%~86.3%[7-8],本研究发现LAD2的MB-MCA发生率为68.6%,其MD平均厚度为(2.68±0.68)mm,MCA平均长度为(21.42±6.42)mm,与以往研究相符[7],其解剖学基础被认为可能与左前降支行程较长、走行相对复杂以及前壁心肌组织较为肥厚等因素有关;同时我们研究发现MB-MCA多为单桥(80.4%),与马恩森等[7]报道高度吻合。本研究70段MB-MCA中,浅表型44段(62.9%),发生率明显高于深厚型26段(37.1%),与以往报道相符[8-9]。本研究未对MB厚度的临床意义进行探讨,而古今等[9]发现深厚型MB收缩期时MCA的缩窄率明显高于浅表型,两者差异具有统计学意义,提示深厚型MB-MCA更易导致心肌缺血。
部分MB-MCA患者可表现为心肌缺血症状,笔者认为其可能机制主要包括:(1)心脏收缩期心肌收缩导致MCA狭窄,心肌血流灌注减少,同时舒张期心肌舒张时间相对不足影响早、中期血流,最终造成冠状动脉的血流储备降低,加剧了心肌缺血。本研究对MB-MCA在心脏收缩期和舒张期进行定量分析,发现收缩期MB厚度平均增加了(1.64±0.56)mm,而MCA直径降低了(1.21±0.36)mm,管腔平均缩窄了57.8%;根据Noble分级法评估MCA的狭窄程度,本研究发现65.1%的MCA存在Ⅱ级狭窄,提示MB-MCA患者多数存在管腔狭窄、心肌缺血,因此临床上必须加以重视。另外有学者发现MB-MCA的长度在心脏收缩和舒张时也会发生变化[7, 10-11],但是否具有临床意义仍需要进一步研究。(2)MB对MCA的机械压迫作用,促进了动脉粥样硬化的发生和发展。MB-MCA是否与冠状动脉粥样硬化具有相关性,仍有争议。国内学者张闽光等[6]发现,各支冠状动脉检出动脉粥样硬化钙化斑块例数及其钙化积分、软斑块例数及其狭窄程度在检出与未检出MB-MCA者之间的差异均无统计学意义,而检出MB-MCA者动脉粥样硬化斑块主要累及近侧,占90.8%,显著多于MCA本身及其远侧;本研究显示粥样斑块发生在MB-MCA近侧者约87.5%,明显高于远侧者12.5%,MCA本身未发现存在粥样斑块,与既往研究结果相符[6, 12]。这与MB-MCA超微结构和流体力学的特征有关[13],研究发现MCA血流均明显高于其近段和远段,冠状动脉内压力增高,血流与MCA内膜之间的剪切力增大,使内皮细胞促进血管舒张因子、生长抑制因子、纤维蛋白溶解物和抗氧化剂的表达,抑制血管收缩因子、生长因子、炎性介质和黏附因子的表达,使内皮细胞不易损伤,也不利于细胞增生、脂质摄取和细胞黏附,具有抗动脉粥样硬化作用[13]。而其近段内皮细胞由于切变力低,容易损伤,成为动脉粥样硬化的血流动力学基础。
综上所述,多层螺旋CT能够无创性地直观显示MB的存在以及其长度和厚度,同时能评价MB-MCA舒张期和收缩期的形态学变化及MCA近侧血管发生粥样硬化的情况,从而为临床治疗计划的制定提供依据,可以部分取代CAG,具有重要的临床应用价值。
 DownLoad:
DownLoad: