






-
心脏淀粉样变(cardiac amyloidosis,CA)是由于不同的前体蛋白异常折叠沉积于心肌细胞间隙中导致的疾病[1-2],伴有心脏功能受损及心脏电传导异常。临床常见的CA分型包括轻链型CA(light chain CA,AL-CA)和转甲状腺素蛋白相关CA(transthyretin-related CA,ATTR-CA),由于AL-CA和ATTR-CA患者的血清生物标志物、治疗方法和预后存在很大差异,因此CA的分型诊断尤为重要。99Tcm-焦磷酸盐(pyrophosphate,PYP)显像可特异性诊断ATTR-CA,随着其临床应用的进展,临床医师对不同采集时间[99Tcm-PYP 注射后1 h(以下简称早期显像)和99Tcm-PYP注射后3 h(以下简称延迟显像)]及不同采集方式(平面显像和断层显像)图像的解读也有了更深入的认识。由于早期平面显像的假阳性率较高,延迟显像心脏血池的清除更好,因此越来越多的研究者建议进行早期断层显像、延迟断层显像和延迟平面显像,以提高诊断的准确率[3-7],但尚需大样本量的研究结果证实。本研究拟比较99Tcm-PYP双时相平面显像和断层显像的各种阳性诊断标准,并通过比较CA不同临床分型(AL-CA和ATTR-CA)的图像特征,评价不同采集时间、采集方式及评分模式在99Tcm-PYP双时相平面显像和断层显像诊断ATTR-CA中的效能。
-
回顾性研究2020年3月至2023年1月于中国医学科学院阜外医院临床疑诊CA的患者157例,其中男性108例、女性49例,年龄(58.9±14.8)岁,范围10~88岁。纳入标准:(1)患者已进行99Tcm-PYP 双时相平面显像和断层显像;(2)经组织病理学检查、免疫组织化学检查或基因检测结果确诊为CA或排除CA。排除标准:(1)经组织病理学检查确诊CA但未行免疫组织化学检查;(2)仅完成99Tcm-PYP早期显像,未行99Tcm-PYP延迟显像。患者的临床资料通过病历系统查询获得,72例(72/157,46%)患者进行了心内膜心肌活检,43例进行了其他组织活检(43/157,27%),93例(93/157,59%)进行了血或尿免疫固定电泳(immunofixation electroforesis,IFE)或游离轻链(free light chain,FLC)检测,157例进行了超声心动图检查(157/157,100%)。本研究经中国医学科学院阜外医院伦理委员会批准(批准号:2023-2187)。因本研究为回顾性研究,豁免签署患者知情同意书。本研究符合《赫尔辛基宣言》的原则。
-
使用美国GE公司Optima NM/CT 640 型SPECT/CT显像仪。99Tcm-PYP由中国医学科学院阜外医院核医学科制备,放射化学纯度≥90%。参照美国核心脏病学会推荐的显像流程[8]及中华医学会核医学分会心脏学组和国家核医学专业质控中心推荐的技术操作规范[9],对患者静脉注射740 MBq 99Tcm-PYP,分别于注射后1、3 h行平面显像及断层显像。平面显像:患者取仰卧位,采集胸部前位及左侧位静态平面图像,矩阵256×256,能窗140 keV(±10%),放大倍数1.46,静态采集750×103计数; 断层显像:矩阵256×256,准直器垂直模式180°采集,3°/帧,40 s/帧,能窗140 keV(±10%),放大倍数1.0。断层显像采集结束后,患者保持体位不动,进行同机低剂量心脏CT扫描(管电压120 kV,管电流10 mA),用于断层显像的衰减校正和图像融合。
-
(1)Perugini法。由2位有5年以上工作经验的核医学科医师比较平面显像中心脏、肋骨的摄取水平并评分,意见不一致时经协商达成一致。心脏无摄取而肋骨摄取正常为0分;心脏摄取低于肋骨摄取为1分;心脏摄取等于或略高于肋骨摄取为2分;心脏摄取明显高于肋骨摄取伴肋骨摄取降低或无摄取为3分。0~1分定义为99Tcm-PYP显像阴性;2~3分定义为99Tcm-PYP显像阳性[9]。
(2)平面显像半定量分析法。在平面显像的心脏区域用圆形勾画ROI,并镜像至对侧肺部,计算ROI平均计数,获得心脏与对侧肺摄取比值(the uptake ratio of heart to contralateral lung,H/CL)。早期平面显像 H/CL≥1.5定义为99Tcm-PYP显像阳性;延迟平面显像H/CL≥1.3定义为99Tcm-PYP显像阳性[9]。由于早期平面显像假阳性率高,因此本研究同时探讨了将延迟平面显像H/CL≥1.5定义为99Tcm-PYP显像阳性的诊断效能。
(3)断层显像半定量评分法。由2位有5年以上工作经验的核医学科医师分别对早期断层显像和延迟断层显像的心肌放射性摄取水平进行半定量评分,意见不一致时经协商达成一致。心肌和血池内均无明显放射性摄取为0分;心脏区域内有放射性摄取但心肌和血池区分不开为1分;心肌可见弥漫性放射性摄取且血池内无明显滞留为2分。断层显像半定量评分2分定义为99Tcm-PYP显像阳性[9]。
-
99Tcm-PYP显像阳性的最终结论以断层显像半定量评分结果为准,临床最终诊断结论则参照美国核心脏病学会和中华医学会心血管病学分会心力衰竭学组推荐的CA临床诊断指南[8, 10]来诊断CA并分型(符合以下3项中1项则诊断为CA):(1)超声或MRI高度怀疑CA,血或尿IFE或FLC实验室检查结果为阳性,则诊断为AL-CA;(2)超声或MRI高度怀疑CA,血和尿IFE或FLC实验室检查结果为阴性,99Tcm-PYP显像为阳性,则诊断为ATTR-CA;(3)心内膜心肌活检结果为阳性,并经免疫组织化学检查确定为AL-CA或ATTR-CA。不符合上述任何一项者则诊断为非CA。以临床分型为分组标准,将所有患者分为AL-CA组、ATTR-CA组、非CA组,比较各组间Perugini法、平面显像半定量分析法、断层显像半定量评分法的诊断结果差异,分析99Tcm-PYP显像不同采集时相和不同采集方式的影像特征及诊断效能。
-
应用IBM SPSS 26.0软件进行统计学分析。符合正态分布的计量资料以
$\bar x \pm s $ -
由表1可知,157例疑诊CA的患者中,CA 83例(其中ATTR-CA 23例、AL-CA 60例)、非CA 74例。非CA组、AL-CA组和ATTR-CA组患者高血压、活检(心内膜心肌活检、其他组织活检)、血或尿IFE或FLC、左心室壁厚度>12 mm的差异均有统计学意义(均P<0.05);性别、年龄、左心室射血分数<50%的差异均无统计学意义(均P>0.05)。99Tcm-PYP显像阳性患者的血和尿IFE、FLC检测结果均为阴性,经心内膜心肌活检诊断为ATTR-CA(图1)。99Tcm-PYP显像阴性患者的血和尿IFE、FLC检测结果均为阴性,心内膜心肌活检为阴性,非特异性改变,临床诊断为限制型心肌病(图2)。
组别 例数 性别
(男/女)年龄(岁, $\bar x \pm s $ 

高血压(例) 活检(例) 血或尿IFE或
FLC(例)超声心动图(例) 心内膜心肌 其他组织 左心室射血
分数<50%左心室壁
厚度>12 mm非CA组 74 52/22 58.0±17.9 35 21 13 26 34 55 AL-CA组 60 39/21 59.6±11.1 15 36 24 53 31 58 ATTR-CA组 23 17/6 60.2±12.2 3 15 6 14 10 23 合计 157 108/49 58.9±14.8 53 72 43 93 75 136 检验值 − χ2=0.758 F=0.296 χ2=12.538 χ2=17.411 χ2=8.407 χ2=38.863 χ2=0.634 χ2=18.436 P值 − 0.685 0.744a 0.002 <0.001 0.015 <0.001 0.728 <0.001 注: −表示无此项数据;a表示采用Bonferroni校正,P<0.016为差异有统计学意义。CA为心脏淀粉样变;AL-CA为轻链型心脏淀粉样变;ATTR-CA为转甲状腺素蛋白相关心脏淀粉样变;IFE为免疫固定电泳;FLC为游离轻链 Table 1. Comparison of general information and partial examination results among non-cardiac amyloidosis (CA) group, light chain cardiac amyloidosis (AL-CA) group, and transthyretin-related cardiac amyloidosis (ATTR-CA) group patients
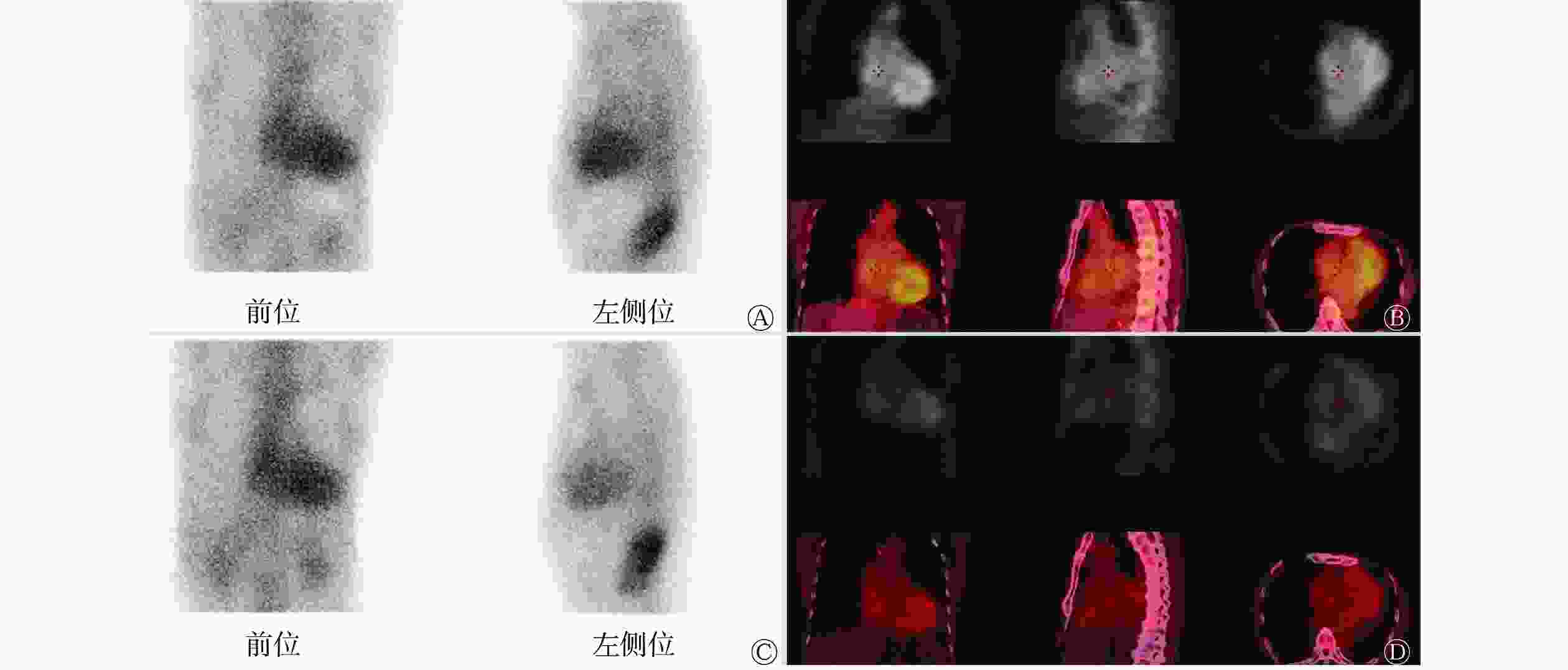
Figure 1. 99Tcm-pyrophosphate (PYP) dual-phase planar imaging and tomographic imaging of a patient (male, 82 years old) with transthyretin-related cardiac amyloidosis
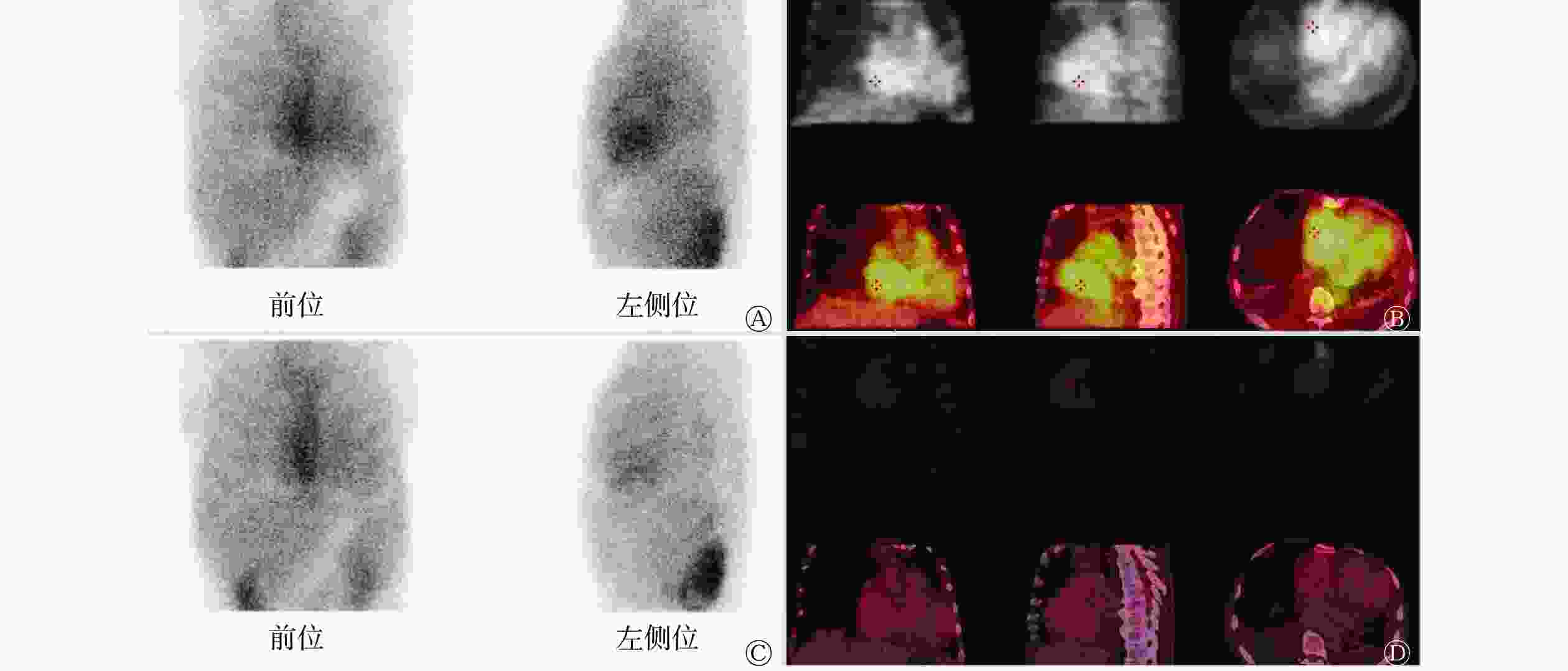
Figure 2. 99Tcm-pyrophosphate (PYP) dual-phase planar imaging and tomographic imaging of a patient (male, 51 years old) with restrictive cardiomyopathy
-
由表2可知,3组患者早期平面显像和延迟平面显像的H/CL按从大到小排序均为ATTR-CA组>AL-CA组>非CA组,且ATTR-CA组早期平面显像和延迟平面显像的H/CL均值均>1.5。依据平面显像半定量分析法,早期平面显像非CA组和AL-CA组阳性患者共32例(23.9%,32/134),ATTR-CA组阳性患者21例(91.3%,21/23);延迟平面显像以H/CL≥1.3为阳性标准时,非CA组和AL-CA组阳性患者共56例(41.8%,56/134),ATTR-CA组阳性患者22例(95.7%,22/23);延迟平面显像以H/CL≥1.5为阳性标准时,非CA组和AL-CA组阳性患者共12例(9.0%,12/134),ATTR-CA组阳性患者17例(73.9%,17/23)。依据Perugini法,早期平面显像非CA组和AL-CA组阳性患者共80例(59.7%,80/134),ATTR-CA组阳性患者23例(100%,23/23);延迟平面显像非CA组和AL-CA组阳性患者共11例(8.2%,11/134),ATTR-CA组阳性患者22例(95.7%,22/23)。依据断层显像半定量评分法,早期断层显像非CA组和AL-CA组阳性患者共1例(0.7%,1/134),ATTR-CA组阳性患者18例(78.3%,18/23);延迟断层显像非CA组和AL-CA组阳性患者共2例(1.5%,2/134),ATTR-CA组阳性患者21例(91.3%,21/23)。ATTR-CA组、非CA组、AL-CA组3组之间的早期显像和延迟显像的H/CL、Perugini法及断层显像半定量评分结果的差异均有统计学意义(均P<0.001)。
组别 早期显像 延迟显像 H/CL Perugini法(例) 断层显像半定
量评分(例)H/CL Perugini法(例) 断层显像半定
量评分 (例)$\bar x \pm s $ 

≥1.5(例) 0分 1分 2分 3分 0分 1分 2分 $\bar x \pm s $ 

≥1.3(例) ≥1.5(例) 0分 1分 2分 3分 0分 1分 2分 非CA组(n=74) 1.33±0.21 15 3 32 38 1 49 25 0 1.23±0.17 25 4 36 32 6 0 71 2 1 AL-CA组(n=60) 1.41±0.18 17 3 16 40 1 21 38 1 1.31±0.15 31 8 13 42 5 0 56 3 1 ATTR-CA组(n=23) 1.94±0.36 21 0 0 9 14 0 5 18 1.74±0.30 22 17 0 1 13 9 1 1 21 检验值 F=64.218 χ2=40.870 χ2=82.932 χ2=126.373 F=65.634 χ2=27.019 χ2=56.386 χ2=114.152 χ2=128.283 P值 <0.001a <0.001 <0.001 <0.001 <0.001a <0.001 <0.001 <0.001 <0.001 注:a表示采用Bonferroni校正,P<0.016为差异有统计学意义。CA为心脏淀粉样变;PYP为焦磷酸盐;AL-CA为轻链型心脏淀粉样变;ATTR-CA为转甲状腺素蛋白相关心脏淀粉样变;H/CL为心脏与对侧肺摄取比值 Table 2. Results of 99Tcm-pyrophosphate (PYP) dual-phase planar imaging and tomographic imaging among non-cardiac amyloidosis (CA) group, light chain cardiac amyloidosis (AL-CA) group, and transthyretin-related cardiac amyloidosis (ATTR-CA) group patients
-
由表3可知,早期显像和延迟显像的H/CL、Perugini法和断层显像半定量评分诊断ATTR-CA的效能相比,早期平面显像Perugini法诊断ATTR-CA的准确率最低,灵敏度为100%、特异度为40.3%、准确率为49.0%;延迟断层显像半定量评分诊断ATTR-CA的准确率最高,灵敏度为91.3%、特异度为98.5%、准确率为97.5%。对不同采集时相和不同采集方式的诊断方法的诊断结果分别进行两两比较,结果显示,早期断层显像半定量评分与延迟断层显像半定量评分诊断ATTR-CA具有较好的一致性(Kappa值=0.835),诊断效能的差异无统计学意义(χ2=110.883,P=0.219);延迟平面显像 Perugini法与延迟断层显像半定量评分诊断ATTR-CA具有较好的一致性(Kappa值=0.784),诊断效能的差异有统计学意义(χ2=101.258,P=0.004),后者的诊断准确率高;其余不同采集时相和不同采集方式的诊断方法之间的诊断一致性一般或较差(Kappa值为0.135~0.679)。
诊断效能 早期显像 延迟显像 H/CL≥1.5 Perugini法
(≥2分)断层显像半定量
评分(=2分)H/CL Perugini法
(≥2分)断层显像半定量
评分(=2分)≥1.3 ≥1.5 灵敏度 91.3(21/23) 100.0(23/23) 78.3(18/23) 95.7(22/23) 73.9(17/23) 95.7(22/23) 91.3(21/23) 特异度 76.1(102/134) 40.3(54/134) 99.3(133/134) 58.2(78/134) 91.0(122/134) 91.8(123/134) 98.5(132/134) 准确率 78.3(123/157) 49.0(77/157) 96.2(151/157) 63.7(100/157) 88.5(139/157) 92.4(145/157) 97.5(153/157) 注: PYP为焦磷酸盐;H/CL为心脏与对侧肺摄取比值 Table 3. Comparison of the efficacy of 99Tcm-pyrophosphate (PYP) dual-phase planar imaging and tomographic imaging in diagnosis of transthyretin-related cardiac amyloidosis (%)
-
CA的2种常见临床分型为AL-CA和ATTR-CA,AL-CA多为肿瘤和感染等导致的多脏器淀粉样变性(包括心脏),常伴有血轻链蛋白水平升高;ATTR-CA是由于肝脏正常合成的甲状腺素转运蛋白解离成单体并错误折叠后沉积于心肌细胞间隙所导致的浸润性病变,根据形成原因不同,又可分为家族性突变型ATTR-CA和老年性野生型ATTR-CA[11]。AL-CA的预后极差,未经治疗的患者的中位生存期不超过6个月,主要治疗方法为化疗;ATTR-CA累及心脏相对较多,老年性野生型ATTR-CA在老年人群中的发病率为20%~30%,中位生存期为43~75个月[12]。AL-CA和ATTR-CA诊断的“金标准”为心内膜心肌活检免疫组织化学分析和基于质谱法的蛋白质组学分析[13],其临床操作复杂、不易开展。放射性核素显像是一种非侵入性的诊断方法,其中99Tcm-PYP显像在CA的分型诊断中的应用价值已得到了肯定[4, 14]。
美国核心脏病学会心脏淀粉样变多模态成像专家共识[8]认为早期平面显像诊断ATTR-CA的假阳性率高,因此本研究旨在比较目前国内外指南中推荐的各种阳性标准的诊断价值,优选最适合临床实践的显像方案。本研究中99Tcm-PYP双时相平面显像和断层显像中采用的阳性评价标准包括平面显像半定量分析法、Perugini法、断层显像半定量评分法,每种评价标准都包括了早期显像和延迟显像两个时相。美国核心脏病学会心脏淀粉样变多模态成像专家共识[8]推荐将早期平面显像H/CL≥1.5和延迟平面显像H/CL≥1.3作为99Tcm-PYP显像的阳性标准,为了降低假阳性率,本研究在此基础上还将延迟平面显像 H/CL≥1.5作为99Tcm-PYP显像的阳性标准。
本研究中,无论使用平面显像半定量分析法、Perugini法,还是断层显像半定量评分法,ATTR-CA患者对99Tcm-PYP均有高摄取,这证实了可以采用99Tcm-PYP显像来特异性诊断ATTR-CA,用于CA的无创性分型诊断。
早期平面显像无论采用平面显像半定量分析法还是Perugini法都出现了假阳性结果,这与文献报道的结论一致[3-7]。早期平面显像的特异度较低,尤其是Perugini法,特异度只有40.3%。早期断层显像半定量评分法的特异度为99.3%,但是灵敏度只有78.3%,这是由于早期断层显像半定量评分法中血池内放射性聚集明显,血池与心肌边界不清晰,都呈现放射性聚集,因此早期断层显像半定量评分为1分的患者例数较多,导致灵敏度降低。
延迟平面显像中以H/CL≥1.3作为99Tcm-PYP显像阳性标准时,非ATTR患者中共56例(56/134,41.8%)诊断为阳性,假阳性率高,特异度仅为58.2%,准确率仅为63.7%;以H/CL≥1.5作为99Tcm-PYP显像阳性标准时,特异度提高至91.0%,准确率达到88.5%。延迟平面显像中Perugini法诊断ATTR-CA的特异度提高至91.8%,准确率(92.4%)略低于早期断层显像。延迟断层显像半定量评分法诊断ATTR-CA的准确率最高,为97.5%,灵敏度和特异度分别为91.3%和98.5%。延迟断层显像时血池内放射性聚集明显清除,心肌与血池内本底的对比度增加,延迟断层显像半定量评分为2分的ATTR-CA患者比例升高,故其诊断准确率最高。
本研究结果显示,对于疑诊CA的患者,单纯采用早期平面显像可能会造成误诊,特别是对于Perugini法评分为2分的患者,最优选的方案是加做延迟断层显像。如果受限于技术或流程原因不能实现,早期断层显像或延迟平面显像 Perugini法(≥2分)也可以减少早期CA的误诊,从而提高诊断准确率。
利益冲突 所有作者声明无利益冲突
作者贡献声明 李薇负责数据的处理与统计分析、 论文的撰写;张宗耀负责设备的维护、 硬件的调试、设备参数的调节、 图像采集的协助;韩凯、王小迪负责图像的采集、 数据的整理与保存; 孙晓昕负责研究方案的设计与完善、研究过程的总体监督、论文的审阅与修订
Clinical application value of 99Tcm-PYP dual-phase planar imaging and tomographic imaging in the diagnosis of transthyretin-related cardiac amyloidosis
- Received Date: 2023-08-28
- Available Online: 2024-01-25
Abstract:
 DownLoad:
DownLoad: