







-
脑血管疾病是指脑部血管的各种疾病,包括脑动脉粥样硬化、脑梗死等[1-2],其可引起脑组织缺血或出血性意外的发生,导致患者认知障碍、残疾甚至死亡。目前,神经系统性疾病住院患者中脑血管疾病的发病率为25%~50%[3],且仍有继续上升的趋势,其中缺血性脑血管病占所有脑血管疾病的70%~80%,动脉粥样硬化是脑血管疾病发病的最主要病因。快速发现、准确定位病灶并确定责任血管对于脑血管病的诊断和治疗十分重要。
目前,磁共振DWI被认为是诊断急性期脑梗死(acute cerebral infarct,ACI)灵敏度最高的影像检查方法,其可反映脑内病灶局部区域水分子的扩散状态,并可通过表观扩散系数(apparent diffusion coefficient,ADC)直观地反映水分子的状态,ADC值越大,组织内的自由水分子越多。与常规MRI相比,DWI对新旧脑梗死的区分以及对腔隙脑梗死的诊断具有明显优势[4]。Wang等[5]的研究结果表明,DWI可以显示脑梗死病灶的部位、分布及其形态。磁共振血管成像(magnetic resonance angiography,MRA)具有操作简单、扫描时间短、灵敏度高、无创、无辐射、无需注射对比剂的优点[6],在临床上的应用较为广泛,其图像可辅助医师明确患者责任血管的位置和范围。DWI和MRA对于ACI患者病灶部位的诊断有时会存在差异,目前尚缺乏关于DWI与MRA对ACI患者诊断一致性的研究。本文对ACI患者的DWI和MRA影像资料进行综合分析,探究DWI与MRA对ACI患者的诊断一致性及其影响因素,从而为ACI患者的诊断及预后提供参考依据。
-
回顾性分析2020年1月至2022年2月于来安家宁医院接受诊治的98例疑似ACI患者的临床资料并纳入训练集,其中男性58例、女性40例,年龄45~80(60.5±3.3)岁,身体质量指数(body mass index,BMI)为(23.30±1.46) kg/m2。按照相同标准选取2022年3至10月于来安家宁医院接受诊治的33例疑似ACI患者纳入验证集,其中男性18例、女性15例,年龄42~79(61.1±3.6)岁,BMI为(23.21±1.23) kg/m2。纳入标准:(1)符合ACI的诊断标准[7],经MRI及CT检查确诊为ACI;(2)临床资料完整。排除标准:(1)合并严重心脏、肝脏、肾脏等器官功能障碍;(2)合并恶性肿瘤;(3)患有其他非血管性脑病;(4)有精神类疾病病史。所有患者均行DWI和MRA检查并在检查前签署了知情同意书。本研究经来安家宁医院医学伦理委员会的批准(批准号:20210817)。
-
收集所有患者的临床资料,包括年龄、性别、BMI、发病时间、吸烟史、饮酒史、高血压病史、糖尿病病史、高血脂病病史、临床表现、临床综合诊断[8]、美国国立卫生研究院卒中量表(national institute of health stroke scale, NIHSS)评分。
-
使用美国GE公司1.5T HDxt MRI,8通道头部线圈对所有患者进行检查。DWI:横断面平扫自旋回波(SE)序列为T1WI、液体衰减反转回复(fluid attenuated inversion recovery,FLAIR)序列和T2WI,b值分别为1 000 s/mm和0 s/mm。扫描参数:回波时间104 ms、重复时间 2 701 ms,层数18,矩阵152×113,层间距0 mm,激励1次,层厚5.5 mm,扫描时间34 s,视野射野23 cm。计算ADC和相对表观扩散系数(relative apparent diffusion coefficient,rADC),rADC=患侧ADC/健侧ADC。
MRA:以三维立体飞行时间法进行扫描。扫描参数:回波时间 6.9 ms、重复时间 25 ms,层数140,矩阵396×226,层间距10 mm,激励4次,层厚20 mm,扫描时间285 s,视野射野20 cm。
DWI和MRA的扫描范围均包括大脑前动脉,大脑中动脉,大脑后动脉主干、分支和Willis动脉环,观察病灶的位置、大小、狭窄程度(0级为闭塞,远端血管无显影;1级为缺失,远端血管部分显影;2级为狭窄>50%,远端血管完全显影;3级为狭窄≤50%,远端血管完全显影)等。
-
应用SPSS 23.0软件对数据进行统计学分析。符合正态分布的计量资料以
$\bar x \pm s $ -
98例疑似ACI的患者中,74例经临床综合诊断为ACI患者,其中DWI检出73例(假阴性7例,假阳性6例)(98.65%);MRA检出71例(假阴性9例,假阳性6例)(95.95%)。DWI与MRA诊断ACI的灵敏度、特异度、准确率、阳性预测值和阴性预测值的差异均无统计学意义(均P>0.05,表1)。
影像检查方法 灵敏度 特异度 准确率 阳性预测值 阴性预测值 弥散加权成像 90.54(67/74) 75.00(18/24) 86.73(85/98) 91.78(67/73) 72.00(18/25) 磁共振血管成像 87.84(65/74) 75.00(18/24) 84.69(83/98) 91.55(65/71) 66.67(18/27) χ2值 0.280 0.000 0.167 0.003 0.173 P值 0.597 1.000 0.683 0.960 0.677 Table 1. Comparison of diagnostic efficacy between diffusion weighted magnetic resonance imaging and magnetic resonance angiography in 98 suspected acute cerebral infarction patients (%)
-
74例确诊ACI的患者中,DWI检查结果为阳性的67例(90.54%),患者病灶表现为高信号,病灶定位与临床组织病理学检查结果一致。其中发病时间≤6 h的患者33例,DWI检出33例(100.00%),病灶表现为异常高信号;发病时间为6~24 h的患者30例,DWI检出26例(86.67%);发病时间为24~72 h的患者11例,DWI检出8例(72.73%)。67例ACI患者健侧与患侧脑组织ADC值的差异均有统计学意义(均P<0.05);与发病≤6 h相比,发病6~24 h的ACI患者患侧ADC值和rADC均明显降低,且差异均有统计学意义(均P<0.05);发病24~72 h的ACI患者患侧ADC值、rADC较发病6~24 h明显升高,且差异均有统计学意义(均P<0.05,表2)。74例ACI患者中,MRA检查结果为阳性的65例(87.84%)患者病变脑血管的分布情况及其狭窄程度见表3,病变血管多为大血管狭窄,其中以大脑中动脉狭窄最多,其次为大脑前动脉、大脑后动脉和颈内动脉、椎-基动脉和左椎动脉、右椎动脉。典型病例的DWI与MRA图像见图1。
发病时间(h) ADC(×10−4 cm2/s) rADC 患侧 健侧 ≤6(n=33) 0.59±0.11a 1.06±0.24 0.53±0.08 6~24(n=26) 0.44±0.10a,b 1.13±0.26 0.43±0.05b 24~72(n=8) 0.53±0.09a,c 1.05±0.17 0.49±0.06c 注:a表示与健侧相比,差异均有统计学意义(t=10.227、12.630、7.646,均P<0.05);b表示与≤6 h相比,差异均有统计学意义(t=5.410、5.569,均P<0.05);c表示与6~24 h相比,差异均有统计学意义(t=2.274、2.835,均P<0.05)。ADC为表观扩散系数;rADC为相对表观扩散系数 Table 2. Comparison of apparent diffusion coefficient and relative apparent diffusion coefficient values in diffusion weighted magnetic resonance imaging of 67 patients with acute cerebral infarction at different onset times
病变血管 狭窄程度 合计 0级 1级 2级 3级 颈内动脉 0 2 3 4 9 大脑前动脉 1 1 2 6 10 大脑中动脉 1 1 3 6 11 大脑后动脉 0 1 3 5 9 椎-基动脉 0 2 4 3 9 左椎动脉 1 1 2 5 9 右椎动脉 1 1 2 4 8 合计 4 9 19 33 65 Table 3. Distribution and stenosis degree of cerebrovascular lesions on magnetic resonance angiography in 65 patients with acute cerebral infarction (case)
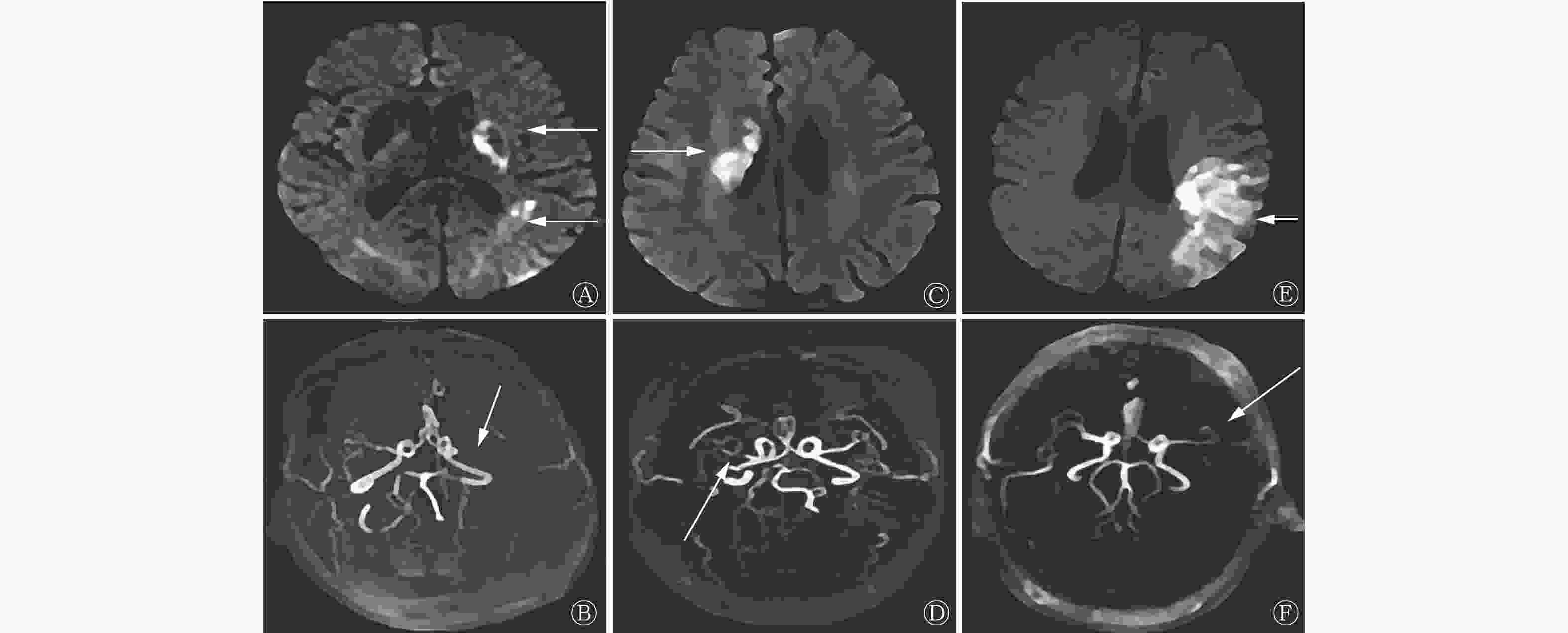
Figure 1. Diffusion weighted imaging and magnetic resonance angiography images of 3 patients with acute cerebral infarction
-
98例疑似ACI的患者中,DWI显示的脑梗死病灶位置与MRA病变血管一致的患者68例(69.39%),不一致的患者30例(30.61%),DWI与MRA检查结果的一致性良好(Kappa值=0.654,P<0.05)。DWI检查结果为阳性的73例患者中有16例MRA检查结果为阴性,DWI检查结果为阴性的25例患者中有14例MRA检查结果为阳性。DWI与MRA的检查结果均为阳性的患者的例数、病变血管和脑梗死病灶位置的分布情况:MRA表现为颈内动脉狭窄的患者6例,DWI显示为丘脑梗死灶;MRA表现为大脑前动脉主干狭窄的患者9例,DWI显示为额叶梗死灶;MRA表现为大脑中动脉主干狭窄的患者10例,其中DWI显示为颞叶梗死灶3例、基底节区梗死灶4例、半卵圆中心梗死灶3例;MRA表现为大脑后动脉主干狭窄的患者7例,DWI显示为枕叶梗死灶;MRA表现为椎-基动脉狭窄的患者8例,其中DWI显示为小脑梗死灶4例、脑干梗死灶4例;MRA表现为左椎动脉狭窄的患者9例,DWI显示为枕叶梗死灶;MRA表现为右椎动脉狭窄的患者8例,DWI显示为枕叶梗死灶。
-
DWI与MRA检查结果一致的患者为A组(68例),不一致的患者为B组(30例),比较两组患者的临床资料。与A组相比,B组中发病时间≤24 h、多发病灶、后循环、梗死病灶长径<2 cm患者的比例明显增加,NIHSS评分明显降低,且差异均有统计学意义(均P<0.05)。两组患者年龄、性别、BMI、吸烟史、饮酒史、糖尿病病史、高血压病史、高血脂病史以及临床表现的差异均无统计学意义(均P>0.05,表4)。
组别 年龄(岁) 性别[例(%)] BMI(kg/m2) 发病时间[例(%)] 吸烟史
[例(%)]饮酒史
[例(%)]男 女 ≤24 h >24 h A组(n=68) 60.11±3.17 38(55.88) 30(44.12) 23.14±1.05 45(66.18) 23(33.82) 22(32.35) 22(32.35) B组(n=30) 60.97±3.39 19(63.33) 11(36.67) 23.55±1.67 27(90.00) 3(10.00) 10(33.33) 9(30.00) 检验值 t=1.212 χ2=0.475 t=1.473 χ2=6.061 χ2=0.009 χ2=0.053 P值 0.229 0.491 0.144 0.014 0.924 0.817 组别 高血压病史
[例(%)]糖尿病病史
[例(%)]高血脂病史
[例(%)]临床表现[例(%)] 头痛、头晕 偏瘫 感觉功能障碍 失语 其他 A组(n=68) 51(75.00) 24(35.29) 21(30.88) 27(39.71) 35(51.47) 12(17.65) 2(2.94) 4(5.88) B组(n=30) 20(66.67) 12(40.00) 9(30.00) 9(30.00) 15(50.00) 7(23.33) 1(3.33) 2(6.67) 检验值 χ2=0.724 χ2=0.198 χ2=0.008 χ2=0.844 χ2=0.018 χ2=0.431 χ2=0.011 χ2=0.022 P值 0.395 0.656 0.930 0.358 0.893 0.512 0.917 0.881 组别 病灶情况[例(%)] 病灶位置[例(%)] 梗死病灶长径[例(%)] NIHSS评分(分) 单发病灶 多发病灶 前循环 后循环 <2 cm ≥2 cm A组(n=68) 53(77.94) 15(22.06) 55(80.88) 13(19.12) 5(7.35) 63(92.65) 7.36±2.50 B组(n=30) 17(56.67) 13(43.33) 15(50.00) 15(50.00) 21(70.00) 9(30.00) 6.31±1.93 检验值 χ2=4.617 χ2=9.728 χ2=41.913 t=2.045 P值 0.032 0.002 <0.001 0.044 注:BMI为身体质量指数;NIHSS为美国国立卫生研究院卒中量表 Table 4. Comparison of clinical data between diffusion weighted magnetic resonance imaging and magnetic resonance angiography in patients with acute cerebral infarction in the consistent group (Group A) and inconsistent group (Group B)
-
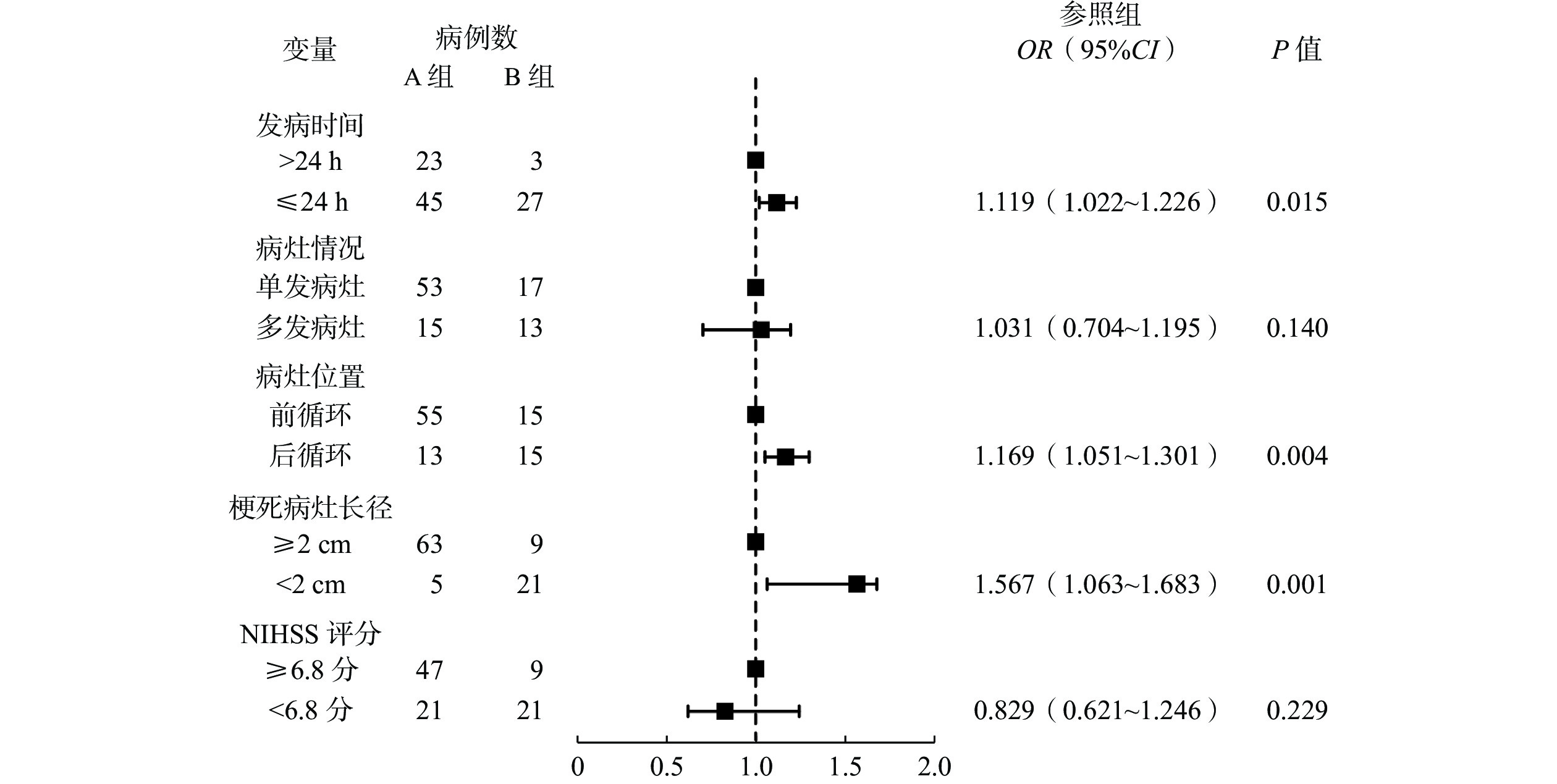
以DWI与MRA检查结果是否一致为因变量,以发病时间、病灶情况、病灶位置、梗死病灶长径、NIHSS评分为自变量,进行多因素Logistic回归分析,结果表明,发病时间≤24 h、后循环、梗死病灶长径<2 cm均是DWI与MRA检查结果不一致的独立危险因素(均P<0.05,图2、表5)。
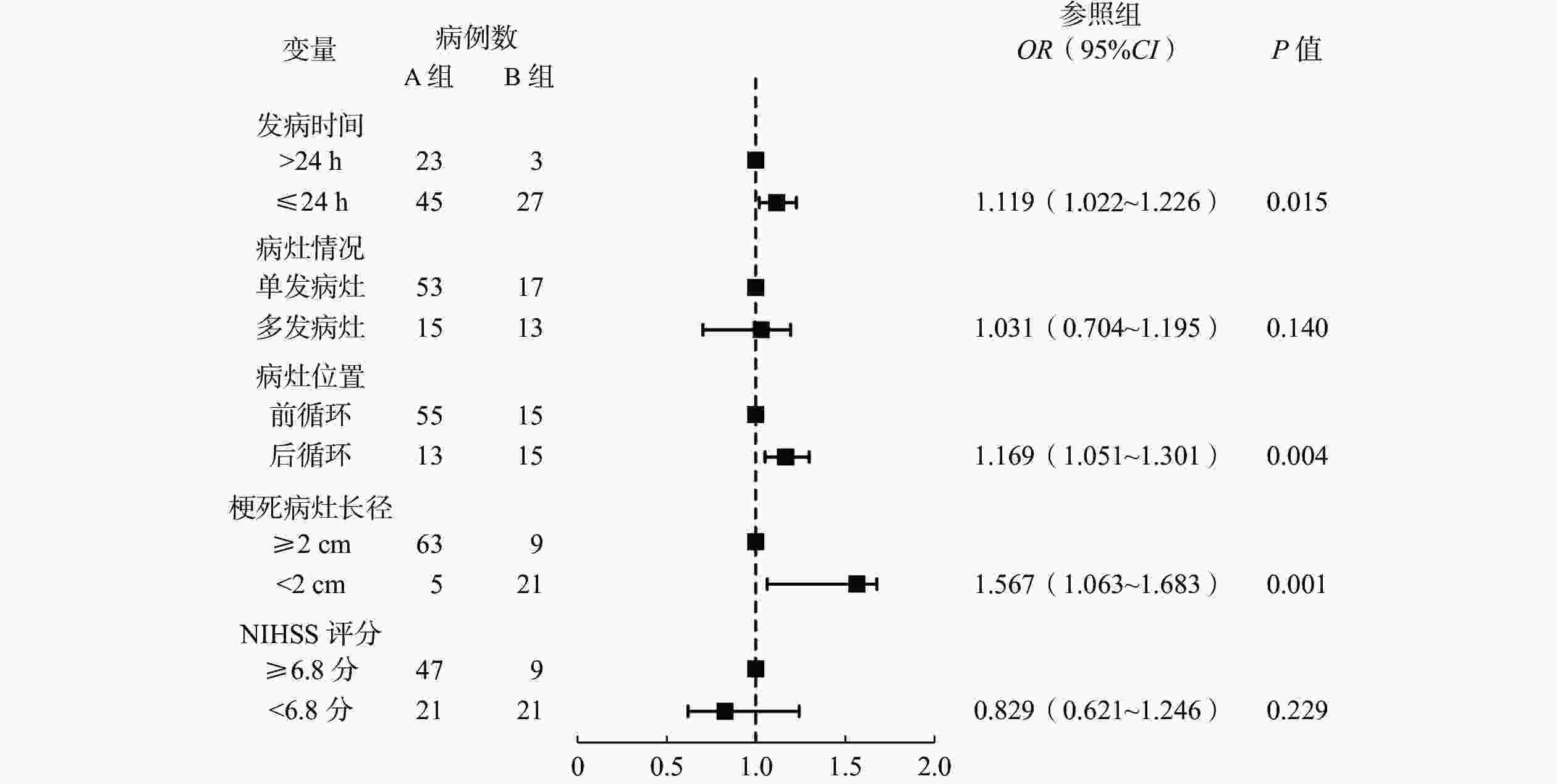
Figure 2. Forest map of risk factors for inconsistent results between diffusion weighted magnetic resonance imaging and magnetic resonance angiography in patients with acute cerebral infarction
指标 量化赋值 发病时间 >24 h=0,≤24 h=1 病灶情况 单发病灶=0,多发病灶=1 病灶位置 前循环=0,后循环=1 梗死病灶长径 ≥2 cm=0,<2 cm=1 NIHSS评分 ≥6.8分=0,<6.8分=1 DWI与MRA检查结果是否一致 否=0,是=1 注:DWI为弥散加权成像;MRA为磁共振血管成像;NIHSS为美国国立卫生研究院卒中量表 Table 5. Multivariate Logistic regression analysis quantitative assignment table for inconsistent results between diffusion weighted magnetic resonance imaging and magnetic resonance angiography in patients with acute cerebral infarction
-
根据ACI患者DWI与MRA检查结果不一致的独立危险因素构建风险列线图预测模型,其中发病时间≤24 h赋20分、后循环赋28分,梗死病灶长径<2 cm赋80分,总分为128分(图3)。

Figure 3. Risk column chart prediction model for inconsistent results between diffusion weighted magnetic resonance imaging and magnetic resonance angiography in patients with acute cerebral infarction
-
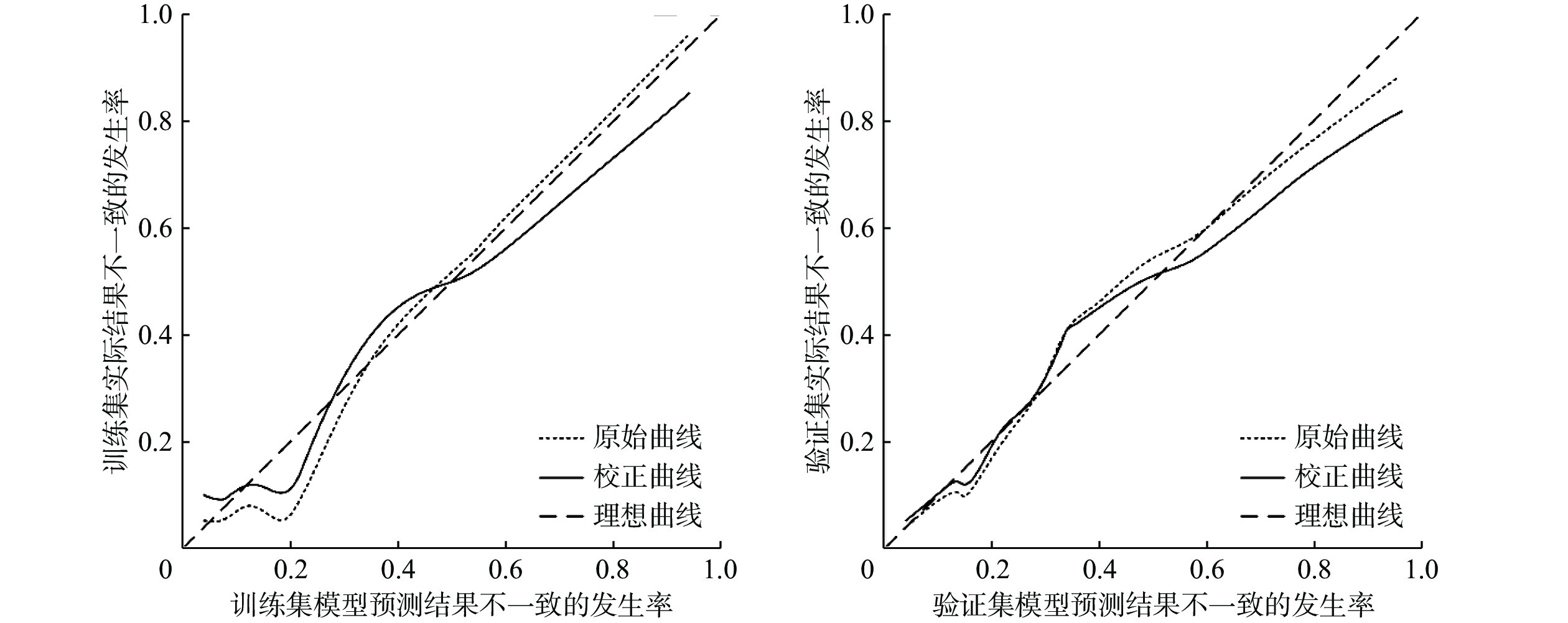
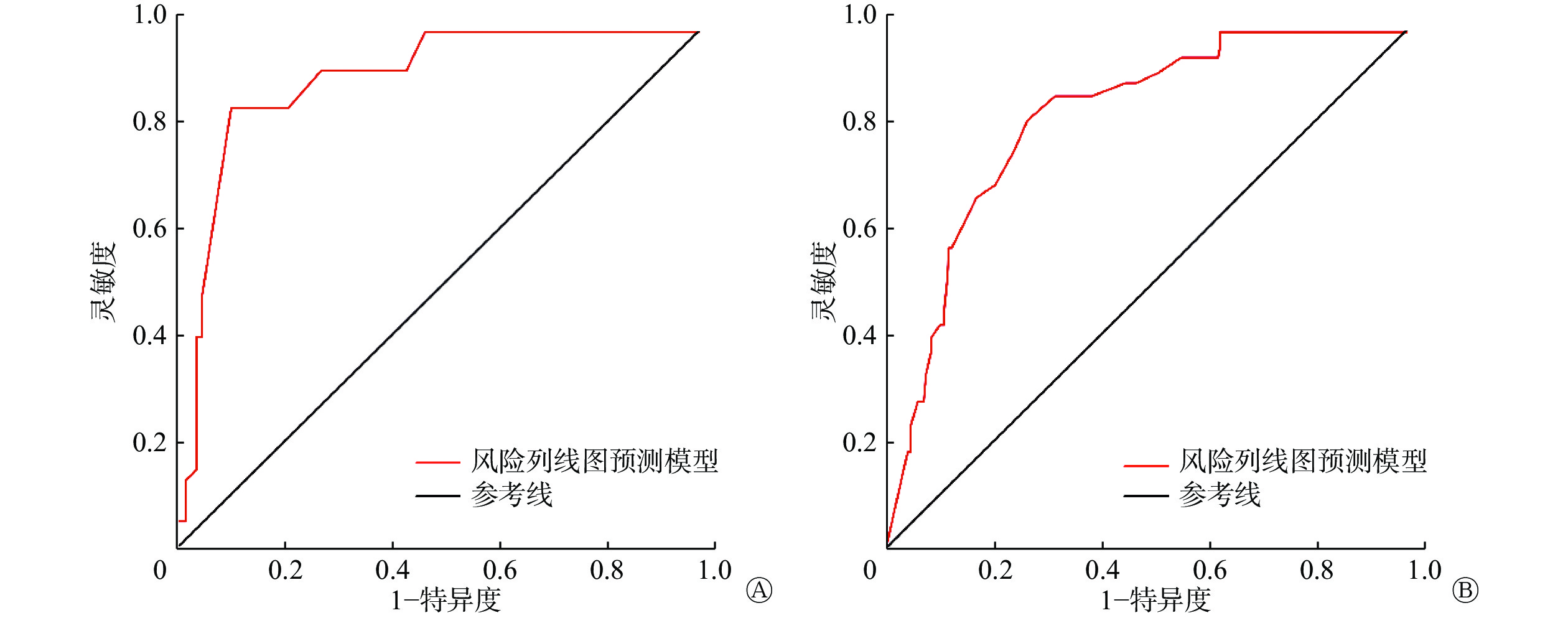
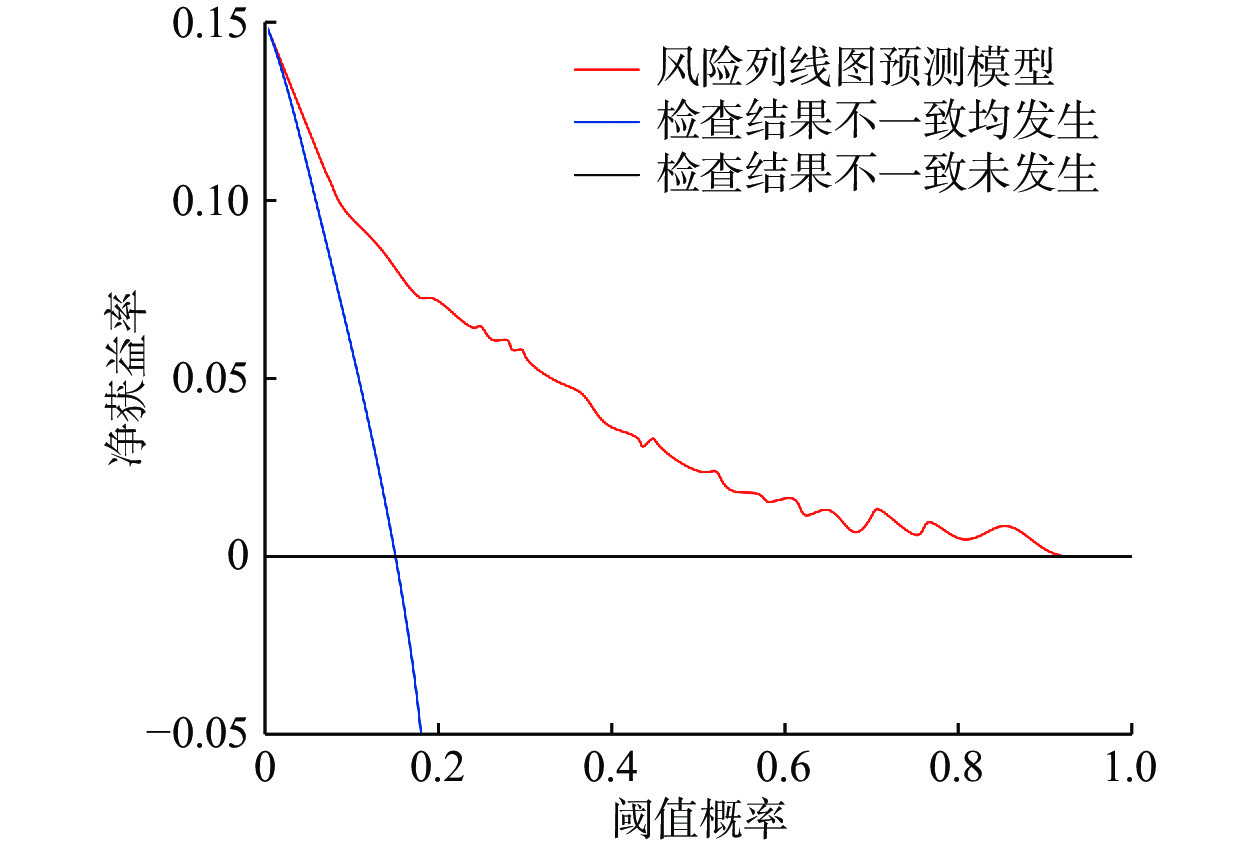
采用Bootstrap法(原始数据重复抽样1 000次后)对风险列线图预测模型进行内部验证,外部验证通过验证集进行验证。训练集和验证集的一致性指数(concordance index,C-index)分别为0.880(95%CI:0.844~0.916,P<0.001)和0.812(95%CI:0.785~0.839,P<0.001)。训练集和验证集的校正曲线与理想曲线均拟合良好(图4)。训练集和验证集ROC的AUC分别为0.930(95%CI:0.899~0.961,P<0.001)、0.855(95%CI:0.812~0.898,P<0.001)(图5)。风险列线图预测模型的DCA曲线显示阈值概率在1%~92%时,净获益率>0(图6)。以上结果均显示该风险列线图预测模型具有较高的精准度,且有效性较好,安全可靠,实用性强。
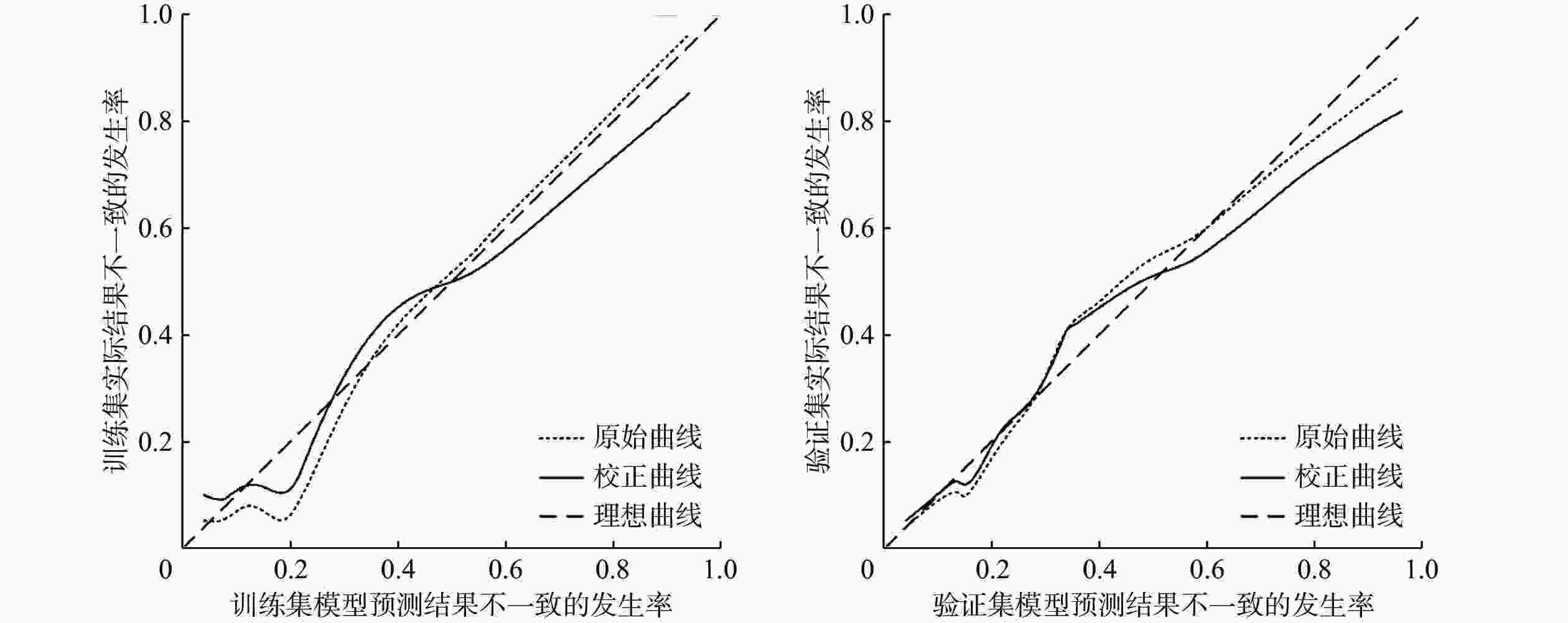
Figure 4. Correction curves of the training and validation sets of the risk column chart prediction model for inconsistent results between diffusion weighted magnetic resonance imaging and magnetic resonance angiography in patients with acute cerebral infarction
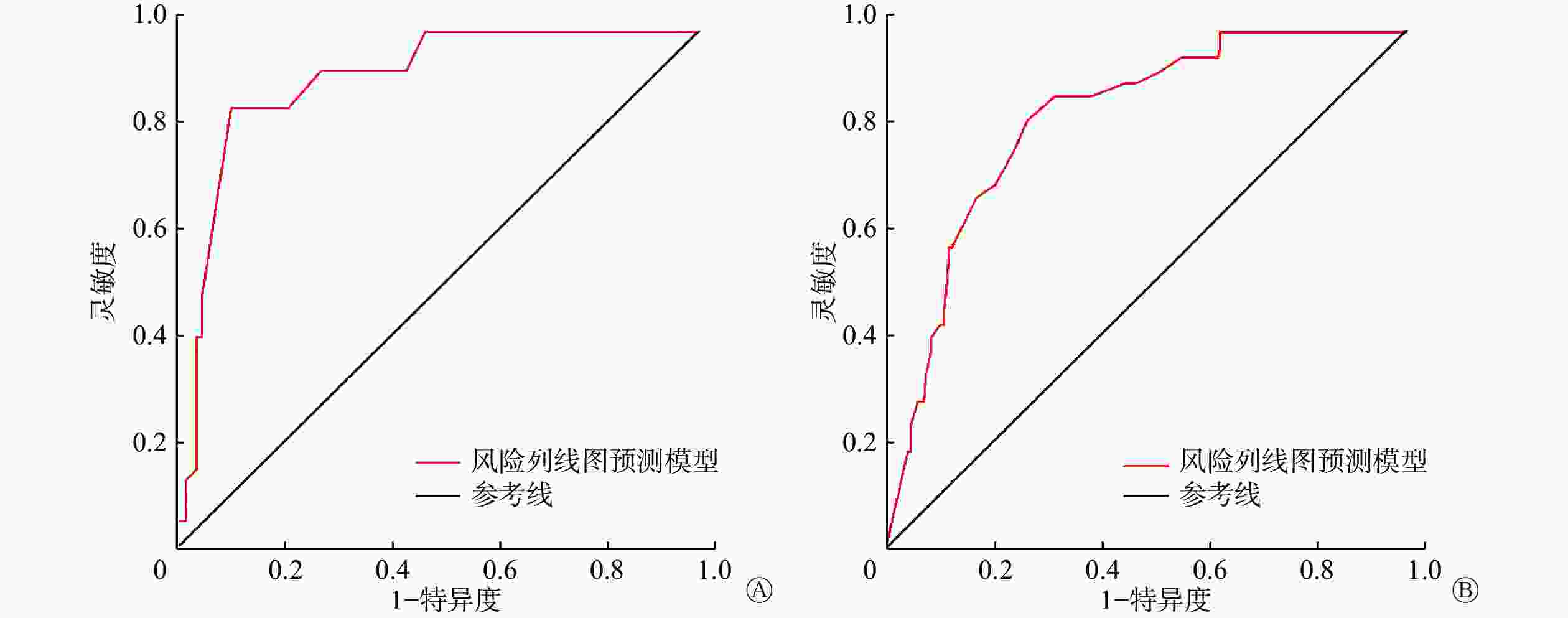
Figure 5. The receiver operating characteristic curve of the risk column chart prediction model training set (A) and validation set (B) for acute cerebral infarction patients with inconsistent results between diffusion weighted magnetic resonance imaging and magnetic resonance angiography

Figure 6. Decision curve analysis of risk column chart prediction model for inconsistent results between diffusion weighted magnetic resonance imaging and magnetic resonance angiography in patients with acute cerebral infarction
-
ACI的发病机制较复杂且危险因素较多,其中以颈动脉粥样硬化最常见[9]。随着人口老龄化的加剧,ACI的发病率不断上升,且其致残、致死率均较高[10]。因此,早期诊断,及时预防、干预,改善ACI患者的预后是临床工作、研究的重点。
近年来,影像检查作为ACI诊断和辅助治疗的主要方法迅速发展。传统CT和常规MRI的诊断灵敏度较低,需要在ACI发病较长时间后才能定位病灶,且难以界定病灶的范围,因此临床应用的价值较低[11]。DWI可早期发现ACI病灶,并准确判断病灶的部位和体积,对ACI患者神经功能的受损情况进行定量评估,为临床医师的诊断及治疗提供依据[12]。本研究结果显示,ACI患者患侧和健侧脑组织ADC值的差异均有统计学意义。患侧ADC值和rADC在患者发病后先明显降低,发病24 h后明显升高,其原因可能是ACI患者在发病24 h内病情逐渐加重,脑细胞的代谢紊乱,导致细胞膜Na+/K+-ATP酶失活,造成水钠潴留,限制了水分子的弥散,使rADC降低。ACI患者发病24 h后rADC升高可能与病灶部位血液灌注的恢复有关。因此,ACI患者发病后72 h内,临床医师可通过rADC了解患者的病理、生理改变和病情变化。
脑部主要供血动脉狭窄或闭塞是ACI发病的主要机制,虽然DWI可定位病灶并对病情进行评估,但无法显示主要的责任血管[13],因此本研究采用MRA检查主要责任血管的位置。MRA可显示三级以上分支动脉血管的狭窄或闭塞情况,且MRA检测出的病变血管与DWI图像显示的病灶位置具有解剖关系,但血液涡流会使MRA图像出现伪影进而造成误诊[14]。MRA可根据血管的狭窄程度和远端血管的显影情况对患者的严重程度进行分级,评估病情,用以指导临床治疗。
本研究中,DWI与MRA检查结果一致的患者68例(69.39%),不一致患者30例(30.61%),二者的一致性较好。多因素Logistic回归分析结果显示,发病时间≤24 h、后循环、梗死病灶长径<2 cm均是DWI与MRA检查结果不一致的独立危险因素。ACI发病早期,患者脑组织的缺血程度或血管狭窄程度较轻,或疾病处于逐渐进展的状态,可能出现漏诊,导致DWI与MRA检查结果不一致。王继蕊等[15]的研究结果表明,在ACI患者发病早期,较多患者的DWI结果为阴性,起病后120 h DWI结果才为阳性。ACI患者脑部梗死病灶过小可能造成漏诊,因此DWI结果为阴性的病灶一般较小,且发生在后循环的概率大于前循环。白向东等[16]的研究结果亦表明,ACI患者DWI-FLAIR不匹配组发生后循环梗死的比例较DWI-FLAIR匹配组高,证实了后循环对脑缺血的耐受性更强、溶栓时间可以适当延长的结论。本研究中,风险列线图预测模型结果显示各危险因素总计128分。ROC曲线、校正曲线和DCA曲线的评价结果显示,该风险列线图预测模型的区分度、准确率和有效性均较高。
本研究具有一定的局限性,如样本量相对不足,且研究周期较短等,因此难免存在一些偏倚。
综上所述,DWI与MRA检查对于ACI患者诊断的一致性较好。发病时间≤24 h、后循环、梗死病灶长径<2 cm均是DWI与MRA检查结果不一致的独立危险因素。DWI可显示早期ACI病灶的位置和缺血程度,MRA则可准确定位责任血管及其狭窄程度,DWI和MRA的广泛应用,使ACI的早期诊断成为可能,从而使医师及时干预,缓解病情,改善患者预后。
利益冲突 所有作者声明无利益冲突
作者贡献声明 高爽负责命题的提出与设计、方法的建立、数据的分析、论文的撰写;王三刚负责论文的修订、数据的收集
Diagnosis consistency and influencing factors of DWI and MRA in patients with acute cerebral infarction
- Received Date: 2022-12-21
- Available Online: 2024-02-25
Abstract:

 DownLoad:
DownLoad: