






-
甲状腺结节(thyroid nodule,TN)是指甲状腺细胞在甲状腺局部异常生长所引起的散在病变,临床常见,发病影响因素较多[1]。临床上,甲状腺炎症、甲状腺腺瘤和甲状腺囊肿等甲状腺疾病均可表现为TN。TN可为单发和多发,多发TN概率较高,但单发TN癌变风险较高[2]。TN多数为良性病变,少数为恶性病变。甲状腺癌前期无明显的临床特征,易漏诊,这使其发病风险在世界范围内显著增加[3],因此对TN的诊断及治疗至关重要。
目前,由于超声具有优异的时空分辨率,其已成为诊断和评估TN的首选检测技术,尤其是对于无症状的甲状腺癌[4]。随着临床上高频超声的广泛应用,TN的检出概率可达到68%[5]。评估TN的发生风险可帮助临床医师对其治疗方式进行选择。临床上采用甲状腺影像报告和数据系统(thyroid imaging reporting and data system,TIRADS)以提高诊断TN的准确率。2017年美国放射学会(American College of Radiology,ACR)提出的TIRADS(ACR-TIRADS)已在我国临床工作中广泛应用[6];同年,欧洲甲状腺协会也发布了成人TN超声恶性风险分层指南,即欧洲甲状腺协会甲状腺影像报告和数据系统(简称EU-TIRADS)[7]。2种TIRADS版本不同,其分层依据也不同,尚无统一标准[8]。目前,关于不同版本TIRADS的研究多数是对TIRADS诊断效能的研究,一致性研究较少,而可重复性和一致性对其是否能在临床上普及和推广十分重要。本研究就TN患者的ACR-TIRADS和EU-TIRADS资料进行综合评价,探究二者的诊断一致性及影响因素,从而为TN患者的诊断和预后以及TIRADS的临床适用性提供参考依据。
-
回顾性分析2019年6月至2022年1月于来安家宁医院(272例)和南京医科大学附属南京医院(10例)经细针穿刺活检(fine needle aspiration,FNA)或手术组织病理学检查结果确诊的282例TN患者的年龄、性别、TN情况(大小、个数、结构、回声、形状、边缘、钙化)、ACR-TIRADS和EU-TIRADS检查结果等资料,其中男性72例、女性210例,年龄(45.9±10.9)岁。纳入标准:(1)经FNA或手术获得组织病理学检查结果确诊;(2)临床资料完整。排除标准:(1)既往有甲状腺手术史;(2)肝肾功能不全、凝血功能障碍、意识障碍;(3)既往有颈部手术史。所有患者均于检查前签署了知情同意书。本研究通过了来安家宁医院医学伦理委员会的批准(批准号:20211208)。
-
使用美国GE公司的Logiq E9型彩色多普勒超声诊断仪(线阵探头,频率9~15 MHz)、佳能医疗系统有限公司的Aplio 700型彩色多普勒超声诊断仪(线阵探头,频率5~14 MHz)、日本东芝公司的Aplio 500型彩色多普勒超声诊断仪(线阵探头,探头频率5~11 MHz)对282例患者的所有TN分别进行ACR-TIRADS和EU-TIRADS分类。
由2位分别有12年和8年甲状腺超声诊断经验的医师进行标准化检查并存图。研究前系统学习ACR-TIRADS[9]和EU-TIRADS分类依据及相关超声征象并选取30个TN讨论并达成一致意见。意见不一致时,再取30个TN讨论直至意见一致。2位超声医师回顾入选患者超声图像,将入选患者的超声征象录入数据库。恶性TN超声诊断征象[10]:实性结节,低或极低回声,边界模糊、不规则,微钙化,纵横比值>1。
-
应用SPSS 23.0软件对数据进行统计学分析。符合正态分布的计量资料以
$\bar x\pm s $ 以FNA和手术获得的组织病理学检查结果为“金标准”,构建ACR-TIRADS和EU-TIRADS分类鉴别诊断良恶性TN的ROC,计算AUC,采用McNemar配对χ2检验比较二者的诊断准确性;采用多分类资料的Kappa检验进行一致性分析;计算灵敏度、特异度、准确率、阳性预测值、阴性预测值以及约登指数。采用Empower Stats和统计软件包“R”绘制森林图。采用Bootstrap法进行多因素Logistic回归预测模型校准度的内部验证。以ACR-TIRADS和EU-TIRADS检查结果相符为A组,不相符为B组,比较2组的超声诊断特征。以赋值为0的变量下的分层为对照分层,以赋值为1的变量下的分层为测试分层;以2种系统检查结果不相符为因变量,以A、B 2组患者超声诊断特征差异有统计学意义的指标为自变量,采用多因素Logistics回归预测模型分析ACR-TIRADS和EU-TIRADS检查结果不相符的独立危险因素。采用临床决策曲线评价模型的精准度。检验水准α=0.05。
-
282例患者共检测出320个TN,其中FNA检测出166个TN(118个良性TN、48个恶性TN);手术检测出154个TN(30个良性TN,124个恶性TN)。
-
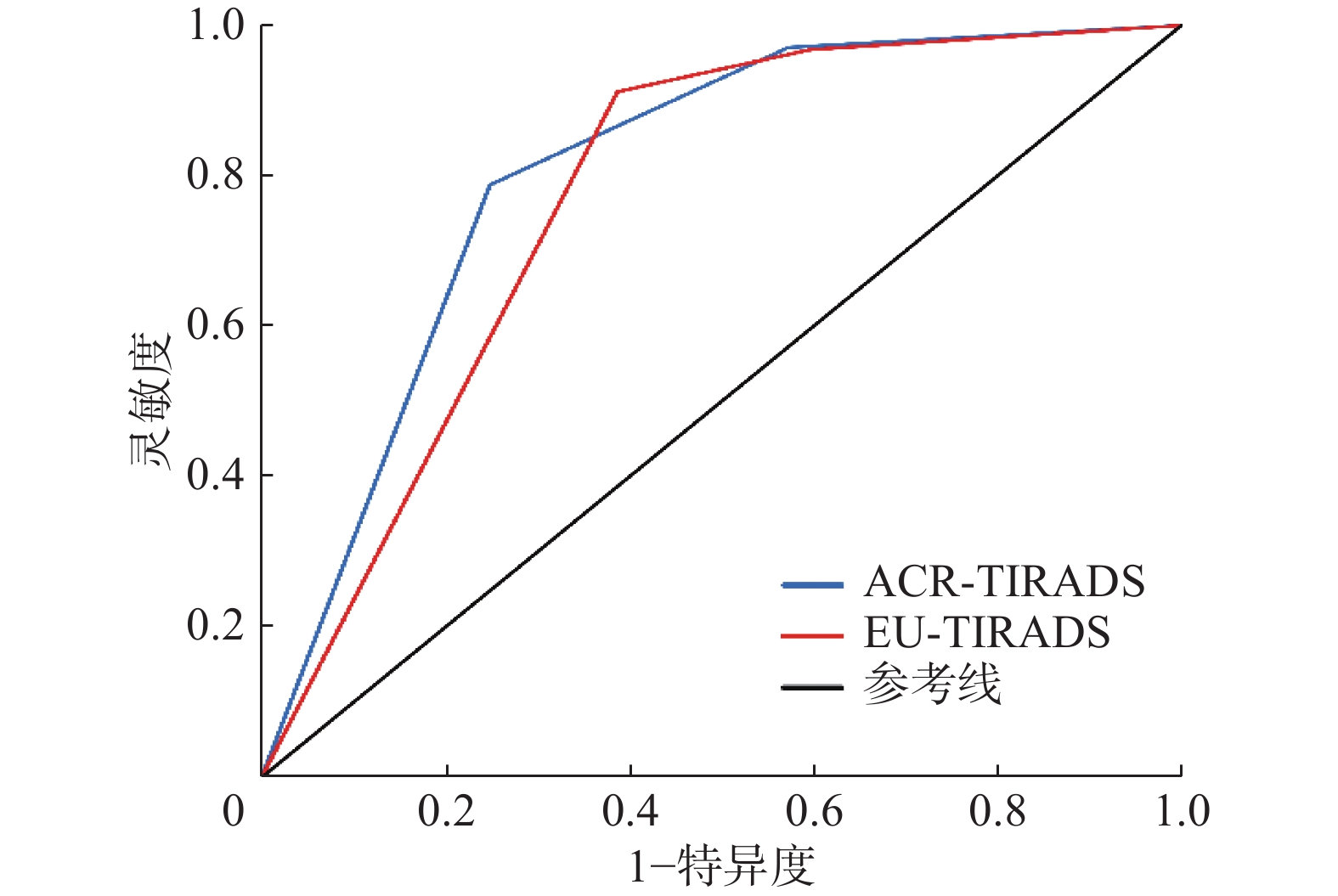
由表1可知,TN的恶性风险均随着ACR-TIRADS和EU-TIRADS分类类别升高而增加。 ACR-TIRADS和EU-TIRADS构建ROC曲线的结果显示,其AUC分别为0.812(95%CI:0.771~0.853)和0.795(95%CI:0.754~0.836),约登指数最大值分别为0.544、0.531,所对应的临界值均为5类(图1)。
甲状腺结节 ACR-TIRADS[例(%)] EU-TIRADS[例(%)] 1类 2类 3类 4类 5类 2类 3类 4类 5类 良性结节(n=148) 4(2.70) 30(20.27) 29(19.59) 49(33.11) 36(24.32) 5(3.38) 55(37.16) 31(20.95) 57(38.51) 恶性结节(n=172) 0(0.00) 2(1.16) 3(1.74) 32(18.60) 135(78.49) 0(0.00) 6(3.49) 9(5.23) 157(91.28) 恶性风险(%) 0(0.00) 6.25 9.38 39.51 78.95 0(0.00) 9.84 22.50 73.36 注:数字1~5表示不同的分类类别。ACR-TIRADS为美国放射学会甲状腺影像报告和数据系统;EU-TIRADS为欧洲甲状腺协会甲状腺影像报告和数据系统 Table 1. Malignant risk analysis of thyroid nodule in American College of Radiology-thyroid imaging reporting and data system and European Thyroid Association-thyroid imaging reporting and data system
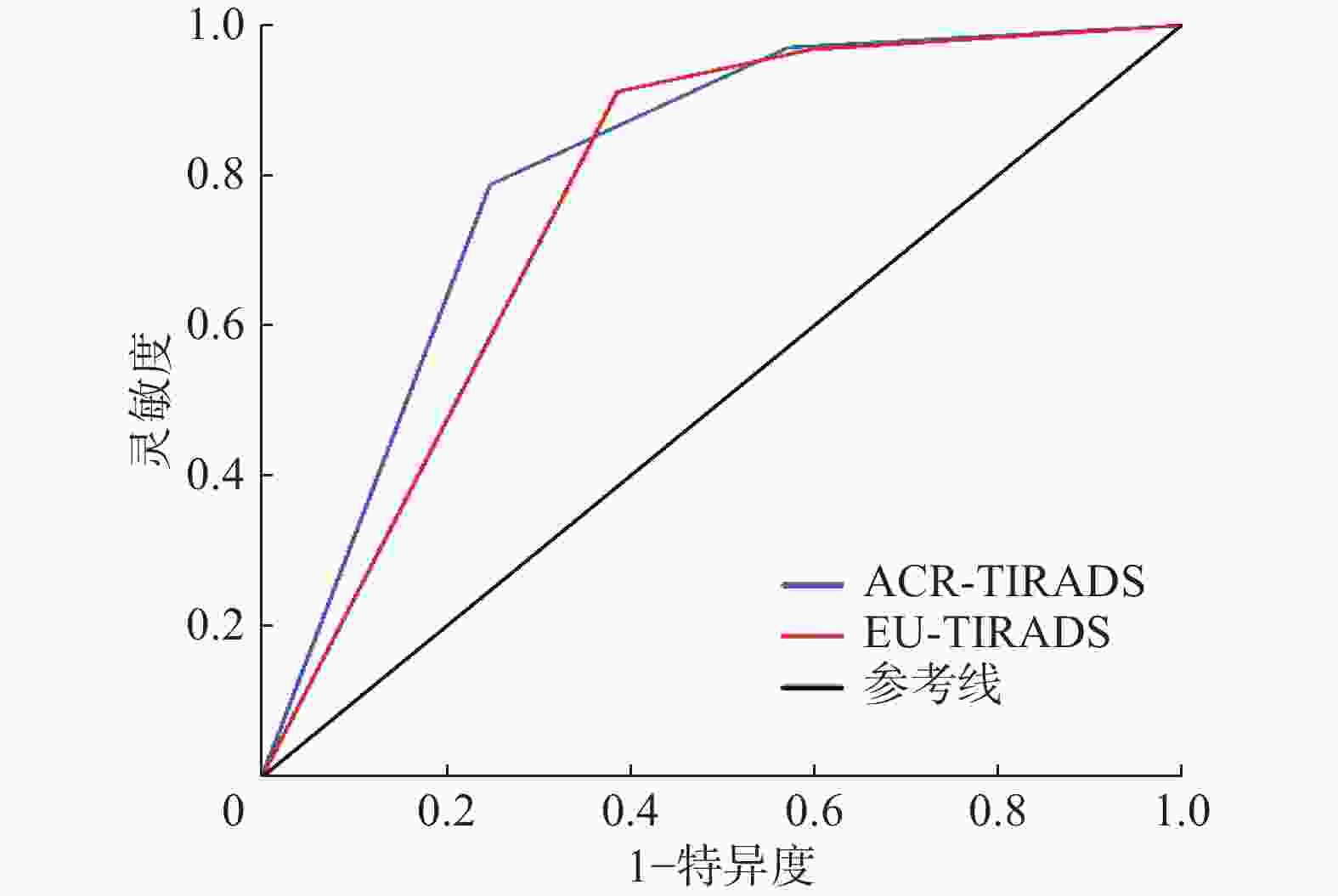
Figure 1. Receiver operating characteristic curves for differential diagnosis of benign and malignant thyroid nodules using American College of Radiology-thyroid imaging reporting and data system and European Thyroid Association-thyroid imaging reporting and data system
ACR-TIRADS和EU-TIRADS的诊断准确率(78.01%对77.62%)、阳性预测值(78.95%对73.36%)的差异均无统计学意义(χ2=0.036、2.796,P=0.849、0.095);EU-TIRADS较ACR-TIRADS的诊断阴性预测值(85.74%对74.75%)、灵敏度(91.54%对79.31%)均更高,差异均有统计学意义(χ2=12.034、19.135,P=0.001、<0.001);ACR-TIRADS较EU-TIRADS的诊断特异度(75.67%对62.38%)更高,差异有统计学意义(χ2=12.900,P<0.001)。
-
由表2、表3可知,ACR-TIRADS 2~4类无论是良性还是恶性TN均与EU-TIRADS 2~4类一致性良好。由表4可知,ACR-TIRADS和EU-TIRADS一致性分析结果显示,ACR-TIRADS 2类中所有TN(18个)均与EU-TIRADS 2类相对应;ACR-TIRADS 3类中有77个TN(96.25%,77/80)与EU-TIRADS 3类相对应;ACR-TIRADS 4类中有70个TN(94.59%,70/74)与EU-TIRADS 4类相对应;ACR-TIRADS 5类中有94个TN(63.51%,94/148)与EU-TIRADS 4类相对应,另外ACR-TIRADS 5类中有54个TN(36.49%,54/148)与EU-TIRADS 5类相对应。
ACR-TIRADS EU-TIRADS 合计 Kappa值 P值 准确率(%) 2 3 4 5 2 0(0.00) 0(0.00) 0(0.00) 0(0.00) 0(0.00) 0.375 <0.001 − 3 1(0.58) 8(4.65) 0(0.00) 0(0.00) 9(5.23) − − − 4 0(0.00) 0(0.00) 30(17.44) 0(0.00) 30(17.44) − − − 5 0(0.00) 0(0.00) 85(49.42) 48(27.91) 133(77.33) − − − 合计 1(0.58) 8(4.65) 115(66.86) 48(27.91) 172(100.00) − − 50.00 注:数字2~5表示不同的分类类别;−表示无此项数据。ACR-TIRADS为美国放射学会提出的甲状腺影像报告与数据系统;EU-TIRADS为欧洲甲状腺协会提出的甲状腺影像报告与数据系统 Table 2. Consistency analysis of American College of Radiology-thyroid imaging reporting and data system and European-thyroid imaging reporting and data system in the examination results of malignant thyroid nodule (cases (%))
ACR-TIRADS EU-TIRADS 合计 Kappa值 P值 准确率(%) 2 3 4 5 2 18(12.16) 0(0.00) 0(0.00) 0(0.00) 18(12.16) 0.844 <0.001 − 3 2(1.35) 69(46.62) 0(0.00) 0(0.00) 71(47.97) − − − 4 0(0.00) 2(1.35) 40(27.03) 2(1.35) 44(29.73) − − − 5 0(0.00) 0(0.00) 9(6.08) 6(4.05) 15(10.14) − − − 合计 20(13.51) 71(47.97) 49(33.11) 8(5.41) 148(100.00) − − 89.86 注:数字2~5表示不同的分类类别;−表示无此项数据。ACR-TIRADS为美国放射学会提出的甲状腺影像报告与数据系统;EU-TIRADS为欧洲甲状腺协会提出的甲状腺影像报告与数据系统 Table 3. Consistency analysis of American College of Radiology-thyroid imaging reporting and data system and European-thyroid imaging reporting and data system in the examination results of benign thyroid nodule (cases (%))
ACR-TIRADS EU-TIRADS 合计 Kappa值 P值 准确率(%) 2 3 4 5 2 18(5.63) 0(0.00) 0(0.00) 0(0.00) 18(5.63) 0.571 <0.001 − 3 3(0.94) 77(24.06) 0(0.00) 0(0.00) 80(25.00) − − − 4 0(0.00) 2(0.63) 70(21.88) 2(0.63) 74(23.13) − − − 5 0(0.00) 0(0.00) 94(29.38) 54(16.88) 148(46.25) − − − 合计 21(6.56) 79(24.69) 164(51.25) 56(17.50) 320(100.00) − − 68.44 注:数字2~5表示不同的分类类别;−表示无此项数据。ACR-TIRADS为美国放射学会提出的甲状腺影像报告与数据系统;EU-TIRADS为欧洲甲状腺协会提出的甲状腺影像报告与数据系统 Table 4. Consistency analyzing of American College of Radiology-thyroid imaging reporting and data system and European-thyroid imaging reporting and data system in the examination results of thyroid nodules (cases (%))
-
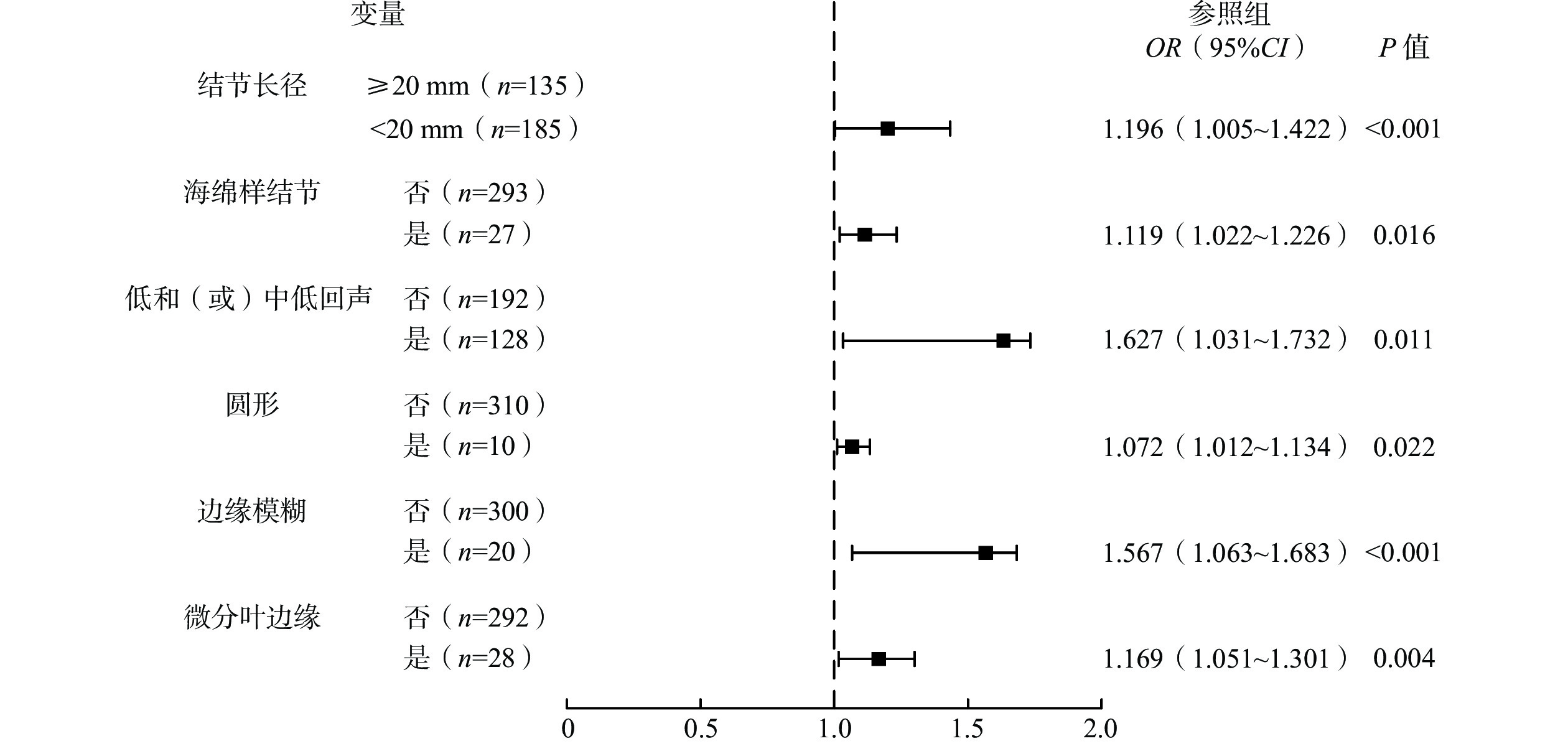
ACR-TIRADS和EU-TIRADS检查结果相符的A组TN共219个,不相符的B组TN共 101个。A、B 2组的超声诊断特征比较结果显示,结节长径(10~15 mm、≥20 mm)、囊性或几乎囊性、海绵样结节、低和(或)中低回声、圆形、边缘以及微钙化均是ACR-TIRADS和EU-TIRADS检查结果不相符的相关因素,差异均有统计学意义(均P<0.05,表5)。多因素Logistic回归分析结果显示,结节长径<20 mm、海绵样结节、低和(或)中低回声、圆形、边缘模糊以及微分叶边缘,均是2种系统检查结果不相符的独立危险因素(均P<0.05,图2)。
组别 结节长径 结构 5~10 mm 10~15 mm 15~20 mm ≥20 mm 囊性或几乎囊性 囊实性 实性或几乎实性 海绵样结节 A组(n=219) 25(11.42) 42(19.18) 39(17.81) 113(51.60) 19(8.68) 54(24.66) 136(62.10) 10(4.57) B组(n=101) 14(13.86) 42(41.58) 23(22.77) 22(21.78) 2(1.98) 21(20.79) 61(60.40) 17(16.83) χ2值 0.386 17.925 1.090 25.195 5.054 0.576 0.085 13.460 P值 0.534 <0.001 0.296 <0.001 0.025 0.448 0.771 <0.001 组别 回声 形状 边缘 高回声或等回声 低和(或)
中低回声极和(或)
显著低回声卵圆形 圆形 直立生长
(纵横比值>1)光滑 模糊 A组(n=219) 98(44.75) 77(35.16) 44(20.09) 175(79.91) 2(0.91) 42(19.18) 187(85.39) 7(3.20) B组(n=101) 35(34.65) 51(50.50) 15(14.85) 80(79.21) 8(7.92) 13(12.87) 53(52.48) 13(12.87) χ2值 2.900 6.773 1.262 0.021 11.212 1.932 39.934 11.042 P值 0.089 0.009 0.261 0.885 0.001 0.165 <0.001 0.001 组别 边缘 钙化 微分叶 针刺样边缘 甲状腺外侵犯 粗大钙化 边缘钙化 微钙化 孤立性性钙化 A组(n=219) 12(5.48) 11(5.02) 2(0.91) 12(5.48) 5(2.28) 62(28.31) 3(1.37) B组(n=101) 16(15.84) 14(13.86) 5(4.95) 8(7.92) 1(0.99) 17(16.83) 0(0.00) χ2值 9.296 7.497 5.266 0.703 0.628 4.899 1.397 P值 0.002 0.006 0.022 0.402 0.428 0.027 0.237 注:ACR-TIRADS为美国放射学会甲状腺影像报告和数据系统;EU-TIRADS为欧洲甲状腺协会甲状腺影像报告和数据系统 Table 5. Comparison of ultrasound diagnostic characteristics between two groups of patients with consistent or inconsistent American College of Radiology-thyroid imaging reporting and data system and European-thyroid imaging reporting and data system examination results (cases (%))

Figure 2. Forest map of risk factors with inconsistent American College of Radiology-thyroid imaging reporting and data system and European-thyroid imaging reporting and data system inspection results
-
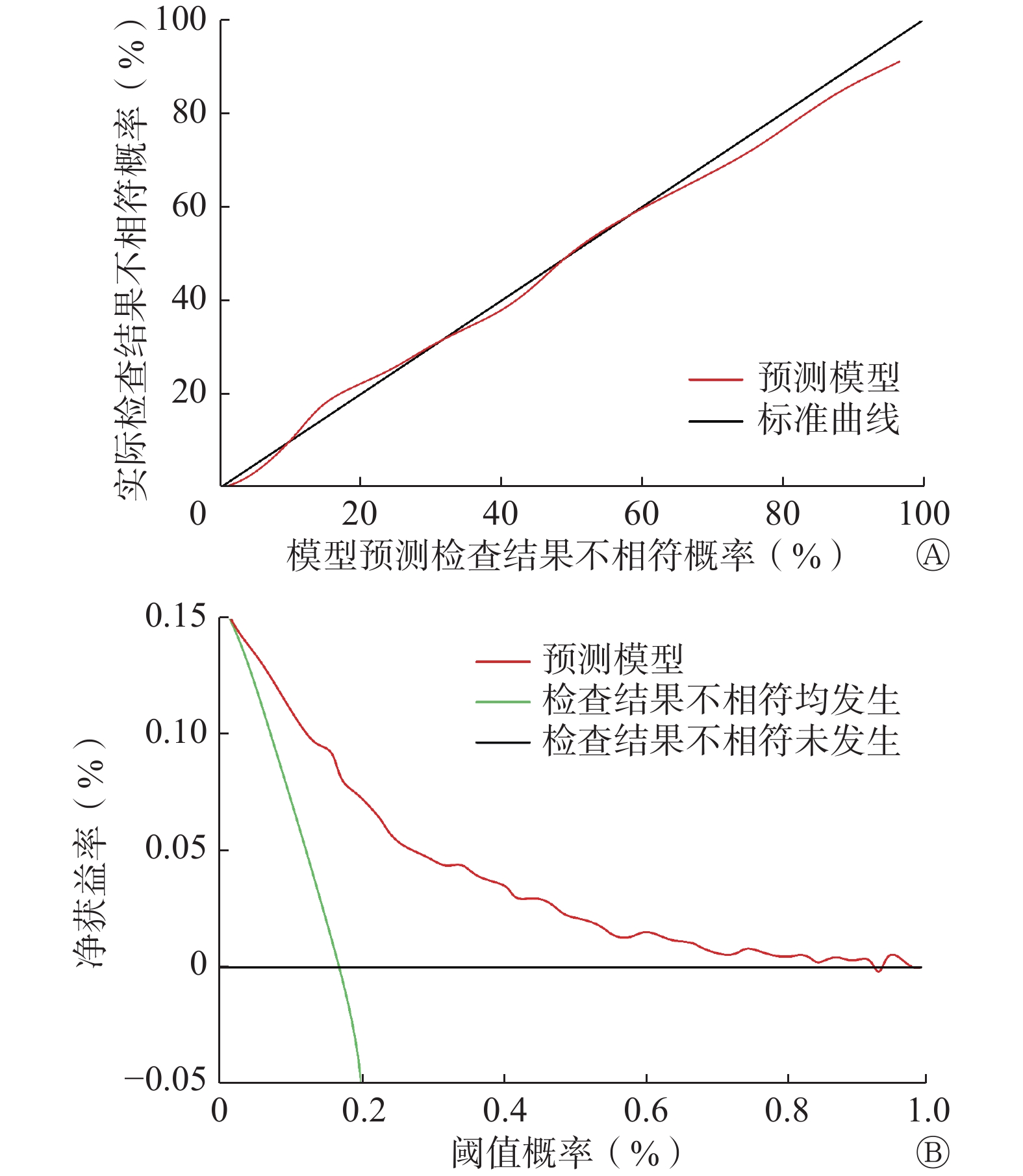
经Bootstrap法内部验证后C指数相同,多因素Logistic回归模型预测ACR-TIRADS和EU-TIRADS检查结果不相符情况与实际情况一致。校准图显示,Logistic回归预测模型与标准曲线拟合度良好(图3A)。通过临床决策曲线评估模型对预测ACR-TIRADS和EU-TIRADS检查结果不相符风险的临床净获益情况。模型阈值概率在0.01~0.94区间时,净获益率>0(图3B)。
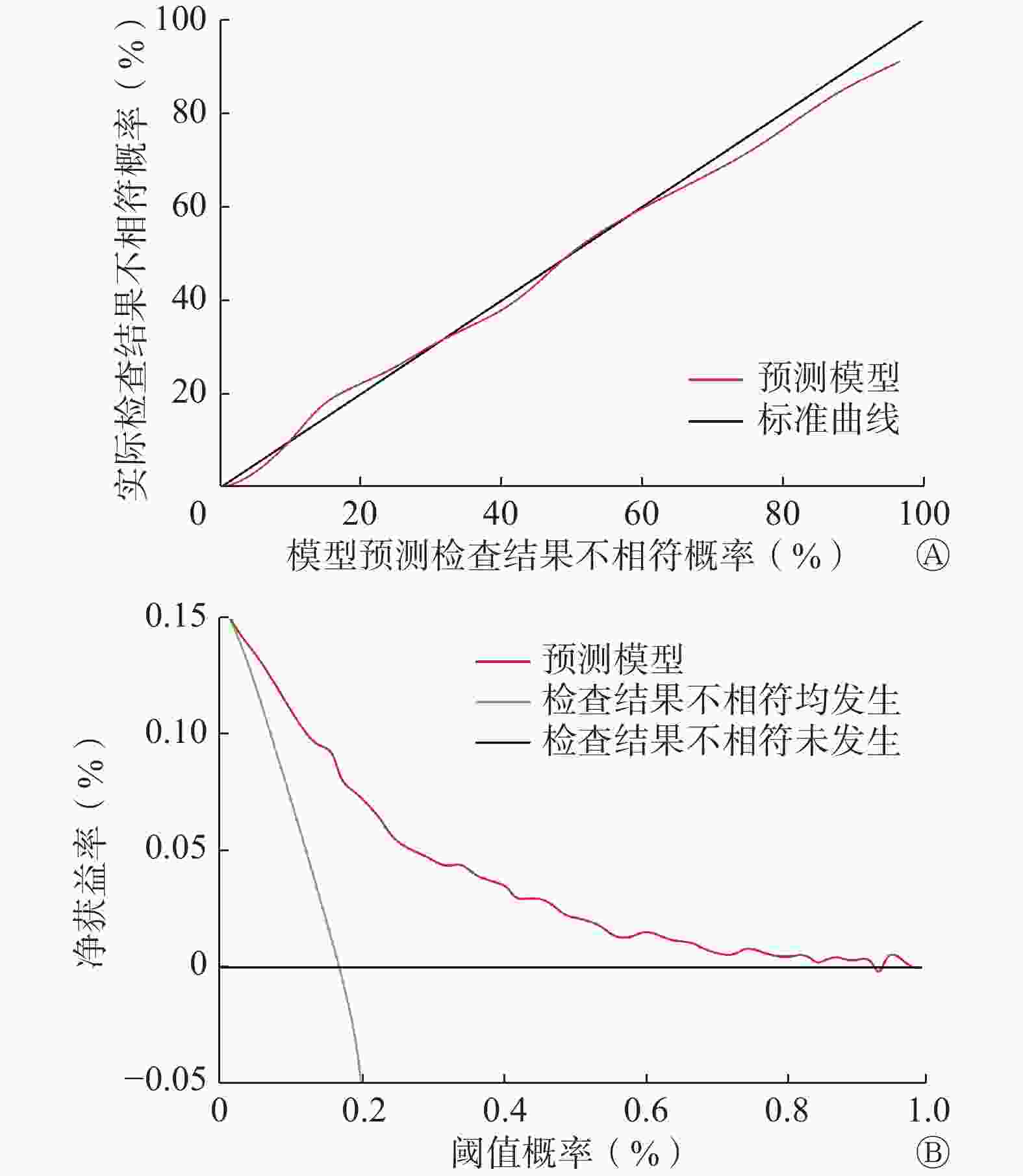
Figure 3. The calibration diagram (A) and decision curves analysis diagram (B) of the risk prediction model for the inconsistency between the results of the two systems in the model prediction
-
据统计,在一般人群中TN的发病概率为4%~8%,且多数患者经手术组织病理学诊断后已是中晚期[11]。目前,TN的诊断方法有多种,包括触诊、超声影像学、FNA或手术组织病理学检查等。其中触诊虽简单、方便,但结果主观;FNA虽创伤小,特异度和灵敏度高,但穿刺失败风险较高,尤其是对于小或微小结节以及多发结节;而手术组织病理学是通过手术切除病变组织,风险较高,对机体功能损害大并有伴多种并发症的可能[12]。在我国TN的超声诊断方法中应用最广泛的是ACR-TIRADS,而EU-TIRADS较少,相关研究结果表明,这2种分类系统对良恶性TN的诊断效能均较高[13]。
在本研究中,TN恶性风险随着ACR-TIRADS和EU-TIRADS分类类别升高而增加。ACR-TIRADS 2~4类无论是良性还是恶性TN均与EU-TIRADS 2~4类一致性良好,而ACR-TIRADS 5类的TN中有63.51%(94/148)分布于EU-TIRADS 4类,有36.49%(54/148)分布于EU-TIRADS 5类。这可能是由于ACR-TIRADS采用得分制,以极低回声、高>宽、甲状腺外侵袭以及点状强回声的权重最大;而EU-TIRADS采用分层制,具备≥1个恶性特征的TN归入5类,导致二者5类恶性TN检查结果显著不一致。与ACR-TIRADS相比,EU-TIRADS的灵敏度(91.54%对 79.31%)较高、特异度(62.38%对75.67%)较低,这与Schenke等[14]和Shen等[15]的研究结果相符。
为进一步明确影响二者检查结果不相符的相关因素,本研究采用多因素Logistic回归预测模型进行分析,结果显示,结节长径<20 mm、海绵样结节、低和(或)中低回声、圆形、边缘模糊以及微分叶边缘,均是二者检查结果不相符的独立危险因素。原因可能为:(1)由于本研究中恶性TN占比较高53.75%(172/320),因此当结节长径≥20 mm时,超声表现出纵向生长及边缘侵犯等特征的概率较高,而2种系统对这些特征的灵敏度均较高,故二者一致性较好,具体情况还有待进一步研究。(2)海绵样结节是一种完全微囊结构,评估难度较大,需明确其是否为完全微囊结构,故二者一致性较差。(3)EU-TIRADS不会根据混合回声结节实性部分的主要回声进行判断,其中若有低回声,则判断为低和(或)中低回声,结节周边回声会影响回声判断,特别是在炎症反应背景下,故判断低和(或)中低回声具有一定主观性,以致二者检查结果不相符。(4)EU-TIRADS的分层依据为结节形状,对于低和(或)中危类,圆形无法归类,故二者一致性较差。(5)在等回声或不均匀回声背景下,如弥漫性甲状腺炎,判断边缘模糊的结节有较大主观性,导致二者检查结果不相符。(6)微分叶是指1个或以上光滑、圆形局部凸起,当凸起单一且不明显时,二者存在较大分歧。Logistic回归预测模型的评价结果显示,其准确度较高。
本研究为回顾性研究,存在一定的局限性,尽管规范检查且标准化采集图像,但在一定程度上,静态存图会影响各超声特征的评估,而实时动态评估更精确。
综上所述,EU-TIRADS较ACR-TIRADS对TN的灵敏度高、特异度低;二者对2~4类TN的检查结果一致性良好;结节长径<20 mm、海绵样结节、低和(或)中低回声、圆形、边缘模糊以及微分叶边缘,均是影响二者检查结果一致性的独立危险因素。
利益冲突 所有作者声明无利益冲突
作者贡献声明 贺然负责命题的提出、研究方法的设计、数据的统计与分析、论文的撰写;郝祥玉负责数据的获取、论文的审阅与修改;卢晓莉负责论文最终版本的修订
Analysis of consistency and difference between ACR-TIRADS and EU-TIRADS in the diagnosis of thyroid nodules
- Received Date: 2022-12-21
- Available Online: 2024-02-25
Abstract:
 DownLoad:
DownLoad: