



-
半月板撕裂是膝关节最常见的创伤类型之一,常表现为活动受限、运动疼痛,若不及时治疗,可继发慢性滑膜炎,加速关节退变[1]。由于膝关节解剖结构复杂,软组织较多,常规X线和CT检查对其缺乏特异性。MRI以其多方位、多平面的成像能力和对软组织分辨率高的特点,成为诊断半月板损伤首选的无创检查[2]。但在临床实践中,其诊断缺乏相关的标准,会出现假阳性与假阴性,尤其是膝板股韧带附着区的外侧半月板后角(posterior horn of the lateral meniscus,PHLM)撕裂,因其少见且具有一定隐匿性,往往容易漏诊。本研究回顾性分析了35例膝板股韧带附着区PHLM撕裂患者的MRI资料,并与非半月板撕裂及健康体检者的膝关节MRI资料进行比较,旨在找出膝板股韧带附着区PHLM撕裂的特异性征象,旨在提高MRI诊断和鉴别诊断的准确率。
-
选取2012年12月至2018年6月在南通市通州区中医院因膝外伤就诊的65例前交叉韧带(anterior cruciate ligaments,ACL)损伤患者为研究对象。将其中35例伴发膝板股韧带附着区PHLM撕裂的患者作为观察组,其余30例非PHLM撕裂患者作为对照A组,另选取同一时间段内在我院例行体检的30名健康者作为对照B组。观察组包括男性19例、女性16例,年龄25~67(44.52±10.11)岁;左膝15例、右膝20例。对照A组男性16例、女性14例,年龄23~68(43.09±9.83)岁;左膝13例、右膝17例。对照B组男性15例、女性15例,年龄20~65(43.87±9.48)岁;左膝14例、右膝16例。3组受试者在性别、年龄等基本情况方面的差异均无统计学意义(χ2= 0.128, F =0.171,均P>0.05)。
-
纳入标准:①观察组和对照A组患者均有膝关节创伤史,并伴有关节肿胀、疼痛、运动障碍等症状,经关节镜确诊,符合ACL损伤的国际诊断标准[3];②对照B组体检者既往无膝关节创伤史,无膝关节炎病史,无关节肿胀、疼痛、运动障碍等症状;③所有患者均于检查前签署了知情同意书。排除标准:①影像学资料不全;②无关节镜明确诊断者;③合并严重心脑血管疾病;④有严重精神类疾病史。
-
采用德国Siemens Avanto 1.5 T超导MRI成像仪行膝关节MRI检查,受检者取仰卧位,受检下肢呈屈曲15~30度。采用膝关节柔线圈,常规矢状面、冠状面和横断面扫描。矢状面序列包括自旋回波T1WI(重复时间425 ms,回波时间7.2 ms)、自旋回波脂肪抑制质子密度加权像(proton density weighted image,PDWI) (重复时间3000 ms,回波时间40 ms)、冠状面脂肪抑制自旋回波PDWI(重复时间3050 ms,回波时间31 ms)和横断面脂肪抑制自旋回波PDWI(重复时间3100 ms,回波时间47 ms)。扫描参数:层厚4.0 mm,层间隔1 mm,视野160~180 mm,矩阵320×320。
-
由2位具有5年以上MRI诊断经验的副主任医师以双盲法对图像进行独立解析,重点评价以下指标:①3组受试者的MRI表现及膝关节周围结构的损伤情况;②在矢状面图像上,对PHLM后部纵行线状高信号影连续显示的层数进行计数;③在横断面图像上,测量PHLM周缘部线状高信号影自内向外延伸的直线长度。如两位医师的判读结果不一致,则请第3位放射科专家再次共同阅片,经讨论确定最终结果。
-
采用SPSS 17.0统计软件对数据进行统计学分析。膝关节MRI征象发生率及其周围结构的损伤情况比较采用χ2检验。膝关节线状高信号影连续显示的层数和自内向外延伸的直线长度数据符合正态分布,以(
$\overline x $ ±s)形式表示,使用单因素方差分析或t检验。鉴别诊断PHLM真、假性撕裂的效能采用受试者工作特征(receiver operating characteristic,ROC)曲线进行分析。P<0.05表示差异有统计学意义。 -
对照A组:膝板股韧带附着区MRI征象(图1中A~C)与对照B组相似(图1中D~F)。83.33%25/30)的患者在MRI矢状位表现为板股韧带与PHLM间呈斜行或垂直线状高信号,23.33%(7/30)的患者在横断面上表现为PHLM后缘线状高信号。
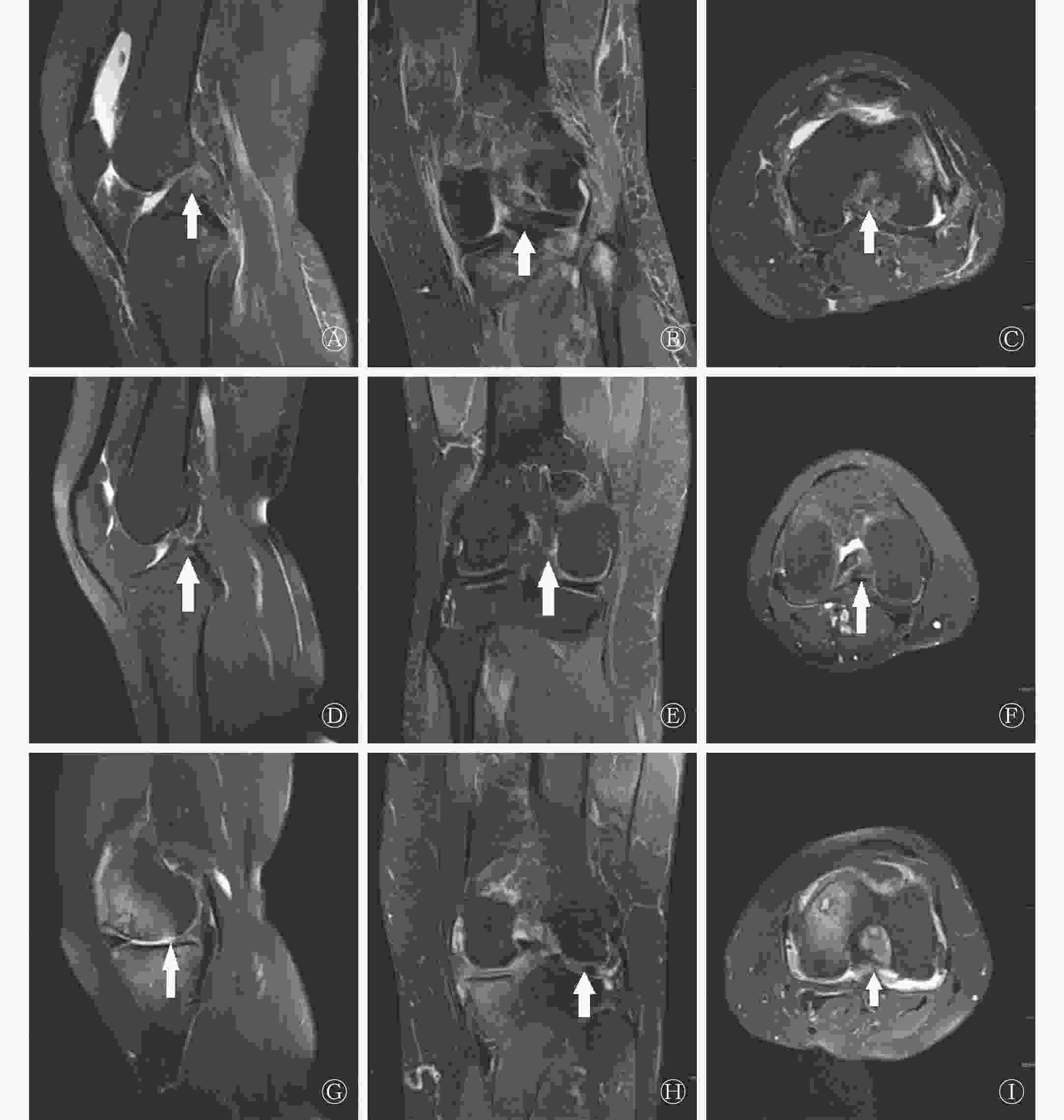
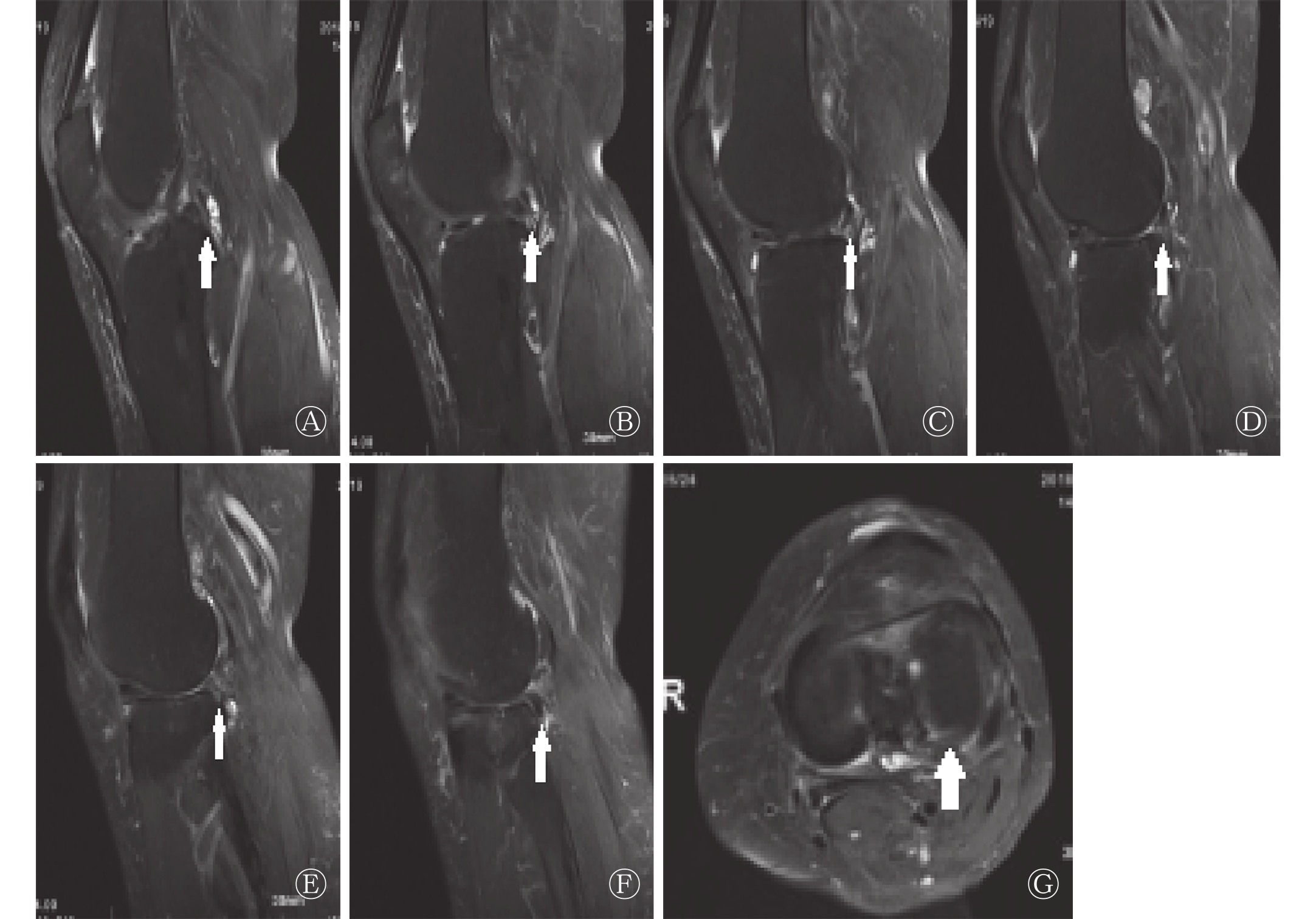
图 1 3例受检者膝板股韧带附着区的MRI图像
Figure 1. Comparison of MRI images of the attachment zone of the knee ligament ligament in the 3 patients
对照B组:76.67%(23/30)的受检者在MRI矢状位PDWI上表现为板股韧带与PHLM间呈斜行或垂直线状高信号(图1中D);冠状位PDWI上同一层面或相邻层面可清晰地观察到板股韧带位于PHLM后根部的后方(图1中E);横断面PDWI上,板股韧带起始部呈条状低信号,PHLM后根部呈条片状低信号,两者之间可见线形脂肪抑制PDWI高信号影,其中26.67%(8/30)的受试者表现为PHLM后缘线状高信号(图1中F)。对照A组与对照B组异常信号检出率的差异均无统计学意义(χ2=0.417、0.089,均P>0.05)(表1)。
组别 例数 矢状面上膝板股
韧带与PHLM间横断面上PHLM后缘 高信号 正常信号 高信号 正常信号 对照A组 30 25(83.33) 5(16.67) 7(23.33) 23(76.67) 对照B组 30 23(76.67) 7(23.33) 8(26.67) 22(73.33) χ2值 0.417 0.089 P值 0.519 0.766 注:表中,MRI:磁共振成像;PHLM:外侧半月板后角。 表 1 对照A组与对照B组膝板股韧带附着区MRI征象比 较[例(%)]
Table 1. Comparison of MRI appearances of plate ligament attachment area between control group A and control group B [case (%)]
观察组:94.29%(33/35)的患者在MRI矢状位PDWI上表现为PHLM周缘部纵向线状高信号(图1中G),连续出现3~8层,其中71.43%(25/35)的患者累及上、下关节面,22.86%(8/35)的患者累及一个关节面;另2例表现为板股韧带附着部PHLM连续性中断。68.57%(24/35)的患者在MRI冠状位PDWI上表现为板股韧带起始部斑片状信号增高及局部形态不规则(图1中H)。横断面PDWI上,91.43%(32/35)的患者表现为PHLM周缘部线状高信号(图1中I)。
-
由表2可见,观察组膝关节其他结构损伤的发生率与对照A组比较,差异均无统计学意义。
组别 例数 内侧半月
板损伤ACL完全断裂 后交叉韧
带损伤关节积液 外侧区间
骨挫伤观察组 35 19(54.29) 26(74.29) 4(11.43) 33(94.29) 16(45.71) 对照A组 30 18(60.00) 19(63.33) 2( 6.67) 29(96.67) 15(50.00) χ2值 0.215 0.910 0.054 0.019 0.119 P值 0.643 0.340 0.817 0.891 0.730 注:表中,ACL:前交叉韧带。 表 2 观察组和对照A组膝关节其他结构损伤情况比较[例(%)]
Table 2. Comparison of other structural injuries of knee joint between observation group and control group A [cases (%)]
-
观察组患者在MRI矢状面和横断面图像上均表现为明显的PHLM周缘部线状高信号,矢状面上可连续检出(5.75±1.38)层(称“连续线征”,见图2中A~F),横断面上自内向外延伸(15.06±5.02) mm(称“拉链征”,见图2中G),与对照A组、B组比较,差异均有统计学意义(F=43.231、36.113,均P<0.05)(表3)。
组别 例数 矢状面连续
检出的层数(层)横断面延伸的
直线长度(mm)观察组 35 5.75±1.38 15.06±5.02 对照A组 30 2.66±1.59 8.54±3.33 对照B组 30 2.81±1.62 7.28±3.17 F值 43.231 36.113 P值 0.000 0.000 注:表中,PHLM:外侧半月板后角。 表 3 3组受检者膝板股韧带附着区PHLM周缘线状高信号 的测量值比较(
$\scriptstyle \overline x $ Table 3. Comparison of measured values of linear high signal of PHLM in the knee ligament attachment zone of 3 groups of subjects (
$\scriptstyle \overline x $ 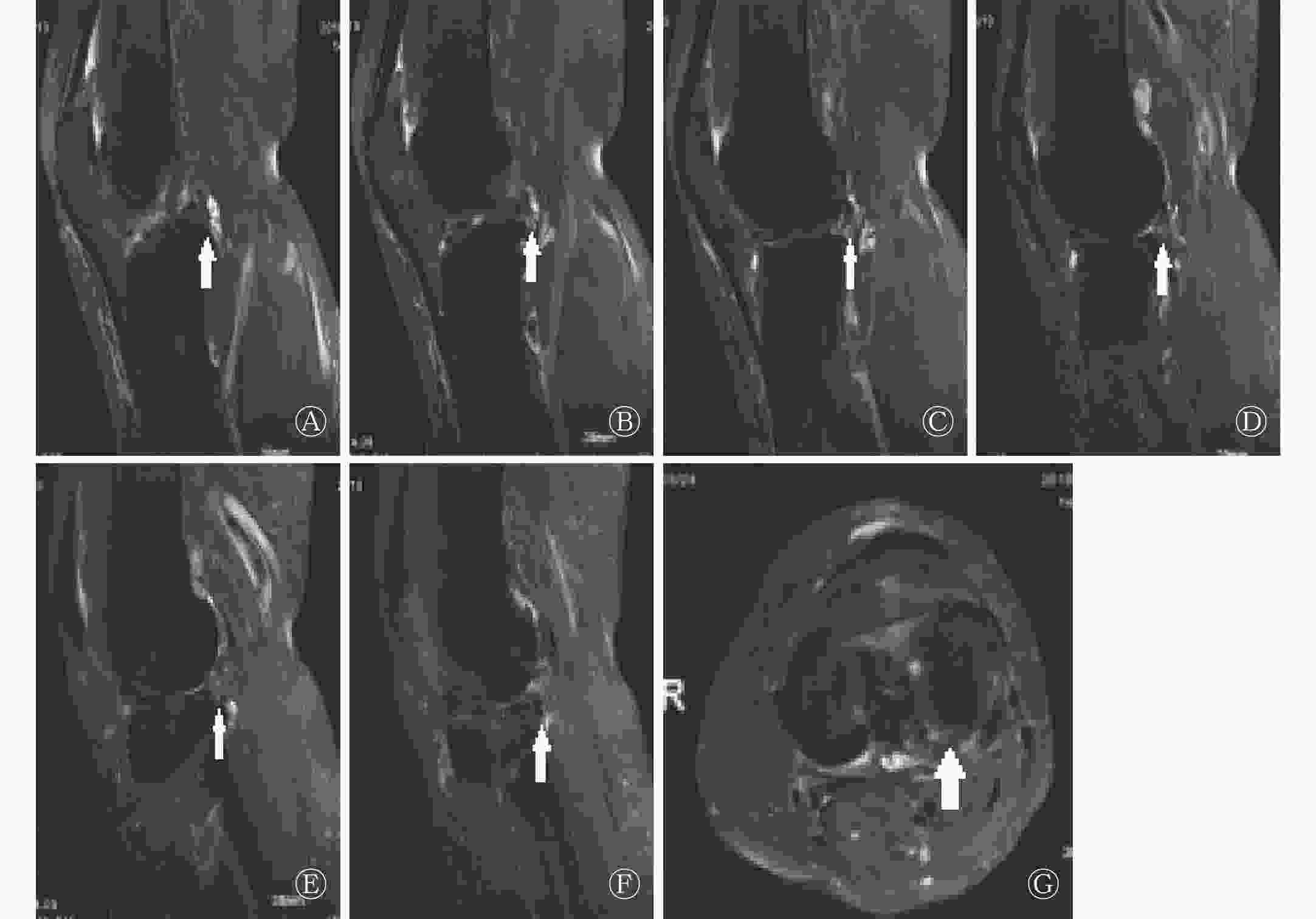
图 2 膝板股韧带附着区PHLM撕裂患者MRI图像
Figure 2. MRI images of patients with PHLM tear in the knee ligament attachment area
分别采用矢状面可连续检出线状高信号层数和横断面上线状高信号延伸的直线长度来鉴别PHLM真、假性撕裂,采用ROC曲线进行分析,曲线下面积分别为0.96和0.92(图3中A~B)。不同诊断标准鉴别PHLM撕裂的灵敏度、特异度和准确率见表4。
诊断标准 灵敏度 特异度 准确率 以≥5层为“连续线征”阳性 91.43%(32/35) 90.00%(54/60) 90.53%(86/95) 以≥10 mm为“拉链征”阳性 85.71%(30/35) 90.00%(54/60) 88.42%(84/95) 联合应用“连续线征”和“拉链征”为阳性 85.71%(30/35) 95.00%(57/60) 91.58%(87/95) 注:表中,PHLM:外侧半月板后角。 表 4 不同诊断标准鉴别PHLM撕裂的灵敏度、特异度和准确率的比较
Table 4. Comparison of sensitivity, specificity and accuracy of different diagnostic criteria for identifying PHLM tears
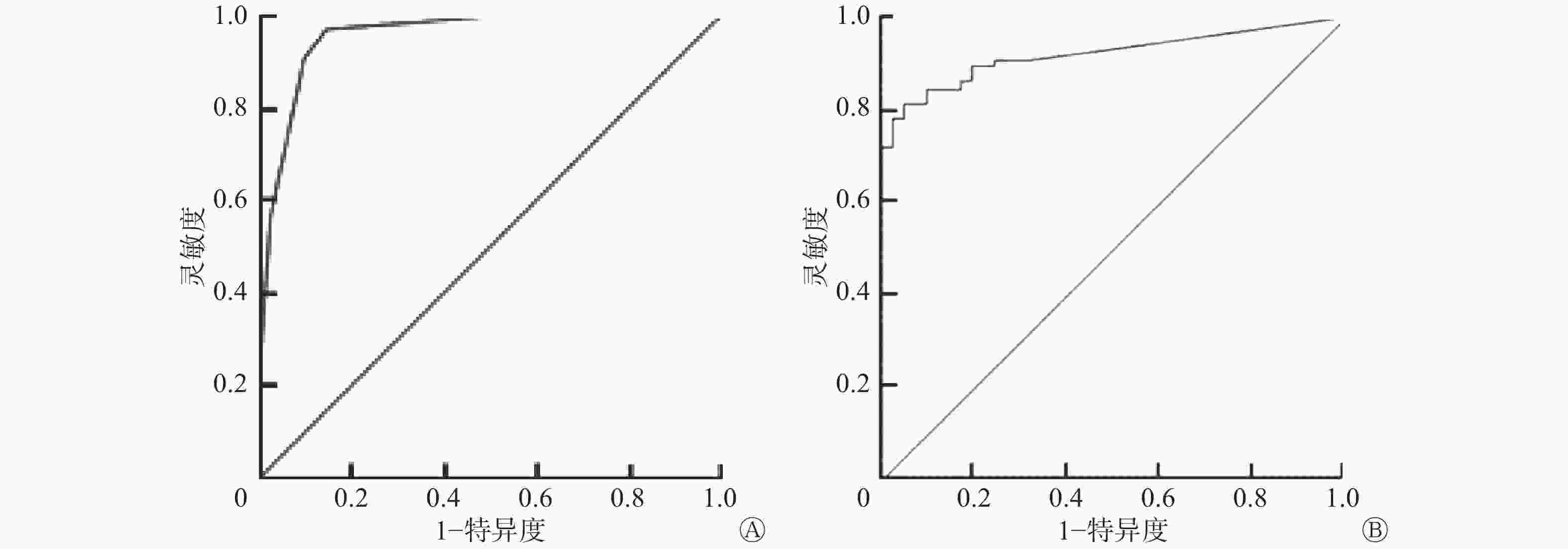
图 3 鉴别PHLM真、假性撕裂的ROC曲线
Figure 3. ROC curve for distinguishing true and false tearing of PHLM
-
PHLM撕裂是临床较为少见的运动创伤,尚缺乏特异性的诊断标准,容易造成误诊或漏诊,从而延误最佳的治疗时间,进一步影响膝关节的稳定,造成关节软骨和关节腔室的继发病变[4-5]。因此,早期、准确地诊断PHLM撕裂对临床治疗方案的选择和后期康复有着重要的临床意义。膝关节镜是目前临床公认的诊断半月板损伤的较准确方法[6],但由于其为有创性检查,且存在一定并发症,患者难以接受,因此不宜作为常规检查手段。X线和CT对关节内软骨和软组织损伤的诊断能力有限[7-8]。MRI以其多方位、多平面的成像能力和对软组织分辨率高的特点,成为诊断半月板损伤最理想的检查方式。
-
膝关节半月板为纤维软骨组织,不含氢质子,因此在MRI各序列上均呈均匀低信号。当半月板发生撕裂时,周围关节液渗入损伤区域,使该区域的氢质子浓度增加,表现为异常高信号。在膝板股韧带附着区,板股韧带自PHLM内缘斜向后上走行,与PHLM之间存在一个恒定间隙,该间隙在MRI上显示为纵行线状异常高信号,容易被误判为PHLM撕裂,但其实质是板股韧带与PHLM之间的固有裂隙被脂肪或液体所填充,在MRI上表现为异常高信号[9-10]。本研究对对照A组患者和对照B组受试者在MRI矢状面和横断面上检出的纵行线状高信号的发生率进行了比较,差异均无统计学意义,这说明此征象是固有解剖间隙所致,并非PHLM撕裂征象。另外,本研究结果发现,PHLM撕裂多伴有交叉韧带损伤、骨挫伤、关节积液等周围结构病变,将观察组与对照组A组比较,结果显示观察组膝关节其他结构损伤的发生率与对照A组比较,差异均无统计学意义,这提示这些损伤与PHLM撕裂无关联。
膝板股韧带附着区PHLM撕裂的病理本质是ACL损伤导致胫骨及半月板根部前移,板股韧带及半月板附着点相对后移,二者综合作用力如解开拉链般钝性撕开,被法国学者Savoye等[11]称为“拉链样”损伤。MRI矢状面图像显示PHLM周缘部纵行线状高信号影自内向外延伸,自后交叉韧带消失层面开始连续计数,可显示多层,并可累及关节面,称之为“连续线征”。PHLM撕裂在横断面上可显示其“拉链样”整体形态,自膝板股韧带附着区向外延伸,PHLM周缘部呈线状高信号影,称之为“拉链征”。
-
膝板股韧带附着区PHLM撕裂最典型的MRI表现为矢状位图像上PHLM周缘部纵向线状高信号,多数累及关节面;冠状位表现为板股韧带起始部斑片状信号增高及局部形态不规则;横断面表现为PHLM周缘部线状高信号。基于上述典型表现,有学者提出将矢状面或横断面异常信号的走行作为鉴别PHLM真、假性撕裂的要点[12],但由于板股韧带附着区解剖结构复杂,假阳性率较高[13]。我们认为PHLM真、假性撕裂的鉴别不单要看异常信号的形态,其长度的差异也很重要。在本研究中,我们分别测量了矢状面可连续检出线状高信号的层数和横断面上线状高信号延伸的直线长度,结果显示观察组患者在矢状面上可连续检出(5.75±1.38)层,横断面上自内向外延伸(15.06±5.02) mm,高于对照A组、B组,且差异有统计学意义。采用ROC曲线分析,以≥5层作为“连续线征”的阳性标准,以≥10 mm作为“拉链征”的阳性标准,联合应用上述2个标准,特异度可达95.00%,准确率可达91.58%,大大提升了诊断效能。
综上所述,膝板股韧带附着区PHLM撕裂在MRI上有明显的征象,辅以“连续线征”和“拉链征”进行鉴别诊断,可显著提升诊断的特异度和准确率。
利益冲突 本研究由署名作者按以下贡献声明独立开展,不涉及任何利益冲突。
作者贡献声明 庄向东负责研究过程的实施、数据的获取与分析,论文的起草及最终版本修订;王小乐负责研究命题的提出和设计。
膝板股韧带附着区外侧半月板后角撕裂的MRI表现及诊断价值
MRI appearance and diagnostic value of the posterior horn of the lateral meniscus tear of the knee ligament attachment zone
-
摘要:
目的 探讨膝板股韧带附着区外侧半月板后角(PHLM)撕裂的MRI表现及鉴别诊断价值。 方法 选取2012年12月至2018年6月因前交叉韧带(ACL)损伤在南通市通州区中医院就诊的35例膝板股韧带附着区PHLM撕裂患者作为观察组,搜集同期30例ACL损伤但非PHLM撕裂患者作为对照A组,另选取同期例行体检的30名健康者作为对照B组。3组受试者均行膝关节MRI检查,观察3组受试者的MRI表现。分别应用χ 2检验、单因素方差分析和t检验分析膝关节MRI征象的发生率、膝关节周围结构的损伤情况及膝关节线状高信号影显示的层数和长度,并采用受试者工作特征(ROC)曲线分析鉴别诊断PHLM真、假性撕裂的效能。 结果 观察组患者在MRI矢状面和横断面图像上均表现为明显的PHLM周缘部线状高信号,矢状面上可连续检出(5.75±1.38)层(称“连续线征”),横断面上自内向外延伸(15.06±5.02)mm(称“拉链征”),与对照A组、B组比较差异均有统计学意义(F=43.231、36.113,均P<0.05)。以“连续线征”和“拉链征”作为阳性标准,MRI诊断膝板股韧带附着区PHLM撕裂的灵敏度为85.71%、特异度为95.00%、准确率为91.58%。 结论 膝板股韧带附着区PHLM撕裂在MRI上有明显的征象,辅以“连续线征”和“拉链征”进行鉴别诊断,可明显提升诊断效果。 Abstract:Objective This study aims to investigate the MRI appearance and diagnostic value of the posterior horn of the lateral meniscus (PHLM) tear of the knee ligament attachment zone. Methods From December 2012 to June 2018, 35 patients with anterior cruciate ligament (ACL) injury combined with PHLM tear in the knee ligament attachment zone were selected as the observation group. Thirty patients with ACL injury but without PHLM tears were collected as the control group A. Another 30 healthy people who received routine physical examination were selected as the control group B. All subjects received knee MRI examination. The MRI performance of all subjects in the three groups was observed. χ2 test, one-way ANOVA, and t-test were used to calculate the incidence of knee MRI signs, the damage of the structure around the knee joint, and the number and length of the linear high-signal images of the knee joint. The receiver operating characteristic curve was used to analyze the effectiveness of differential diagnosis of true and false tear in PHLM. Results Patients in the observation group showed significant linear hyperintense on the MRI sagittal plane and cross-sectional images. The sagittal plane was continuously detected (5.75±1.38) layers (called "continuous line sign"), extending from the inside to the outside (15.06 ± 5.02) mm (called "zipper sign"). The number of layers on the sagittal plane and the length of the transverse section in the observation group were higher than those in the control groups A and B ( F =43.231, 36.113, both P < 0.05). Combined with "continuous line sign" and "zipper sign" as the positive criteria, the sensitivity was 85.71%, the specificity was 95%, and the accuracy was 91.58%. Conclusion The PHLM tear in the knee ligament attachment zone had obvious signs on MRI, supplemented by "continuous line sign" and "zipper sign" for differential diagnosis, which could significantly improve the diagnostic effect. -
图 1 3例受检者膝板股韧带附着区的MRI图像
Figure 1. Comparison of MRI images of the attachment zone of the knee ligament ligament in the 3 patients
图 2 膝板股韧带附着区PHLM撕裂患者MRI图像
Figure 2. MRI images of patients with PHLM tear in the knee ligament attachment area
图 3 鉴别PHLM真、假性撕裂的ROC曲线
Figure 3. ROC curve for distinguishing true and false tearing of PHLM
表 1 对照A组与对照B组膝板股韧带附着区MRI征象比 较[例(%)]
Table 1. Comparison of MRI appearances of plate ligament attachment area between control group A and control group B [case (%)]
组别 例数 矢状面上膝板股
韧带与PHLM间横断面上PHLM后缘 高信号 正常信号 高信号 正常信号 对照A组 30 25(83.33) 5(16.67) 7(23.33) 23(76.67) 对照B组 30 23(76.67) 7(23.33) 8(26.67) 22(73.33) χ2值 0.417 0.089 P值 0.519 0.766 注:表中,MRI:磁共振成像;PHLM:外侧半月板后角。  下载: 导出CSV
下载: 导出CSV
表 2 观察组和对照A组膝关节其他结构损伤情况比较[例(%)]
Table 2. Comparison of other structural injuries of knee joint between observation group and control group A [cases (%)]
组别 例数 内侧半月
板损伤ACL完全断裂 后交叉韧
带损伤关节积液 外侧区间
骨挫伤观察组 35 19(54.29) 26(74.29) 4(11.43) 33(94.29) 16(45.71) 对照A组 30 18(60.00) 19(63.33) 2( 6.67) 29(96.67) 15(50.00) χ2值 0.215 0.910 0.054 0.019 0.119 P值 0.643 0.340 0.817 0.891 0.730 注:表中,ACL:前交叉韧带。
下载: 导出CSV
表 3 3组受检者膝板股韧带附着区PHLM周缘线状高信号 的测量值比较(
$\scriptstyle \overline x $ Table 3. Comparison of measured values of linear high signal of PHLM in the knee ligament attachment zone of 3 groups of subjects (
$\scriptstyle \overline x $ 组别 例数 矢状面连续
检出的层数(层)横断面延伸的
直线长度(mm)观察组 35 5.75±1.38 15.06±5.02 对照A组 30 2.66±1.59 8.54±3.33 对照B组 30 2.81±1.62 7.28±3.17 F值 43.231 36.113 P值 0.000 0.000 注:表中,PHLM:外侧半月板后角。
下载: 导出CSV
表 4 不同诊断标准鉴别PHLM撕裂的灵敏度、特异度和准确率的比较
Table 4. Comparison of sensitivity, specificity and accuracy of different diagnostic criteria for identifying PHLM tears
诊断标准 灵敏度 特异度 准确率 以≥5层为“连续线征”阳性 91.43%(32/35) 90.00%(54/60) 90.53%(86/95) 以≥10 mm为“拉链征”阳性 85.71%(30/35) 90.00%(54/60) 88.42%(84/95) 联合应用“连续线征”和“拉链征”为阳性 85.71%(30/35) 95.00%(57/60) 91.58%(87/95) 注:表中,PHLM:外侧半月板后角。
下载: 导出CSV
-
[1] 欧阳红斌, 李朝晖, 赖永娥, 等. 膝关节半月板损伤磁共振成像诊断与关节镜检查对比研究[J]. 现代医用影像学, 2017, 26(2): 298−299, 323.
Ouyang HB, Li ZH, Lai YE, et al. Comparative study of magnetic resonance imaging diagnosis and arthroscopic examination of knee meniscus injury[J]. Modern Med Imagel, 2017, 26(2): 298−299, 323.[2] Hare HB, Lohmander LS, Kise NJ, et al. Middle-aged patients with an MRI-verified medial meniscal tear report symptoms commonly associated with knee osteoarthritis[J]. Acta Orthop, 2017, 88(6): 664−669. DOI: 10.1080/17453674.2017.1360985. [3] Ruiz ME, Erickson SJ. Medial and lateral supporting structures of the knee. Normal MR imaging anatomy and pathologic findings[J]. Magn Reson Imaging Clin N Am, 1994, 2(3): 381−399. [4] 刘艳玲, 武淮昌, 张东臣, 等. 非膝关节半月板撕裂16例的磁共振成像误诊分析[J]. 实用医学影像杂志, 2016, 17(6): 507−509. DOI: 10.16106/j.cnki.cn14−1281/r.2016.06.016.
Liu YL, Wu HC, Zhang DC, et al. MRI misdiagnosis analysis of 16 cases with non knee joint meniscus tear[J]. J Pract Med Imaging, 2016, 17(6): 507−509. DOI: 10.16106/j.cnki.cn14−1281/r.2016.06.016.[5] Furumatsu T, Kodama Y, Kamatsuki Y, et al. Meniscal extrusion progresses shortly after the medial meniscus posterior root tear[J]. Knee Surg Relat Res, 2017, 29(4): 295−301. DOI: 10.5792/ksrr.17.027. [6] 庞博, 龚金山. MR与关节镜诊断半月板损伤的临床价值研究[J]. 医学影像学杂志, 2017, 27(9): 1782−1784, 1792.
Pang B, Gong JS. Comparative study of magnetic resonance imaging and knee arthroscopy in the diagnosis of meniscus injury[J]. J Med Imaging, 2017, 27(9): 1782−1784, 1792.[7] 薛婷. CT与MRI影像学诊断膝关节损伤的临床分析[J]. 中国医药指南, 2018, 16(13): 149−150. DOI: 10.15912/j.cnki.gocm.2018.13.110.
Xue T. Clinical analysis of CT and MRI imaging in the diagnosis of knee joint injury[J]. Guide China Med, 2018, 16(13): 149−150. DOI: 10.15912/j.cnki.gocm.2018.13.110.[8] Beaufils P, Becker R, Kopf S, et al. The knee meniscus: management of traumatic tears and degenerative lesions[J/OL]. EFORT Open Rev, 2017, 2(5): 195−203[2018-09-08]. https://www.ncbi.nlm.nih.gov/pubmed/28698804. DOI: 10.1302/2058-5241.2.160056. [9] Kruger N, McNally E, Al-Ali S, et al. Three-dimensional reconstructed magnetic resonance scans: accuracy in identifying and defining knee meniscal tears[J/OL]. World J Orthop, 2016, 7(11): 731−737[2018-09-08]. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5112342/. DOI: 10.5312/wjo.v7.i11.731. [10] 黄耀渠, 赵晓梅, 伍琼慧, 等. 膝板股韧带附着区半月板真、假性撕裂的MRI表现及鉴别诊断[J]. 中华放射学杂志, 2016, 50(4): 269−273. DOI: 10.3760/cma.j.issn.1005−1201.2016.04.008.
Huang YQ, Zhao XM, Wu QH, et al. MRI features and differential diagnosis of real and pseudo-tears of lateral meniscus at the insertion site of meniscofemoral ligament[J]. Chin J Radiol, 2016, 50(4): 269−273. DOI: 10.3760/cma.j.issn.1005−1201.2016.04.008.[11] Savoye PY, Ravey JN, Dubois C, et al. Magnetic resonance diagnosis of posterior horn tears of the lateral meniscus using a thin axial plane: the zip sign-a preliminary study[J]. Eur Radiol, 2011, 21(1): 1511−1519. DOI: 10.1007/s00330−010−1882−8. [12] 闫新成, 郭苏晋, 杨广夫, 等. 膝关节板股韧带MRI分析[J]. 实用放射学杂志, 2011, 27(9): 1404−1406. DOI: 10.3969/j.issn.1002−1671.2011.09.030.
Yan XC, Guo SJ, Yang GF, et al. MRI analysis of the meniscofemoral ligament of the knee[J]. J Pract Radiol, 2011, 27(9): 1404−1406. DOI: 10.3969/j.issn.1002−1671.2011.09.030.[13] 王蓼, 江凯, 成科, 等. 膝关节外侧半月板假撕裂MRI征象分析及临床意义[J]. 中国骨伤, 2015, 28(7): 669−672. DOI: 10.3969/j.issn.1003−0034.2015.07.021.
Wang L, Jiang K, Cheng K, et al. MRI ainalysis of the pseudo-tears of the lateral meniscus of the knee and its clinical significance[J]. China J Orthop Trauma, 2015, 28(7): 669−672. DOI: 10.3969/j.issn.1003−0034.2015.07.021. -

 点击查看大图
点击查看大图

计量
- 文章访问数: 3731
- HTML全文浏览量: 3330
- PDF下载量: 7
