


-
甲状旁腺功能亢进症(hyperparathyroidism,HPT)是由于甲状旁腺分泌甲状旁腺激素(parathyroid hormone,PTH)过多继发钙磷代谢紊乱,累及多个器官和系统的一种常见内分泌疾病。血清PTH水平明显升高是诊断HPT的主要依据,影像学定位及定性诊断一般在其基础上进行。99Tcm-MIBI双时相平面显像扫描野大,操作简单,是传统的HPT影像学检查方法[1],但单纯的核素平面显像无法进行精准的解剖定位,而SPECT/CT能够实现功能图像和解剖图像的同机融合,为鉴定病灶来源和检出小病灶提供了帮助,降低了对HPT的误诊率和漏诊率,明显提高了对甲状旁腺病灶的定位以及定性的诊断效能[2]。所以,99Tcm-MIBI SPECT/CT断层融合显像已成为目前HPT术前最主要的影像学检查手段之一。目前有关HPT病灶重量对核素显像影响的研究较少,本研究通过回顾性分析22例HPT患者的99Tcm-MIBI双时相平面显像和99Tcm-MIBI SPECT/CT早期断层融合显像资料,探讨甲状旁腺病灶重量对两种显像方法诊断灵敏度的影响。
-
收集2017年2月至2018年10月在昆山市第一人民医院临床诊断为HPT并经手术病理学确诊的患者22例(原发性HPT患者9例、继发性HPT患者13例),其中男性9例、女性13例,年龄28~73(50.77±8.79)岁。所有患者均于术前一个月内接受血清PTH水平检测,并行99Tcm-MIBI双时相平面显像及99Tcm-MIBI SPECT/CT早期断层融合显像。所有患者均于检查前签署了甲状旁腺核素检查知情同意书。
纳入标准:①均经病理学结果证实;②血清PTH水平明显升高,伴或不伴血钙升高;③HPT手术治疗后血清PTH及血钙恢复至正常水平,半年后PTH水平再次明显升高。排除标准:①血清PTH水平未见明显增高,超声检查甲状旁腺区未见明显异常回声;②血清PTH水平一过性增高,未经临床治疗,一个月后复查血清PTH水平正常者。
-
使用德国SIEMENS公司Symbia T2 SPECT/CT扫描仪,显像剂为99Tcm-MIBI,由上海欣科医药有限公司苏州分公司提供,放射性化学纯度>95%。
-
①患者准备。静脉注射740 MBq的99Tcm-MIBI显像剂,15~30 min后行早期正面平面显像,平面扫描结束后在同一扫描野立即行SPECT断层采集,并行常规CT平扫,显像完成后进行图像重建以及CT衰减校正,并对SPECT断层图像和CT平扫图像进行同机融合。2 h后行延迟正面平面显像。扫描野均为颈部至胸骨柄体交界处。②显像参数。平面(静态)采集参数:低能高分辨率准直器,矩阵256×256,图像模拟放大倍数为2.6,总采集时间5 min。SPECT采集参数:双探头配置180°,探头旋转180°,非圆轨道步进采集,每帧20 s,帧数32,矩阵128×128。CT扫描参数:管电压120 kV,管电流160 mAs,层厚3 mm,层间距5 mm。
-
图像由两位核医学主治以上职称医师对双时相平面显像和SPECT/CT早期断层融合图像进行独立诊断分析,诊断出现分歧时,经第3位副主任医师判读,三者相互讨论获得一致性结果。
双时相平面显像诊断标准[1]:延迟相平面显像在甲状旁腺区域或纵隔区可见明显放射性浓聚,判断为阳性。早期平面显像病灶呈现浓聚状态,而延迟显像阴性者,判断为平面显像病灶存在早期快速洗脱。99Tcm-MIBI SPECT/CT早期断层融合显像诊断标准:在SPECT图像放射性浓聚灶对应的位置,CT图像可见结节状软组织密度影,判断为阳性。
按病灶重量将所有病灶分为两组,A组:病灶重量≤1.00 g,B组:病灶重量>1.00 g。
-
手术标本通过肉眼和石蜡切片(苏木精-伊红染色)镜下观察,并结合免疫组化(链霉菌抗生物素蛋白-过氧化物酶连结法)进行确诊,功能亢进的甲状旁腺组织(包括腺瘤、腺癌及增生)为真阳性;正常的甲状旁腺组织为真阴性;非甲状旁腺病变为假阳性;手术病理学结果证实为功能亢进的甲状旁腺组织但99Tcm-MIBI显像无阳性发现为假阴性。
-
采用SPSSl7.0软件进行统计学分析。符合正态分布的计量资料以均值±标准差(
${\bar x} \pm {{s}}$ )表示。对不同甲状旁腺病灶重量组别间各显像方法的灵敏度及不同组别间的早期洗脱率采用χ2检验(理论频数<5时,采用Fisher's检验);在方差齐的情况下,对两种显像方法的阳性病灶横截面最大径平均值的比较采用t检验。P<0.05为差异有统计学意义。 -
22例患者共切除58个病变甲状旁腺组织,以术后病理学结果作为“金标准”,共检出49个真阳性病灶,其中3个病理学诊断结果为腺瘤伴不典型增生、7个为良性腺瘤、39个为增生。3个假阳性病灶为甲状腺结节,6个真阴性病灶为正常甲状旁腺组织。另外,术中还发现,全部病理学诊断结果为阳性的患者中有4例同时伴甲状腺内病变(3例为结节性甲状腺肿、1例为结节性甲状腺肿伴囊性变)。99Tcm-MIBI双时相平面显像和99Tcm-MIBI SPECT/CT早期断层融合显像诊断结果为真阳性、假阴性、假阳性、真阴性的病灶数分别为32、16、4、6和41、9、2、6。
-
切除的58个甲状旁腺病灶的重量为0.09~9.78(1.54±1.33)g。其中A组共有病灶30个,B组共有病灶28个。99Tcm-MIBI双时相平面显像对A、B两组的诊断灵敏度分别为47.83%和84.00%,差异有统计学意义(χ2=7.05,P=0.008);99Tcm-MIBI SPECT/CT早期断层融合显像对A、B两组的诊断灵敏度分别为78.26%和85.19%,差异无统计学意义(χ2=0.40,P=0.525)。99Tcm-MIBI SPECT/CT早期断层融合显像对A组的诊断灵敏度高于99Tcm-MIBI双时相平面显像,差异有统计学意义(χ2=4.57,P=0.033)。99Tcm-MIBI SPECT/CT早期断层融合显像对B组的诊断灵敏度高于99Tcm-MIBI双时相平面显像,但差异无统计学意义(χ2=0.01,P=0.906)。具体数据见表1。典型病例的99Tcm-MIBI双时相平面显像及99Tcm-MIBI SPECT/CT早期断层融合显像图像分别见图1和图2。
组别 灵敏度 特异度 准确率 显像1 A组 47.83%(11/23) 85.71%(6/7) 56.67%(17/30) B组 84.00%(21/25) − (0/3) 75.00%(21/28) 显像2 A组 78.26%(18/23) 85.71%(6/7) 80.00%(24/30) B组 85.19%(23/27) − (0/1) 82.14%(23/28) 注:表中,显像1:99Tcm-MIBI双时相平面显像;显像2:99Tcm-MIBI SPECT/CT早期断层融合显像;A组病灶重量≤1.00 g,B组病灶重量>1.00 g;−:无真阴性病灶。MIBI:甲氧基异丁基异腈;SPECT:单光子发射计算机体层摄影术;CT:计算机体层摄影术 表 1 两种显像方法在不同质量组中的灵敏度、特异度和 准确率比较
Table 1. Comparison of sensitivity, specificity and accuracy of two imaging methods in different weight groups
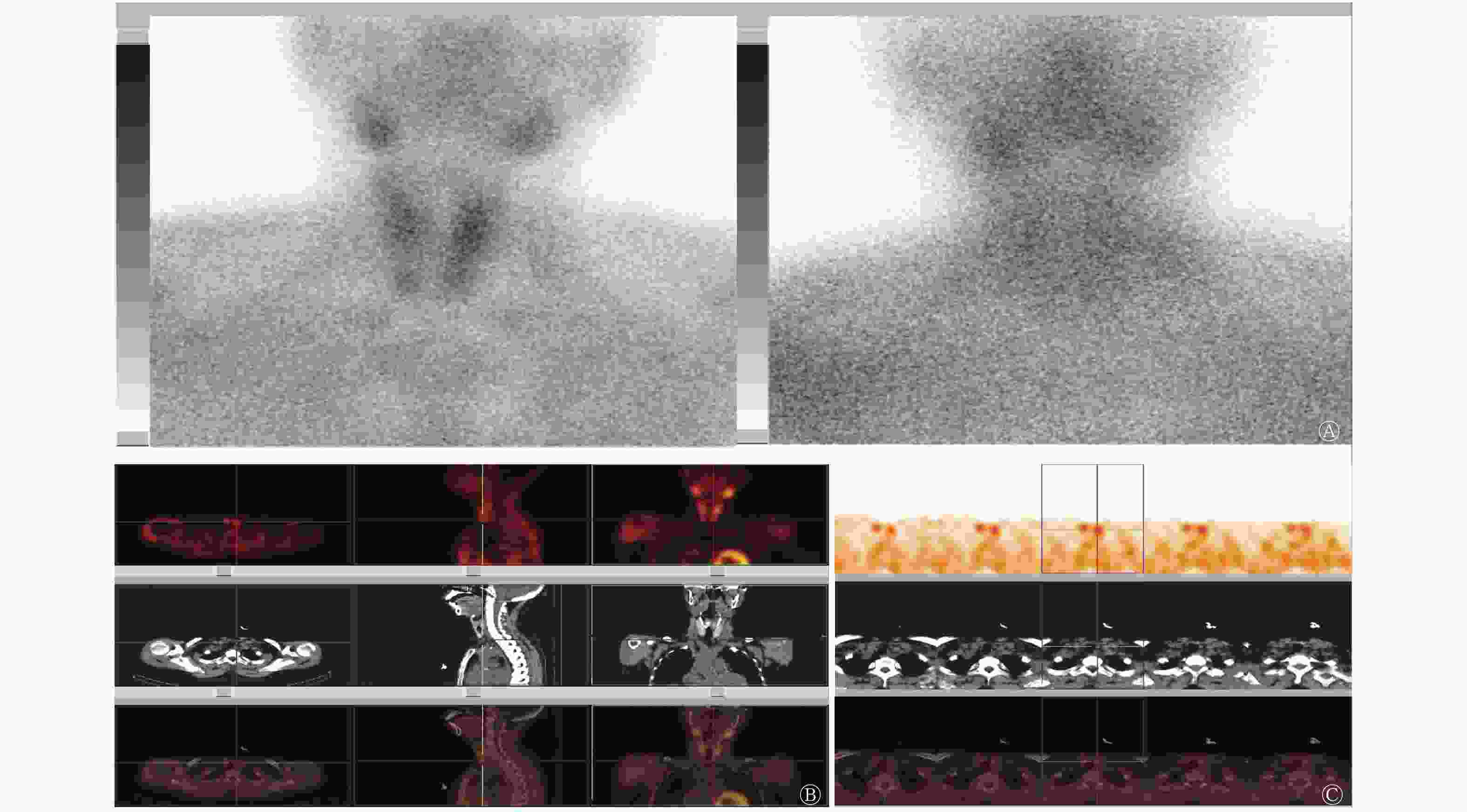
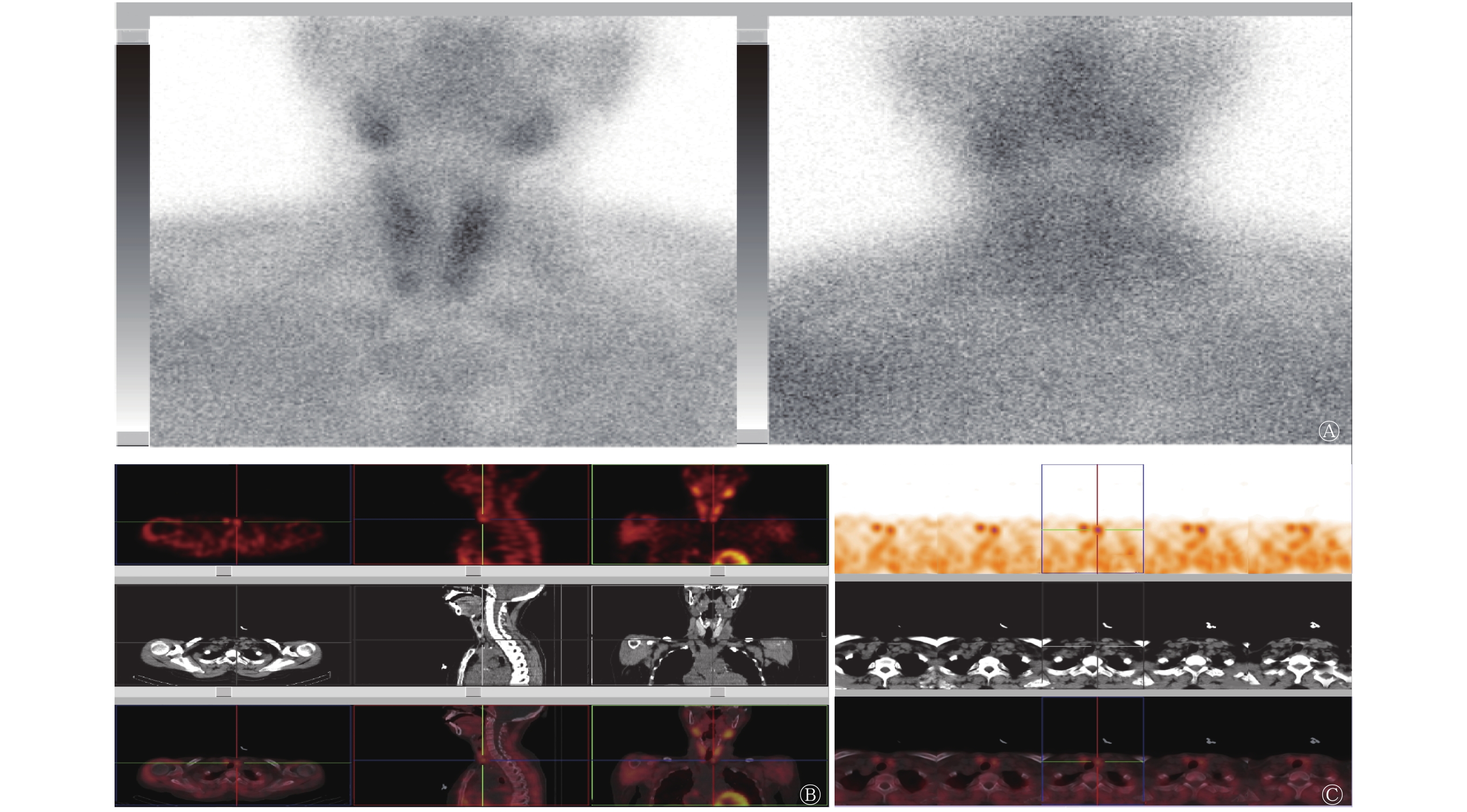
图 1 继发性甲状旁腺功能亢进症患者(女性,47岁)的99Tcm-MIBI双时相平面显像及SPECT/CT断层融合显像图
Figure 1. 99Tcm-MIBI dual-phase planar imaging and SPECT/CT fusion imaging of secondary hyperparathyroidism(female, 47 years old)
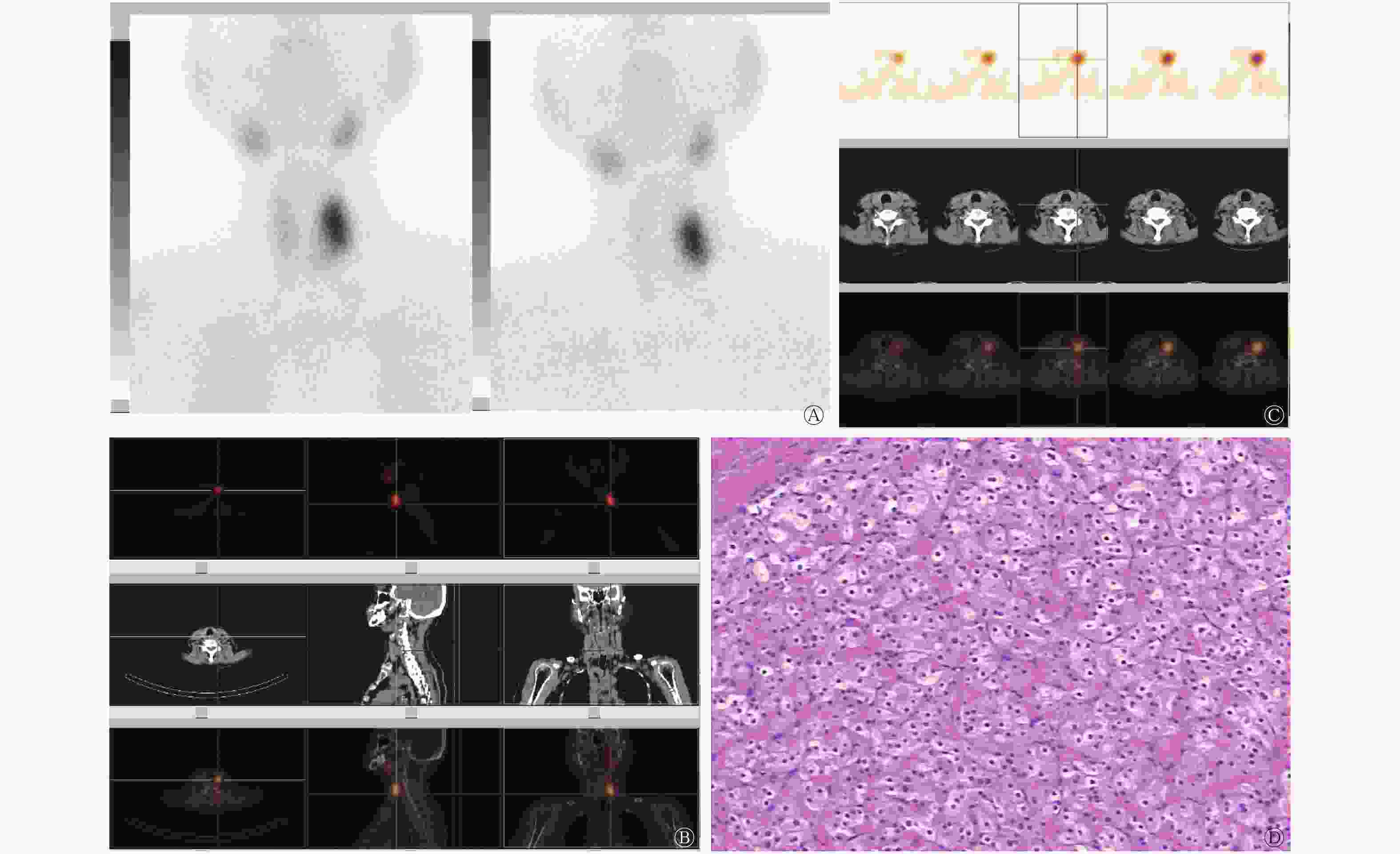
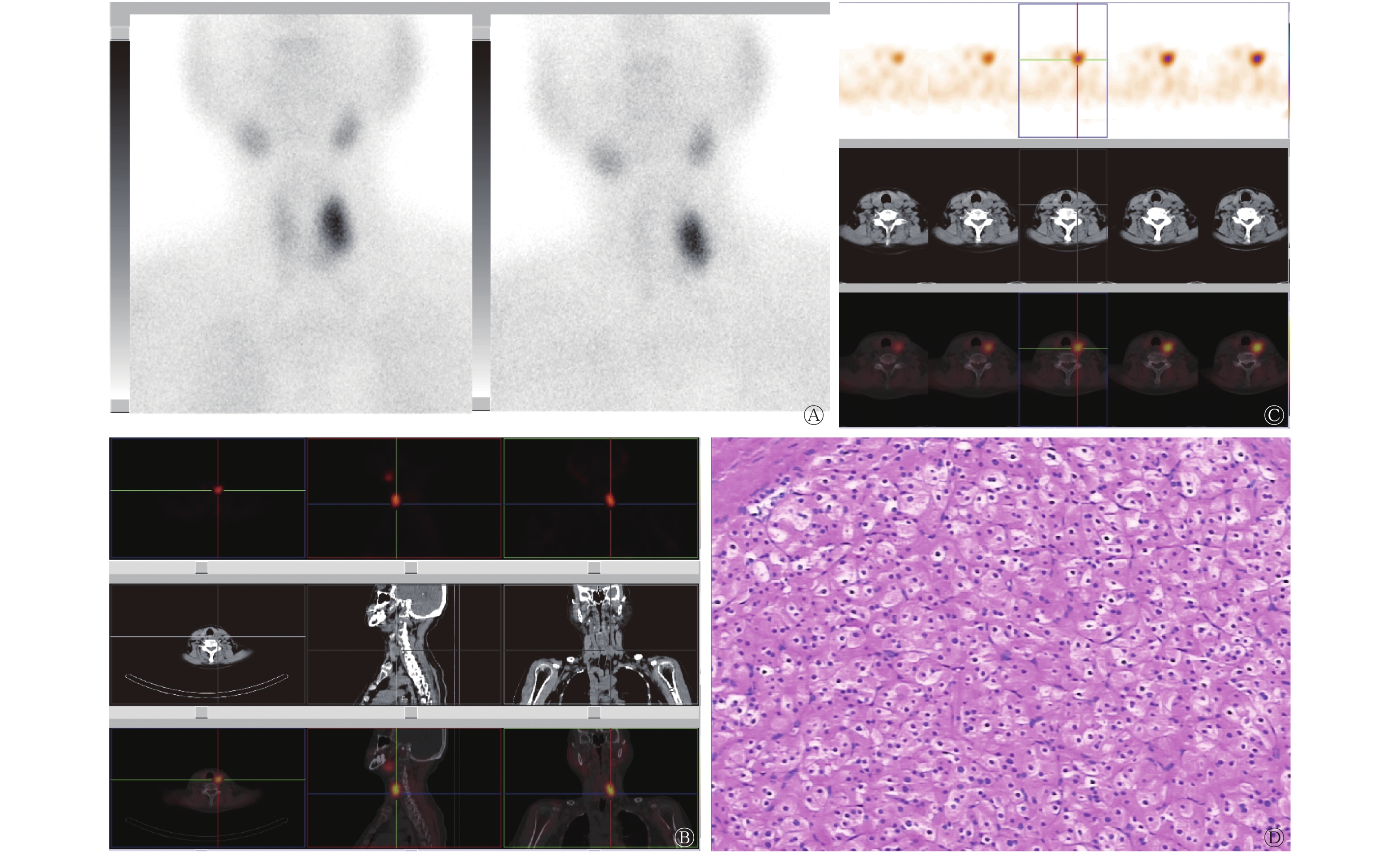
图 2 原发性甲状旁腺功能亢进症患者(女性,68岁)的99Tcm-MIBI双时相平面显像图、SPECT/CT断层融合显像图及病理图
Figure 2. 99Tcm-MIBI dual-phase planar imaging, SPECT/CT fusion imaging, ultrasound imaging and pathological section of primary hyperparathyroidism(female, 68 years old)
-
对99Tcm-MIBI双时相平面显像的放射性浓聚灶浓聚情况进行统计,结果发现,A组存在早期洗脱的病灶数为9个,早期洗脱率为30.00%(9/30),B组存在早期洗脱的病灶数为2个,早期洗脱率为7.14%(2/28),两者之间的差异有统计学意义(χ2=4.92,P=0.027)。
-
两种检查方法的阳性病灶横截面最大径分别为(12.83±4.18) mm和(10.38±4.51) mm,差异有统计学意义(t=2.486,P=0.018)。
-
甲状旁腺腺瘤一般较小,重量为70 mg~1 g,而原发性甲状旁腺增生,一个腺体超过60 mg即视为异常。在既往报道中有关病灶大小对99Tcm-MIBI显像诊断效能的影响存在分歧[3-4]。有研究结果显示,当病灶重量<500 mg时,平面显像的假阴性率增加,而病灶重量>1500 mg时,平面显像的阳性率接近100%[5]。结合既往研究,本研究对比了所有甲状旁腺病灶的重量,以1.00 g为界限,结果发现,双时相平面显像对病灶重量>1.00 g的B组的诊断灵敏度高于病灶重量≤1.00 g的A组,两者之间差异有统计学意义。由于平面显像的分辨率较低,一般为10 mm,对于体积较大的病灶的诊断灵敏度较高,而对于直径<10 mm的病灶的检出率则较低[6]。Vulpio等[7]认为当甲状旁腺病灶的最大横截面直径<8 mm时,99Tcm-MIBI双时相平面显像的灵敏度和特异度会明显降低。本研究结果也显示,当甲状旁腺重量较小时,其体积和病灶直径也相对较小,平面显像的检测灵敏度较低。另外,一般认为当病灶较小时,病灶的功能状态相对也较低,对MIBI的洗脱速度相对较快,而双时相平面显像要以延迟平面显像仍存在放射性浓聚灶作为判断基础,所以对一些洗脱较快的病灶存在漏诊现象[8];而病灶重量相对较大且同时未伴有囊变或钙化等病理性改变时,功能状态也相对高,早期洗脱的现象相对较少。Wachtel等[9]对2185例HPT患者的99Tcm-MIBI显像结果进行了统计分析,结果发现,38.3%的病灶未能得到准确定位,这些未定位的病灶与阳性病灶相比,甲状旁腺的体积更小、重量更轻、增生性病变更多。在本研究中,我们对双时相平面显像早期洗脱现象进行统计,A组病灶早期洗脱率为30.00%,B组病灶早期洗脱率为7.14%,两者之间的差异有统计学意义;此外,我们还发现,双时相平面显像对B组的诊断灵敏度高于A组,或与此有一定关系。
我们对病灶重量≤1.00 g组中两种显像方法的诊断灵敏度也进行了分析,结果显示,99Tcm-MIBI SPECT/CT早期断层融合显像对A组的诊断灵敏度高于99Tcm-MIBI双时相平面显像。究其原因可能是:一般小的甲状旁腺病灶功能状态也相对较低,99Tcm-MIBI SPECT/CT早期断层融合显像通过病灶对99Tcm-MIBI的摄取情况和CT提供的解剖信息进行综合判断,避免了部分病灶因为洗脱速度较快而造成的双时相平面显像的漏诊。另外,还可能是由于SPECT/CT配备诊断级螺旋CT,具有较高的空间分辨率,对于小病灶的检出具有更明显的优势[10]。而对于病灶重量>1.00 g组中的甲状旁腺病灶,99Tcm-MIBI SPECT/CT早期断层融合显像较双时相平面显像则未显示出更高的诊断灵敏度。
甲状旁腺腺瘤重量>2 g称为巨大甲状旁腺腺瘤,甲状旁腺癌腺体重量为2~10 g,单个增生的甲状旁腺腺体甚至可以超过10 g,当甲状旁腺病灶体积过大且同时与甲状腺组织前后重叠时,99Tcm-MIBI双时相平面显像会因为甲状腺区可能呈现弥漫性的浓聚而引起漏诊或误诊[11]。由于病灶放射性浓聚范围较大,平面显像难以判断病灶来源,而SPECT/CT断层融合显像可根据甲状旁腺病灶的组织密度、形态清楚定位放射性浓聚灶来源。本研究结果显示,99Tcm-MIBI SPECT/CT早期断层融合显像对B组的诊断灵敏度高于99Tcm-MIBI双时相平面显像,但差异无统计学意义。这说明对于病灶的精确定位方面,SPECT/CT早期断层融合显像更具优势。
尽管目前没有研究者提出99Tcm-MIBI甲状旁腺显像所能探测出的最小病灶大小,且也有研究者认为99Tcm-MIBI显像的灵敏度并不易受病灶大小和重量的影响[12],但我们认为HPT病灶重量无疑是影响甲状旁腺99Tcm-MIBI平面显像的重要因素之一。另外,我们也分别对99Tcm-MIBI双时相平面显像和99Tcm-MIBI SPECT/CT早期断层融合显像阳性病灶的横截面最大直径进行了统计,两者之间的差异有统计学意义,此研究结果也证明SPECT/CT断层融合显像较平面显像检出病灶的体积更小。
病灶的病理类型也是影响99Tcm-MIBI显像灵敏度的重要因素之一,有研究结果表明,双时相平面显像对甲状旁腺腺瘤的诊断灵敏度为75%~95%,而对甲状旁腺增生病灶的诊断灵敏度为30%~85%[13],99Tcm-MIBI SPECT/CT断层融合显像对增生甲状旁腺病灶的检出灵敏度高于99Tcm-MIBI双时相平面显像[14]。由于本研究的病例较少,故未对病灶按病理类型进行分组研究,但本研究中继发性HPT病例较多,这可能也是99Tcm-MIBI SPECT/CT早期断层融合显像的诊断灵敏度高于99Tcm-MIBI双时相平面显像的原因之一。
99Tcm-MIBI核素显像对HPT病灶的检出结果在一定程度上还受到病灶数量、功能状态及位置等的影响,另外血钙水平、维生素D及P糖蛋白等也可能影响显像结果。其中HPT患者血清PTH水平在一定程度上反映了HPT病灶的功能状态,测定血清PTH水平是诊断HPT的主要临床依据。花瞻等[15]认为,较大的甲状旁腺病变腺体的血清PTH水平升高明显,易被检出,而PTH水平轻中度升高、病灶体积较小或存在多个增生腺体时,双时相平面显像对病灶的检出相对困难,此时采用断层显像可以提高对病灶的检出能力。在本研究中,我们主要针对病灶重量对显像的影响进行分析,研究对象中继发性HPT患者相对较多,存在多例多病灶的HPT,故未对试验分组间的血清PTH水平进行分析。但血清PTH水平无疑也是影响99Tcm-MIBI显像的较大因素之一。
综上所述,甲状旁腺病灶重量对双时相平面显像的检出率有影响,病灶重量较小时,双时相平面显像对其检出的灵敏度较低;但对早期断层融合显像的灵敏度无明显影响。99Tcm-MIBI SPECT/CT早期断层融合显像对HPT具有更高的诊断效能,可以对临床诊断、治疗甲状旁腺疾病带来较好的增益效果。
利益冲突 本研究由署名作者按以下贡献声明独立开展,不涉及任何利益冲突。
作者贡献声明 王静负责试验数据的整理、相关文献的查阅及论文的撰写;朱玉春、章斌负责试验的设计、论文的审阅;蔡国强、周伟负责论文的修改及审阅;秦海峰、周青负责现场试验及试验数据的收集。
甲状旁腺病灶重量对99Tcm-MIBI显像诊断灵敏度的影响
The influence of parathyroid lesion weight on diagnostic sensitivity of 99Tcm-MIBI imaging
-
摘要:
目的 探讨甲状旁腺病灶重量对99Tcm-甲氧基异丁基异腈(MIBI)双时相平面显像及其 SPECT/CT早期断层融合显像诊断灵敏度的影响。 方法 收集2017年2月至2018年10月在昆山市第一人民医院经手术病理学确诊的甲状旁腺功能亢进患者22例,其中男性9例、女性13例,年龄28~73(50.77±8.79)岁。所有患者均于术前行99Tcm -MIBI双时相平面显像、99Tcm-MIBI SPECT/CT早期断层融合显像,以术后病理学结果为“金标准”。按切除的病灶重量将全部病灶分为两组,A组:病灶重量≤1.00 g,B组:病灶重量>1.00 g。采用χ2检验分析两种显像方法对不同重量组的诊断效能。 结果 22例患者中,共切除病灶58个。99Tcm-MIBI双时相平面显像对A、B两组的诊断灵敏度分别为47.83%(11/23)和84.00%(21/25),差异有统计学意义(χ2=7.05,P=0.008);99Tcm-MIBI SPECT/CT早期断层融合显像对A、B两组的诊断灵敏度分别为78.26%(18/23)和85.19%(23/27),差异无统计学意义(χ2=0.40,P=0.525)。99Tcm-MIBI SPECT/CT早期断层融合显像对A组的诊断灵敏度高于99Tcm-MIBI双时相平面显像,差异有统计学意义(χ2=4.57,P=0.033)。99Tcm-MIBI SPECT/CT早期断层融合显像对B组的诊断灵敏度高于99Tcm-MIBI双时相平面显像,但差异无统计学意义(χ2=0.01,P=0.906)。 结论 甲状旁腺病灶重量对99Tcm-MIBI双时相平面显像诊断灵敏度有影响,当病灶重量较小时,99Tcm-MIBI双时相平面显像对其的诊断灵敏度较低;而病灶重量对99Tcm-MIBI SPECT/CT早期断层融合显像的诊断灵敏度无明显影响。 -
关键词:
- 99m锝甲氧基异丁基异腈 /
- 体层摄影术,发射型计算机,单光子 /
- 体层摄影术,X线计算机 /
- 甲状旁腺功能亢进症
Abstract:Objective To investigate the effect of parathyroid lesion weight on the diagnostic sensitivity of 99Tcm-MIBI dual-phase plane imaging and 99Tcm-MIBI SPECT/CT tomography fusion imaging. Methods A total of 22 patients with hyperparathyroidism that was confirmed via operation and pathology in the First People's Hospital of Kunshan were collected from February 2017 to October 2018. The patients included 9 males and 13 females aged 28–73 (50.77±8.79) years old. All patients underwent 99Tcm-MIBI biphasic imaging and 99Tcm-MIBI SPECT/CT fusion imaging in the early stage. The gold standard was postoperative pathological results. All resected lesions were divided into two groups: group A, wherein lesion weight ≤1.00 g, and group B, wherein lesion weight >1.00 g. χ2 test was used to analyze the diagnostic efficacy of the two imaging methods in the different weight groups. Results A total of 58 lesions were removed from the 22 patients via surgical operation. The diagnostic sensitivity values of 99Tcm-MIBI dual-phase plane imaging for groups A and B were 47.83% (11/23) and 84.00% (21/25) respectively, and were statistically significantly different between the two groups (χ2=7.05, P=0.008). The diagnostic sensitivity values of 99Tcm-MIBI SPECT/CT early tomography for groups A and B were 78.26% (18/23) and 85.19% (23/27), respectively, and did not show significant differences between the two groups (χ2=0.40, P=0.525). In group A, the diagnostic sensitivity of 99Tcm-MIBI SPECT/CT early tomography was higher than that of dual-phase plane imaging; this difference was statistically significant (χ2=4.57, P=0.033). In group B, the diagnostic sensitivity of 99Tcm-MIBI SPECT/CT early tomography was higher than that of dual-phase plane imaging; however, no significant difference was observed (χ2=0.01, P=0.906). Conclusions The weight of parathyroid lesions has an effect on dual-phase planar imaging. Specifically, sensitivity decreased when the parathyroid glands were light. However, lesion weight had no significant effect on the diagnostic sensitivity of early tomographic fusion imaging. -
图 1 继发性甲状旁腺功能亢进症患者(女性,47岁)的99Tcm-MIBI双时相平面显像及SPECT/CT断层融合显像图
Figure 1. 99Tcm-MIBI dual-phase planar imaging and SPECT/CT fusion imaging of secondary hyperparathyroidism(female, 47 years old)
图 2 原发性甲状旁腺功能亢进症患者(女性,68岁)的99Tcm-MIBI双时相平面显像图、SPECT/CT断层融合显像图及病理图
Figure 2. 99Tcm-MIBI dual-phase planar imaging, SPECT/CT fusion imaging, ultrasound imaging and pathological section of primary hyperparathyroidism(female, 68 years old)
表 1 两种显像方法在不同质量组中的灵敏度、特异度和 准确率比较
Table 1. Comparison of sensitivity, specificity and accuracy of two imaging methods in different weight groups
组别 灵敏度 特异度 准确率 显像1 A组 47.83%(11/23) 85.71%(6/7) 56.67%(17/30) B组 84.00%(21/25) − (0/3) 75.00%(21/28) 显像2 A组 78.26%(18/23) 85.71%(6/7) 80.00%(24/30) B组 85.19%(23/27) − (0/1) 82.14%(23/28) 注:表中,显像1:99Tcm-MIBI双时相平面显像;显像2:99Tcm-MIBI SPECT/CT早期断层融合显像;A组病灶重量≤1.00 g,B组病灶重量>1.00 g;−:无真阴性病灶。MIBI:甲氧基异丁基异腈;SPECT:单光子发射计算机体层摄影术;CT:计算机体层摄影术  下载: 导出CSV
下载: 导出CSV
-
[1] Mandal R, Muthukrishnan A, Ferris RL, et al. Accuracy of early-phase versus dual-phase single-photon emission computed tomography/computed tomography in the localization of parathyroid disease[J]. Laryngoscope, 2015, 125(6): 1496−1501. DOI: 10.1002/lary.25020. [2] Sumana BS, Sabaretnam M, Sarathi V, et al. Functional parathyroid cystic adenoma: A rare cause of hypercalcemic crisis with primary hyperparathyroidism[J]. Indian J Pathol Microbiol, 2015, 58(4): 487−490. DOI: 10.4103/0377−4929.168847. [3] 钟箫, 欧晓红, 李林, 等. <sup>99</sup>Tc<sup>m</sup>-MIBI SPECT/CT融合显像在甲状旁腺功能亢进症术前诊断中的应用价值[J]. 中华核医学与分子影像杂志, 2017, 37(7): 395−399. DOI: 10.3760/cma.j.issn.2095−2848.2017.07.004.
Zhong X, Ou XH, Li L, et al. Value of <sup>99</sup>Tc<sup>m</sup>-MIBI SPECT/CT in pre-operative diagnosis of primary and secondary hyperparathyroidism[J]. Chin J Nucl Med Mol Imaging, 2017, 37(7): 395−399. DOI: 10.3760/cma.j.issn.2095−2848.2017.07.004.[4] Kim YI, Jung YH, Hwang KT, et al. Efficacy of <sup>99m</sup>Tc-sestamibi SPECT/CT for minimally invasive parathyroidectomy: comparative study with <sup>99m</sup>Tc-sestamibi scintigraphy, SPECT, US and CT[J]. Ann Nucl Med, 2012, 26(10): 804−810. DOI: 10.1007/s12149−012−0641−0. [5] 张长明, 马欢, 张玉芳, 等. <sup>99</sup>Tc<sup>m</sup>-MIBI断层及同机CT融合显像在继发性甲状旁腺功能亢进症术前定位诊断中的价值[J]. 中华内分泌外科杂志, 2016, 10(1): 23−25. DOI: 10.3760/cma.j.issn.1674−6090.2016.01.006.
Zhang CM, Ma H, Zhang YF, et al. Value of <sup>99</sup>Tc<sup>m</sup>-MIBI tomography and registration with integrated CT in preoperative localization and diagnosis of secondary hyperparathyroidism[J]. J Endocr Surg, 2016, 10(1): 23−25. DOI: 10.3760/cma.j.issn.1674−6090.2016.01.006.[6] Wei WJ, Shen CT, Song HJ, et al. Comparison of SPET/CT, SPET and Planar Imaging Using <sup>99m</sup>Tc-MIBI as Independent Techniques to Support Minimally Invasive Parathyroidectomy in Primary Hyperparathyroidism: A Meta-Analysis[J]. Hell J Nucl Med, 2015, 18(2): 127−135. DOI: 10.1967/s002449910207. [7] Vulpio C, Bossola M, De Gaetano A, et al. Usefulness of the combination of ultrasonography and <sup>99m</sup>Tc-sestamibi scintigraphy in the preoperative evaluation of uremic secondary hyperparathyroidism[J]. Head Neck, 2010, 32(9): 1226−1235. DOI: 10.1002/hed.21320. [8] Martínez-Rodríguez I, Banzo I, Quirce R, et al. Early Planar and Early SPECT Tc-99m Sestamibi Imaging: Can It Replace the Dual-Phase Technique for the Localization of Parathyroid Adenomas by Omitting the Delayed Phase?[J]. Clin Nucl Med, 2011, 36(9): 749−753. DOI: 10.1097/RLU.0b013e318217568a. [9] Wachtel H, Bartlett EK, Kelz RR, et al. Primary Hyperparathyroidism With Negative Imaging: A Significant Clinical Problem[J]. Ann Surg, 2014, 260(3): 474−482. DOI: 10.1097/SLA.0000000000000875. [10] Ozkan ZG, Unal SN, Kuyumcu S, et al. Clinical Utility of Tc-99m MIBI SPECT/CT for Preoperative Localization of Parathyroid Lesions[J]. Indian J Surg, 2017, 79(4): 312−318. DOI: 10.1007/s12262−016−1489−7. [11] 邹珍, 常娅妮, 崔雅丽, 等. 巨大甲状旁腺腺瘤99Tcm-MIBI双时相SPECT/CT显像一例[J]. 国际放射医学核医学杂志, 2017, 41(2): 156−158. DOI: 10.3760/cma.j.issn.1673-4114.2017.02.014.ZOUZ,
Zou Z, Chang YN, Cui YL, et al. 99Tcm-MIBI dual phase SPECT/CT in a case of giant parathyroid adenoma[J]. Int J Radiat Med Nucl Med, 2017, 41(2): 156−158. DOI: 10.3760/cma.j.issn.1673-4114.2017.02.014.[12] Noda S, Onoda N, Kashiwagi S, et al. Strategy of operative treatment of hyperparathyroidism using US scan and <sup>99m</sup>Tc-MIBI SPECT/CT[J]. Endocr J, 2014, 61(3): 225−230. DOI: 10.1507/endocrj.ej13−0292. [13] 许小飞, 刘雅洁, 张伟晓, 等. <sup>99</sup>Tc<sup>m</sup>-MIBI延迟显像对继发性甲状旁腺功能亢进症异位病灶的诊断价值[J]. 中华核医学与分子影像杂志, 2016, 36(5): 431−435. DOI: 10.3760/cma.j.issn.2095−2848.2016.05.011.
Xu XF, Liu YJ, Zhang WX, et al. Diagnostic value of dual-phase <sup>99</sup>Tc<sup>m</sup>-MIBI scintigraphy in patients with ectopic secondary hyperparathyroidism[J]. Chin J Nucl Med Mol Imaging, 2016, 36(5): 431−435. DOI: 10.3760/cma.j.issn.2095−2848.2016.05.011.[14] Lavely WC, Goetze S, Friedman KP, et al. Comparison of SPECT/CT, SPECT, and Planar Imaging with Single- and Dual- Phase <sup>99m</sup>Tc-Sestamibi Parathyroid Scintigraphy[J]. J Nucl Med, 2007, 48(7): 1084−1089. DOI: 10.2967/jnumed.107.040428. [15] 花瞻, 姚力, 张凌. 继发性甲状旁腺功能亢进的外科治疗[J]. 临床内科杂志, 2012, 29(5): 305−307. DOI: 10.3969/j.issn.1001−9057.2012.05.005.
Hua Z, Yao L, Zhang L. Surgical treatment of secondary hyperparathyroidism[J]. J Clin Intern Med, 2012, 29(5): 305−307. DOI: 10.3969/j.issn.1001−9057.2012.05.005. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 44432
- HTML全文浏览量: 10869
- PDF下载量: 44
