


-
心肌灌注显像(myocardial perfusion imaging, MPI)是一种无创的可用于检查心脏病的方法,其巨大的临床应用价值已在世界范围内被广泛接受,成为目前冠心病诊断、危险度分层、疗效评价以及预后判断的重要影像学方法。冠心病与Graves甲状腺功能亢进症(简称甲亢)均可产生心悸、胸闷、心前区不适等症状,临床上常常混淆、不易区分,且两者可同时存在。甲亢合并稳定性心绞痛时,常规的无创检查方法,如心电图、超声心动图等常无阳性发现,冠状动脉CT可发现冠状动脉狭窄但不能提供狭窄的病理生理学意义,且行冠状动脉CT检查需要静脉注入碘造影剂,对于甲亢患者并不适合。本研究对一例确诊为Graves甲亢且疑似冠心病的患者应用MPI进行冠心病诊断及危险度分层,在其引导下行经皮冠状动脉介入治疗(percutaneous coronary intervention,PCI)治疗的案例进行了报道。
-
患者女性,70岁,因“间断心悸、胸闷、憋气1月余,劳累后加重10 d”于2015年9月在天津市第三中心医院住院治疗。既往高血压病史8年余,最高血压为195/100 mmHg,平时服用苯磺酸氨氯地平及倍他乐克降压治疗;糖尿病史8年余,平时服用瑞格列奈及二甲双胍治疗;Graves甲亢病史1年余,现服用甲巯咪唑5 mg/日治疗。
体格检查:皮肤潮湿,双眼轻度外突,触诊甲状腺I度肿大,质地中等、无压痛、未扪及明显结节,心音有力,心率为90次/分,节律整齐,各瓣膜听震区未闻及杂音,双下肢不肿,手颤(+)。
甲状腺功能及相关抗体检查见表1。血脂:总胆固醇为5.89(正常参考值0~5.20)mmol/L,甘油三酯为5.38(正常参考值为0~1.70)mmol/L,高密度脂蛋白胆固醇为1.26(正常参考值为1.29~1.55)mmol/L,低密度脂蛋白胆固醇为2.28(正常参考值为2.70~3.10)mmol/L,极低密度脂蛋白胆固醇为2.35(正常参考值为0.18~0.91)mmol/L。空腹血糖水平为9.00 mmol/L,餐后2 h血糖为12.30 mmol/L,糖化血红蛋白为7.2%(正常参考值为4.0%~6.0%)。肌红蛋白为59(正常参考值为0~107)ng/mL,肌酸激酶同工酶为1.0(正常参考值为0~4.3)ng/mL,肌钙蛋白Ⅰ为0.05(正常参考值为0~0.40)ng/mL,B型钠尿肽为43.5(正常参考值为0~100.0)pg/mL。
游离甲状腺功能及相关抗体 正常范围 PCI前 PCI后1周 PCI后1月 PCI后1年 PCI后2年 FT3(pmol/L) 3.1~6.8 8.94 5.60 5.86 5.72 5.40 FT4(pmol/L) 12~22 28.72 21.12 15.80 13.57 14.29 TSH(mIU/L) 0.27~4.2 0.01 0.02 0.04 0.33 0.52 TgAb(IU/mL) 45~125 15.60 − 17.85 15.20 16.35 TPOAb(IU/mL) 65~85 6.59 − 6.25 6.32 5.86 TRAb(IU/mL) <1.75 5.26 − 5.76 3.52 2.26 注:表中,“−”表示无此项数据;PCI:经皮冠状动脉介入治疗;FT3:游离三碘甲腺原氨酸;FT4:游离甲状腺素;TSH:促甲状腺激素;TgAb:抗甲状腺球蛋白抗体;TPOAb:甲状腺过氧化物酶抗体;TRAb:促甲状腺素受体抗体。 表 1 一女性Graves甲亢合并冠心病患者经皮冠状动脉介入治疗前后游离甲状腺功能及相关抗体水平
Table 1. Free thyroid function and related antibody level of a female patient having Graves' hyperthyroidism complicated with coronary artery heart disease before and after percutaneous coronary intervention
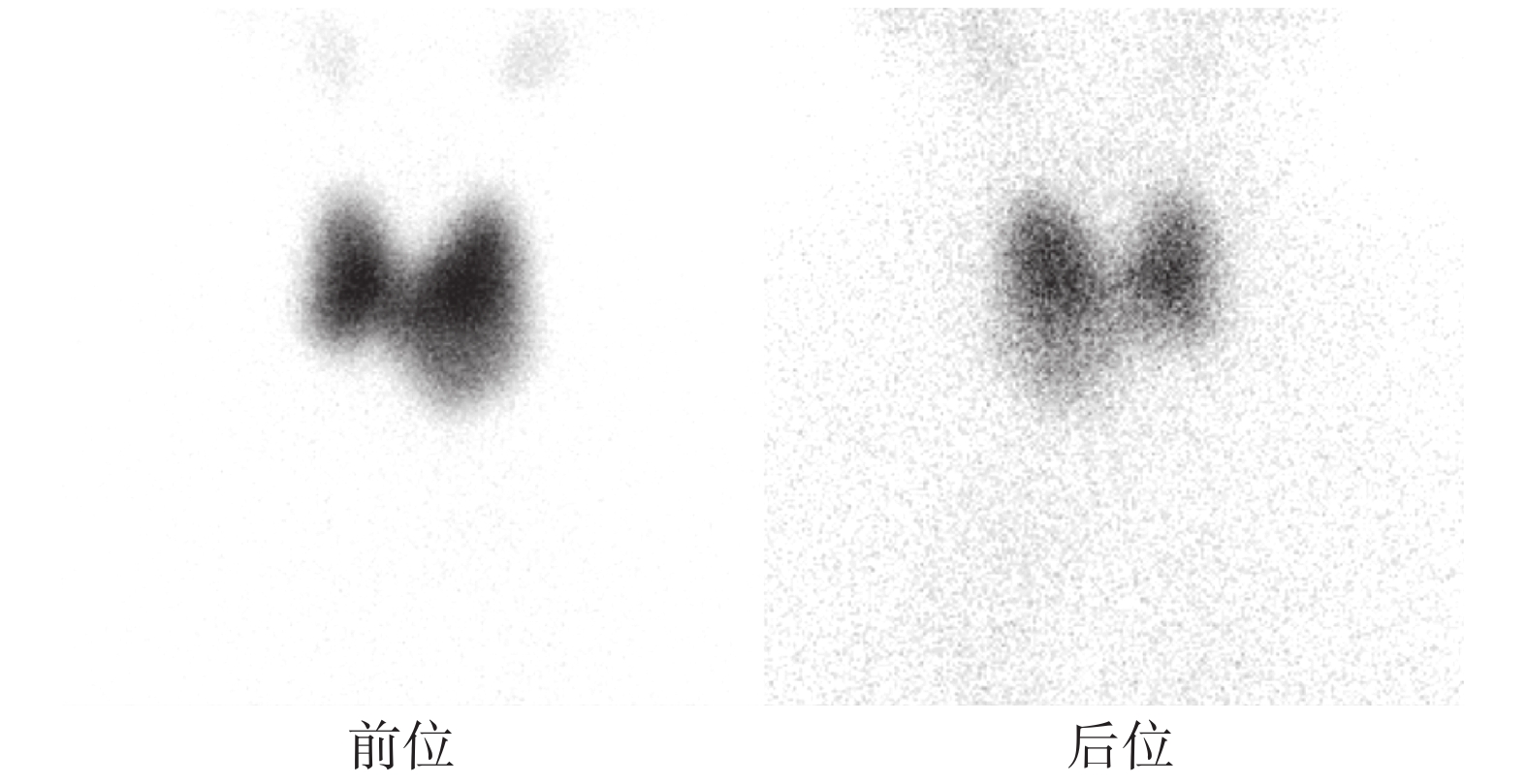
心电图:窦性心律,心率为90次/分,非特异性ST-T异常。甲状腺彩超:双叶甲状腺多发结节(TI-RADSⅡ类),最大位于左叶下极,约3.1 cm×2.0 cm。甲状腺静态显像:双叶甲状腺肿大(左叶为著)伴核素摄取能力不均匀增强,甲状腺左叶下极摄取能力减低(图1)。
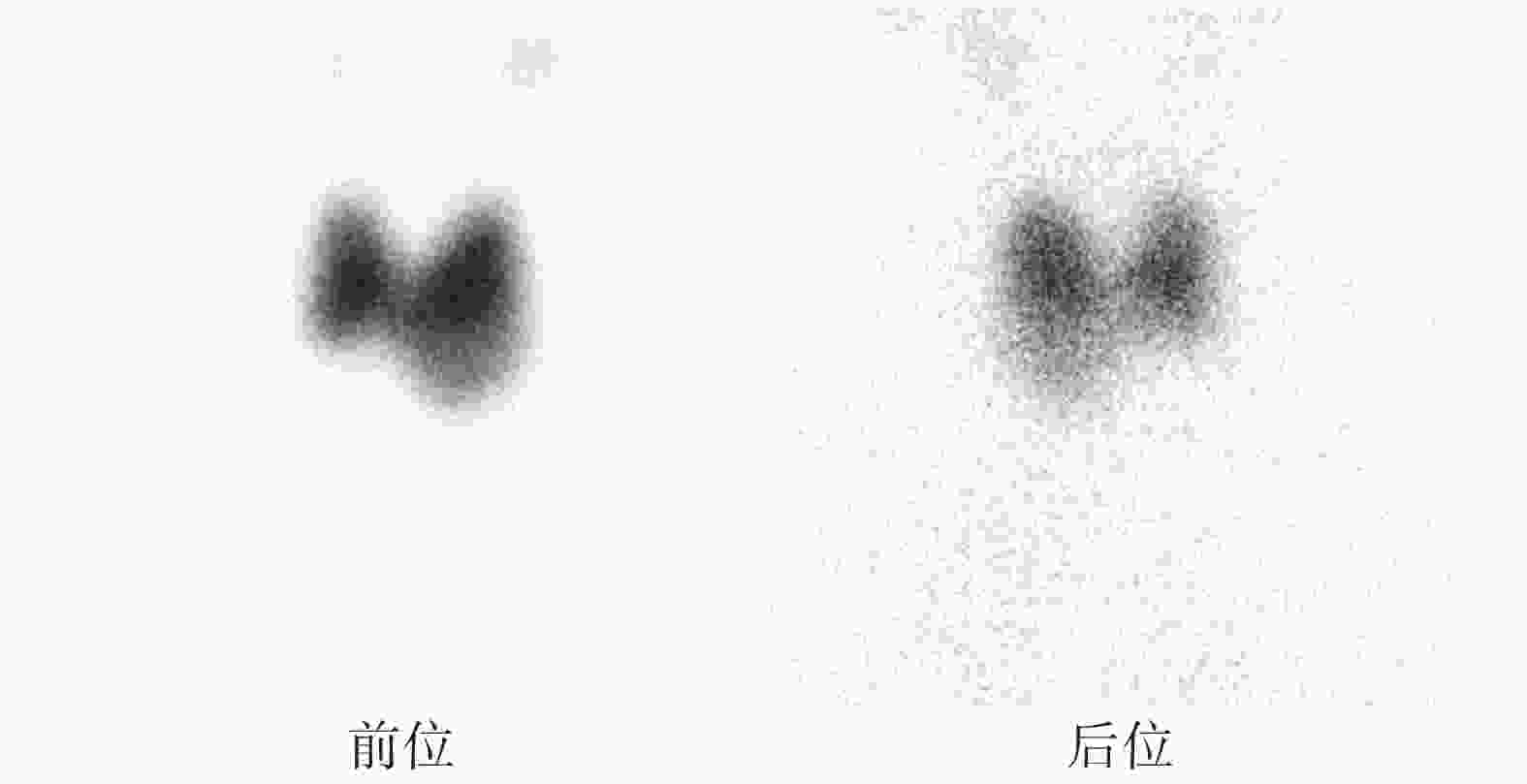
图 1 Graves甲亢合并冠心病患者(女性,70岁)甲状腺前、后位静态显像图
Figure 1. Thyroid scintigraphy of a 70-year-old female patient with both Graves' hyperthyroidism and coronary artery heart disease
入院主要诊断:①怀疑冠心病;②Graves甲亢;③2型糖尿病;④高血压病3级(极高危);⑤高脂血症;⑥甲状腺多发结节。
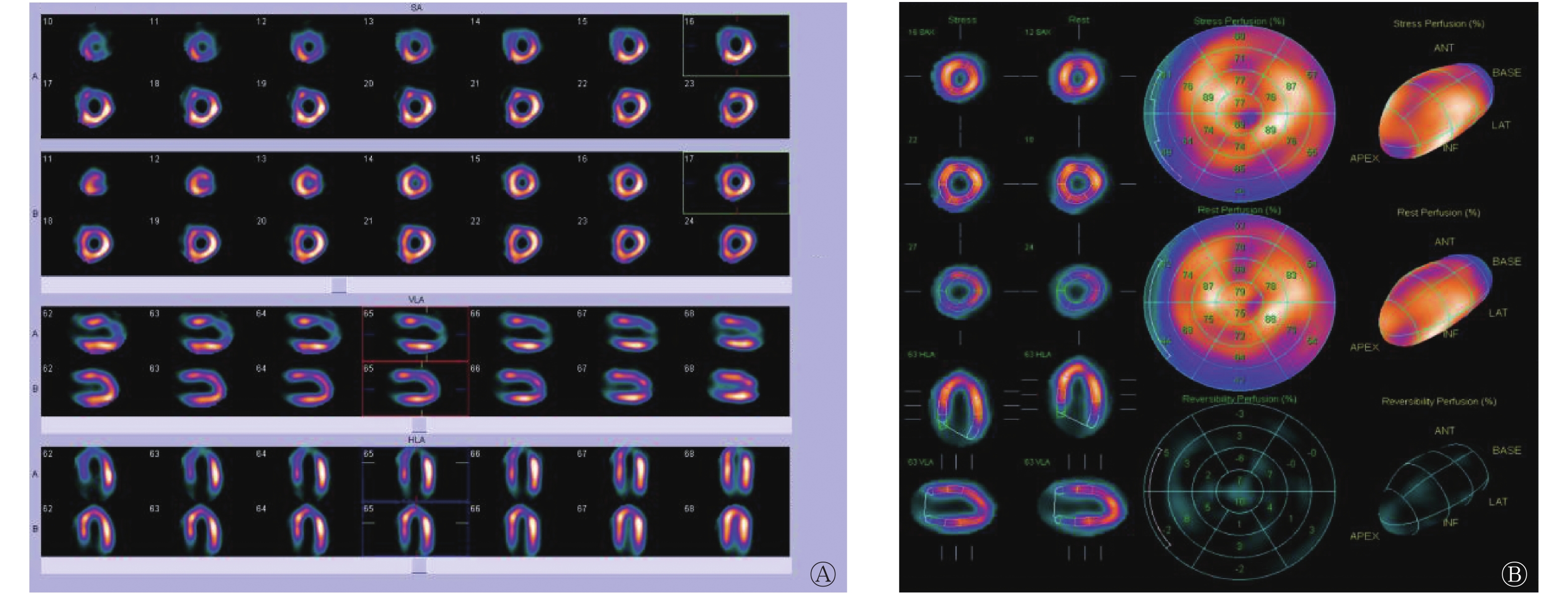
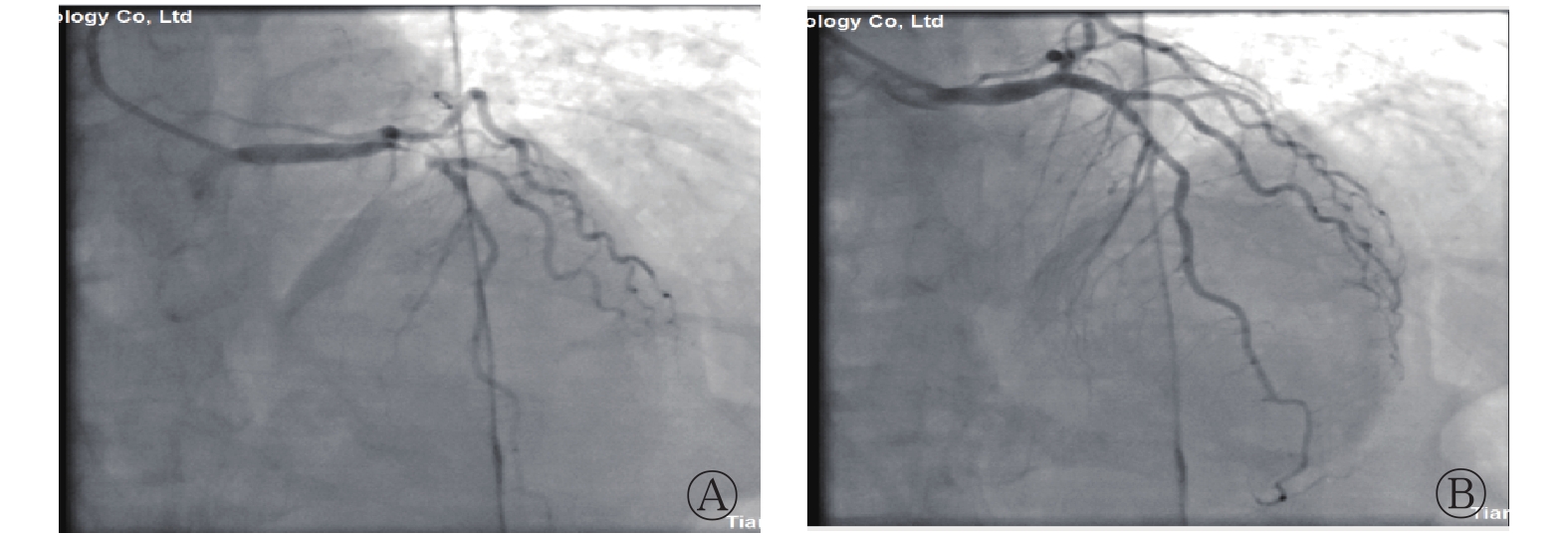
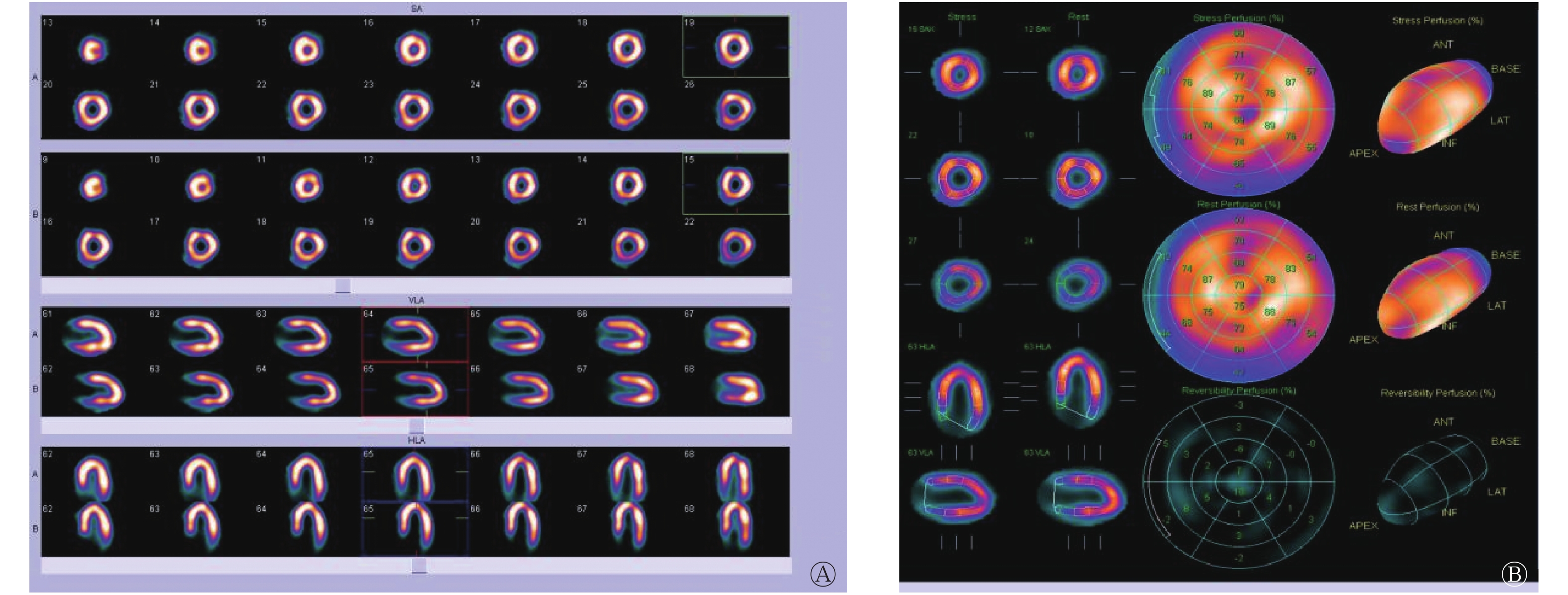
入院后予以控制血压、血糖、降脂、抗凝、β受体阻滞剂控制心室率等治疗,并将甲巯咪唑加量至15 mg/日控制甲亢。患者住院期间仍间断发作心前区不适,为明确患者症状是否与“冠心病、心肌缺血”有关,遂于入院后1周在我院核医学科接受两日法静息+ATP负荷MPI检查,结果提示左冠状动脉供血区出现大范围可逆性心肌缺血(图2)。尽管患者患有Graves甲亢,属于接受碘造影剂的相对禁忌,但甲状腺激素水平属轻度增高,已给予适量抗甲状腺药物治疗且无不良反应,而MPI提示大范围可逆性心肌缺血,危险度分层属于冠心病高危,权衡利弊后,患者最终接受冠状动脉造影检查。术中见左冠状动脉前降支近段95%狭窄,植入支架一枚(图3)。患者术后心前区不适等症状完全缓解,继续口服甲巯咪唑15 mg/日治疗甲亢,1周后复查游离甲状腺功能发现,仅TSH低于正常,甲巯咪唑逐渐减量至5 mg/日维持治疗。后续门诊随访甲状腺功能结果见表1,3个月后复查静息+ATP负荷MPI未见可逆性心肌缺血(图4)。
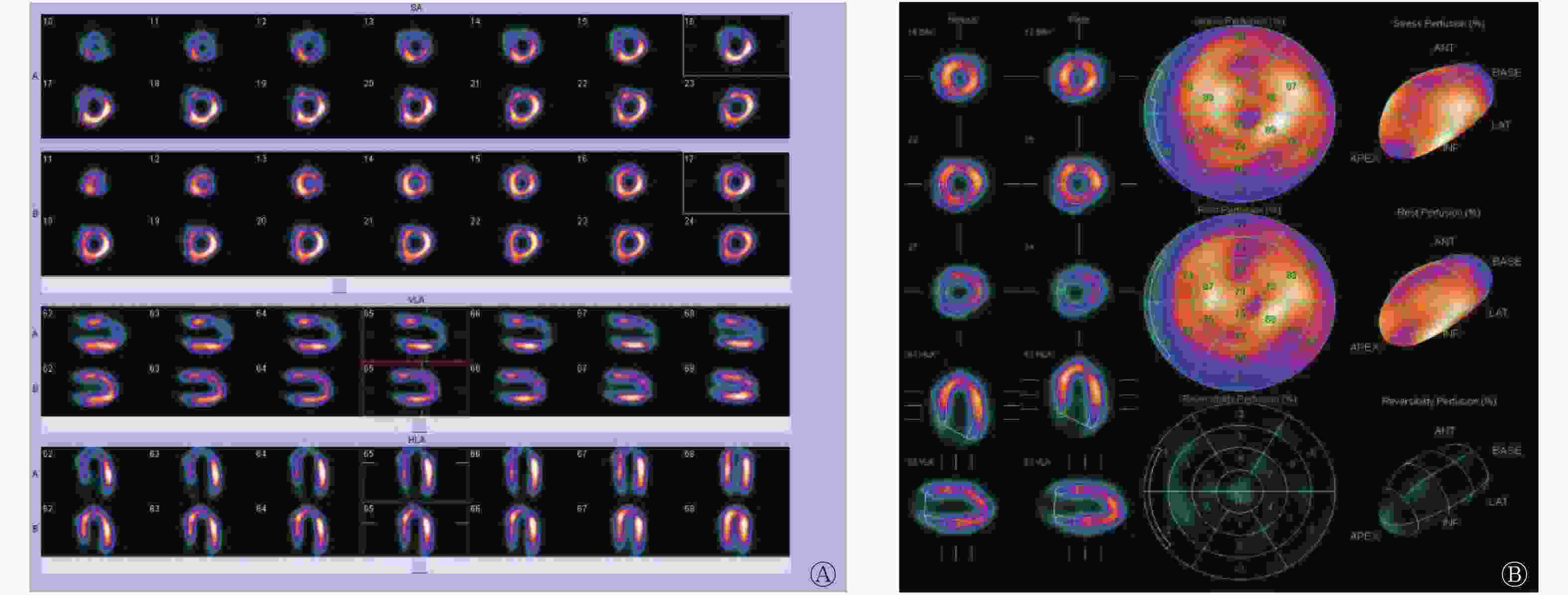
图 2 Graves甲亢合并冠心病患者(女性,70岁)三磷酸腺苷负荷+静息心肌血流灌注显像图
Figure 2. Adenosine triphosphate stressing and resting myocardial perfusion imaging of a 70-year-old female patient with Graves' hyperthyroidism complicated and coronary artery heart disease
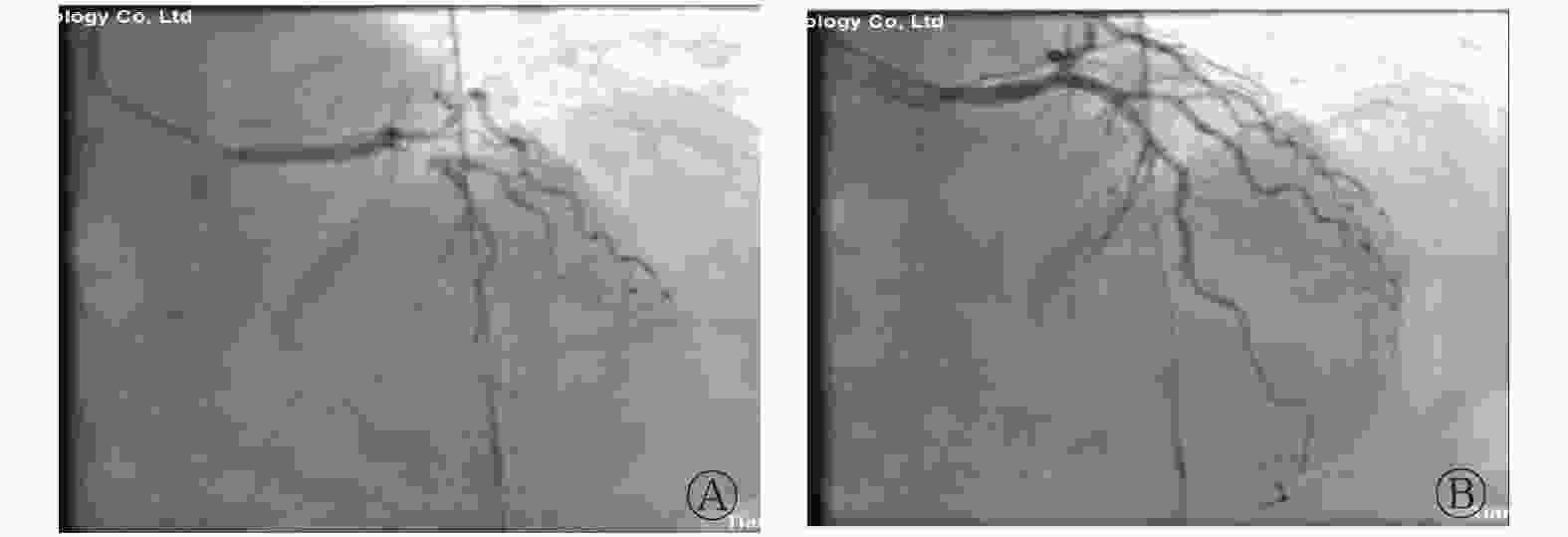
图 3 Graves甲亢合并冠心病患者(女性,70岁)冠状动脉造影图
Figure 3. Coronary angiography of a 70-year-old female patient with both Graves' hyperthyroidism and coronary artery heart disease
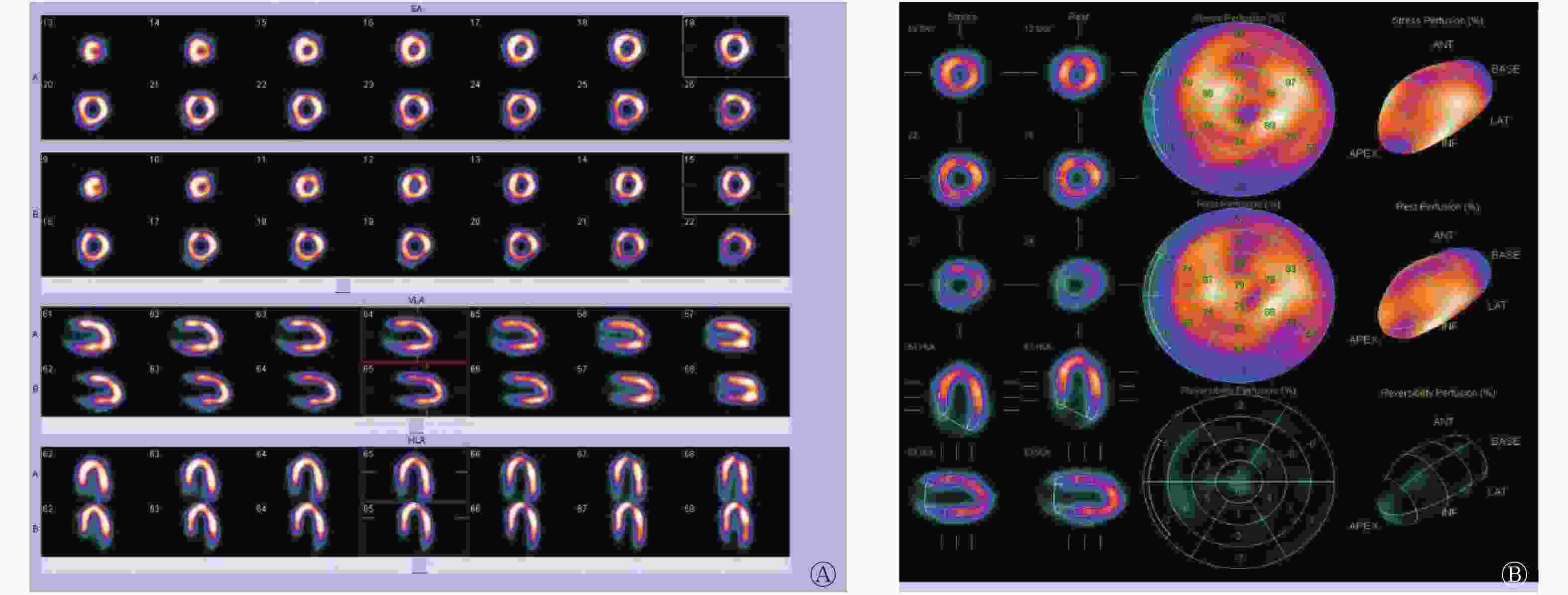
图 4 Graves甲亢合并冠心病患者(女性,70岁)经皮冠状动脉介入治疗术后3个月复查三磷酸腺苷负荷+静息心肌血流灌注显像图
Figure 4. The recheck of adenosine triphosphate stressing and resting myocardial perfusion imaging of a 70-year-old female patient with Graves' hyperthyroidism complicated and coronary artery heart disease three months after percutaneous coronary intervention
-
Graves甲亢时甲状腺激素合成过多,释放入血,可引起心血管系统兴奋性增高、需氧量增加,从而产生心悸、胸闷、心率增快、心脏扩大、心房纤颤、脉压增大等症状和体征。冠心病是冠状动脉发生严重粥样硬化或痉挛,使冠状动脉狭窄或阻塞以及血栓形成造成管腔闭塞,导致心肌缺血、缺氧或梗死的一类心脏病。两者症状相似,临床上常常混淆、不易区分,且可合并存在,有文献报道其发生率为0.5%~20%[1]。ATP介入负荷MPI诊断冠心病具有较高的效能[2],除能明确有无可逆性心肌缺血及缺血的部位、范围和程度外,还可以用于冠心病危险度分层,帮助患者决定是否需要接受PCI等侵入性治疗方案[3],在进行ATP负荷试验前应排除禁忌症(包括IIo以上房室传导阻滞、低血压、哮喘、急性心肌梗死等),负荷试验中应密切观察患者情况并用心电仪器监护其变化,若出现停药指征(如明显心绞痛、ST段抬高≥0.1 mV或压低>0.2 mV及各类严重心律失常)时应及时停药。本研究中该例患者Graves甲亢诊断明确,且有高龄、高血压、糖尿病、高脂血症等冠心病高危因素,采用静息+ATP负荷MPI明确了冠心病的诊断,且存在大范围可逆性心肌缺血,冠心病危险度分层为高危(负荷总评分:26分,总缺损面积:29%),因此有必要在治疗甲亢的同时针对冠心病进行恰当的干预。
中国经皮冠状动脉介入治疗指南(2016)[4]指出对于大面积缺血(缺血面积>左心室10%)的稳定性冠心病患者应进行血运重建治疗。但对于合并甲亢的患者,由于担心行冠状动脉造影时注入碘对比剂会加重患者的甲亢病情甚至诱发甲亢危象,所以是否进行侵入性治疗还存在争议,且对于此类患者行PCI后的预后如何尚无研究明确[5]。目前常用的非离子型碘造影剂碘克沙醇的禁忌症包括未经控制的甲亢患者。从本研究中的该例患者来看,甲状腺功能水平轻度升高,且已合理应用抗甲状腺药物控制甲亢症状,未违反造影剂使用禁忌。结合患者大范围心肌缺血及冠心病高危情况,经患者知情同意后决定行冠状动脉造影,术中尽量减少碘对比剂的使用剂量。术后继续应用甲巯咪唑及β受体阻滞剂,密切监测病情,患者无甲亢危象及甲亢症状加重情况发生,术后3个月复查静息+ATP负荷MPI提示可逆性心肌缺血完全恢复正常,继续随访甲状腺功能亦完全恢复正常。
综上,我们认为对于甲亢合并有冠心病高危因素(如高龄、高血压、糖尿病、高脂血症等)的患者在排除禁忌症的情况下可以应用核医学MPI进行冠心病危险度分层。对于筛选出的冠心病高危患者在合理用药使甲亢得到控制的同时可酌情进行冠状动脉造影检查。术后应继续服用抗甲状腺药物及β受体阻滞剂治疗,密切随访其甲状腺功能的变化,调整抗甲状腺药物的用量。本研究对使用了碘造影剂的甲亢合并冠心病患者的预后提供了一定的参考价值。
利益冲突 本研究由署名作者按以下贡献声明独立开展,不涉及任何利益冲突。
作者贡献声明 张建萍负责论文的撰写与修改;刘雪辉负责研究命题的提出、设计及指导,张建萍、于泓煦、刘娜、沈慧、陈兵负责数据、图像的获取、提供与分析。
心肌灌注显像引导下行PCI治疗的Graves甲亢合并冠心病一例
Graves' hyperthyroidism complicated with coronary heart disease treated by percutaneous coronary intervention under the guidance of myocardial perfusion imaging: a case report
-
摘要: 笔者介绍了一例因心悸、胸闷、憋气入院的Graves甲状腺功能亢进症(简称甲亢)合并冠心病的病例。其Graves甲亢诊断明确,且合并高龄、高血压、糖尿病、高脂血症等冠心病的高危因素。行两日法静息+三磷酸腺苷负荷心肌灌注显像(MPI)发现患者存在大范围心肌缺血,其冠心病危险度分层为高危,权衡利弊后建议其行冠状动脉造影。经皮冠状动脉介入治疗术后患者血运重建良好且无甲亢危象发生。本研究旨在提示甲亢合并可疑冠心病患者在排除相关禁忌后应采用核医学MPI进行冠心病危险度分层,以进一步指导治疗方案。
-
关键词:
- 格雷夫斯病 /
- 甲状腺功能亢进症 /
- 冠心病 /
- 心肌灌注显像 /
- 单光子发射计算机体层摄影术 /
- 经皮冠状动脉介入治疗
Abstract: A patient hospitalized with palpitation, chest tightness, and shortness of breath was reported in this study. She was definitively diagnosed with Graves' hyperthyroidism and had several risk factors of coronary heart disease (CHD), including old age, hypertension, diabetes, and hyperlipidemia. Resting and ATP stressing myocardial perfusion imaging were applied in 2 days to determine whether CHD exists in this patient. Results confirmed that the patient has extensive myocardial ischemia and a high risk of cardiac adverse events. Thus, coronary angiography was suggested. Revascularization was achieved after percutaneouscoronary intervention, and no hyperthyroidism crisis occurred. MPI is recommended for patients with hyperthyroidism and suspected CHD after excluding correlative contraindications to facilitate the risk stratification of CHD and guide further treatment strategies. -
图 1 Graves甲亢合并冠心病患者(女性,70岁)甲状腺前、后位静态显像图
Figure 1. Thyroid scintigraphy of a 70-year-old female patient with both Graves' hyperthyroidism and coronary artery heart disease
图 2 Graves甲亢合并冠心病患者(女性,70岁)三磷酸腺苷负荷+静息心肌血流灌注显像图
Figure 2. Adenosine triphosphate stressing and resting myocardial perfusion imaging of a 70-year-old female patient with Graves' hyperthyroidism complicated and coronary artery heart disease
图 3 Graves甲亢合并冠心病患者(女性,70岁)冠状动脉造影图
Figure 3. Coronary angiography of a 70-year-old female patient with both Graves' hyperthyroidism and coronary artery heart disease
图 4 Graves甲亢合并冠心病患者(女性,70岁)经皮冠状动脉介入治疗术后3个月复查三磷酸腺苷负荷+静息心肌血流灌注显像图
Figure 4. The recheck of adenosine triphosphate stressing and resting myocardial perfusion imaging of a 70-year-old female patient with Graves' hyperthyroidism complicated and coronary artery heart disease three months after percutaneous coronary intervention
表 1 一女性Graves甲亢合并冠心病患者经皮冠状动脉介入治疗前后游离甲状腺功能及相关抗体水平
Table 1. Free thyroid function and related antibody level of a female patient having Graves' hyperthyroidism complicated with coronary artery heart disease before and after percutaneous coronary intervention
游离甲状腺功能及相关抗体 正常范围 PCI前 PCI后1周 PCI后1月 PCI后1年 PCI后2年 FT3(pmol/L) 3.1~6.8 8.94 5.60 5.86 5.72 5.40 FT4(pmol/L) 12~22 28.72 21.12 15.80 13.57 14.29 TSH(mIU/L) 0.27~4.2 0.01 0.02 0.04 0.33 0.52 TgAb(IU/mL) 45~125 15.60 − 17.85 15.20 16.35 TPOAb(IU/mL) 65~85 6.59 − 6.25 6.32 5.86 TRAb(IU/mL) <1.75 5.26 − 5.76 3.52 2.26 注:表中,“−”表示无此项数据;PCI:经皮冠状动脉介入治疗;FT3:游离三碘甲腺原氨酸;FT4:游离甲状腺素;TSH:促甲状腺激素;TgAb:抗甲状腺球蛋白抗体;TPOAb:甲状腺过氧化物酶抗体;TRAb:促甲状腺素受体抗体。  下载: 导出CSV
下载: 导出CSV
-
[1] 陈秀林. 甲状腺功能亢进症合并急性心肌梗死患者的临床分析[J]. 中国急救医学, 2011, 31(7): 664−666. DOI: 10.3969/j.issn.1671−7171.2013.09.041.
Chen XL. Clinical Analysis of Hyperthyroidism Complicated with Acute Myocardial Infarction[J]. J Clin Res, 2011, 31(7): 664−666. DOI: 10.3969/j.issn.1671−7171.2013.09.041.[2] 姚稚明, 王蒨, 田月琴, 等. ATP介入心肌灌注显像诊断冠心病的多中心研究[J]. 中华核医学与分子影像杂志, 2014, 34(4): 292−295. DOI: 10.3760/cma.j.issn.2095−2848.2014.04.006.
Yao ZM, Wang Q, Tian YQ, et al. A multi-center trial on the study of ATP stress myocardial perfusion imaging in the detection of coronary artery disease[J]. Chin J Nucl Med Mol Imaging, 2014, 34(4): 292−295. DOI: 10.3760/cma.j.issn.2095−2848.2014.04.006.[3] Hung GU, Ko KY, Lin CL, et al. Impact of initial myocardial perfusion imaging versus invasive coronary angiography on outcomes in coronary artery disease: a nationwide cohort study[J]. Eur J Nucl Med Mol Imaging, 2018, 45(4): 567−574. DOI: 10.1007/s00259−017−3872−4. [4] 中华医学会心血管病学分会介入心脏病学组, 中国医师协会心血管内科医师分会血栓防治专业委员会, 中华心血管病杂志编辑委员会. 中国经皮冠状动脉介入治疗指南(2016)[J]. 中华心血管病杂志, 2016, 44(5): 382−400. DOI: 10.3760/cma.j.issn.0253−3758.2016.05.006.
Interventional cardiology group of cardiovascular branch of Chinese Medical Association, Thrombus Prevention and Control Professional Committee of Cardiovascular Branch of Chinese Medical Association, Editorial Board of Chinese Journal of Cardiovascular Disease. Guidelines for percutaneous coronary intervention in China (2016)[J]. Chin J Cardiol, 2016, 44(5): 382−400. DOI: 10.3760/cma.j.issn.0253−3758.2016.05.006.[5] 艾倩, 杨会明, 李江兴, 等. 冠状动脉造影剂对急性冠状动脉综合征患者近期甲状腺功能及预后的影响[J]. 山东医药, 2013, 53(32): 65−67. DOI: 10.3969/j.issn.1002−266X.2013.32.025.
Ai Q, Yang HM, Li JX, et al. Effect of coronary artery contrast agent on thyroid function and prognosis in patients with acute coronary syndrome[J]. Shandong Med J, 2013, 53(32): 65−67. DOI: 10.3969/j.issn.1002−266X.2013.32.025. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 2825
- HTML全文浏览量: 1798
- PDF下载量: 10