




-
颅内动脉瘤(intracranial aneurysm,IAN)是颅内局部的动脉血管发生异常改变而产生的瘤样突起[1]。IAN主要的危险是破裂时易引起蛛网膜下腔出血,且破裂后的病死率和致残率特别高[2]。正确诊断IAN是临床实施治疗的基础,只有不断提高IAN的诊断水平,才能及时制定出有效可行的治疗方案。数字减影血管造影(digital subtraction angiography,DSA)仍然是目前诊断IAN的“金标准”,与二维DSA(two-dimensional DSA,2D-DSA)技术相比,三维DSA(three-dimensional DSA,3D-DSA)技术是旋转血管造影技术和计算机三维图像处理技术的结合,能够更好地显示IAN的三维形态和空间关系。但是DSA属有创性检查,会引起一定的并发症,而且费用高。随着CT及MRI等的发展,多层螺旋CT血管成像(computed tomographic angiography,CTA)、MR血管成像(magnetic resonance angiography,MRA)等对IAN的检出率越来越接近DSA,能够更清晰地显示IAN的比邻关系,而且是无创性检查[3]。因此,本研究采用Meta分析对不同类型CTA、MRA诊断IAN的准确率进行全面地评价,同时采用间接比较的方法分析不同类型的CTA、MRA等在诊断IAN方面的差异,以期为IAN的正确诊断、及时治疗及预后评估等提供合理的依据。
-
由2名研究者在PubMed(1966年1月至2018年1月)、EMbase(1974年1月至2018年1月)、Cochralle图书馆(2018年第1期)和中国知网(1994年1月至2018年1月)、中国生物医学文献数据库(1978年1月至2018年1月)、维普网(1989年1月至2011年12月)、万方数据库(1997年1月至2018年1月)等平台进行计算机检索。参考《The Bayes Library of Diagnostic Studies and Reviews》[3],将检索词分为目标疾病、待评价试验、诊断准确性指标3部分,中文检索词包括:“颅内动脉瘤”、“计算机体层摄影术”、“CT血管成像”、“磁共振血管成像”、“MR血管成像”等。英文检索词包括:“Intracranial aneurysm”,“Computer tomography angiography”,“CT angiography”,“CTA”,“Magnetic resonance angiography”,“MR angiography”,“MRA”,“Intracranial aneurysms”等。检索文种包括中文和英文。同时运用Google Scholar等搜索引擎在互联网上查找相关文献,并追溯已纳入文献的参考文献,扩大检索范围。
-
纳入标准:①有关CTA、MRA诊断IAN的文献,无前瞻性或回顾性研究限制。②疑似有IAN的患者。③诊断方法包括待评价研究为CTA、MRA,无类型和磁场强度限制,以2D-DSA和(或)3D-DSA为比较标准。④测量指标包括验前概率、验后概率、合并阳性似然比(positive likelihood ratio,PLR合并)、合并阴性似然比(negative likelihood ratio,NLR合并)、诊断比值比(diagnosis odds ratio,DOR)、合并灵敏度(sensitivity,SEN合并)、合并特异度(specificity,SPE合并)、综合受试者工作特征(summary receiver operating characteristic,SROC)曲线的曲线下面积(area under curve,AUC)等。
排除标准:①疾病已确诊或已知的研究;②无法提取数据的研究;③对照非“金标准”或不只“金标准”的研究;④非诊断性研究;⑤数据重复的研究。
-
由2名研究者按照纳入、排除标准独立筛选文献,资料提取表提取信息内容主要包括:①纳入研究的一般特征,包括第一作者、发表时间、国家、仪器型号、研究类型(前瞻性或回顾性);②研究对象的基本特征,包括参考标准、样本量及四格表数据(真阳性、假阳性、假阴性、真阴性)。
-
质量评价采用诊断准确性试验质量评价工具(quality assessment of diagnostic accuracy studies,QUADAS)2评分标准[4],并根据Cochrane协作网诊断性试验系统评价方法学部分,采用其中11个评价条目进行文献的质量评估,对每项研究逐条按照“是”、“否”以及“不清楚”进行评价。具体评价条目(1~11)依次为:疾病谱组成、病例选择标准、疾病进展偏倚、部分参照偏倚、多重参照偏倚、混合偏倚、试验解读偏倚、“金标准”解读偏倚、临床解读偏倚、难以解释的试验结果、退出病例评价。
-
采用Stata 12.0统计分析软件绘制Deek's漏斗图评估纳入文献的发表偏倚。采用Meta-disc1.4统计分析软件计算纳入文献的SEN合并、SEP合并、DOR、PLR合并、NLR合并及95%CI,绘制SROC曲线并计算AUC。通过Q检验和I2进行异质性分析,P>0.05且I2<50%为研究结果间不存在异质性,采用固定效应模型进行数据合并分析;P<0.05且I2>50%为研究结果间存在异质性,采用随机效应模型进行分析。P<0.05表示差异有统计学意义。
-
初步检索获得相关文献1754篇,导入Endnote X7软件去重后剩余1022篇,通过阅读题目和摘要后排除与本研究纳入标准不符的文献271篇,初筛后符合标准的文献155篇,再按纳入标准及数据完整性进行筛选,最终纳入38篇诊断研究文献。
-
纳入38篇CTA、MRA诊断IAN的临床研究文献[5-42],共5212例患者。其中中文文献27篇、英文文献11篇。前瞻性研究22篇,回顾性研究8篇,未明确研究类型的8篇。纳入的38篇文献中,应用CTA诊断IAN的文献26篇,其中16层螺旋CTA 4篇、64层螺旋CTA 5篇、128层螺旋CTA 6篇、256层螺旋CTA 2篇、双源CTA(dual-energy CTA,DE CTA) 4篇、多层螺旋CTA 1篇和单纯CTA 4篇;应用不同类型MRA诊断IAN的文献19篇,其中三维时间飞跃法MRA(three-dimensional time of flight MRA,3D-TOF MRA)12篇、对比增强MRA(contrast enhancement MRA,CE-MRA)2篇、单纯MRA 5篇,同时包含3D-TOF MRA及CE-MRA的文献1篇;不同MRA磁场强度的文献总数为16篇,其中1.5 T 6篇、3.0 T 9篇、0.5 T 1篇;同时应用CTA和MRA诊断IAN的文献4篇。
-
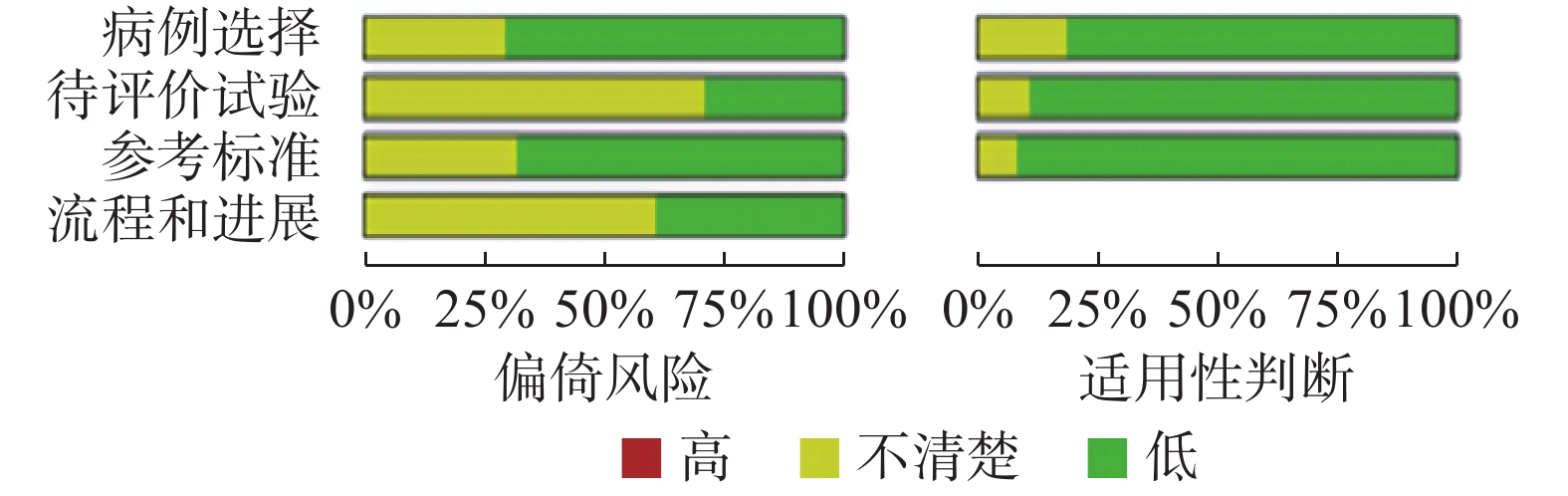
根据QUADAS-2质量评价标准对纳入的38个研究进行质量评价:①病例选择方面,有8个研究未涉及,2个研究为“否”;②待评价试验方面,有22个研究未涉及;③参考标准方面,有9个研究未涉及,1个研究为“否”;④病例流程和进展情况方面(待评价试验和参考标准之间是否有恰当的时间间隔),有17个研究未涉及。具体评价结果见图1。由图1可以看出所纳入的文献质量一般。
图 1 CT血管成像和MR血管成像纳入研究质量评估的风险构成比图
Figure 1. Chart of risk composition for quality assessment of studies included in CT angiography and MR angiography
-
①采用随机效应模型汇总分析,Meta分析结果显示:CTA诊断IAN的SEN合并为0.947、SPE合并为0.916、DOR为195.328(95%CI:97.367,391.847)、PLR合并为11.218(95%CI:6.861,18.341)、NLR合并为0.057 (95%CI:0.040,0.082),验前概率和验后概率分别为20%和74%,ROC曲线的AUC为0.98(95% CI:0.96,0.99)。MRA诊断IAN的SEN合并为0.935、SPE合并为0.956、AUC为0.98(95% CI:0.97,0.99)。由此可见,CTA、MRA诊断IAN的漏诊率均较低,且诊断准确率均较高(表1)。
类型 SEN合并(95%CI) SPE合并(95%CI) PLR合并(95%CI) NLR合并(95%CI) DOR(95%CI) 验前概率(%) 验后概率(%) CTA 0.947(0.926, 0.963) 0.916(0.864, 0.949) 11.218(6.861, 18.341) 0.057(0.040, 0.082) 195.328(97.367, 391.847) 20 74 MRA 0.935(0.899, 0.958) 0.956(0.917, 0.977) 21.285(11.114, 40.766) 0.068(0.044, 0.107) 311.421(126.935, 764.038) 20 84 注:表中,CTA:CT血管成像;MRA:磁共振血管成像;IAN:颅内动脉瘤;SEN合并:合并灵敏度;CI:可信区间;SPE合并:合并特异度;PLR合并:合并阳性似然比;NLR合并:合并阴性似然比;DOR:诊断比值比。 表 1 CTA、MRA诊断IAN的Meta分析结果
Table 1. Meta analysis results of CT angiography and MR angiography in the diagnosis of intracranial aneurysm disease
②分别以不同类型CTA、MRA诊断IAN为分析单位,亚组分析结果显示:不同类型CTA、MRA诊断IAN的SEN合并、SPE合并、PLR合并、NLR合并、验前概率、验后概率之间的差异无统计学意义,这表明不同类型CTA与MRA诊断IAN的准确率基本一致,二者均可以用来诊断IAN,且CTA和MRA诊断准确率均较高(表2)。
亚型 文献
篇数SEN合并(95%CI) SPE合并(95%CI) PLR合并(95%CI) NLR合并(95%CI) DOR(95%CI) 验前概
率(%)验后概
率(%)CTA类型 16层螺旋CTA 4 0.953
(0.916, 0.975)0.967
(0.798, 0.995)28.604
(4.163, 196.525)0.048
(0.026, 0.088)594.491
(73.379, 4816.364)20 88 64层螺旋CTA 5 0.968
(0.936, 0.984)0.920
(0.630, 0.987)12.096
(2.085, 70.178)0.035
(0.017, 0.073)347.788
(42.119, 2871.749)20 75 256层螺旋CTA 2 0.928
(0.868, 0.967)0.762
(0.528, 0.918)3.835
(0.184, 79.766)0.100
(0.050, 0.202)28.324
(2.333, 343.890)− − 128排螺旋CTA 6 0.938
(0.885, 0.968)0.958
(0.820, 0.991)22.425
(4.669, 107.698)0.064
(0.033, 0.127)348.032
(45.280, 2675.042)20 85 DE CTA 4 0.812
(0.766, 0.851)0.813
(0.707, 0.894)5.687
(1.478, 21.883)0.133
(0.037, 0.471)49.441
(4.685, 521.700)− − MRA类型 3D-TOF MRA 12 0.941
(0.901, 0.966)0.963
(0.922, 0.983)25.170
(11.749, 53.920)0.061
(0.036, 0.105)412.212
(141.521, 1200.661)20 86 CE-MRA 2 0.949
(0.874, 0.986)0.800
(0.614, 0.923)4.734
(2.307, 9.713)0.064
(0.024, 0.172)72.347
(17.108, 305.950)− − 注:表中,CTA:CT血管成像;MRA:磁共振血管成像;SEN合并:合并灵敏度;CI:可信区间;SPE合并:合并特异度;PLR合并:合并阳性似然比;NLR合并:合并阴性似然比;DOR:诊断比值比;DE CTA:双能CT血管成像;3D-TOF MRA:三维时间飞跃法磁共振血管成像;CE-MRA:对比增强磁共振血管成像;−:无此数据。 表 2 不同类型CTA和MRA亚组的Meta分析结果
Table 2. Meta analysis results of different types of CT angiography and MR angiography subtypes
-
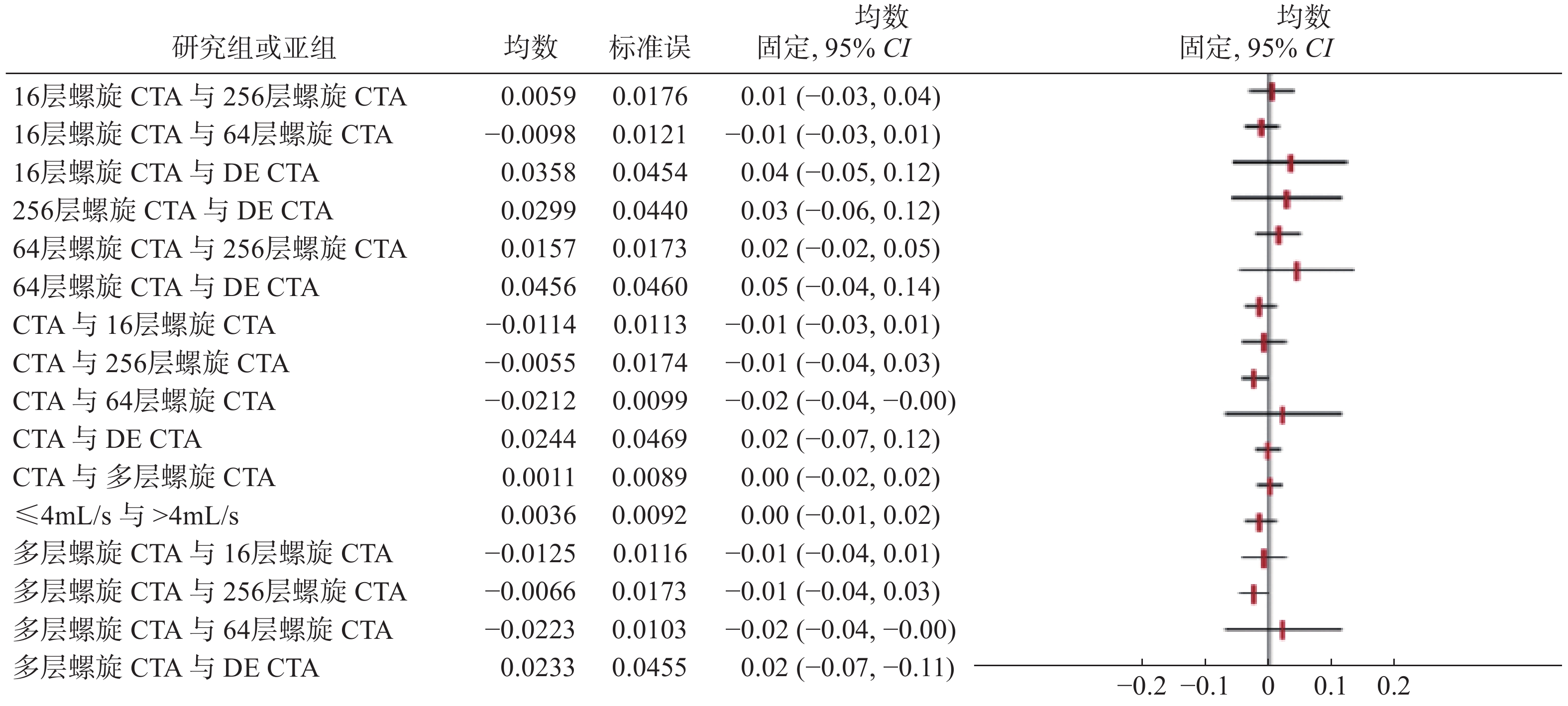
CTA、多层螺旋CTA、16层螺旋CTA、64层螺旋CTA、256层螺旋CTA和DE CTA诊断IAN的AUC之间的差异均无统计学意义(图2)。将CTA对比剂的注射流率分成≤4 mL/s和>4 mL/s两部分,结果显示不同类型对比剂不同注射流率的AUC之间的差异均无统计学意义(图2)。
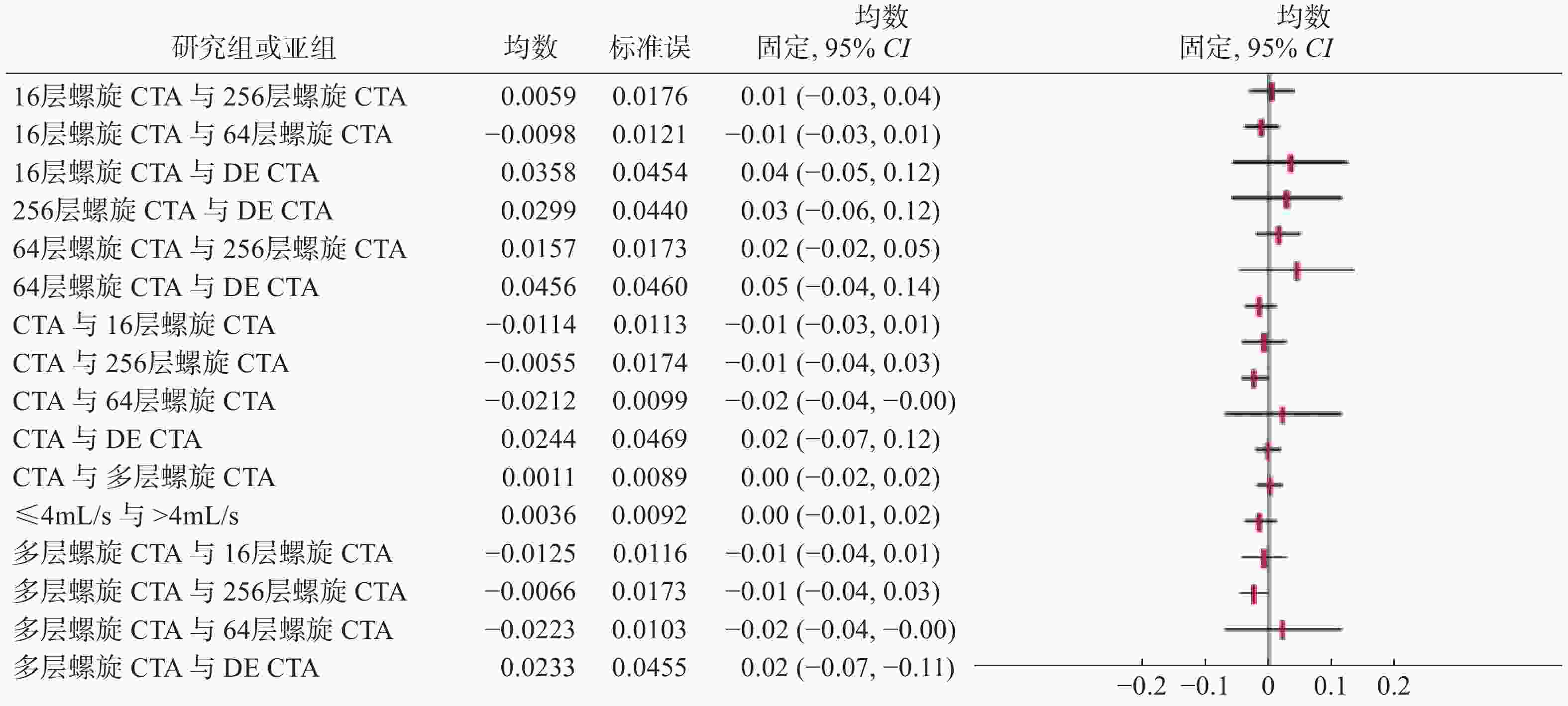
图 2 不同类型CTA及CTA对比剂不同注射流率的间接比较
Figure 2. Indirect comparison of velocity of different CT angiography types and CT angiography comparison materials
-
磁场强度分别为1.5T和3.0T MRA诊断IAN的AUC之间的差异均无统计学意义(图3)。

图 3 不同磁场强度MRA的间接比较
Figure 3. Indirect comparison of MR angiography with different magnetic field intensity
-
以有效样本量的平方根的倒数为横坐标,DOR(ln DOR)为纵坐标绘制漏斗图,CTA的斜率系数为−1.46,P=0.155>0.05 [t=−1.46,95%CI(−22.808,3.785)],这说明存在发表偏倚的可能性较小;MRA的斜率系数为−5.89,P<0.001 [t=−5.98,95%CI(−61.209,−29.733)],这说明存在发表偏倚的可能性较大(图4)。
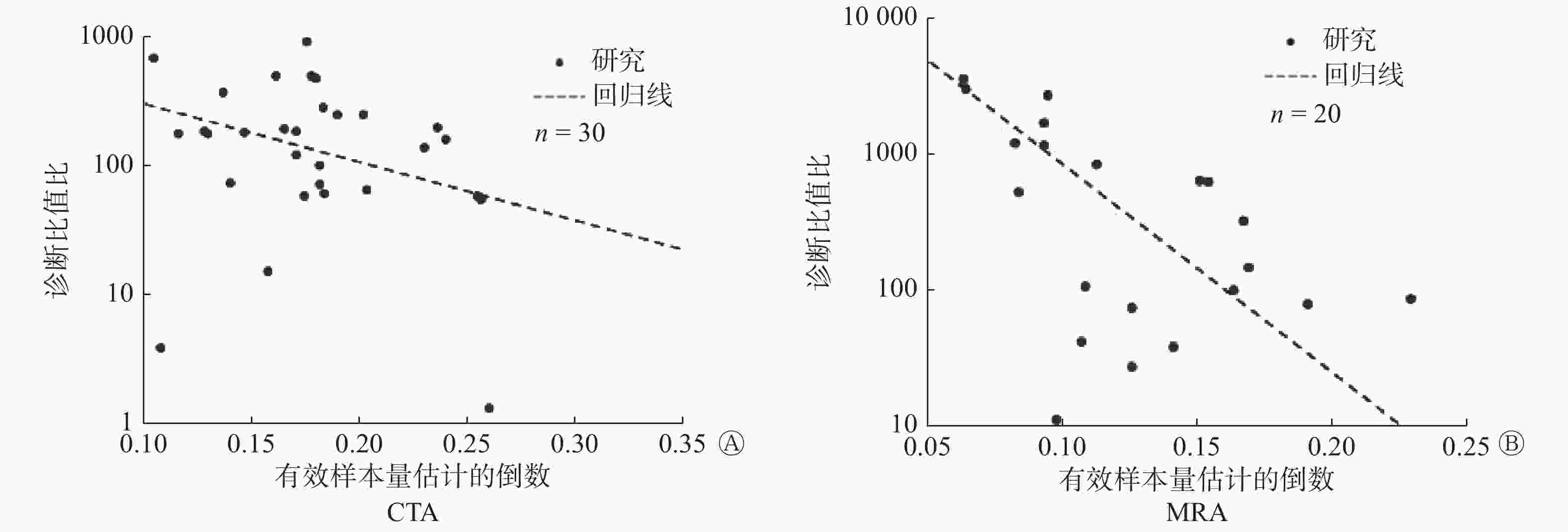
图 4 CTA 和MRA纳入文献发表偏倚的Deck's漏斗图
Figure 4. Deck's funnel plot of publication bias for CT angiography and MR angiography literature
-
IAN患者的颅内局部动脉血管发生了瘤样突起,未破裂者通常无明显症状,但当动脉瘤直径超过7 mm时可出现局部压迫感,破裂后易导致蛛网膜下腔出血,致使病死率和致残率升高[43]。因此,及时正确诊断对IAN患者的治疗和康复有重要意义。CTA、MRA检查为无创性检查,CTA经血管注入造影剂后进行CT成像,可以获得清晰的颅内血管图像。MRA利用电磁波可重建患者的身体情况,可避免颅底骨和海绵窦等的干扰,对诊断IAN具有很高的临床价值[44]。
本研究Meta分析结果显示:①CTA诊断IAN的SEN合并为94.7%、SPE合并为91.6%,这说明其漏诊率和误诊率均较低;PLR合并为11.218>5,这表明CTA结果为阳性时,患IAN的可能性大,NLR合并为0.057<0.2,这表明CTA结果为阴性时,基本可以排除疑似IAN的可能性;CTA的验后概率(74%)相对验前概率(20%)提高较多,这说明CTA用于诊断IAN是有效的。本研究CTA诊断IAN的ROC曲线的AUC为0.98,接近1,这说明诊断的准确率较高,CTA对IAN有一定的价值。②MRA诊断IAN的SEN合并为93.5%、SPE合并为95.6%,显示其漏诊率和误诊率较低;PLR合并为21.285>5,表明MRA结果为阳性时,有患IAN的可能性,NLR合并为0.068<0.2,表明MRA结果为阴性时,基本可以排除疑似IAN的可能性;MRA的验后概率(84%)相对验前概率(20%)提高较多,这说明MRA用于诊断IAN是有效的;MRA诊断IAN的ROC曲线的AUC为0.98,接近1,这说明诊断的准确率较高,MRA对IAN有一定的价值。由此可见,CTA的准确率与MRA的准确率基本一致,二者均可以用来诊断IAN,且CTA和MRA的诊断准确率均较高。
本研究的优势:①同时分析了CTA、MRA诊断IAN的准确率;②采用间接比较的方法分析了不同类型CTA、不同类型MRA及不同磁场强度MRA诊断IAN的准确率,并且还对CTA对比剂不同注射流率是否对结果有影响进行了分析;③不但呈现了SEN合并、SEP合并、DOR、PLR合并、NLR合并、SROC这些基础结果,还加入了验前概率、验后概率、AUC,提高了可信度。
本研究的局限性:①本研究在CTA、MRA方面的异质性均较高,故采用了亚组分析,但MRA的亚组因资料提取不足仅有两组,而全面分析异质性的来源需要更多的亚组数据;②有一部分纳入研究在表述诊断结果时不统一,阴性结果采用患者数进行报告而阳性结果采用瘤数;③有大部分研究未报告待评价试验阈值及诊断试验与参考标准检测的间隔时间;④MRA存在发表偏倚。因此,建议今后研究:①尽量遵循诊断准确性研究摘要报告规范(STARD),提高诊断性试验报告的质量;②尽量选取设计良好的研究,纳入充足的数据进行分析;③文献信息应报告完整,方便实际应用或为医疗决策提供参考;④诊断性试验和参考标准尽量同步进行,诊断时采用“双盲法”评估;⑤尽可能采用前瞻性研究,以避免回顾性偏倚的影响。
本研究Meta分析结果提示:CTA和MRA对IAN诊断均有相对较高的灵敏度和特异度,且SROC AUC相等,显示CTA和MRA作为无创性检查对IAN具有较高的准确性且诊断效能较为一致。虽然之前有Meta分析提示CTA对于IAN的诊断价值均高于MRA[45],但本研究通过大样本进一步研究证实CTA和MRA对IAN的诊断效能一致,均可作为首选诊断方法。因此,临床医师可以选择无创的CTA或MRA来诊断IAN,具体选择可结合医院及患者自身情况,旨在做出性价比高的诊断决策。
利益冲突 本研究由署名作者按以下贡献声明独立开展,不涉及任何利益冲突。
作者贡献声明 王道英负责本研究命题的提出、设计及论文的撰写;李海洋、王海军负责文献的检索、查重及筛选;李星辉负责资料的提取及统计学的分析;田金徽负责资料、结果的审核及论文的校对。
不同类型CT和MR血管成像诊断颅内动脉瘤准确率的Meta分析
Diagnostic accuracy of different types of computed tomographic angiography and magnetic resonance angiography for intracranial aneurysm: a Meta-analysis
-
摘要:
目的 分析评价不同类型CT血管成像(CTA)和MR血管成像(MRA)诊断颅内动脉瘤(IAN)的准确率。 方法 检索PubMed、EMbase、Cochralle图书馆和中国知网、中国生物医学文献数据库、维普网、万方数据库,收集2018年1月以前有关不同类型CTA和MRA诊断IAN的中、英文文献,按照诊断性研究的纳入标准筛选文献,并依据诊断准确性试验质量评价工具2标准进行质量评价。采用Stata 12.0及Meta-Disc 1.4软件对纳入的文献进行Meta分析,分别比较CTA、MRA及亚组之间的合并灵敏度(SEN合并)、合并特异度(SPE合并)、诊断比值比(DOR)、合并阳性似然比(PLR合并)、合并阴性似然比(NLR合并)、验前概率和验后概率等性能指标,绘制森林图和综合受试者工作特征(SROC)曲线并计算曲线下面积(AUC)。采用Stata 12.0统计分析软件绘制Deek's漏斗图评估纳入文献的发表偏倚。通过Q检验和I2进行异质性分析。 结果 检索获得1754篇文献,最终纳入38篇临床诊断研究,包括5212例患者。Meta分析结果显示:①CTA诊断IAN的SEN合并、SPE合并、DOR、PLR合并、NLR合并、AUC、验前概率和验后概率分别为0.947(95%CI:0.926,0.963)、0.916(95%CI:0.864,0.949)、195.328(95%CI:97.367,391.847)、11.218(95%CI:6.861,18.341)、0.057(95%CI:0.040,0.082)、0.98(95%CI:0.96,0.99)、20%和74%;②MRA诊断IAN的SEN合并、SPE合并、DOR、PLR合并、NLR合并、AUC、验前概率和验后概率分别为0.935(95%CI:0.899,0.958)、0.956(95%CI:0.917,0.977)、311.421(95%CI:126.935,764.038)、21.285(95%CI:11.114,40.766)、0.068(95%CI:0.044,0.107)、0.98(95%CI:0.97,0.99)、20%和84%;③亚组分析结果显示:不同类型的CTA和MRA诊断IAN之间AUC的差异均无统计学意义。 结论 不同类型CTA与MRA均可以诊断IAN,诊断准确性均较高且基本一致,CTA和MRA均可作为诊断IAN的首选检查手段。 -
关键词:
- 计算机体层摄影血管造影术 /
- 磁共振血管造影术 /
- 颅内动脉瘤 /
- Meta分析
Abstract:Objective To perform a Meta-analysis to systematically review the accuracy different types of computed tomographic angiography (CTA) and magnetic resonance angiography (MRA) for intracranial aneurysm (IAN). Methods PubMed, EMbase, Cochralle library, Cnki, China biomedical literature database, weipu, wanfang and other databases were searched to collect Chinese and English literatures on IAN diagnosis by different types of CTA and MRA before January 2018.The references were evaluated and screened according to the criteria of diagnostic research. In addition, quality assessment was conducted according to the Quality Assessment of Diagnostic Accuracy Studies 2, RevMan 5.3 and Metadisc 1.4 software was used to respectively compare the summary sensitivity (SEN), summary specificity (SPE), diagnostic odds ratio (DOR), summary positive likelihood ratio (PLR), summary negative likelihood ratio (NLR), pre-test probability, post-test probability between CTA, MRA and subgroup. The forest figure and a summary of receiver operating characteristic curve (SROC) was drawn out and the area under curve (AUC) was calculated. Deek's funnel plot was drawn by Stata 12.0 statistical analysis software to evaluate the publication bias of included literature. Heterogeneity was analyzed by Q test and I2. P<0.05 indicated that the difference was statistically significant. Results A total of 1754 records was retrieved and 38 studies involving 5212 patients were included. The results of meta-analysis showed that: ① The summary SEN, summary SPE, DOR, summary PLR, summary NLR, AUC, pre-test probability, post-test probability of CTA were: 0.947 (95%CI: 0.926, 0.963), 0.916 (95%CI: 0.864, 0.949), 195.328 (95%CI: 97.367, 391.847), 11.218 (95%CI: 6.861, 18.341), 0.057 (95%CI: 0.040, 0.082), 0.98 (95%CI: 0.96, 0.99), 20% and 74%; ② The summary SEN, summary SPE, DOR, summary PLR, summary NLR, AUC, pre-test probability, post-test probability of MRA were: 0.935 (95%CI: 0.899, 0.958), 0.956 (95%CI: 0.917, 0.977), 311.421 (95%CI:126.935, 764.038), 21.285 (95%CI: 11.114, 40.766), 0.068 (95%CI: 0.044, 0.107), 0.98 (95%CI: 0.97, 0.99), 20% and 84%; ③ The results of subgroup analysis showed that: there were no statistical difference between the different types of CTA and MRA in SROC. Conclusions The different types of CTA and MRA can be used to diagnose IAN, and the diagnostic accuracy is relatively high and basically consistent. Both CTA and MRA can be used as the first choice for diagnosing IAN. -
图 1 CT血管成像和MR血管成像纳入研究质量评估的风险构成比图
Figure 1. Chart of risk composition for quality assessment of studies included in CT angiography and MR angiography
图 2 不同类型CTA及CTA对比剂不同注射流率的间接比较
Figure 2. Indirect comparison of velocity of different CT angiography types and CT angiography comparison materials
图 3 不同磁场强度MRA的间接比较
Figure 3. Indirect comparison of MR angiography with different magnetic field intensity
图 4 CTA 和MRA纳入文献发表偏倚的Deck's漏斗图
Figure 4. Deck's funnel plot of publication bias for CT angiography and MR angiography literature
表 1 CTA、MRA诊断IAN的Meta分析结果
Table 1. Meta analysis results of CT angiography and MR angiography in the diagnosis of intracranial aneurysm disease
类型 SEN合并(95%CI) SPE合并(95%CI) PLR合并(95%CI) NLR合并(95%CI) DOR(95%CI) 验前概率(%) 验后概率(%) CTA 0.947(0.926, 0.963) 0.916(0.864, 0.949) 11.218(6.861, 18.341) 0.057(0.040, 0.082) 195.328(97.367, 391.847) 20 74 MRA 0.935(0.899, 0.958) 0.956(0.917, 0.977) 21.285(11.114, 40.766) 0.068(0.044, 0.107) 311.421(126.935, 764.038) 20 84 注:表中,CTA:CT血管成像;MRA:磁共振血管成像;IAN:颅内动脉瘤;SEN合并:合并灵敏度;CI:可信区间;SPE合并:合并特异度;PLR合并:合并阳性似然比;NLR合并:合并阴性似然比;DOR:诊断比值比。  下载: 导出CSV
下载: 导出CSV
表 2 不同类型CTA和MRA亚组的Meta分析结果
Table 2. Meta analysis results of different types of CT angiography and MR angiography subtypes
亚型 文献
篇数SEN合并(95%CI) SPE合并(95%CI) PLR合并(95%CI) NLR合并(95%CI) DOR(95%CI) 验前概
率(%)验后概
率(%)CTA类型 16层螺旋CTA 4 0.953
(0.916, 0.975)0.967
(0.798, 0.995)28.604
(4.163, 196.525)0.048
(0.026, 0.088)594.491
(73.379, 4816.364)20 88 64层螺旋CTA 5 0.968
(0.936, 0.984)0.920
(0.630, 0.987)12.096
(2.085, 70.178)0.035
(0.017, 0.073)347.788
(42.119, 2871.749)20 75 256层螺旋CTA 2 0.928
(0.868, 0.967)0.762
(0.528, 0.918)3.835
(0.184, 79.766)0.100
(0.050, 0.202)28.324
(2.333, 343.890)− − 128排螺旋CTA 6 0.938
(0.885, 0.968)0.958
(0.820, 0.991)22.425
(4.669, 107.698)0.064
(0.033, 0.127)348.032
(45.280, 2675.042)20 85 DE CTA 4 0.812
(0.766, 0.851)0.813
(0.707, 0.894)5.687
(1.478, 21.883)0.133
(0.037, 0.471)49.441
(4.685, 521.700)− − MRA类型 3D-TOF MRA 12 0.941
(0.901, 0.966)0.963
(0.922, 0.983)25.170
(11.749, 53.920)0.061
(0.036, 0.105)412.212
(141.521, 1200.661)20 86 CE-MRA 2 0.949
(0.874, 0.986)0.800
(0.614, 0.923)4.734
(2.307, 9.713)0.064
(0.024, 0.172)72.347
(17.108, 305.950)− − 注:表中,CTA:CT血管成像;MRA:磁共振血管成像;SEN合并:合并灵敏度;CI:可信区间;SPE合并:合并特异度;PLR合并:合并阳性似然比;NLR合并:合并阴性似然比;DOR:诊断比值比;DE CTA:双能CT血管成像;3D-TOF MRA:三维时间飞跃法磁共振血管成像;CE-MRA:对比增强磁共振血管成像;−:无此数据。
下载: 导出CSV
-
[1] 王茂雪, 李明泉, 罗松. Meta分析评价双能量头颅CTA诊断颅内动脉瘤准确性[J]. 中国医学影像技术, 2018, 34(1): 35−38. DOI: 10.13929/j.1003−3289.201704006.
Wang MX, Li MQ, Luo S. Diagnostic accuracy of dual-energy CT angiography in patients with intracranial aneurysm: Meta-analysis[J]. Chin J Med Imaging Technol, 2018, 34(1): 35−38. DOI: 10.13929/j.1003−3289.201704006.[2] Macdonald RL, Schweizer TA. Spontaneous subarachnoid haemorrhage[J]. Lancet, 2017, 389(10069): 655−666. DOI: 10.1016/S0140−6736(16)30668−7. [3] Josephson CB, White PM, Krishan A, et al. Computed tomography angiography or magnetic resonance angiography for detection of intracranial vascular malformations in patients with intracerebral aemorrhage[J/OL].Cochrane Database Syst Rev, 2014, 1(9): CD009372[2018-10-24]. 10.1002/14651858.CD009372.pub2/full">https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD009372.pub2/full. DOI: 10.1002/14651858.CD009372.pub2. [4] 刘鸣. 系统评价、Meta-分析设计与实施方法[M]. 北京: 人民卫生出版社, 2011: 73−74.
Liu M. Design and implementation methods of systematic evaluation and meta-analysis[M]. Beijing: People's Medical Publishing House, 2011: 73−74.[5] 晋晖, 徐红卫, 程敬亮, 等. 3.0 T磁共振3D-TOF-MRA对颅内微小动脉瘤的诊断价值[J]. 重庆医学, 2015, 44(27): 3842−3844. DOI: 10.3969/j.issn.1671−8348.
Jin H, Xu HW, Cheng JL, et al. The diagnostic value of 3.0 T magnetic resonance 3D-TOF-MRA in intracranial micro aneurysms[J]. Chongqing Med, 2015, 44(27): 3842−3844. DOI: 10.3969/j.issn.1671−8348.[6] 何文根, 谭显西, 赵兵, 等. 3D-CTA、3D-DSA对颅内动脉瘤临床诊断价值的对比[J]. 国际神经病学神经外科学杂志, 2010, 37(3): 191−195.
He WG, Tan XX, Zhao B, et al. Detection of aneurysms by 3D-CTA in patients acutely suspected of having a intracranial aneurysm and comparison with 3D-DSA[J]. J Int Neurol Neurosurg, 2010, 37(3): 191−195.[7] 程英, 蔡新琦, 郑伟武, 等. 64层螺旋CT脑动脉瘤血管成像的应用研究[J]. 解剖与临床, 2010, 15(1): 33−35.
Cheng Y, Cai XQ, Zheng WW, et al. Detection of Cerebral Aneurysms with 64-slice Spiral CT Angiography[J]. Anat Clin, 2010, 15(1): 33−35.[8] 陈圣攀, 张波, 叶明, 等. CTA与MRA对颅内动脉瘤诊断价值探讨[J]. 潍坊医学院学报, 2016, 38(2): 87−89.
Chen SP, Zhang B, Ye M, et al. Evaluation of CTA and MRA in Diagnosis of Intracranial Aneurysms[J]. Acta Acad Med Weifang, 2016, 38(2): 87−89.[9] 赵年. CT血管造影对脑动脉瘤患者的诊断价值[J]. 广西医科大学学报, 2015, 32(6): 964−965.
Zhao N. CT angiography in the diagnosis of cerebral aneurysms[J]. Acta Guangxi Med Univ, 2015, 32(6): 964−965.[10] 赵东生, 李竹强, 乔海舟, 等. DE-CTA与MRA用于颅内动脉瘤诊断的临床价值比较[J]. 临床合理用药杂志, 2015, 8(3A): 152−153.
Zhao DS, Li ZQ, Qiao HZ, et al. Comparison of the clinical value of DE-CTA and MRA in the diagnosis of intracranial aneurysms[J]. Chin J Clin Ration Drug Use, 2015, 8(3A): 152−153.[11] 陈光文, 印隆林, 李迎春, 等. DSCTA和3.0 T MRA评价颅内动脉瘤的对比研究[J]. 生物医学工程学杂志, 2013, 30(5): 993−998.
Chen GW, Yin LL, Li YC, et al. Comparative Analysis of Dual Resource Computed Tomography Angiography and 3.0 T Magnetic Resonance Angiography in the Diagnosis of Intracranial Aneurysms[J]. J Biomed Eng, 2013, 30(5): 993−998.[12] 盛亮, 陈建华, 陈洁, 等. 多层螺旋CT血管成像诊断颅内动脉瘤的临床价值[J]. 实用医学杂志, 2008, 24(9): 1554−1555. DOI: 10.3969/j.issn.1006−5725.2008.09.035.
Sheng L, Chen JH, Chen J, et al. Clinical value of multislice spiral CT angiography in diagnosing intracranial aneurysms[J]. J Pract Med, 2008, 24(9): 1554−1555. DOI: 10.3969/j.issn.1006−5725.2008.09.035.[13] 陆明, 王健, 李传明, 等. 双源CT血管成像与数字减影血管成像对颅内动脉瘤的评价[J]. 中国医学科学院学报, 2010, 32(6): 615−618. DOI: 10.3881/j.issn.1000−503X.2010.06.005.
Lu M, Wang J, Li CM, et al. Evaluation of Intracranial Aneurysms Using Dual-source Computed Tomographic Angiography and Digital Subtraction Angiography[J]. Acta Acad Med Sin, 2010, 32(6): 615−618. DOI: 10.3881/j.issn.1000−503X.2010.06.005.[14] 章永强, 赵海玲, 江晓勇, 等. 三维时间飞跃法MRA筛选温岭社区人群颅内动脉瘤研究[J]. 介入放射学杂志, 2015, 24(12): 1039−1042. DOI: 10.3969/j.issn.1008−794X.2015.12.003.
Zhang YQ, Zhao HL, Jiang XY, et al. 3D-TOF MRA screening of intracranial aneurysms in the population of Wenling community[J]. J Intervent Radiol, 2015, 24(12): 1039−1042. DOI: 10.3969/j.issn.1008−794X.2015.12.003.[15] 张恒, 马长江, 李璐, 等. CT与MR诊断颅内动脉瘤敏感性和特异性对比[J]. 现代医用影像学, 2017, 26(3): 650−652.
Zhang H, Ma CJ, Li L, et al. The sensitivity and specificity of CT and MR in diagnosing intracranial aneurysms were compared[J]. Mod Med Imageol, 2017, 26(3): 650−652.[16] 张慧, 郭君武, 李杰. 双源CT在颅内动脉瘤诊断中的初步研究[J]. 中国实用神经疾病杂志, 2015, 18(14): 99−100. DOI: 10.3969/j.issn.1673−5110.2015.14.068.
Zhang H, Guo JW, Li J. A preliminary study of double-source CT in the diagnosis of intracranial aneurysms[J]. Chin J Pract Nerv Dis, 2015, 18(14): 99−100. DOI: 10.3969/j.issn.1673−5110.2015.14.068.[17] 许云飞, 尉传社, 王峥超, 等. 3.0 T三维时间飞越法MRA对颅内动脉瘤的诊断价值[J]. 现代医药卫生, 2007, 23(23): 3480−3482. DOI: 10.3969/j.issn.1009−5519.2007.23.003.
Xu YF, Wei CS, Wang ZC, et al. The diagnostic value of 3.0 T three-dimensional time of flight magnetic resonance angiography in intracranial aneurysms[J]. Mod Med Health, 2007, 23(23): 3480−3482. DOI: 10.3969/j.issn.1009−5519.2007.23.003.[18] 张鹤, 李明华, 方淳, 等. 3.0 T时间飞跃法MRA诊断颅内动脉瘤− 与DSA对照[J]. 介入放射学杂志, 2008, 17(9): 618−622. DOI: 10.3969/j.issn.1008−794X.2008.09.003.
Zhang H, Li MH, Fang C, et al. Detection of intracranial aneurysm with time-of-flight MRA at 3.0 Tesla: comparison with digital subtraction angiography[J]. J Intervent Radiol, 2008, 17(9): 618−622. DOI: 10.3969/j.issn.1008−794X.2008.09.003.[19] 张政, 韩剑虹, 李迎春, 等. 256层螺旋CT三维血管成像与三维DSA诊断颅内动脉瘤的对比分析[J]. 中国脑血管病杂志, 2012, 9(1): 21−26. DOI: 10.3969/j.issn.1672−5921.2012.01.005.
Zhang Z, Han JH, Li YC, et al. Comparative analysis of 256-slice CT angiography and 3D digital subtraction angiography in the diagnosis of intracranial aneurysms[J]. Chin J Cerebrovas Dis, 2012, 9(1): 21−26. DOI: 10.3969/j.issn.1672−5921.2012.01.005.[20] 刘献伟, 杨小庆, 刘文, 等. 3D-TOF-MRA最大密度投影法与多平面重建法对颅内动脉瘤的诊断价值[J]. 中外医学研究, 2012, 10(13): 1−2. DOI: 10.3969/j.issn.1674−6805.2012.13.001.
Liu XW, Yang XQ, Liu W, et al. The Value of MIP and MPR in 3D TOF MRA to the Diagnosis of Cerebral Aneurysm[J]. Chin For Med Res, 2012, 10(13): 1−2. DOI: 10.3969/j.issn.1674−6805.2012.13.001.[21] 张荣恒, 高江晖, 马洪宇, 等. 16层螺旋CTA在急诊脑动脉瘤中的应用价值[J]. 中国伤残医学, 2014, 22(4): 46−47.
Zhang RH, Gao JH, Ma HY, et al. Value of applying 16-slice CTA to the diagnosis of acute cerebral aneurysm[J]. Chin J Trauma Disabil Med, 2014, 22(4): 46−47.[22] 罗贤斌. 16排螺旋CT在颅内动脉瘤中的诊断价值[J]. 当代医学, 2011, 17(36): 72−73. DOI: 10.3969/j.issn.1009−4393.2011.36.047.
Luo XB. Diagnostic value of 16- slice spiral CT in intracranial aneurysms[J]. Contemp Med, 2011, 17(36): 72−73. DOI: 10.3969/j.issn.1009−4393.2011.36.047.[23] 吕国士, 李庆春, 左宏, 等. 64层螺旋CT脑血管造影在颅内动脉瘤诊断中的应用[J]. 医学影像学杂志, 2007, 17(1): 7−10. DOI: 10.3969/j.issn.1006−9011.2007.01.003.
Lyu GS, Li QC, Zuo H, et al. Diagnotic application of intracranial aneurysm by 64-detector row CT angiography[J]. J Med Imaging, 2007, 17(1): 7−10. DOI: 10.3969/j.issn.1006−9011.2007.01.003.[24] 孙涛, 李宏, 包权. 64层螺旋CT血管造影术诊断颅内动脉瘤的临床应用价值[J]. 牡丹江医学院学报, 2008, 29(2): 61−63. DOI: 10.3969/j.issn.1001−7550.2008.02.037.
Sun T, Li H, Bao Q. Clinical value of 64-slice spiral CT angiography in the diagnosis of intracranial aneurysms[J]. J Mudanjiang Med Coll, 2008, 29(2): 61−63. DOI: 10.3969/j.issn.1001−7550.2008.02.037.[25] 王恒地, 赵永霞, 李增友. 64层螺旋CT血管造影在诊断颅内动脉瘤中的作用[J]. 中国辐射卫生, 2008, 17(3): 366−367. DOI: 10.3969/j.issn.1004−714X.2008.03.067.
Wang HD, Zhao YX, Li ZY. Role of 64-slice spiral CT angiography in the diagnosis of intracranial aneurysms[J]. Chin J Radiol Health, 2008, 17(3): 366−367. DOI: 10.3969/j.issn.1004−714X.2008.03.067.[26] 钱惠农, 王有刚, 朱蕴杰, 等. 64排螺旋CT血管造影诊断颅内动脉瘤[J]. 现代预防医学, 2009, 36(16): 3189−3191.
Qian HN, Wang YG, Zhu YJ, et al. Diagnosis of intracranial aneurysm with 64-slice spiral CT angiography[J]. Mod Prev Med, 2009, 36(16): 3189−3191.[27] 修俊刚, 刘剑, 江耿思, 等. 256层螺旋3D-CT血管造影与DSA对颅内动脉瘤诊断的对比研究[J]. 中国微侵袭神经外科杂志, 2012, 17(8): 347−349.
Xiu JG, Liu J, Jiang GS, et al. Comparative study of 256-slice spiral 3D-CT angiography and DSA in the diagnosis of intracranial aneurysms[J]. Chin J Minim Invasive Neurosurg, 2012, 17(8): 347−349.[28] 柏根基, 王煊. 颅内动脉瘤3D DCE-MRA与DSA对照研究[J]. 临床放射学杂志, 2008, 27(2): 160−162. DOI: 10.3969/j.issn.1001−9324.2008.02.005.
Bo GJ, Wang X. Comparative Study of Three Dimensional Dynamic Contrast Enhanced MR Angiography and Digital Subtraction Angiography for Intracranial Aneurysms[J]. J Clin Radiol, 2008, 27(2): 160−162. DOI: 10.3969/j.issn.1001−9324.2008.02.005.[29] 周孟, 刘筱霜, 肖艳, 等. 容积CT数字减影血管造影诊断颅内动脉瘤的价值及影响因素[J]. 中国医学影像技术, 2016, 32(5): 688−691. DOI: 10.13929/j.1003−3289.2016.05.014.
Zhou M, Liu XS, Xiao Y, et al. Value and factors affected efficiency of volume computed tomographic digital subtraction angiography in diagnosis of intracranial aneurysms[J]. Chin J Med Imaging Technol, 2016, 32(5): 688−691. DOI: 10.13929/j.1003−3289.2016.05.014.[30] 陈雄钊, 龙晚生, 李伟, 等. 头颅CT血管造影诊断颅内动脉瘤临床价值探讨[J]. 中国当代医药, 2013, 20(13): 114−115. DOI: 10.3969/j.issn.1674−4721.2013.13.055.
Chen XZ, Long WS, Li W, et al. Clinical value of cranial CT angiography in the diagnosis of intracranial aneurysms[J]. Chin Mod Med, 2013, 20(13): 114−115. DOI: 10.3969/j.issn.1674−4721.2013.13.055.[31] 韩磊, 王志刚, 丁璇, 等. 64排螺旋CT血管造影VR成像与DSA在颅内动脉瘤诊断中的对比研究[J]. 山东大学学报: 医学版, 2008, 46(3): 296−300.
Han L, Wang ZG, Ding X, et al. A comparison of volume rendering and digital subtraction angiography in the diagnosis of intracranial aneurysms[J]. J Shandong Univ: Health Sci, 2008, 46(3): 296−300.[32] Grandin CB, Mathurin P, Duprez T, et al. Diagnosis of intracranial aneurysms: accuracy of MR angiography at 0.5 T[J]. AJNR Am J Neuroradiol, 1998, 19(2): 245−252. [33] Chen YC, Sun ZK, Li MH, et al. The clinical value of MRA at 3.0 T for the diagnosis and therapeutic planning of patients with subarachnoid haemorrhage[J]. Eur Radiol, 2012, 22(7): 1404−1412. DOI: 10.1007/s00330−012−2390−9. [34] Li H, Yan L, Li MH, et al. Evaluation of intracranial aneurysms with high-resolution MR angiography using single-artery highlighting technique: correlation with digital subtraction angiography[J]. Radiol Med, 2013, 118(8): 1379−1387. DOI: 10.1007/s11547−012−0871−1. [35] Jayaraman MV, Mayo-Smith WW, Tung GA, et al. Detection of Intracranial Aneurysms: Multi-Detector Row CT Angiography Compared with DSA[J]. Radiology, 2004, 230(2): 510−518. DOI: 10.1148/radiol.2302021465. [36] Pierot L, Portefaix C, Rodriguez-Régent C, et al. Role of MRA in the detection of intracranial aneurysm in the acute phase of subarachnoid hemorrhage[J]. J Neuroradiol, 2013, 40(3): 204−210. DOI: 10.1016/j.neurad.2013.03.004. [37] Horikoshi T, Fukamachi A, Nishi H, et al. Detection of intracranial aneurysms by three-dimensional time-of-flight magnetic resonance angiography[J]. Neuroradiology, 1994, 36(3): 203−207. DOI: 10.1007/bf00588131. [38] Uysal E, Yanbuloğlu B, Ertürk M, et al. Spiral CT angiography in diagnosis of cerebral aneurysms of cases with acute subarachnoid hemorrhage[J]. Diagn Interv Radiol, 2005, 11(2): 77−82. [39] Ramasundara S, Mitchell PJ, Dowling RJ. Bone subtraction CT angiography for the detection of intracranial aneurysms[J]. J Med Imaging Radiat Oncol, 2010, 54(6): 526−533. DOI: 10.1111/j.1754−9485.2010.02211.x. [40] Metens T, Rio F, Balériaux D, et al. Intracranial Aneurysms: Detection with Gadolinium-Enhanced Dynamic Three-dimensional MR Angiography-Initial Results[J]. Radiology, 2000, 216(1): 39−46. DOI: 10.1148/radiology.216.1.r00jl1139. [41] Xing W, Chen WH, Sheng J, et al. Sixty-Four-Row Multislice Computed Tomographic Angiography in the Diagnosis and Characterization of Intracranial Aneurysms: Comparison with 3D Rotational Angiography[J]. World Neurosurg, 2011, 76(1/2): 105−113. DOI: 10.1016/j.wneu.2011.01.046. [42] Lenhart M, Bretschneider T, Gmeinwieser J, et al. Cerebral CT angiography in the diagnosis of acute subarachnoid hemorrhage[J]. Acta Radiol, 1997, 38(5): 791−796. DOI: 10.1080/02841859709172412. [43] Kim T, Lee H, Ahn S, et al. Incidence and risk factors of intracranial aneurysm: A national cohort study in Korea[J]. Int J Stroke, 2016, 11(8): 917−927. DOI: 10.1177/1747493016660096. [44] 刘海峰, 许永生, 陈小莉, 等. 3D-TOF-MRA诊断颅内动脉瘤价值的Meta分析[J]. 临床放射学杂志, 2017, 36(10): 1396−1400.
Liu HF, Xu YS, Chen XL, et al. The Value of 3D-TOF MRA for Diagnosing Intracranial Aneurysm: A Meta Analysis[J]. J Clin Radiol, 2017, 36(10): 1396−1400.[45] 张沥, 王寅中, 雷军强. CT血管成像与MR血管成像对颅内动脉瘤诊断价值的Meta分析[J]. 中国脑血管病杂志, 2012, 9(9): 466−471. DOI: 10.3969/j.issn.1672−5921.2012.09.004.
Zhang L, Wang YZ, Lei JQ. Diagnostic value of CT angiography and MR angiography for intracranial aneurysms: a Meta-analysis[J]. Chin J Cerebrovasc Dis, 2012, 9(9): 466−471. DOI: 10.3969/j.issn.1672−5921.2012.09.004. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 3582
- HTML全文浏览量: 2681
- PDF下载量: 18