


-
冠心病是心血管内科患者死亡的最常见原因,据报道显示其发病率超过10%[1]。随着经皮冠状动脉介入治疗(percutaneous coronary intervention,PCI)术的不断发展,临床上行PCI的冠心病患者逐渐增多。99Tcm-MIBI心肌灌注显像是可以反映心肌灌注情况的无创性检查,且同时可以获得左室壁运动及心功能等各项指标,其临床应用价值逐渐受到重视[2]。目前已有研究报道99Tcm-MIBI用于冠心病患者危险度分层,可以为患者是否行PCI术的决策提供有力证据[3]。患者行PCI后6个月易发生支架内再狭窄,99Tcm-MIBI用于再狭窄的诊断以及远期预后评估均有较好效果[4-5]。但有关99Tcm-MIBI应用于冠心病患者PCI后近期效果的研究较少。行PCI后的治疗效果判断不应局限于狭窄的血管是否再通,缺血心肌有无回复血流灌注是判断的关键。本研究通过对124例冠心病患者于行PCI前、后行99Tcm-MIBI检查,发现99Tcm-MIBI是判断PCI术后近期疗效和预后的有效方法。现报道如下。
-
将2014年10月至2017年3月于重庆市涪陵中心医院就诊的124例行PCI术的冠心病患者作为研究对象,其中男性68例、女性56例,患者年龄43~79(61.89±17.21)岁,病程3~6年,平均病程(4.38±1.64)年。于行PCI前3 d内行99Tcm-MIBI心肌灌注显像,需同时行99Tcm-MIBI静息心肌灌注显像(rest myocardial perfusion imaging,RMPI)和负荷心肌灌注显像(stress myocardial perfusion imaging,SMPI)。PCI术后3 d内行99Tcm-MIBI-SMPI。纳入标准:(1)冠心病的诊断符合2014版《冠心病诊断与治疗指南》中的标准[6],(2)患者均有胸闷、典型或不典型胸痛等临床症状,并经冠状动脉造影检查,结果显示1支以上冠状动脉管腔狭窄≥50%。(3)患者行PCI的适应证均符合《中国经皮冠状动脉介入治疗指南2012》中的标准[7],且冠状动脉造影检查结果显示1支以上冠状动脉管腔狭窄≥70%。排除标准:合并急性心肌梗塞、不稳定型心绞痛、严重心律失常、心功能III-IV级、严重心瓣膜病、急性肺栓塞、心肌炎者不纳入研究。所有患者均知情同意并签署知情同意书,本研究通过我院医学伦理委员会批准。术后3 d内行99Tcm-MIBI-SMPI。
-
99Tcm-MIBI-SMPI检查前2 d内停用扩血管药和抗心律失常药,4 h内禁食。行常规血生化、心电图和心脏超声检查,心电监护监测不良反应。建立静脉输液双通道,一侧微泵持续推注ATP 0.14 mg/kg·min,共6 min。另一侧于泵入ATP 3 min末时注射显像剂99Tcm-MIBI,总量925~1110 MBq。发生以下4种情况时,应立即停止ATP 泵入,严重时应给予硝酸甘油、氨茶碱等药物治疗:①心电图显示ST段下降大于2.5 mm或抬高大于1 mm;②典型的胸闷、胸痛的心绞痛症状;③血压急剧升高,大于220/100 mmHg或血压急剧下降,舒张压<50 mmHg;④严重的心律失常。ATP泵入的总量为0.84 mg/kg。0.5 h后进食牛奶或油煎蛋等高脂食物,1.5 h后行SPECT心肌灌注显像检查。采集数据用心电图为门控信号,平面像每个心动周期采集8~16帧,RR窗宽为15%,矩阵128×128,断层像每个心动周期采集8~12帧,RR窗值为20%,矩阵为64×64,由于每帧包含8~12份图,故采集时间要明显延长,以保证重建图像有足够的计数,减少统计误差对图像的影响。通过计算机叠加多个心动周期,获取心肌灌注图像的同时,也获取左心室壁运动及心功能指标参数。
99Tcm-MIBI-RMPI 于行99Tcm-MIBI-SMPI 1 d后进行,图像采集方法同99Tcm-MIBI-SMPI。对比负荷和静息状态下的灌注显像结果。
-
采用美国心脏协会的方法将左心室按照冠状动脉的分布分成17个心肌节段[8]。采用4分法评价显像结果:0分为放射性分布正常,1分为放射性分布轻度稀疏,2、3分分别为放射性分布中度或重度稀疏,4分为放射性分布缺损。总负荷分值(summed stress score,SSS)为99Tcm-MIBI-SMPI检查中17个节段得分的总和,总差分值为 99Tcm-MIBI-SMPI中17个节段得分的总和减去99Tcm-MIBI-RMPI中17个节段得分的总和。99Tcm-MIBI-SMPI 与99Tcm-MIBI-RMPI 差值≥1时为可逆性缺损,差值为0时为不可逆性缺损。
-
所有患者术前和术后均通过心脏彩色超声多普勒成像仪(飞利浦高端智能彩色超声系统 HD15)对患者心功能进行评估,其中左心室射血分数(left ventricular ejection fractions,LEVF)用于评估左室射血功能,左心室舒张末容积(end-diastolic volume,EDV)用于评估左室舒张功能,左心室收缩末期容积(end-systolic volume,ESV)用于评估左心室收缩功能。
-
PCI术后的患者,接受99Tcm-MIBI-SMPI检查后出院,根据99Tcm-MIBI-SMPI显示的缺血完全改善(RMPI放射性分布完全改善)、部分改善(RMPI放射性分布部分改善)、未改善(RMPI放射性分布未改善)3种情况将患者分为3组。出院1年内每间隔6个月对患者进行电话随访。统计指标如下。严重心血管事件包括:①半年或1年内发生心肌梗死;②半年或1年内发生心源性死亡。一般心血管事件包括:①半年或1年内再次行PCI或心脏搭桥术;②半年或1年内再次出现心绞痛症状,且严重程度不低于PCI手术前。124例入组患者均纳入统计,无失访及删失病例。
-
采用SPSS 24.0软件进行统计学分析。符合正态分布的计量资料采用均数±标准差的形式表示,在方差齐性检验(Levene's test)示方差均齐性的条件下,两组间数据比较采用student-t检验。计数资料采用例数(百分比)的形式表示,两组间数据比较采用χ2检验。P<0.05时表示差异有统计学意义。
-
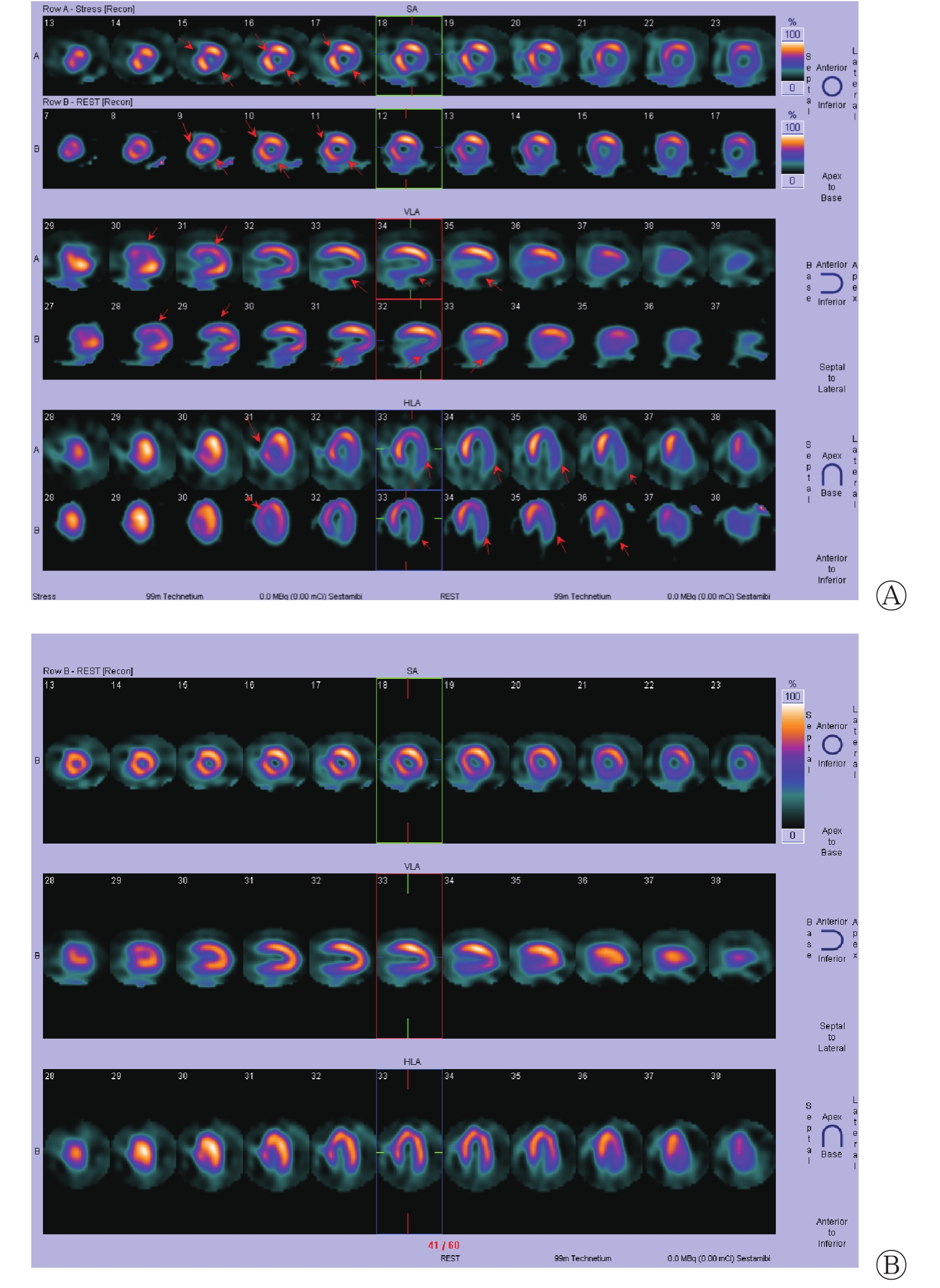
124例冠心病患者中,PCI术前99Tcm-MIBI-SMPI检查显示可逆性缺损节段272个,不可逆性缺损节段360个,SSS总分为1598分,PCI术后99Tcm-MIBI-SMPI检查显示可逆性缺损节段25个,改善247个(247/272=90.81%),不可逆性缺损节段198个,改善162个(162/360=45.00%),SSS总分为636分。图1为1例冠心病患者PCI术前、后99Tcm-MIBI-SMPI的对比结果,可见患者术前有可逆性缺损2个(前壁近间隔、前上间隔),不可逆性缺损3个(左心室下壁、侧壁、下壁近心底部),术后3处缺损明显改善,2处未改善(左心室下壁、前上间隔)。

图 1 冠心病(男性、68岁)患者PCI术前和术后99Tcm-MIBI结果比较
Figure 1. Comparison of 99Tcm-MIBI results before and after percutaneous coronary intervention in a patient with coronary heart disease (male, 68 years old)
-
患者PCI术后的心功能参数LVEF、EDV 和ESV较PCI术前均有明显的改善,且差异均有统计学意义(t=−7.450、4.304、12.144,均P<0.01)(表1)。
心功能指标 PCI术前 PCI术后 t值 P值 LVEF(%) 32.86±8.48 40.31±10.52 −7.450 0.001 EDV(mL) 186.74±43.12 162.62±45.12 4.304 0.001 ESV(mL) 132.37±9.28 116.28±11.47 12.144 0.001 注:表中,PCI:经皮冠状动脉介入治疗;LVEF:左心室射血分数;EDV:舒张末容积;ESV:收缩末期容积。 表 1 124例冠心病患者经皮冠状动脉介入治疗术前和术后心功能指标对比
Table 1. Comparison of cardiac function indexes before and after percutaneous coronary intervention in 124 patients with coronary heart disease
-
124例患者接受PCI术后,99Tcm-MIBI-SMPI结果显示缺血节段完全改善36例,部分改善62例,未改善26例。99Tcm-MIBI-SMPI显示缺血完全改善、部分改善、未改善的3组患者半年和一年心血管事件总发生率有明显的升高趋势,且差异有统计学意义(χ2=142.668、106.225,均P<0.05)(表2)。
PCI术后缺血节段改善情况 严重心血管事件 一般心血管事件 合计 半年 一年 半年 一年 半年 一年 完全改善(n=36) 0 1 1 2 1 3 部分改善(n=62) 3 5 5 9 8 14 未改善(n=26) 3 4 7 11 10 15 χ2值 142.668 106.225 P值 <0.05 <0.05 注:表中,PCI:经皮冠状动脉介入治疗;严重心血管事件:半年内或1年内发生心肌梗死、心源性死亡;一般心血管事件:半年或1年内再次行PCI或心脏搭桥术、再次出现心绞痛症状。 表 2 124例不同缺血程度的冠心病患者发生心血管事件的 情况(例)
Table 2. Comparison of death and acute cardiovascular events in 124 patients with coronary heart disease of different degrees of ischemia
-
PCI术后99Tcm-MIBI-SMPI检查显示,可逆性缺损节段25个,改善247个(247/272=90.81%)。可逆性缺损节段能否改善是评估患者PCI 手术效果的关键。不可逆性缺损节段198个,改善162个(162/360=45.0%),198个缺损节段没有改善的原因分析可能为:①狭窄或堵塞的血管没有再通,PCI手术失败;②心肌组织缺血时间过长,血流灌注恢复后坏死的心肌细胞无法恢复功能;③行SMPI检查时心肌细胞功能尚未完全恢复;④发生PCI术后再狭窄。有研究结果显示,PCI术后1~3 d即可发生再狭窄,发生率可达10%,再狭窄的发生率在PCI术后半年内迅速上升[9]。因此,PCI术后99Tcm-MIBI-SMPI检查结果显示不可逆性缺损节段的改善可以肯定PCI术的效果,但放射性分布稀疏和(或)缺损没有改善不能说明PCI术没有效果。
我们的研究结果显示,99Tcm-MIBI-SMPI显示缺血完全改善、部分改善、未改善3组患者半年和一年心血管事件总发生率有明显的升高趋势,且差异有统计学意义,这说明PCI术后行99Tcm-MIBI-SMPI检查不仅可以观察PCI的手术效果,也可以反映患者的预后,即99Tcm-MIBI-SMPI检查结果显示缺损节段改善越完全,患者的预后越好,心血管事件发生率越低。但本研究纳入的患者样本量不大,且为电话随访,患者并未经过影像学检查证实结论,因此预后的结果可能具有一定的局限性。
综上,对行PCI术的冠心病患者手术前后进行99Tcm-MIBI心肌灌注显像检查,可以较好地评估PCI的近期疗效,同时对远期预后也有一定的预测作用。
利益冲突 本研究由署名作者按以下贡献声明独立开展,不涉及任何利益冲突。
作者贡献声明 张科负责数据的收集和论文的撰写;谭红霞负责统计分析和文献的查询;宋波负责数据的分析和论文的审阅。
99Tcm-MIBI心肌灌注显像对行PCI术的冠心病患者中的近期效果的评估作用
The recent effect observation of 99Tcm-MIBI myocardial perfusion imaging in coronary heart disease patients with percutaneous coronary intervention
-
摘要:
目的 探讨99Tcm-MIBI心肌灌注显像(99Tcm-MIBI)对行经皮冠状动脉介入治疗(PCI)术的冠心病患者近期疗效的评估作用。 方法 收集2014年10月至2017年3月于重庆市涪陵中心医院行PCI术的冠心病患者124例,其中,男性68例、女性56例,年龄43~79(61.89±17.21)岁。术前3 d内给予负荷心肌灌注显像(99Tcm-MIBI-SMPI)和静息心肌灌注显像(99Tcm-MIBI-RMPI)检查,术后3 d内给予99Tcm-MIBI-SMPI检查。所有患者均进行为期1年的电话随访,按缺血完全改善、部分改善、未改善分为3组,统计发生一般心血管事件和严重心血管事件的例数。两组间计量资料的比较采用student-t检验,计数资料的比较采用χ 2检验。 结果 124例患者中,PCI术前99Tcm-MIBI-SMPI检查显示可逆性缺损节段272个,不可逆性缺损节段360个,总负荷分值(SSS)1598分;PCI术后99Tcm-MIBI-SMPI检查显示可逆性缺损节段25个,改善247个(247/272=90.81%),不可逆性缺损节段198个,改善162个(162/360=45.00%),SSS总分636分。患者PCI术后的心功能参数左心室射血分数、舒张末容积和收缩末期容积较PCI术前均有明显的改善,且差异均有统计学意义(t=−7.450、4.304、12.144,均P<0.01);术后99Tcm-MIBI-SMPI 显示缺血完全改善、部分改善、未改善3组患者半年和一年心血管事件总发生率有明显的升高趋势(χ2=142.668、106.225,均P<0.05)。 结论 99Tcm-MIBI心肌灌注显像检查用于评估冠心病患者行PCI术的近期疗效有较好作用,且对患者的远期预后有一定的预测效果。 -
关键词:
- 心肌灌注显像 /
- 冠心病 /
- 经皮冠状动脉介入治疗
Abstract:Objective To explore the recent effect of 99Tcm-methoxyisobutylisonitrile myocardial perfusion imaging (99Tcm -MIBI) in coronary heart disease (CHD) patients with percutaneous coronary intervention (PCI). Methods From October 2014 to March 2017, a total of 124 patients [including 68 males and 56 females, aged 43~79 (61.89±17.21)] with CHD undergoing PCI in Fuling central hospital were used as research objects and underwent adenosine-loading myocardial perfusion imaging (99Tcm -MIBI-SMPI) and 99Tcm MIBI rest myocardial perfusion imaging (99Tcm-MIBI-RMPI) within 3 days before PCI and 99Tcm-MIBI-SMPI within 3 days after PCI. All patients were followed up for 1 year via telephone calls. According to complete improvement, partial improvement and no improvement of ischemia, they were divided into three groups. The cases of general cardiovascular events and serious cardiovascular events were calculated. Student-t test was used to compare the measurement data between the two groups, and χ2 test was used to compare the count data. Results In the 124 patients, 99Tcm-MIBI-SMPI examination before PCI showed 272 reversible defect sections and 360 irreversible defect sections. The summed stress score was 1598 points. 99Tcm-MIBI-SMPI examination after PCI showed 25 reversible defect sections, 247 sections (247/272=90.81%) improved, 198 irreversible defect sections, and 162 sections (162/360=45.00%) improved. The summed stress score was 636 points. After PCI, the left ventricular ejection fraction, end diastolic velocity, and end systolic volume of patients showed significant improvement. The differences were statistically significant (t=−7.450, 4.304, 12.144, all P<0.01). Postoperative 99Tcm MIBI-SMPI indicated the completely improved, improved, and partly improved status of the three groups of ischemia patients, and the improvement showed an significantly increased trend in both half year and 1 year total incidence of cardiovascular events (χ2=142.668, 106.225, both P<0.05). Conclusion 99Tcm-MIBI has good effect on CHD patients with PCI and on their long-term prognosis. -
图 1 冠心病(男性、68岁)患者PCI术前和术后99Tcm-MIBI结果比较
Figure 1. Comparison of 99Tcm-MIBI results before and after percutaneous coronary intervention in a patient with coronary heart disease (male, 68 years old)
表 1 124例冠心病患者经皮冠状动脉介入治疗术前和术后心功能指标对比
Table 1. Comparison of cardiac function indexes before and after percutaneous coronary intervention in 124 patients with coronary heart disease
心功能指标 PCI术前 PCI术后 t值 P值 LVEF(%) 32.86±8.48 40.31±10.52 −7.450 0.001 EDV(mL) 186.74±43.12 162.62±45.12 4.304 0.001 ESV(mL) 132.37±9.28 116.28±11.47 12.144 0.001 注:表中,PCI:经皮冠状动脉介入治疗;LVEF:左心室射血分数;EDV:舒张末容积;ESV:收缩末期容积。  下载: 导出CSV
下载: 导出CSV
表 2 124例不同缺血程度的冠心病患者发生心血管事件的 情况(例)
Table 2. Comparison of death and acute cardiovascular events in 124 patients with coronary heart disease of different degrees of ischemia
PCI术后缺血节段改善情况 严重心血管事件 一般心血管事件 合计 半年 一年 半年 一年 半年 一年 完全改善(n=36) 0 1 1 2 1 3 部分改善(n=62) 3 5 5 9 8 14 未改善(n=26) 3 4 7 11 10 15 χ2值 142.668 106.225 P值 <0.05 <0.05 注:表中,PCI:经皮冠状动脉介入治疗;严重心血管事件:半年内或1年内发生心肌梗死、心源性死亡;一般心血管事件:半年或1年内再次行PCI或心脏搭桥术、再次出现心绞痛症状。
下载: 导出CSV
-
[1] 高翔. 缺血性心脏病的临床及流行病学研究[J]. 中西医结合心血管病杂志, 2016, 4(34): 99, 102. DOI: 10.16282/j.cnki.cn11−9336/r.2016.34.184.
Gao X. Clinical and epidemiological study of ischemic heart disease[J]. Cardiovasc Dis J Integr Tradit Chin West Med, 2016, 4(34): 99, 102. DOI: 10.16282/j.cnki.cn11−9336/r.2016.34.184.[2] 热孜万古丽·买买提, 李晓玉, 杨文革, 等. 腺苷注射液负荷心肌灌注显像在老年女性冠状动脉粥样硬化性心脏病诊断中的临床价值[J]. 中国医药, 2017, 12(9): 1294−1297. DOI: 10.3760/cma.j.issn.1673−4777.2017.09.004.
Maimaiti R, Li XY, Yang WG, et al. Clinical value of adenosine for myocardial perfusion imaging in diagnosis of coronary heart disease in elderly women[J]. China Med, 2017, 12(9): 1294−1297. DOI: 10.3760/cma.j.issn.1673−4777.2017.09.004.[3] 李勇, 张海山, 胡文强, 等. ATP负荷99Tcm-MIBI门控心肌SPECT显像在冠状动脉临界病变危险分层中的价值[J]. 中国动脉硬化杂志, 2018, 26(6): 626−632. DOI: 10.3969/j.issn.1007−3949.2018.06.016.
Li Y, Zhang HS, Hu WQ, et al. The value of ATP stress 99Tcm-MIBI gated myocardial SPECT imaging in the risk stratification of intermediate coronary lesion[J]. Chin J Arterioscler, 2018, 26(6): 626−632. DOI: 10.3969/j.issn.1007−3949.2018.06.016.[4] Smit JM, Hermans MP, Dimitriu-Leen AC, et al. Long-term prognostic value of single-photon emission computed tomography myocardial perfusion imaging after primary PCI for STEMI[J]. Eur Heart J Cardiovasc Imaging, 2018, 19(11): 1287−1293. DOI: 10.1093/ehjci/jex332. [5] Koh AS, Lye WK, Chia SY, et al. Long-Term Prognostic Value of Appropriate Myocardial Perfusion Imaging[J]. Am J Cardiol, 2017, 119(12): 1957−1962. DOI: 10.1016/j.amjcard.2017.03.026. [6] 中华医学会心血管病学分会介入心脏病学组, 中华医学会心血管病学分会动脉粥样硬化与冠心病学组, 中国医师协会心血管内科医师分会血栓防治专业委员会, 等. 稳定性冠心病诊断与治疗指南[J]. 中华心血管病杂志, 2018, 46(9): 680−694. DOI: 10.3760/cma.j.issn.0253−3758.2018.09.004.
Section of Interventional Cardiology of Chinese Society of Cardiology, Section of Atherosclerosis and Coronary Artery Disease of Chinese Society of Cardiology, Specialty Committee on Prevention and Treatment of Thrombosis of Chinese College of Cardiovascular Physicians, et al. Guideline on the diagnosis and treatment of stable coronary artery disease[J]. Chin J Cardiol, 2018, 46(9): 680−694. DOI: 10.3760/cma.j.issn.0253−3758.2018.09.004.[7] 中华医学会心血管病学分会介入心脏病学组, 中国医师协会心血管内科医师分会血栓防治专业委员会, 中华心血管病杂志编辑委员会. 中国经皮冠状动脉介入治疗指南(2016)[J]. 中华心血管病杂志, 2016, 44(5): 382−400. DOI: 10.3760/cma.j.issn.0253−3758.2016.05.006.
Section of Interventional Cardiology of Chinese Society of Cardiology of Chinese Medical Association, Specialty Committee on Prevention and Treatment of Thrombosis of Chinese College of Cardiovascular Physicians, Editorial Board of Chinese Journal of Cardiology. Chinese guideline for percutaneous coronary intervention(2016)[J]. Chin J Cardiol, 2016, 44(5): 382−400. DOI: 10.3760/cma.j.issn.0253−3758.2016.05.006.[8] Cerqueira MD, Weissman NJ, Dilsizian V, et al. Standardized myocardial segmentation and nomenclature for tomographic imaging of the heart. A statement for healthcare professionals from the Cardiac Imaging Committee of the Council on Clinical Cardiology of the American Heart Association[J]. J Nucl Cardiol, 2002, 9(2): 240−245. DOI: 10.1067/mnc.2002.123122. [9] 李剑明, 史蓉芳, 李婷, 等. 核素显像心肌灌注缺损与CTCA冠状动脉不同狭窄程度的关系分析[J]. 中华核医学杂志, 2011, 31(6): 394−399. DOI: 10.3760/cma.j.issn.0253−9780.2011.06.011.
Li JM, Shi RF, Li T, et al. The relationship between perfusion defects on myocardial SPECT and stenotic severity on CT coronary angiography[J]. Chin J Nucl Med, 2011, 31(6): 394−399. DOI: 10.3760/cma.j.issn.0253−9780.2011.06.011. -

 点击查看大图
点击查看大图
图(1)表(2)
计量
- 文章访问数: 2758
- HTML全文浏览量: 1606
- PDF下载量: 23