


-
放疗靶区和邻近的组织器官,特别是危及器官实际受到的照射剂量,即吸收剂量,是评估放疗疗效和不良反应或损伤的基础。由于直接计算的物理剂量(physical dose,PhD)受总剂量、分割计量、分次数等因素影响很大,难以进行比较,所以对预期疗效、不良反应和危及器官损伤的预测需要进行生物效应剂量(biological effective dose,BED)的换算。BED是指每次1.8~2.0 Gy,每周5次,总剂量60.0~70.0 Gy,即60.0~70.0 Gy/30~35次/6~7周的剂量分割模式下的剂量[1],一般以2.0 Gy计算,即常规2.0 Gy分次的等效剂量(equivalent dose in 2.0 Gy/f,EQD2)。这既是讨论肿瘤吸收剂量进行疗效判定的标准,也是靶区周围危及器官剂量控制的标准[2-4]。
在目前以适形和调强技术为主的精确放疗模式下,危及器官能够明确排除在靶区以外,所以每次的受照剂量较常规放疗明显减少[5-6]。常规分割模式下,危及器官每次的实际照射剂量明显低于2.0 Gy,因此危及器官特别是对分次剂量更为敏感器官的BED与PhD明显不同[7]。本研究结合L-Q(linear quadratic)模型[8],应用深圳市医诺智能科技发展有限公司的RTIS软件,在胸部肿瘤放疗患者中对这一问题进行探讨。
-
选取2016年5月16日至2016年12月31日于我院应用美国VARIAN Eclipse Aria和美国PHILIPS Pinnacle计划系统完成治疗的30例胸部肿瘤患者,包括非小细胞肺癌、小细胞肺癌、食管癌、胸腺瘤和恶性淋巴瘤等。纳入标准:进行胸部靶区适形和调强放疗的患者。排除标准:胸部以外靶区照射患者。对上述治疗计划进行分析,治疗计划为95%计划靶体积(planning target volume,PTV)30~60 Gy/15~30次/3~6周。所有患者均在治疗前签署了知情同意书。
-
应用医诺RTIS V2.13软件,调取患者治疗计划,在常规计划评估界面显示脊髓和PTV的剂量分布情况。运行BED模块程序,匹配脊髓α/β值=3和PTV α/β值=10,显示脊髓和PTV的BED。两种情况均可同时显示剂量-体积直方图。从程序调取脊髓和PTV的最小、最大和平均剂量的PhD和BED数值进行统计分析。
-
应用SPSS 19.0软件对数据进行统计学分析。脊髓和PTV的PhD和BED各均值符合正态分布且方差齐,分别进行均值比较和t检验,P<0.05表示差异有统计学意义。
-
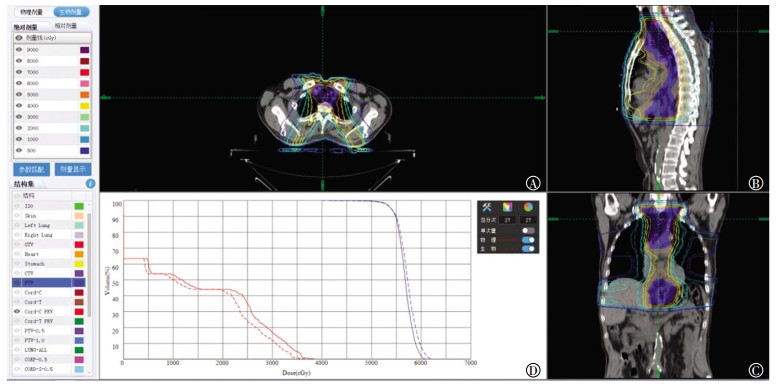
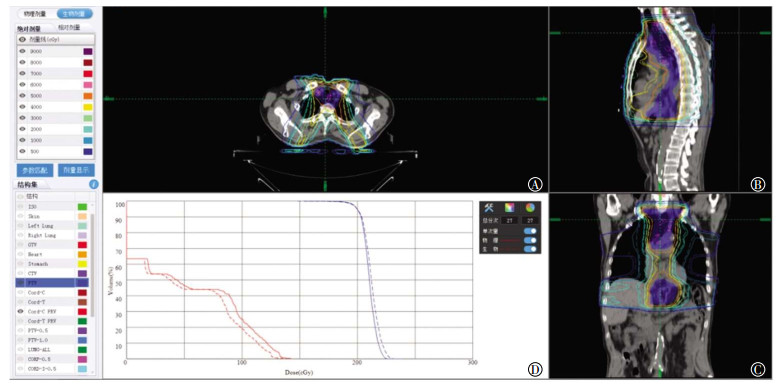
评估显示1次剂量或总剂量下的PhD和BED等剂量曲线,从剂量-体积直方图可以看出,脊髓的BED曲线位于PhD曲线左侧,而PTV的BED曲线位于PhD曲线右侧(图 1中D、图 2中D)。
图 1 单次照射脊髓和PTV的PhD和BED(男性,54岁)
Figure 1. The results of physicat dose and biological effective dose in cord and planning target volume for single radiation
图 2 30次照射脊髓和PTV的PhD与BED(男性,54岁)
Figure 2. The results of physicat dose and biological effective dose in cord and planning target volume for 30 radiations
由表 1可见,脊髓的PhD和BED的最小、最大、平均剂量的差异均有统计学意义(t=0.826、6.143、5.234,均P<0.05);而PTV的PhD和BED的最小、最大、平均剂量的差异均无统计学意义(t=6.953、-2.164、-1.193,均P>0.05)。但由于脊髓是典型的串行器官,因此,最小剂量、平均剂量的参考价值较小,临床主要应用最大剂量。
名称 脊髓 PTV 最小剂量 最大剂量 平均剂量 最小剂量 最大剂量 平均剂量 PhD 80.41±274.75 3398.00±1200.95 1265.79±762.49 3615.51±1566.10 5505.26±1731.64 4984.33±1615.59 EQD2 74.71±249.34 3118.93±1181.96 1181.44±742.18 3500.97±1576.92 5672.93±1791.98 5047.63±1646.57 t值 0.826 6.143 5.234 6.953 -2.164 -1.193 P值 0.04 0 0 0.122 0.071 0.061 注:表中,PTV:计划靶体积;PhD:物理剂量;EQD2:2.0 Gy的等效剂量。 表 1 30 例胸部肿瘤患者脊髓和PTV的PhD与EQD2比较(x±s)
Table 1. The comparison of physical dose and biological effective dose in cord and planning target volume for 30 thoracic tumor patients(x±s)
-
依据线性二次方程(L-Q模型)计算出2.0 Gy照射1次和30次时脊髓(α/β比值=3.0)在不同剂量曲线的PhD和BED。由表 2可见,随着剂量曲线下降,PhD和BED也随之降低,而且相同剂量曲线的BED较PhD更低。
剂量曲线/% 单次PhD/Gy 单次BED/Gy 30次PhD/Gy 30次BED/Gy 100 2 2 60 60 90 1.8 1.73 54 51.84 80 1.6 1.47 48 44.16 70 1.4 1.23 42 36.96 60 1.2 1.01 36 30.24 50 1 0.8 30 24 40 0.8 0.61 24 18.24 30 0.6 0.43 18 12.96 20 0.4 0.27 12 8.16 10 0.2 0.13 6 3.84 注:表中,PhD:物理剂量;BED:生物效应剂量。 表 2 30例胸部肿瘤患者接受2.0 Gy 1次和30次照射时脊髓在不同剂量曲线下的PhD和BED
Table 2. The data of physiacal dose and biological effective dose of cord in different dose curves with 2.0 Gy single and 30 radiations for 30 patients
-
本研究应用的RTIS V2.13软件的治疗计划评估功能具有PhD显示和BED显示的双重模式,并且可以对照显示。在治疗计划评估中,可以选择单次治疗或全程治疗,软件以三维断面剂量曲线图和剂量-体积直方图形式显示PhD和BED(图 1、图 2)。
-
放疗是利用放射线(主要是X射线)杀灭肿瘤细胞并治疗肿瘤。虽然近年来研究者认识到放疗与免疫的关系,并赋予放疗以全新概念[10],但是,对靶区剂量的控制和对周围组织特别是危及器官的最大限度防护,仍是放射物理学研究的主要问题[11]。虽然一直强调对于病变组织给予更高的剂量,但是在常规放疗中,射线不能充分避开周围正常组织和危及器官,因此受到正常组织特别是危及器官耐受性的限制,治疗剂量必须限制在一定水平[12]。也就是说,靶区附近危及器官的耐受量限制了靶区剂量的提高,因此不能实现由于提高肿瘤照射剂量而获得的疗效最大化。
近年来,临床放疗取得了突飞猛进的发展,以适形和调强技术为代表,现代放疗进入了以精确定位、精确计划、精确治疗为特色的时代。精确放疗的最大优势是靶区可以获得均匀的最大剂量的照射,同时靶区周围组织特别是危及器官受到最小剂量的照射[13-17]。在这种治疗模式的治疗计划下,危及器官的受照剂量一般位于等剂量曲线70%以下的剂量范围。也就是说,在常规分割模式下,危及器官每次实际的受照剂量往往低于1.4 Gy,显然,其生物效应明显降低,特别是对于脊髓等对分割剂量非常敏感的晚反应组织,其损伤程度明显降低。
上世纪20年代,国际辐射单位与测量委员会(ICRU)规范了辐射剂量单位,量化了辐射标准,放射物理、放射生物研究和临床治疗有了统一的剂量标准。PhD是指生物组织得到或吸收的剂量。根据国际原子能委员会第30号报告定义,BED是对生物体辐射反应程度的测量[18]。显然,PhD和BED是两个不同的概念,两者考察的侧重点完全不同。PhD是实际受到射线照射的量值,BED是受照剂量转化为常规分割后的量值。但是,两者又有密切联系,PhD越大,BED越大,生物效应越明显。然而,不同的组织或器官对这种增大的反应能力有很大差异。
1973年,Chadwick和Leenhouts[19]根据细胞存活曲线推导出L-Q模型,使不同时间、剂量、次数或不同分割方案的BED得以比较。同时,也可以通过BED对同一组织或危及器官在不同PhD下的生物效应进行评估[8]。
从放射生物学或放射损伤角度来说,脊髓几乎没有增殖能力,损伤后仅以修复代偿其正常功能,是典型的晚反应组织,对分次剂量的变化极为敏感,加大分次剂量时,损伤明显加重。相反,在常规分割模式下,随着PhD的降低,BED明显下降,损伤风险进一步减小。
颈部、胸部和上腹部肿瘤进行放疗时,脊髓均是需要控制受照剂量的危及器官。但是,使用PhD对分次剂量极为敏感的晚反应组织的生物效应进行评价显然不科学,需要换算为BED。在常规分割模式下,适形和调强治疗技术可以很好地防护邻近的组织器官,能够确保脊髓受到更低的照射剂量,这种低剂量带来更低的BED,使脊髓得到更好的保护[26]。另一方面,这种更高的脊髓BED耐受,可以使靶区的照射剂量得到提高,同时可以提高肿瘤的控制率。
临床放疗计划的审核需要考虑靶区剂量和危及器官受量,在常规分割模式下,靶区位于95%剂量曲线之内,因此PhD相当于BED,但是靶区以外的组织和危及器官因PhD的下降,会出现PhD与BED不一致。脊髓等晚反应组织对分次剂量更为敏感,因此会出现BED的进一步下降,也就是说脊髓等器官的耐受性提高。等剂量曲线下,实际BED与PhD并不一致,但这种差别在PhD图上看不出来。例如一个治疗计划,常规分割2.00 Gy/次,治疗次数为35,靶区PhD和BED约为70.00 Gy,如果脊髓剂量曲线为70%,则PhD为49.00 Gy,如果按照脊髓最大耐受剂量45.00 Gy进行评估,则计划不可行。但是,考虑脊髓实际以1.40 Gy/次的分割剂量受到照射,虽然PhD达到了49.00 Gy,但BED仅为43.05 Gy,显然在脊髓最大耐受剂量范围之内,则计划可行。
临床进行计划评估的常用软件,即治疗计划系统均是直接显示PhD,不能显示不同剂量曲线下当前靶区或危及器官的BED。因为一般临床治疗计划要求靶区位于95%剂量范围内,所以靶区本身PhD和BED差别不大,一般靶区的肿瘤组织α/β值较高(>10),对分次剂量并不敏感,因此在常规分割模式下,PhD与BED差别不大。但对于危及器官,特别是脊髓,随着PhD的下降,BED进一步降低,生物效应更趋于降低,因此对器官的保护效应更加明显。从肿瘤控制角度来说,这种确有把握的脊髓受量可以转化为靶区剂量的提高,从而提高肿瘤的控制率。在临床放疗计划中考虑到这种差别,并进行BED的评估显然可以使治疗计划更加科学、合理,对肿瘤的控制和脊髓损伤的防护均可达到最大化。
多年来,剂量-时间等放射生物学因素对临床BED研究具有明确的指导意义[28]。本研究应用RTIS V2.13软件对脊髓BED进行研究的结果与放射生物学理论值相符。在临床应用中,RTISV2.13软件系统对靶区和危及器官除了以直观的剂量曲线和剂量-体积直方图形式显示以外,也以数值列表形式显示体积、PhD和BED的最小剂量、最大剂量和平均剂量,以便于进一步细节评价。RTIS V2.13软件编程以线性二次方程(L-Q模型)公式为内核,同时考虑了优先级和治疗中断等对BED有影响的临床和放射生物学参数,α/β比值有常规预设,但也可以根据临床治疗自行设定,以进行个体化的评估。
总之,在常规分割治疗模式下应用适形和调强技术,应使用BED对脊髓的受照剂量进行控制和评估,从而提高肿瘤的治疗愈率。
胸部肿瘤适形和调强常规分割放疗脊髓生物效应剂量研究
The study for biological effect dose of spinal cord in thoracic tumors with the model of conformal and intensity modulated technique and conventional fractionation
-
摘要:
目的探讨对常规分割模式下胸部肿瘤适形和调强放疗技术进行脊髓生物效应剂量(BED)评估的必要性和可行性。 方法选取2016年5月16日至2016年12月31日于唐山市人民医院放化疗科收治的胸部肿瘤患者30例,应用医诺RTIS治疗计划评估模块对所有患者的治疗计划进行评估,并进行物理剂量(PhD)和BED的比较。依据线性二次方程(L-Q模型)计算2.0 Gy照射1次和30次时脊髓在不同剂量曲线的PhD和RED。组间比较采用t检验。 结果脊髓的RED曲线位于PhD曲线左侧,计划靶体积(PTV)的BED曲线位于PhD曲线右侧。30例患者的治疗计划中,脊髓的最小、最大、平均PhD与BED分别为(80.41±274.75)、(3398.00±1200.95)、(1265.79±762.49)cGy和(74.71±249.34)、(3118.93±1181.96)、(1181.44±742.18)cGy,差异均有统计学意义(t=0.826、6.143、5.234,P < 0.05);PTV的最小、最大、平均PhD和BED分别为(3615.51±1566.10)、(5505.26±1731.64)、(4984.33±1615.59)cGy和(3500.97±1576.92)、(5672.93±1791.98)、(5047.63±1646.57)cGy,差异均无统计学意义(t=6.953、-2.164、-1.193,均P>0.05)。随着剂量曲线的下降,PhD和BED也随之降低,而且相应剂量曲线的BED较PhD更低。 结论从增强靶区控制和脊髓保护的角度,胸部肿瘤精确常规分割放疗有必要进行脊髓的BED评估。 -
关键词:
- 胸部肿瘤 /
- 放射疗法, 调强适形 /
- 脊髓 /
- 常规分割 /
- 生物效应剂量
Abstract:ObjectiveTo investigate the necessity and feasibility of evaluation for spinal cord biological effect dose (BED) in clinical radiotherapy on thoracic tumors in the model of conformal or intensity modulated technique and conventional fractionation. MethodsFrom 16 May 2016 to 31 December 2016, 30 patients accepting thoracic radiotherapy were selected in the Radio-chemotherapy department of Tangshan City People's Hospital. Radiotherapy plans of these patients were evaluated by the evaluation module of the RTIS treatment plan system, and then the physical dose(PhD) and BED were compared, respectively. After that, the PhD and BED of the spinal cord in different dose curves for 2.0 Gy irradiation 1 and 30 times were calculated by the linear quadratic equation(L-Q model). T test was used for all comparison between groups in statistics. ResultsThe BED curve of the spinal cord was on the left of the PhD curve, and the BED curve of planning target volume(PTV) was on the right of the PhD curve. In the radiotherapy plans of the 30 patients, for the spinal cord, the minimum maximum, average doses of PhD and BED were (80.41±274.75), (3398.00±1200.95), (1265.79±762.49) cGy and (74.71±249.34), (3118.93±1181.96), (1181.44±742.18) cGy, separately, the differences of them were significantly(t=0.826, 6.143, 5.234, all P < 0.05). However, for the PTV of target the minimum, maximum, average doses of PhD and BED were (3615.51±1566.10), (5505.26±1731.64), (4984.33±1615.59) cGy and (3500.97±1576.92), (5672.93±1791.98), (5047.63±1646.57) cGy, all of them were no significances in statistics (t=6.953, -2.164, -1.193, all P>0.05). With the decline of the dose curve, the PhD and BED were reducing, and the BED were lower than the PhD in the curve for corresponding dose. ConclusionsIn the radiotherapy of thoracic tumors, considering potential enhancement of local target control and better spinal cord protection, it is necessary to evaluate the BED of the spinal cord. -
图 1 单次照射脊髓和PTV的PhD和BED(男性,54岁)
Figure 1. The results of physicat dose and biological effective dose in cord and planning target volume for single radiation
图 2 30次照射脊髓和PTV的PhD与BED(男性,54岁)
Figure 2. The results of physicat dose and biological effective dose in cord and planning target volume for 30 radiations
表 1 30 例胸部肿瘤患者脊髓和PTV的PhD与EQD2比较(x±s)
Table 1. The comparison of physical dose and biological effective dose in cord and planning target volume for 30 thoracic tumor patients(x±s)
名称 脊髓 PTV 最小剂量 最大剂量 平均剂量 最小剂量 最大剂量 平均剂量 PhD 80.41±274.75 3398.00±1200.95 1265.79±762.49 3615.51±1566.10 5505.26±1731.64 4984.33±1615.59 EQD2 74.71±249.34 3118.93±1181.96 1181.44±742.18 3500.97±1576.92 5672.93±1791.98 5047.63±1646.57 t值 0.826 6.143 5.234 6.953 -2.164 -1.193 P值 0.04 0 0 0.122 0.071 0.061 注:表中,PTV:计划靶体积;PhD:物理剂量;EQD2:2.0 Gy的等效剂量。  下载: 导出CSV
下载: 导出CSV
表 2 30例胸部肿瘤患者接受2.0 Gy 1次和30次照射时脊髓在不同剂量曲线下的PhD和BED
Table 2. The data of physiacal dose and biological effective dose of cord in different dose curves with 2.0 Gy single and 30 radiations for 30 patients
剂量曲线/% 单次PhD/Gy 单次BED/Gy 30次PhD/Gy 30次BED/Gy 100 2 2 60 60 90 1.8 1.73 54 51.84 80 1.6 1.47 48 44.16 70 1.4 1.23 42 36.96 60 1.2 1.01 36 30.24 50 1 0.8 30 24 40 0.8 0.61 24 18.24 30 0.6 0.43 18 12.96 20 0.4 0.27 12 8.16 10 0.2 0.13 6 3.84 注:表中,PhD:物理剂量;BED:生物效应剂量。
下载: 导出CSV
-
[1] Jones B, Dale RG, Deehan C, et al. The role of biologically effective dose(BED) in clinical oncology[J]. Clin Oncol(R Coll Radiol), 2001, 13(2):71-81. DOI:10.1053/clon.2001.9221. [2] Fowler JF. 21 years of biologically effective dose[J]. Br J Radiol, 2010, 83(991):554-568. DOI:10.1259/bjr/31372149. [3] Mouttet-Audouard R, Lacornerie T, Tresch E, et al. What is the normal tissues morbidity following Helical Intensity Modulated Radiation Treatment for cervical cancer?[J]. Radiother Oncol, 2015, 115(3):386-391. DOI:10.1016/j.radonc.2015.02.010. [4] Hopewell JW, Millar WT, Lindquist C, et al. Application of the concept of biologically effective dose (BED) to patients with Vestibular Schwannomas treated by radiosurgery[J]. J Radiosurg SBRT, 2013, 2(4):257-271. [5] Su SF, Huang Y, Xiao WW, et al. Clinical and dosimetric characteristics of temporal lobe injury following intensity modulated radiotherapy of nasopharyngeal carcinoma[J]. Radiother Oncol, 2012, 104(3):312-316. DOI:10.1016/j.radonc.2012.06.012. [6] Lee SH, Lee KC, Choi J, et al. Clinical applicability of biologically effectivedose calculation for spinal cord in fractionatedspine stereotactic body radiation therapy[J]. Radiol Oncol, 2015, 49(2):185-191. DOI:10.1515/raon-2015-0008. [7] Wambersie A, Menzel HG, Gahbauer RA, et al. Biological weighting of absorbed dose in radiation therapy[J]. Radiat Prot Dosimetry, 2002, 99(1/4):445-452. [8] Iwata H, Matsufuji N, Toshito T, et al. Compatibility of the repairable-conditionally repairable, multi-target and linear-quadratic models in converting hypofractionated radiation doses to single doses[J]. J Radiat Res, 2013, 54(2):367-373. DOI:10.1093/jrr/rrs089. [9] Jin JY, Huang YM, Brown SL, et al. Radiation dose-fractionation effects in spinal cord:comparison of animal and human data[J]. J Radiat Oncol, 2015, 4(3):225-233. DOI:10.1007/s13566-015-0212-9. [10] Deloch L, Derer A, Hartmann J, et al. Modern Radiotherapy Concepts and the Impact of Radiation on Immune Activation[J]. Front Oncol, 2016, 6:141. DOI:10.3389/fonc.2016.00141. [11] 李玉, 徐慧军.现代肿瘤放射物理学[M].北京:中国原子能出版社, 2015:526-530.
Li Y, Xu HJ. Modern radiophysicson tumor[M]. Beijing:China Atomic Energy Press, 2015:526-530.[12] Gandhi AK, Sharma DN, Rath GK, et al. Early clinical outcomes and toxicity of intensity modulated versus conventional pelvic radiation therapy for locally advanced cervix carcinoma:a prospective randomized study[J]. Int J Radiat Oncol Biol Phys, 2013, 87(3):542-548. DOI:10.1016/j.ijrobp.2013.06.2059. [13] Co J, Mejia MB, Dizon JM. Evidence on effectiveness of intensity-modulated radiotherapy versus 2-dimensional radiotherapy in the treatment of nasopharyngeal carcinoma: Meta-analysis and a systematic review of the literature[J]. Head Neck, 2016, 38 Suppl 1: E2130S-2142. DOI: 10.1002/hed.23977. [14] Peng G, Wang T, Yang KY, et al. A prospective, randomized study comparing outcomes and toxicities of intensity-modulated radiotherapy vs. conventional two-dimensional radiotherapy for the treatment of nasopharyngeal carcinoma[J]. Radiother Oncol, 2012, 104(3):286-293. DOI:10.1016/j.radonc.2012.08.013. [15] Zhang MX, Li J, Shen GP, et al. Intensity-modulated radiotherapy prolongs the survival of patients with nasopharyngeal carcinoma compared with conventional two-dimensional radiotherapy:A 10-year experience with a large cohort and long follow-up[J]. Eur J Cancer, 2015, 51(17):2587-2595. DOI:10.1016/j.ejca. 2015.08.006. [16] Zhou GQ, Yu XL, Chen M, et al. Radiation-induced temporal lobe injury for nasopharyngeal carcinoma: a comparison of intensity-modulated radiotherapy and conventional two-dimensional radiotherapy[J/OL]. PLoS One, 2013, 8(7): e67488[2018-02-05]. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3707870/pdf/pone.0067488.pdf. DOI: 10.1371/journal.pone.0067488. [17] Dolezel M, Odrazka K, Zouhar M, et al. Comparing morbidity and cancer control after 3D-conformal (70/74 Gy) and intensity modulated radiotherapy (78/82 Gy) for prostate cancer[J]. Strahlenther Onkol, 2015, 191(4):338-346. DOI:10.1007/s00066-014-0806-y. [18] 殷蔚伯, 余子豪, 徐国镇, 等.肿瘤放射治疗学[M]. 4版.北京:中国协和医科大学出版社, 2008:276.
Yin WB, Yu ZH, Xu GZ, et al. Radiation oncology[M]. 4th ed. Beijing:China Union Medical University Press, 2008:276.[19] Chadwick HK, Leenhouts HP. A molecular therapy of cell survival[J]. Physic Med Biol, 1973, 18:78-87. doi: 10.1088/0031-9155/18/1/007 [20] Sanpaolo P, Barbieri V, Genovesi D. Biologically effective dose and definitive radiation treatment for localized prostate cancer:treatment gaps do affect the risk of biochemical failure[J]. Strahlenther Onkol, 2014, 190(8):732-738. DOI:10.1007/s00066-014-0642-0. [21] Jin JY, Huang Y, Brown SL, et al. Radiation dose-fractionation effects in spinal cord:comparison of animal and human data[J]. J Radiat Oncol, 2015, 4(3):225-233. DOI:10.1007/s13566-015-0212-9. [22] Barendsen GW. Dose fractionation, dose rate and iso-effect relationships for normal tissue responses[J]. Int J Radiat Oncol Biol Phys, 1982, 8(11):1981-1997. doi: 10.1016/0360-3016(82)90459-X [23] Maciejewski B, Taylor JM, Withers HR. Alpha/beta value and the importance of size of dose per fraction for late complications in the supraglottic larynx[J]. Radiother Oncol, 1986, 7(4):323-326. doi: 10.1016/S0167-8140(86)80061-5 [24] Brenner DJ. Fractionation and late rectal toxicity[J]. Int J Radiat Oncol Biol Phys, 2004, 60(4):1013-1015. DOI:10.1016/j.ijrobp.2004.04.014. [25] Miralbell R, Robert SA, Zubizarreta E, et al. Dose-fraction sensitivity of prostate cancer deduced from radiotherapy outcomes of 5969 patients in seven international institutional datasets:α/β=1.4(0.9-2.2) Gy[J]. Int J Radiat Oncol Biol Phys, 2012, 82(1):e17-24. DOI:10.1016/j.ijrobp.2010.10.075. [26] Turesson I, Notter G. The influence of fraction size in radiotherapy on the late normal tissue reaction -Ⅰ:Comparison of the effects of daily and once-a-week fractionation on human skin[J]. Int J Radiat Oncol Biol Phys, 1984, 10(5):593-598. doi: 10.1016/0360-3016(84)90289-X [27] Machtay M, Bae K, Movsas B, et al. Higher biologically effective dose of radiotherapy is associated with improved outcomes for locally advanced non-small cell lung carcinoma treated with chemoradiation:an analysis of the radiation therapy oncology group[J]. Int J Radiat Oncol Biol Phys, 2012, 82(1):425-434. DOI:10.1016/j.ijrobp.2010.09.004. [28] Xia B, Chen GY, Cai XW, et al. The effect of bioequivalent radiation dose on survival of patients with limited-stage small-cell lung cancer[J]. Radiat Oncol, 2011, 6:50. DOI:10.1186/1748-717X-6-50. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 3399
- HTML全文浏览量: 2461
- PDF下载量: 5