



-
Graves甲状腺功能亢进症(简称甲亢)患者伴有骨量减少甚至骨质疏松,这已引起临床医师的普遍重视。131I治疗通过破坏甲状腺滤泡,使甲状腺激素水平恢复正常或降低,骨转化动力减弱,骨代谢可趋于正常[1]。双能X线吸收法(dual energy X-ray absorptiometry, DXA)测定骨密度(bone mineral density, BMD)是目前诊断骨质疏松的有效手段与金标准,并能很好地预测骨折风险[2],但腰椎骨质增生会造成常规前后位BMD测定结果的假阳性增高,影响对患者骨量的准确评价[3]。腰椎能谱CT可通测定椎体中间层面松质骨中钙(水)的含量,更加灵敏、精确地评价骨矿含量[4]。本研究通过能谱CT测定68例Graves甲亢患者腰椎钙(水)密度,分析其与DXA测定BMD结果的相关性,并了解131I治疗前后腰椎钙(水)密度的变化,探讨能谱CT成像对Graves甲亢患者骨量评估的价值,以及131I治疗对甲亢患者骨量的影响。
-
收集2015年6月至10月期间在我科住院首次接受131I治疗、随访半年以上且临床资料齐全的68例Graves甲亢患者作为研究对象,其中男性13例,女性55例,年龄21~67(40.6±10.7)岁,病程1个月至20年。将女性未绝经者及男性≤50岁定义为青年组,而将绝经后女性及>50岁男性定义为高龄组。诊断及入选标准包括:高代谢症候群,FT3、FT4水平升高及TSH水平降低,同时具备甲状腺肿大、突眼、胫前黏液性水肿、血清甲状腺刺激免疫球蛋白[本研究为促甲状腺素受体抗体(thyrotrophin receptor antibody,TRAb)]阳性之一者,甲状腺吸131I率增高(或ECT检查可见甲状腺摄取核素能力增强)[5]。所有患者均除外合并肝、肾功能损害、其他内分泌疾病及骨关节病史,无应用钙剂、维生素D及糖皮质激素史。
-
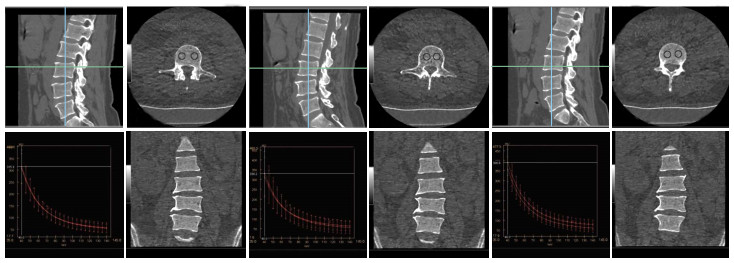
常规采集病史,进行体格检查,检测血清FT3、FT4、TSH、TRAb、抗甲状腺球蛋白抗体、甲状腺过氧化物酶抗体水平,甲状腺行超声检查估算重量,测定甲状腺最高摄131I率及有效半衰期,采用美国Lunar公司的DPX-L型双能X线骨密度仪测定腰椎BMD。根据国际BMD测量标准将测定结果分为骨量正常组(T或Z值>-1标准差)、骨量减低组(T或Z值-1~ -2.5标准差)和骨质疏松组(T或Z值≤ -2.5标准差)[6]。腰椎CT采集图像,扫描参数:管电压在140 kVp和80 kVp瞬时切换,自动mAs,辐射剂量为14.4 mGy,后台重建成1.25 mm层厚的钙(水)密度图像,由两名影像专业的主治医师分别测量钙(水)密度值,选取第3腰椎上、中、下3个层面,每个层面勾画2~3个大小为90~100 mm2的ROI,ROI应距离椎体边缘3 mm以上,并避开椎后静脉丛及骨岛等影响因素,将测量结果取平均值,获得该椎体的钙(水)密度值(图 1)。
图 1 能谱CT测量Graves甲状腺功能亢进症患者第3腰椎钙(水)密度图
Figure 1. The calcium-water concentration measurement of Graves hyperthyroidism patient's L3 by CT spectral imaging
我们采用计算剂量法结合患者自身因素进行适当调整而得到个体化131I治疗剂量(具体方法参见131I治疗格雷夫斯甲亢指南推荐的第22项),并一次性给予患者服用[7]。本研究患者口服131I剂量为74~555 MBq(2~15 mCi),平均剂量为(240.5±88.8)MBq[(6.5±2.4)mCi]。
全部病例均随访半年以上,依据《131I治疗格雷夫斯甲亢指南(2013版)》评价131I治疗甲亢的疗效[7]。治疗后半年复查甲状腺功能以及腰椎能谱CT。所有患者均在治疗前签署了知情同意书。
-
应用SPSS15.0软件进行统计学分析。所有数据用均数±标准差(x±s)表示,不同性别及年龄组DXA测定的腰椎BMD比较采用独立样本t检验(符合正态分布且方差齐);不同骨量组别的第3腰椎钙(水)密度比较采用非参数统计Kruskal-Wallis H检验及Mann-Whitney U检验(因各组间方差不齐),不同骨量组别的第3腰椎BMD比较采用单因素方差分析,腰椎能谱CT与DXA测定结果的关系采用Pearson相关分析及线性回归分析;Graves甲亢患者治疗前后腰椎钙(水)密度的比较采用配对t检验。P < 0.05表示差异有统计学意义。
-
DXA测定腰椎BMD的结果显示,68例Graves甲亢患者中骨量正常40例(58.8%),骨量减少21例(30.9%),骨质疏松7例(10.3%)。男性甲亢患者的BMD(0.92±0.35)g/cm3与女性患者(1.03±0.25)g/cm3比较,差异无统计学意义(t=-1.284,P>0.05)。高龄组患者的BMD(0.72±0.35)g/cm3低于青年组患者(1.03±0.29)g/cm3,差异有统计学意义(t=-3.660,P < 0.01)。高龄组患者的BMD(0.72±0.35)g/cm3低于青年组患者[(1.03±0.29)g/cm2],差异有统计学意义(t=-3.660, P < 0.01)。
骨量正常组患者、骨量减少组、骨质疏松组进行第3腰椎钙(水)密度比较,3组间差异有统计学意义(χ2=35.811,P < 0.001)。骨量正常组腰椎钙(水)密度高于骨量减少组与骨质疏松组,差异均有统计学意义(Z=4.903、3.974,均P < 0.001),骨量减少组腰椎钙(水)密度高于骨质疏松组,差异有统计学意义(Z=-3.502, P < 0.001)(表 1)。
组别 例数 最小值 最大值 x±s χ2值 P值 骨量正常组 40 34.62 112.48 64.33±14.65 35.811 0.000 骨量减少组 21 36.96 55.77 48.29±4.45 骨质疏松组 7 40.22 43.30 41.65±1.21 表 1 不同骨量组别的Graves甲状腺功能亢进症患者第3腰椎钙(水)密度比较(g/cm3)
Table 1. Comparison of calcium (water) densities of L3 in Graves hyperthyroidism patients with different bone mass(g/cm3)
骨量正常组患者的第3腰椎BMD为(1.252±0.305)g/cm2,骨量减少组为(1.103±0.254)g/cm2,而骨质疏松组为(0.539±0.066)g/cm2,3组间差异有统计学意义(F=12.968, P < 0.001)。其中骨量正常组和骨量减少组第3腰椎BMD的差异无统计学意义(t=1.910, P>0.05),但均高于骨质疏松组(t=6.294、4.589, 均P < 0.001)(表 2)。
组别 例数 最小值 最大值 x±s χ2值 F值 骨量正常组 40 1.04 1.44 1.252±0.305 12.968 0.000 骨量减少组 21 0.96 1.32 1.103±0.254 骨质疏松组 7 0.42 0.60 0.539±0.066 表 2 不同骨量组别的Graves甲状腺功能亢进症患者第3腰椎骨密度比较(g/cm2)
Table 2. Comparison of bone mineral densitys of L3 in Graves hyperthyroidism patients with different bone mass (g/cm2)
-
以DXA测定的腰椎BMD为横坐标,能谱CT测定第3腰椎钙(水)密度为纵坐标,将每例甲亢患者成对的数据描述在直角坐标系上,形成散点图(图 2)。由图 2可见二者大致呈线性正相关趋势。
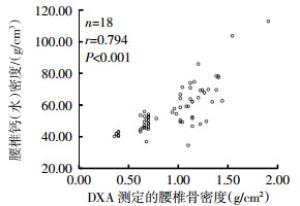
图 2 Graves甲亢患者腰椎能谱CT与DXA测定结果的相关性
Figure 2. The relationship between calcium(water) densities and BMDs in Graves hyperthyroidism patients
由图 2可见,DXA测定的BMD在1.0~1.5 g/cm2范围内,椎体钙(水)密度值波动比较大。将BMD测定结果代入线性回归方程计算所得的椎体钙(水)密度与实测值进行比较,其中8例患者二者接近(差异≤2 g/cm3),7例患者后者高于前者,而另外15例(占50%)患者前者高于后者。这15例患者的年龄为(48.2±5.7)岁,其中10例患者相应CT图像见腰椎骨质增生。
进一步对甲亢患者的第3腰椎钙(水)密度与DXA测定的腰椎BMD进行Pearson相关分析,结果呈高度相关(r=0.794)。对其进行假设检验,检验水准α=0.01、t=10.605、P < 0.001,故可认为二者之间有正相关关系。由线性回归分析得到线性回归方程:第3腰椎钙(水)密度=24.485+34.529腰椎BMD。由此可见,我们可以用Graves甲亢患者的腰椎钙(水)密度来评估患者骨量。
-
全部患者131I治疗后半年复查腰椎能谱CT,再次测定第3腰椎钙(水)密度值,131I治疗后Graves甲亢患者的腰椎钙(水)密度(62.23±11.77)g/cm3较治疗前(57.04±14.54)g/cm3增加,即患者的骨量改善,差异有统计学意义(t=8.84,P < 0.001)。
-
本组68例Graves甲亢患者131I治疗后随访半年,完全缓解36例,甲状腺功能减退(简称甲减)15例,部分缓解13例,无效或复发4例。我们将完全缓解及甲减定义为甲亢治愈,将部分缓解、无效或复发定义为甲亢未愈。甲亢治愈组患者131I治疗后腰椎钙(水)密度(65.01±11.74)g/cm3较治疗前(59.26±15.61)g/cm3增加(t=7.86,P < 0.001),而甲亢未愈组患者治疗后腰椎钙(水)密度(52.17±7.65)g/cm3较治疗前(50.39±7.82)g/cm3变化不显著,差异无统计学意义(t=2.29,P=0.062)。
-
Graves甲亢是一种常见的自身免疫性甲状腺疾病,除表现为甲状腺腺体合成和分泌过多的甲状腺激素,引起以神经、循环、消化等系统兴奋性增高和代谢亢进的症候群外,过多的甲状腺激素还会引起骨矿物质代谢紊乱,加速骨吸收,导致骨质疏松,严重者甚至发生骨折[8-9]。其可能的机制包括:①过多分泌的甲状腺激素直接作用于骨骼,使骨转换加快;②甲状腺激素的分泌增多干扰了活性维生素D3的生成,从而导致肠道钙吸收降低;③甲亢患者经常腹泻,容易出现负钙、负磷平衡;④甲亢时由于分解代谢加速,引起钙、磷代谢紊乱,可出现高转换性骨质疏松[10-12]。
DXA是测定BMD的标准方法,其精确度高、重复性好。本研究的腰椎BMD测定结果显示,30.9%(21/68)的Graves甲亢患者伴有骨量减少,10.3%(7/68)的患者伴有骨质疏松。高龄组甲亢患者腰椎BMD低于青年组,与健康人群变化规律类似,但已有研究证实甲亢患者的骨密度明显低于性别和年龄相匹配的正常人群,尤其是女性和高龄患者[8, 13]。
能谱CT的基物质成像技术是近年来开发的可比较简单准确地测量骨密度的新技术。它通过高低瞬间切换技术,获得两组能量数据进行基物质密度成像。当基物质恰好是组织中含有的两种主要成分时,则可以反映组织内该物质的相对含量[4]。陈靖等[14]利用能谱CT定量分析腰椎中钙的含量,证实可选择钙和水作为配对的基物质,获得骨小梁中钙的含量,来达到间接定量评估骨量的目的。本研究通过腰椎能谱CT测定Graves甲亢患者第3腰椎钙(水)密度,并与同一患者DXA测量的腰椎BMD结果进行相关性分析,证实二者呈高度正相关(r=0.794),故可将腰椎能谱CT定量分析技术用于Graves甲亢患者骨量的评估。
然而DXA是一种区域面密度测量方法,易受多种外部因素的干扰,如腰椎间盘的退行性改变、骨质增生及运动终板硬化症等均可导致腰椎BMD的假性增高[3, 15]。本研究结果显示,30例DXA测定的BMD在1.0~1.5 g/cm2范围内的患者中,15例平均年龄在(48.2±5.7)岁的患者根据BMD结果推算的腰椎钙(水)密度值要高于实测值,其中10例(约占66.67%)患者合并有骨质增生。可见对伴有腰椎骨质增生的部分中老年患者,DXA测定的BMD结果可能会高估患者的骨量状况。
DXA的测量结果包括皮质骨和松质骨在内的所有骨量的总和,但二者的代谢转换率不同,皮质骨的存在会降低观察治疗反应的敏感性[16]。能谱CT可以区分开皮质骨和松质骨,在非侵入性地评估治疗反应方面具有非常大的潜力[17],故可以更灵敏地评估Graves甲亢患者131I治疗前后骨量的变化。本研究采用能谱CT测定的腰椎钙(水)密度来评估Graves甲亢患者131I治疗后骨量的变化,结果证实,131I治疗后患者的腰椎钙(水)密度较治疗前增加,患者的骨量得到改善。我们进一步分析Graves甲亢经131I治疗后转归与骨量变化的关系,结果显示,甲亢治愈组患者的腰椎钙(水)密度较治疗前明显增加,而甲亢未愈组患者较治疗前差异无统计学意义。其原因可能为甲亢治愈组患者甲状腺激素水平恢复正常或低于正常,骨转换的动力减弱,骨代谢随之趋于正常;而未愈组患者增高的甲状腺激素可导致骨转换加速,骨矿物质丢失,骨量改善不明显。经131I治疗的Graves甲亢患者即使未采用抗骨质疏松治疗,BMD也可恢复正常,与既往的研究结果基本一致[1, 12, 18]。
Graves甲亢患者如合并有骨量减少甚至骨质疏松,可优先考虑131I治疗,因为甲亢的有效缓解有利于骨代谢的恢复。本研究尚存在一些不足,如样本量较小,未能对病程长短不同、病情严重程度不一的Graves甲亢患者的骨量状况及131I治疗前后变化进行分层分析;未进一步分析经131I干预治疗后能谱CT测得的钙(水)密度值与DXA测定的腰椎BMD的关系,未比较采取补充维生素D及钙剂等干预治疗对骨量的影响等。
腰椎能谱CT评估Graves甲状腺功能亢进症患者131I治疗前后骨量变化的价值
Changes of bone mass in patients with Graves' hyperthyroidism before and after 131I therapy based on CT spectral imaging
-
摘要:
目的探讨能谱CT成像对Graves甲状腺功能亢进症(简称甲亢)患者骨量评估的价值,以及131I治疗对Graves甲亢患者骨量的影响。 方法收集2015年6月至10月期间在我科接受131I治疗的68例Graves甲亢患者[(男性13例、女性55例,年龄(40.6±10.7)岁],治疗前采用双能X线吸收法(DXA)测定腰椎骨密度(BMD),能谱CT测定第3腰椎钙(水)密度,采用Pearson相关分析及线性回归探讨二者的相关性。治疗后半年随访评价疗效,复查腰椎能谱CT,采用配对t检验比较131I治疗前后骨量变化。 结果DXA的测定结果显示,68例Graves甲亢患者中有21例伴有骨量减少(30.9%),7例伴有骨质疏松(10.3%)。骨量正常组患者的第3腰椎钙(水)密度为(64.33±14.65)g/cm3,骨量减少组为(48.29±4.45)g/cm3,而骨质疏松组为(41.65±1.21)g/cm3,3组间差异有统计学意义(χ2=35.811,P < 0.001)。骨量正常组患者的第3腰椎BMD为(1.252±0.305)g/cm2,骨量减少组为(1.103±0.254)g/cm2,而骨质疏松组为(0.539±0.066)g/cm2,3组间差异有统计学意义(F=12.968,P < 0.001)。Graves甲亢患者的第3腰椎钙(水)密度与DXA测定的腰椎BMD呈高度正相关(r=0.794,假设检验水准α=0.01,t=10.605,P < 0.001)。由线性回归分析得到线性回归方程:第3腰椎钙(水)密度=24.485+34.529腰椎BMD。治疗后半年随访发现,甲亢治愈组患者131I治疗后腰椎钙(水)密度较治疗前增加,骨量改善,差异有统计学意义(t=7.86,P < 0.001);而甲亢未愈组患者较治疗前变化不显著,差异无统计学意义(t=2.29,P=0.062)。 结论能谱CT测得的腰椎钙(水)密度可用于评估Graves甲亢患者的骨量。患者经131I治疗后,骨量可随着甲亢的有效缓解而显著改善。 Abstract:ObjectiveTo investigate the value of CT spectral imaging to evaluate bone mass in patients with Graves' hyperthyroidism, and the changes of bone mass before and after 131I therapy. MethodsSixty-eight patients(13 males, 55 females; age 40.6±10.7yr) with Graves' hyperthyroidism who received 131I therapy from June to October 2015 were involved in our study. The bone mineral density(BMD) of lumbar was obtained by dual energy X-ray absorptiometry(DXA), and the calcium-water concentration of L3 was measured by CT spectral imaging before 131I therapy. Pearson correlation analysis and linear regression were performed to explore the relationship between them. All clinical data were collected to assess the efficacy of 131I therapy after 6 months. CT spectral imaging was repeated, in order to compare the changes of bone mass using comparative t-test. ResultsOf these patients with Graves' hyperthyroidism, 30.9% (21/68) patients with osteopenia and 10.3%(7/68) patients with osteoporosis were diagnosed according to the results of BMD by DXA. The calcium (water) densities of L3 were (64.33±14.65), (48.29±4.45) and (41.65±1.21) g/cm3 in patients with normal bone mass, bone loss and osteoporosis, respectively. The differences between the three groups were statistically significant (χ2=35.811, P < 0.001). The bone mineral density of L3 were (1.252±0.305), (1.103±0.254) and (0.539±0.066) g/cm3 in patients with normal bone mass, bone loss and osteoporosis, respectively. The differences between the three groups were statistically significant (F=12.968, P < 0.001). The calcium-water concentrations of L3 (g/cm3) were highly correlated with BMD values (g/cm2) of lumbar determined by DXA(r=0.794, hypothesis testing standard α=0.01, t=10.605, P < 0.001). Equation of linear regression:the calcium-water concentration of L3=24.485+34.529 BMD value of lumbar. Furthermore, after 131I therapy, the calcium-water concentrations of L3 increased(t=7.86, P < 0.001) in the cured group of patients. But there weren't significant difference in the uncured group of patients(t=2.29, P=0.062). ConclusionsCT spectral imaging can be used to evaluate bone mass in patients with Graves' hyperthyroidism. Bone mass can be improved with remission of hyperthyroidism after 131I therapy. -
Key words:
- Graves disease /
- Hyperthyroidism /
- Tomograp, X-ray computed /
- Bone mass /
- Radionuclide therapy /
- Iodine Radioisotopes
-
图 1 能谱CT测量Graves甲状腺功能亢进症患者第3腰椎钙(水)密度图
Figure 1. The calcium-water concentration measurement of Graves hyperthyroidism patient's L3 by CT spectral imaging
图 2 Graves甲亢患者腰椎能谱CT与DXA测定结果的相关性
Figure 2. The relationship between calcium(water) densities and BMDs in Graves hyperthyroidism patients
表 1 不同骨量组别的Graves甲状腺功能亢进症患者第3腰椎钙(水)密度比较(g/cm3)
Table 1. Comparison of calcium (water) densities of L3 in Graves hyperthyroidism patients with different bone mass(g/cm3)
组别 例数 最小值 最大值 x±s χ2值 P值 骨量正常组 40 34.62 112.48 64.33±14.65 35.811 0.000 骨量减少组 21 36.96 55.77 48.29±4.45 骨质疏松组 7 40.22 43.30 41.65±1.21  下载: 导出CSV
下载: 导出CSV
表 2 不同骨量组别的Graves甲状腺功能亢进症患者第3腰椎骨密度比较(g/cm2)
Table 2. Comparison of bone mineral densitys of L3 in Graves hyperthyroidism patients with different bone mass (g/cm2)
组别 例数 最小值 最大值 x±s χ2值 F值 骨量正常组 40 1.04 1.44 1.252±0.305 12.968 0.000 骨量减少组 21 0.96 1.32 1.103±0.254 骨质疏松组 7 0.42 0.60 0.539±0.066
下载: 导出CSV
-
[1] 高继兵, 蔡善武, 黄海泉, 等.甲亢131Ⅰ治疗前后骨密度及相关指标变化分析[J].中华核医学杂志, 2005, 25(4):237-239. doi: 10.3760/cma.j.issn.2095-2848.2005.04.016
Gao JB, Cai SW, Huang HQ, et al. Changes of bone mineral density and related parameters in patients of hyperthyroidism before and after 131I therapy[J]. Chin J Nucl Med, 2005, 25(4):237-239. doi: 10.3760/cma.j.issn.2095-2848.2005.04.016[2] El MA, Roux C. DXA scanning in clinical practice[J]. QJM, 2008, 101(8):605-617. DOI:10.1093/qjmed/hcn022. [3] Karabulut O, Tuncer MC, Karabulut Z, et al. Relationship between radiographic features and bone mineral density in elder men[J]. Folia Morphol (Warsz), 2010, 69(3):170-176. [4] 陈靖, 郑邵微, 苗延巍, 等.能谱CT定量钙(水)密度技术对腰椎椎体内及椎体间骨密度差异的研究[J].大连医科大学学报, 2015, 37(3):289-292. DOI:10.11724/jdmu.2015.03.21.
Chen J, Zheng SW, Miao YW, et al. Intra and inter vertebral calcium(water) density variation measured by Gemstone Spectral Imaging[J]. J Dalian Med Univ, 2015, 37(3):289-292. DOI:10.11724/jdmu.2015.03.21.DOI:10.11724/jdmu.2015.03.21.[5] 蒋宁一, 匡安仁, 谭建, 等. 131I治疗Graves甲亢专家共识[J].中华核医学与分子影像杂志, 2010, 30(5):346-351. DOI:10.3760/cma.j.issn.0253-9780.2010.05.019.
Jiang NY, Kuang AR, Tan J, et al. Expert consensus for 131I treatment of Graves hyperthyroidism[J]. Chin J Nucl Med Mol Imaging, 2010, 30(5):346-351.DOI:10.3760/cma.j.issn.0253-9780.2010.05.019.[6] 袁园, 卫红艳, 刘萍, 等.甲状腺功能亢进对骨代谢影响[J].临床荟萃, 2012, 27(3):206-209.
Yuan Y, Wei HY, Liu P, et al. Effect of hyperthyroidism on bone metabolism[J]. Clin Focus, 2012, 27(3):206-209.[7] 蒋宁一, 林岩松, 关海霞, 等. 131I治疗格雷夫斯甲亢指南[J].中华核医学与分子影像杂志, 2013, 33(2):83-95. DOI:10.3760/cma.j.issn.2095-2848.2013.02.002.
Jiang NY, Lin YS, Guan HX, et al. Clinical guidelines for 131I treatment of Graves hyperthyroidism[J]. Chin J Nucl Med Mol Imaging, 2013, 33(2):83-95. DOI:10.3760/cma.j.issn.2095-2848. 2013.02.002.[8] 邱明琪, 胡美华.甲状腺功能亢进症患者骨密度变化的临床分析[J].实用临床医学, 2012, 13(6):16-17, 20. DOI:10.3969/j.issn.1009-8194.2012.06.006.
Qiu MQ, Hu MH. Bone mineral density in patients with hyperthyroidism[J]. Pract Clin Med, 2012, 13(6):16-17, 20. DOI:10.3969/j.issn.1009-8194.2012.06.006.[9] Dhanwal DK. Thyroid disorders and bone mineral metabolism[J]. Indian J Endocrinol Metab, 2011, 15(Suppl 2):S107-112. DOI:10.4103/2230-8210.83339. [10] Gorka J, Taylor-Gjevre RM, Arnason T. Metabolic and clinical consequences of hyperthyroidism on bone density[J/OL]. Int J Endocrinol, 2013, 2013: 638727[2018-03-07]. https://www.ncbi.nlm.nih.gov/pubmed/23970897. DOI: 10.1155/2013/638727. [11] Tuchendler D, Bolanowski M. The influence of thyroid dysfunction on bone metabolism[J]. Thyroid Res, 2014, 7(1):12. DOI:10.1186/s13044-014-0012-0. [12] 王勇, 丁勇, 邢家骝, 等.甲状腺功能亢进患者131碘治疗前后骨密度的变化[J].临床荟萃, 2015, 30(1):74-77. DOI:10.3969/j.issn.1004-583X.2015.01.020.
Wang Y, Ding Y, Xing J L, et al. Bone mineral density change in hyperthyroidism patients before and after 131I treatment[J]. Clin Focus, 2015(1):74-77. DOI:10.3969/j.issn.1004-583X.2015. 01.020.[13] 张红, 叶爱玲, 廖二元.女性甲状腺功能亢进症患者的骨密度变化[J].中南大学学报(医学版), 2008, 33(5):452-455. DOI:10.3321/j.issn:1672-7347.2008.05.015.
Zhang H, Ye AL, Liao EY. Change in bone mineral density in female patients with hyperthyroidism[J]. J Cent South Univ (Med Sci), 2008, 33(5):452-455. DOI:10.3321/j.issn:1672-7347. 2008. 05.015.[14] 陈靖, 董越, 葛莹, 等.探讨能谱CT宝石能谱成像技术用于骨密度测量的可行性[J].中国医学影像技术, 2013, 29(1):133-137.
Chen J, Dong Y, Ge Y, et al. Feasibility of bone density measurement based on CT gemstone spectral imaging[J]. Chin J Med Imaging Technol, 2013, 29(1):133-137.[15] Grampps S. Radiology of osteoporosis[M]. Berlin:Springer, 2008:163-173. [16] 张昕, 王峻, 苏晋生, 等.定量CT与双能X线吸收测定仪测量腰椎各椎体间骨密度差异性研究[J].中国医学影像学杂志, 2011, 19(12):884-886, 930. DOI:10.3969/j.issn.1005-5185. 2011. 12.002.
Zhang X, Wang J, Su JS, et al. Differences of BMD betweenlumbar vertebrae measured by QCT and DXA[J]. Chin J Med Imaging, 2011, 19(12):884-886, 930. DOI:10.3969/j.issn.1005-5185. 2011. 12.002.[17] Anderson NG, Butler AP. Clinical applications of spectral molecular imaging:potential and challenges[J]. Contrast Media Mol Imaging, 2014, 9(1):3-12. DOI:10.1002/cmmi.1550. [18] Vestergaard P, Mosekilde L. Hyperthyroidism, bone mineral, and fracture risk-a meta-analysis[J]. Thyroid, 2003, 13(6):585-593. DOI:10.1089/105072503322238854. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 3522
- HTML全文浏览量: 2396
- PDF下载量: 10