


 下载:
下载:
-
肺大细胞神经内分泌癌(large cell neuroendocrine carcinoma, LCNEC)是一种少见的神经内分泌癌,具有恶性度高、侵袭性强、预后较差等特点[1]。肺LCNEC的临床特征及影像学表现缺乏特异性,诊断较为困难,误诊率较高。以往对肺LCNEC的影像学表现多集中在CT研究,而在PET/CT显像特征方面的研究少见。我们回顾性分析37例肺LCNEC患者的临床资料,分析其18F-FDG PET/CT的影像学表现,旨在提高对该病的认识。
-
收集2009年10月至2017年5月在我院接受18F-FDG PET/CT检查并经病理证实为肺LCNEC的37例患者的临床资料,其中9例经穿刺活检病理证实、28例经手术病理证实。所有患者中男性30例、女性7例,年龄47~82岁,中位年龄61岁。纳入标准:①病理结果证实为肺LCNEC;② 18F-FDG PET/CT检查资料完整;③ PET/CT检查前均未接受任何肿瘤相关治疗。排除标准:①合并其他恶性肿瘤病史;②有胸部手术史;③临床资料及PET/CT显像资料不完整。所有患者中临床表现为咳嗽、咳痰者19例,其中6例伴痰中带血;胸痛者5例;胸闷者3例;咯血2例;余8例患者无明显症状,常规体检发现肺部占位。28例接受手术的肺LCNEC患者,临床分期根据第八版国际肺癌肿瘤-淋巴结-转移(tumor-node-metastasis, TNM)分期标准进行分期,9例行穿刺活检的患者临床分期参考PET/CT显像结果,其中Ⅰ期22例(ⅠA2期9例、ⅠA3期4例、ⅠB期9例)、Ⅱ期5例(ⅡA期1例、ⅡB期4例)、Ⅲ期7例、Ⅳ期3例。
-
PET/CT显像仪为德国西门子公司生产的Biograph 16 HR型,显像剂18F-FDG由我院核医学科自制,放化纯度>95%。所有患者检查前禁食6 h以上,测空腹指尖血糖并控制血糖≤7.0 mmol/L,经肘静脉注射18F-FDG 3.70~5.55 MBq/kg后休息60 min,排空膀胱后行PET/CT检查,先行CT扫描,CT扫描参数:管电压120 kV,管电流140 mA,层厚3.75 mm,准直1.5 mm。PET数据采集采用三维模式,采集6~7个床位,每个床位2~3 min。应用CT数据进行衰减校正,迭代法重建。所有患者在PET/CT扫描结束时,再行胸部屏气CT扫描:电压120 kV,电流205 mA,层厚5 mm,均行1.5 mm薄层重建。
由2位核医学副主任医师共同阅片,意见不一致时共同协商解决。重点观察病灶的位置、形态、大小、密度及边缘情况等。沿肺LCNEC病灶最大层面勾画ROI,由软件自动得出原发灶的SUVmax,在胸部屏气CT纵隔窗图像上测量肿瘤最大径。
-
采用SPSS 17.0软件对数据进行统计学分析。计量资料符合正态分布,采用均数±标准差表示。SUVmax与肿瘤最大径的相关性采用Pearson相关性分析。采用受试者工作特性(receiver operating characteristic,ROC)曲线计算诊断的灵敏度、特异度及曲线下面积(area under curve,AUC)。P<0.05表示差异有统计学意义。
-
37例患者均为单发,其中周围型28例(28/37,75.7%)、中央型9例(9/37,24.3%)。病灶位于左肺20例(20/37,54.1%),包括左肺上叶12例、左肺下叶8例;位于右肺17例(17/37,45.9%),包括右肺上叶9例、右肺中叶1例、右肺下叶7例。26例病灶(26/37,70.3%)呈圆形或类圆形,11例病灶(11/37,29.7%)形态不规则。肿瘤最大径1.3~7.4(3.2±1.5)cm。
30例病灶(30/37,81.1%)可见分叶征,多为浅分叶;10例病灶(10/37,27.0%)可见毛刺征,其中2例表现为长毛刺、8例为短毛刺。29例病灶(29/37,78.4%)边界清晰,8例病灶边界不清。5例伴有阻塞性肺炎,1例伴有阻塞性肺不张,9例病灶(9/37,24.3%)可见胸膜凹陷征。
33例病灶(33/37,89.2%)密度均匀,2例病灶可见液化坏死,1例病灶可见空洞形成,1例病灶内见点状钙化,1例病灶内见充气支气管征。
-
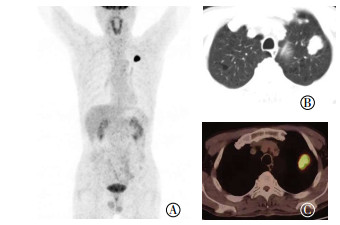
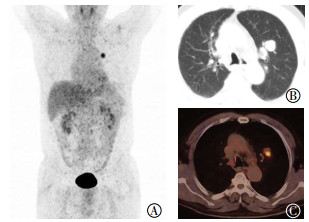
37例患者的病灶18F-FDG代谢程度均高于肝脏,其中34例的病灶(34/37,91.9%)18F-FDG代谢均匀性增高、3例18F-FDG代谢呈环状增高。SUVmax为11.7±5.2(3.3~25.3)。SUVmax与肿瘤最大径呈正相关(r=0.569,P=0.000),典型病例的PET/CT图像见图 1、2。
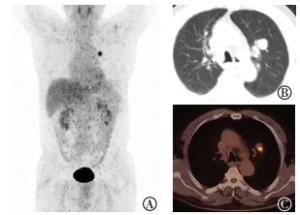
图 1 左肺上叶肺大细胞神经内分泌癌的PET/CT显像图
Figure 1. The PET/CT image of large cell neuroendocrine carcinoma in left upper lung: male of 73 years old
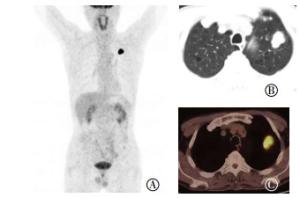
图 2 左肺上叶肺大细胞神经内分泌癌(ⅡB期)的PET/CT显像图
Figure 2. The PET/CT image of large cell neuroendocrine carcinoma in left upper lung: male of 58 years old
-
15例病灶伴有肺门和(或)纵隔淋巴结转移;8例可见远处转移,包括骨转移4例、肾上腺转移1例、肝脏及骨转移2例、肾上腺及骨转移1例。
-
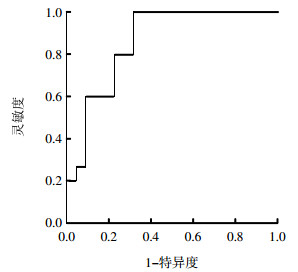
15例伴有淋巴结转移的肺LCNEC原发灶SUVmax为15.2±4.4, 22例无淋巴结转移的肺LCNEC原发灶SUVmax为9.3±4.2,二者差异有统计学意义(t=-4.106,P=0.000)。ROC曲线分析结果显示,AUC为0.858,95%置信区间为0.738~0.977(图 3)。约登指数最大为0.573,所对应的SUVmax为11.9,为诊断淋巴结转移的最佳界值点,灵敏度为80.0%,特异度为77.3%。这说明SUVmax越大,诊断的灵敏度越低,特异度越高。
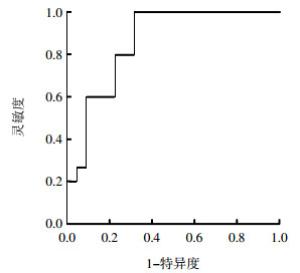
图 3 肺大细胞神经内分泌癌患者18F-FDG PET/CT显像原发肿瘤SUVmax预测淋巴结转移状态的ROC曲线分析
Figure 3. The receiver operating characteristic curve of 18F-FDG PET/CT imaging to predict the lymphatic metastasis
-
肺LCNEC是一类低分化、高度恶性的神经内分泌癌,其特点是预后不良,发病率较低,多见于中老年男性,中位发病年龄为60岁。其临床表现无特异性,多表现为咳嗽、咳痰、咯血和胸痛等。本研究37例患者,年龄47~82,中位年龄61岁,其中男性30例(男女比例4.3 : 1),临床表现以咳嗽、咳痰者多见,与文献报道[2-4]基本一致。
肺LCNEC的影像学表现以往多见于CT研究,表现为双肺均可发生,好发于双肺上叶,周围型多见,多呈类圆形,边缘光滑,毛刺少见,密度较均匀,肿瘤较大时可出现坏死,钙化少见[5-6]。而PET/CT集CT的解剖形态成像与PET的功能代谢显像于一身,不仅可以观察病灶的CT特征,还能分析病灶的代谢情况,在肿瘤的诊断、分期及疗效评价方面具有明显的优势[7]。目前,关于肺LCNEC的PET/CT表现,文献报道少见。Lee等[8]报道了31例肺LCNEC的18F-FDG PET/CT表现,结果显示周围型23例、中央型8例;20例病灶边缘光滑,29例可见分叶征,13例可见毛刺征,2例可见充气支气管征,2例可见钙化,胸膜凹陷征9例,所有病灶均未见空洞;病灶的中位SUVmax为8.9,范围3.1~17.2。另一项研究回顾性分析了16例肺LCNEC的18F-FDG PET/CT显像资料,SUVmax为13.7±7.4(5.0~31.9)[9]。本研究37例患者均为单发,其中28例(28/37,75.7%)为周围型,30例病灶(30/37,81.1%)可见分叶征,多为浅分叶,这提示肺LCNEC多为发生在外周的肺内结节或肿块,而肿瘤分叶是由于肿瘤在各个方向生长速度不一致或受肺内正常结构制约所致,大部分肺LCNEC可见分叶,这提示肿瘤呈膨胀性或堆积性生长。本研究有10例病灶可见毛刺征,9例病灶可见胸膜凹陷征,这提示肿瘤可刺激引起周围纤维结缔组织增生,并可对邻近胸膜进行牵拉;仅1例病灶内见充气支气管征,这表明肿瘤很少出现癌细胞沿支气管或肺泡伏壁生长。肺LCNEC恶性程度高,本研究37例病灶18F-FDG摄取均高于肝脏,SUVmax为11.7±5.2,SUVmax与肿瘤最大径呈正相关,这些结果在一定程度上反映了肿瘤的生物学行为:肿瘤恶性度越高,细胞增殖越快,肿瘤葡萄糖代谢越旺盛,病灶摄取18F-FDG则越高。
肺LCNEC可发生远处转移,一项研究报道了22例肺LCNEC的CT表现,其中发生骨转移6例、肝转移4例、肾上腺转移2例[10]。PET/CT一次成像可观察病灶的全身分布情况,在诊断恶性肿瘤远处转移方面具有明显的优势。本研究37例患者中,8例发现远处转移,其中最常见的是骨转移,与文献报道[10]基本一致。
肺LCNEC恶性程度高,预后差,中位生存期相对较短。一项研究回顾性分析22例肺LCNEC的临床资料,经过中位随访21.3个月,13例患者死亡,中位生存期为16.8个月,2年生存率仅为18.2%,经过多因素生存分析表明淋巴结转移是影响患者预后的独立危险因素[11]。由此可见,淋巴结转移状态与患者的预后密切相关,而判断淋巴结转移的金标准是病理学检查,但是其只能在手术取得活组织标本后才能实施,而对于那些不能手术或不能耐受手术的患者,判断淋巴结转移就存在一定的困难。目前,临床多采用常规影像学技术来判断淋巴结转移情况,如CT或MRI等,但是常规影像学技术多是通过淋巴结大小来判断淋巴结转移情况,而肿大淋巴结不一定发生转移,较小的淋巴结也可能已经发生了转移。因此,寻找一种更加方便、有效且无创的检查技术来判断肺LCNEC患者淋巴结是否转移,对临床实施个体化治疗具有重要意义。PET/CT通过反映肿瘤细胞的代谢水平来判断淋巴结转移状态,还可通过淋巴结的代谢改变来判断有无转移,而此种代谢的改变往往早于形态学的改变。Kaseda等[12]研究纳入了246例临床Ⅰ期非小细胞肺癌患者,结果表明原发肿瘤的SUVmax是预测淋巴结转移的独立影响因素。本研究结果发现,有淋巴结转移的肺LCNEC患者的原发灶SUVmax明显高于无淋巴结转移的患者,且差异有统计学意义。我们利用ROC曲线对淋巴结转移进行分析,AUC为0.858,以SUVmax=11.9作为界值点,诊断淋巴结转移的灵敏度为80.0%,特异度为77.3%,这表明原发肿瘤SUVmax可为判断淋巴结转移状态提供参考依据。
肺LCNEC主要应与肺鳞癌、肺腺癌进行鉴别。肺鳞癌18F-FDG摄取较高,二者PET显像不易鉴别,但是肺鳞癌中央型多见,肿瘤较大时常出现液化坏死,并可形成空洞,空洞壁厚薄不均匀,而肺LCNEC多为周围型,密度多较均匀,液化坏死少见。肺腺癌以周围型多见,18F-FDG摄取有时也较高,但是肺腺癌病灶边缘常可见毛刺征,且肺腺癌病灶的分叶征多为深分叶,而肺LCNEC多为浅分叶,病灶周围毛刺少见。
总之,肺LCNEC好发于中老年男性,其18F-FDG PET/CT多表现为周围型类圆形软组织结节或肿块,边缘光整伴浅分叶,充气支气管征及钙化少见,18F-FDG摄取较高,原发灶的SUVmax是判断淋巴结转移的重要半定量指标。
肺大细胞神经内分泌癌的18F-FDG PET/CT表现
18F-FDG PET/CT manifestations of pulmonary large cell neuroendocrine carcinoma
-
摘要:
目的探讨肺大细胞神经内分泌癌(LCNEC)的18F-氟脱氧葡萄糖(FDG)PET/CT的影像学表现。 方法回顾性分析2009年10月至2017年5月经病理证实的37例肺LCNEC患者的18F-FDG PET/CT影像学表现,包括病灶位置、形态特征、代谢和淋巴结转移情况,以及最大标准化摄取值(SUVmax)预测淋巴结转移的价值。SUVmax与肿瘤最大径的相关性采用Pearson相关性分析。 结果37例肺LCNEC患者均为单发,其中周围型28例(28/37,75.7%)、中央型9例(9/37,24.3%)。30例病灶(30/37,81.1%)可见分叶征,多为浅分叶;10例病灶(10/37,27.0%)可见毛刺征。29例病灶(29/37,78.4%)边界清晰,9例病灶(9/37,24.3%)可见胸膜凹陷征,2例病灶可见液化坏死,1例病灶可见空洞形成,1例病灶内见点状钙化,1例病灶内见充气支气管征。37例病灶18F-FDG代谢程度均高于肝脏,SUVmax为11.7±5.2(3.3~25.3),肿瘤最大径为(3.2±1.5)cm,SUVmax与肿瘤最大径呈正相关(r=0.569,P=0.000)。15例病灶伴有肺门和(或)纵隔淋巴结转移,8例可见远处转移,包括骨转移4例、肾上腺转移1例、肝脏及骨转移2例、肾上腺及骨转移1例。约登指数最大为0.573,所对应的SUVmax为11.9,诊断效率最高,灵敏度为80.0%,特异度为77.3%。 结论肺LCNEC的18F-FDG PET/CT多表现为周围型类圆形软组织结节或肿块,边缘清晰,充气支气管征少见,18F-FDG摄取较高。原发肿瘤SUVmax是判断淋巴结转移的重要半定量指标。 -
关键词:
- 肺肿瘤 /
- 神经内分泌癌 /
- 正电子发射断层显像计算机体层摄影术 /
- 氟脱氧葡萄糖F18
Abstract:ObjectiveTo investigate the 18F-FDG PET/CT manifestations of pulmonary large cell neuroendocrine carcinoma(LCNEC). MethodsThe 18F-FDG PET/CT manifestations of 37 lung LCNEC patients confirmed by pathology from October 2009 to May 2017 were analyzed. These manifestations include lesion location, shape characteristics, lymph node metastasis, lesion metabolism, and predictive value of primary tumor maximum standardized uptake value(SUVmax) for lymph node metastasis. Pearson's correlation was used to analyze the relation between primary tumor SUVmax and maximum tumor diameter. ResultsAll 37 patients with lung LCNEC were with single lung node, including 28 patients located peripherally(28/37, 75.7%) and 9 patients located centrally(9/37, 24.3%). Lobulation of tumors was found in 30 cases(30/37, 81.1%), and spiculation was observed in 10 cases(10/37, 27.0%). The tumors were smooth and well defined in 29 cases(29/37, 78.4%), whereas pleural indentation, necrosis, cavity, calcification, and air bronchograms were found in 9, 2, 1, 1, and 1 cases, respectively. The metabolism of 18F-FDG in 37 lesions was higher than that in the liver. The SUVmax was 11.7±5.2(3.3-25.3), and the maximum tumor diameter(3.2±1.5) cm. These two parameters showed a positive correlation(r=0.569, P=0.000). Mediastinal and/or hilar lymphadenectasis was observed in 15 cases. Distant metastasis was observed in 8 cases, including bone metastasis in 4 cases, adrenal gland metastasis in 1 cases, liver and bone metastasis in 2 cases, and adrenal gland and bone metastasis in 1 case. Primary tumor SUVmax had a predictive value for lymph node metastasis. When the cut-off value was 11.9, the Youden index was 0.573, and the diagnostic efficiency was the highest with 80% sensitivity and 77.3% specificity. ConclusionsThe 18F-FDG PET/CT manifestations of most pulmonary large cell neuroendocrine carcinoma are characterized by round soft tissue nodules or masses with clear margins, rare air bronchograms, and high 18F-FDG uptake. Primary tumor SUVmax is an important semi-quantitative indicator for predicting lymph mode metastasis. -
图 1 左肺上叶肺大细胞神经内分泌癌的PET/CT显像图
Figure 1. The PET/CT image of large cell neuroendocrine carcinoma in left upper lung: male of 73 years old
图 2 左肺上叶肺大细胞神经内分泌癌(ⅡB期)的PET/CT显像图
Figure 2. The PET/CT image of large cell neuroendocrine carcinoma in left upper lung: male of 58 years old
-
[1] Kasajima A, Ishikaw a Y, Iwata A, et al. Inflammation and PD-L1 expression in pulmonary neuroendocrine tumors[J]. Endocr Relat Cancer, 2018, 25(3):339-350. DOI:10.1530/ERC-17-0427. [2] Derks JL, Leblay N, Thunnissen E, et al. Molecular Subtypes of Pulmonary Large-cell Neuroendocrine Carcinoma Predict Chemotherapy Treatment Outcome[J]. Clin Cancer Res, 2018, 24(1):33-42. DOI:10.1158/1078-0432.CCR-17-1921. [3] Cattoni M, Vallières E, Brown LM, et al. Improvement in TNM staging of pulmonary neuroendocrine tumors requires histology and regrouping of tumor size[J]. J Thorac Cardiovasc Surg, 2018, 155(1):405-413. DOI:10.1016/j.jtcvs.2017.08.102. [4] Hoton D, Humblet Y, Libbrecht L. Phenotypic variation of an ALK-positive large-cell neuroendocrine lung carcinoma with carcinoid morphology during treatment with ALK inhibitors[J]. Histopathology, 2018, 72(4):707-710. DOI:10.1111/his.13388. [5] Akata S, Okada S, Maeda J, et al. Computed tomographic findings of large cell neuroendocrine carcinoma of the lung[J]. Clin Imaging, 2007, 31(6):379-84. DOI:10.1016/j.clinimag.2007.04.027. [6] 郭健, 叶兆祥, 冯小伟, 等.肺大细胞神经内分泌癌的MSCT表现[J].中国医学影像技术, 2013, 29(1):79-83.
Guo J, Ye ZX, Feng XW, et al. MSCT findings of lung large cell neuroendocrine carcinoma[J]. Chin J Med Imaging Technol, 2013, 29(1):79-83.[7] 金民山, 张俊, 姜一逸, 等. 18F-FDG PET/CT在不明原发灶肿瘤中的临床应用价值[J].国际放射医学核医学杂志, 2017, 41(2):94-97. DOI:10.3760/cma.j.issn.1673-4114.2017.02.003.
Jin MS, Zhang J, Jiang YY, et al. Clinical value of 18F-FDG PET/CT in cancer of unknown primary[J]. Int J Radiat Med Nucl Med, 2017, 41(2):94-97. DOI:10.3760/cma.j.issn.1673-4114. 2017.02. 003.[8] Lee KW, Lee Y, Oh SW, et al. Large cell neuroendocrine carcinoma of the lung:CT and FDG PET findings[J]. Eur J Radiol, 2015, 84(11):2332-2338. DOI:10.1016/j.ejrad.2015.07.033. [9] Kaira K, Murakami H, Endo M, et al. Biological correlation of 18F-FDG uptake on PET in pulmonary neuroendocrine tumors[J]. Anticancer Res, 2013, 33(10):4219-4228. [10] 严振辉, 柳学国, 何亚奇, 等.肺大细胞神经内分泌癌的临床影像学特点与诊断(附22例分析)[J].现代医用影像学, 2015, 24(3):375-379.
Yan ZH, Liu XG, He YQ, et al. Clinical imaging and characteristics diagnosis of pulmonary large cell neuroendocrine carcinoma (Analysis of 22 cases)[J]. Mod Med Imagel, 2015, 24(3):375-379.[11] 钱哲, 胡瑛, 郑华, 等.肺大细胞神经内分泌癌22例临床分析[J].中国肺癌杂志, 2016, 19(2):82-87. DOI:10.3779/j.issn.1009-3419.2016.02.05.
Qian Z, Hu Y, Zheng H, et al. Clinical analysis of 22 cases of pulmonary large cell neuroendocrine cancer[J]. Chin J Lung Cancer, 2016, 19(2):82-87. DOI:10.3779/j.issn.1009-3419. 2016. 02.05.[12] Kaseda K, Asakura K, Kazama A, et al. Risk Factors for Predicting Occult Lymph Node Metastasis in Patients with Clinical Stage Ⅰ Non-small Cell Lung Cancer Staged by Integrated Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography[J]. World J Surg, 2016, 40(12):2976-2983. DOI:10.1007/s00268-016-3652-5. -

 点击查看大图
点击查看大图
图(3)
计量
- 文章访问数: 3688
- HTML全文浏览量: 3016
- PDF下载量: 11