


 下载:
下载:

-
滑膜炎、痤疮、脓疱病、骨肥厚、骨髓炎(synovitis,acne,pustulosis,hyperostosis,osteom-yelitis,SAPHO)综合征是一种少见疾病,由Chamot等[1]于1987年首次提出,该病以骨、关节病变和皮肤损害为特点。国内对该病的报道较少,以SPECT/CT骨显像研究报道的则更少。笔者回顾性分析了9例SAPHO综合征患者的SPECT/CT骨显像图像,旨在探讨SPECT/CT骨显像在SAPHO综合征诊断中的临床价值,以期提高对SAPHO综合征的认识。
-
2013年10月至2017年6月在我院诊治并怀疑SAPHO综合征的患者11例,其中男性2例、女性9例,年龄47~65岁,平均年龄(54.3±8.2)岁。病例纳入及排除标准:单发或多发骨骼病变,排除临床诊断明确的骨转移瘤、骨折和骨髓炎患者。入选患者均进行常规检验血沉、C反应蛋白及人类白细胞抗原B27抗体,且均接受99Tcm-MDP全身骨显像+局部断层显像及同机或异机CT扫描,获得SPECT全身骨显像和局部SPECT骨显像、CT显像、SPECT/CT融合显像图像。所有患者或家属均于检查前签署了知情同意书。
-
SAPHO综合征的诊断标准[2-4]如下:①无菌性滑膜炎、骨肥厚或骨髓炎伴有严重型痤疮或特征性手足脓疱疮;②无菌性滑膜炎、骨肥厚或骨髓炎累及中轴骨或四肢骨,特别是累及前上胸壁胸肋锁骨区、椎体和骶髂关节或儿童多个长骨的干骺端;③慢性复发性多灶性骨髓炎。符合②或③诊断标准的患者可以伴有或不伴有皮肤损害。
-
静脉注射99Tcm-MDP(江苏省原子医学研究所提供)740~925 MBq,嘱患者多饮水,3 h后排空膀胱,行常规全身骨平面显像,显像仪器为美国GE公司Infinia VC型SPECT仪,配低能高分辨型准直器,全身骨显像扫描参数为:能峰140 keV,矩阵1024×256,窗宽20%,放大倍数1,采用自动人体轮廓轨迹采集,扫描速度20~25 cm/min。根据全身骨显像结果选择阳性病灶进行局部断层显像+同机或异机CT扫描。局部断层显像参数为:矩阵64×64,放大倍数1,采集360°,双探头各旋转180°,步进6°,每帧30 s。早期6例采用异机诊断级CT(美国GE公司Discovery CT 750 HD宝石能谱CT)扫描,CT扫描参数为:层厚5.0 mm,层距5.0 mm,扫描完成后重建1.25 mm,螺距0.984,管电压140 kV,管电流250 mA;后期5例均采用同机定位CT扫描(SPECT仪器升级为美国GE公司Infinia VC Hawkeye 4型SPECT/CT),CT扫描参数为:层厚5.0 mm,层距5.0 mm,螺距1.9,管电压140 kV,管电流2.5 mA。采集结束后在Infinia VC Hawkeye 4型SPECT/CT仪后处理工作站分别重建全身骨平面SPECT及局部阳性病灶同机或异机SPECT/CT断层骨融合图像。
-
由2位核医学科副主任医师和1名影像科副主任医师共同阅片,4种图像的印象诊断与最后诊断符合者,判定为“符合”,病变性质待定或印象诊断与最后诊断不一致者,判定为“不符合”。骨显像判断标准为:正常骨骼显影清晰,头颅、脊柱、骨盆放射性分布均匀,双侧肢体、肋骨放射性分布对称、均匀;骨骼出现放射性异常浓聚灶或稀疏、缺损区,判定为阳性。CT判断标准为:正常骨骼结构纹理清晰,骨性关节面光滑、平整;骨骼受累包括骨质破坏、增生硬化、骨质肥厚,关节面侵蚀破坏、硬化、间隙变窄等,判定为阳性。
-
应用SPSS 17.0软件进行统计学分析。组间准确率的比较采用χ2检验,P < 0.05表示差异有统计学意义。
-
本组11例临床怀疑SAPHO综合征患者中,4例经骨病变部位穿刺活检确诊,病理诊断为慢性非特异性炎症、终板炎等,5例至少经2年以上随访病情最终转归而确诊,2例经手术及组织病理检查证实为骨转移瘤(分别为肺癌和乳腺癌)。确诊的9例患者的临床病程为半年至十几年;8例合并有皮肤损害,其中手、足同时合并脓疱疮者6例,手掌、脚掌单发脓疱疮者各1例;3例患者血沉、C反应蛋白轻度升高,1例人类白细胞抗原B27抗体阳性。
-
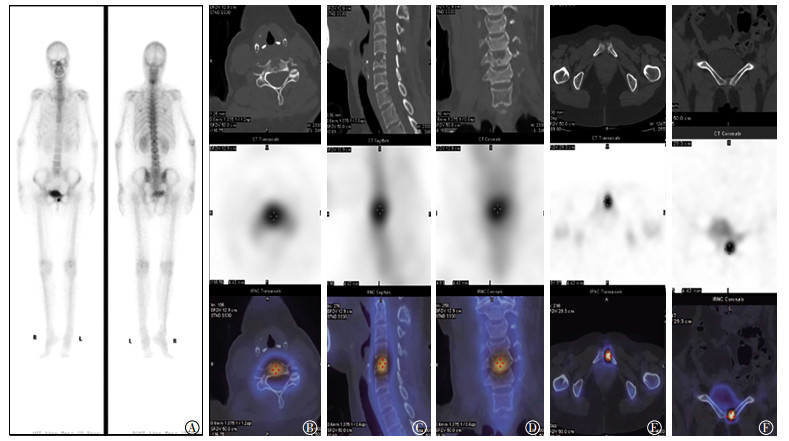
确诊SAPHO综合征的9例患者骨显像结果均有异常,表现为1个至多个部位骨异常放射性浓聚区。SPECT全身骨显像确诊6例,发现41个病灶出现放射性浓聚(胸锁关节8个、胸肋关节10个、胸骨柄体联合关节2个、剑突2个、颈椎5个、胸椎6个、腰椎6个、骶髂关节1个、耻骨联合1个),诊断准确率、灵敏度和特异度分别为63.6%(7/11)、66.7%(6/9)和50.0%(1/2);SPECT/CT骨显像确诊9例,共发现44个病灶(胸锁关节9个、胸肋关节10个、胸骨柄体联合关节2个、剑突2个、颈椎5个、胸椎7个、腰椎7个、骶髂关节1个、耻骨联合1个),诊断准确率、灵敏度和特异度分别为90.9%(10/11)、100%(9/9)和50.0%(1/2)。SPECT/CT骨显像对SAPHO综合征的诊断准确率明显高于单纯的SPECT(90.9% vs. 63.6%),差异具有统计学意义(χ2=11.82,P < 0.05)。9例确诊SAPHO的患者中,8例患者前上胸壁胸肋锁骨区受累,双侧对称性受累4例,不对称性受累4例,SPECT骨显像发现22处病灶(胸锁关节8个、胸肋关节10个、胸骨柄体联合2个、剑突2个),SPECT/CT发现23处病灶(胸锁关节9个、胸肋关节10个、胸骨柄体联合关节2个、剑突2个),SPECT骨显像表现为放射性分布异常浓聚,典型者呈“牛头征”,放射性浓聚区呈牛角状外形(图 1、2);4例脊柱受累,SPECT骨显像发现17处病灶(颈椎5个、胸椎6个、腰椎6个),SPECT/CT发现19处病灶(颈椎5个、胸椎7个、腰椎7个),SPECT骨显像表现为灶状或条带状放射性浓聚(图 2、3);另外,1例骶髂关节受累,为单侧非对称性受累,1例耻骨联合受累,CT表现为受累骨、软骨膨胀,骨质肥厚、硬化,骨性关节面和椎体终板虫噬状骨质破坏,伴随骨质增生、硬化,关节间隙变窄,甚至消失,关节周围软组织肿胀,肌腱附着点钙化等。

图 1 SAPHO综合征患者SPECT/CT图像
Figure 1. SPECT/CT images of patient with SAPHO syndrome

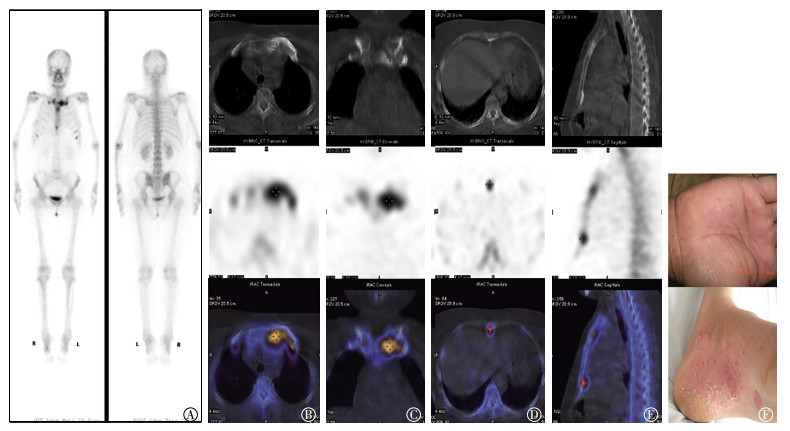
图 2 SAPHO综合征患者SPECT/CT图像
Figure 2. SPECT/CT images of patient with SAPHO syndrome

图 3 SAPHO综合征患者SPECT/CT图像
Figure 3. SPECT/CT images of patient with SAPHO syndrome
本组病例中,发现早期隐匿性病灶5处(胸肋锁骨区1处、颈椎1处、胸椎2处、腰椎1处),骨显像有异常放射性浓聚,而临床无相关症状及体征,CT也未见明显异常;发现代谢活性减低病灶1处(胸肋锁骨区),CT见明显骨质增生、肥厚、硬化,但骨显像未见明显异常。
-
1987年,Chamot等[1]首先描述了滑膜炎、痤疮、脓疱疮、骨肥厚、骨髓炎综合征,并取这5种病变的英文名称的首字母组合在一起,命名为SAPHO综合征。此前用来描述该病的名称多达50多个,如胸肋锁骨肥厚症、慢性复发性多发骨髓炎、关节骨炎合并手足脓疱疮、获得性骨肥大综合征等[5]。该病病因不明,可能与细菌或病毒感染启动的自身免疫反应有关,有学者认为这是一种血清阴性脊椎关节病,也有学者认为是牛皮癣性关节炎的一个亚型[6-7],还有学者报道已从SAPHO综合征患者体内分离出痤疮丙酸杆菌,并认为痤疮丙酸杆菌持续性轻度感染能够触发机体自身非特异性的T细胞免疫反应异常激活[8],从而造成非特异性的炎性损伤等。
SAPHO综合征好发于30~50岁中青年人,男女发病率均等,呈慢性病程,临床上以间断复发和缓解为特点,病程呈迁延性和自限性,但大多数预后良好。该病的特征为皮肤和骨关节的慢性无菌性炎症反应,但二者不一定同时发生[9]。皮肤病变具有诊断提示性和特征性,但并不是SAPHO综合征诊断的必要条件,其皮肤损害主要为手足掌的对称性脓疱疮和(或)面部和胸前痤疮、银屑病等,发病率约为60%[10],可与骨关节病变同时出现,或发生于骨关节病变之前或之后数年。本组患者中,合并皮肤损害8例(88.9%,8/9),其中大部分为手足脓疱疮(7例),银屑病仅1例,与文献报道相差较大[10],可能与患者例数较少有关。SAPHO综合征患者的实验室检查结果中血沉、白细胞、C反应蛋白等可轻、中度升高,类风湿因子阴性,部分患者人类白细胞抗原B27抗体可呈阳性。本组患者中,3例血沉、C反应蛋白轻度升高,1例人类白细胞抗原B27抗体阳性。SAPHO综合征患者的骨关节病变表现为受累骨关节处肿痛,基本病变为无菌性骨髓炎和关节炎,病理检查结果为骨病变处慢性非特异性炎症。本组患者中,4例进行了骨病变部位穿刺活检,病理结果诊断为慢性非特异性炎症、终板炎等,与文献报道相符[11]。
骨、关节受累是SAPHO综合征的重要特征。成人最常累及前上胸壁胸肋锁骨区(65%~90%),其次为脊柱(32%~52%)与骶髂关节(20%~52%),外周扁骨、长骨也可累及,儿童最易累及下肢长骨干骺端[12]。骨、关节受累主要包括滑膜炎、骨髓炎、骨肥厚及肌腱附着点关节病,可累及中轴骨和外周骨,可以单发或多发,可同时或先后发生。早期以骨侵蚀为主,后期以骨质增生硬化、骨肥厚为主,但两种病变常同时存在,骨质侵蚀多发生于骨性关节面或椎体终板,CT表现为关节面下骨质和椎体终板虫蚀状或小孔洞状骨质侵蚀,破坏灶边缘毛糙。骨质增生、骨肥厚是慢性炎症反应分别累及髓腔和骨皮质的表现,骨髓炎通常表现为骨质增生硬化,而骨肥厚则是慢性骨膜反应所致,这些病理过程在CT上表现为骨髓腔均匀或不均匀硬化、骨皮质增厚等,具有高度特征性,是引起疼痛的主要原因,而在骨显像中则表现为局部骨盐代谢活跃(放射性浓聚)[13]。
SPECT骨显像灵敏度高,易于早期发现骨骼的异常代谢活动及没有症状的隐匿性病灶(无临床症状和放射学检查阴性),CT可以显示骨骼精细解剖结构,SPECT/CT联合应用提高了对病灶解剖定位的准确率及骨显像特异度,可以精准定位、辅助定性及评价病灶代谢活性。SAPHO综合征典型的骨显像表现为胸肋锁骨区“牛头”状的放射性核素浓聚,胸骨柄形如牛的头颅,炎症性的胸锁关节及相邻肋骨形如牛角,具有高度特征性[14],也有呈“T”形或“领结”样高浓聚,其放射性浓聚的高低也间接反映了病灶活性的强弱。本组确诊的9例SAPHO综合征患者中,前上胸壁受累8例(88.9%,8/9),经SPECT骨显像发现22处病灶,SPECT/CT发现23处,双侧对称性受累4例,表现为典型的“牛头征”;发现早期隐匿性病灶1处(胸肋锁骨区),骨显像有异常放射性浓聚,而临床无相关症状及体征,CT也未见明显异常;另发现CT异常而骨盐代谢正常1处(胸肋锁骨区),CT见明显骨质增生、肥厚、硬化,但骨显像未见明显异常,原因可能与病灶较陈旧,近期无活动有关,提示骨病变的代谢活性。SAPHO综合征患者脊柱亦常受累,以胸椎最多,其次是腰椎、颈椎。椎体受累一般为多发连续或非连续性,骨显像表现为灶状或条带状放射性浓聚,SPECT/CT表现为受累椎体终板侵蚀、硬化,椎间隙变窄,椎旁骨化,椎体楔形变,尤其是椎体边角侵蚀,Laredo等[15]认为这是诊断该病的重要征象。本组患者中,脊柱受累4例(44.4%,4/9),共涉及19个椎体,骶髂关节、耻骨联合受累各1例;发现早期隐匿性病灶4处(颈椎1处、胸椎2处、腰椎1处)。郝新忠等[16]认为骨性关节面侵蚀破坏的程度与其周围骨质硬化“不匹配”性改变是诊断该病的另一重要征象,即骨侵蚀相对较小,而其周围骨硬化范围相对较大。在本组患者中,椎体终板侵蚀及周围骨质硬化表现与此征象相符。
SPECT/CT骨显像在SAPHO综合征诊断中的应用国内报道较少。本研究中经SPECT骨显像诊断SAPHO综合征的准确率、灵敏度和特异度分别为63.6%、66.7%和50.0%;SPECT/CT分别为90.9%、100%和50.0%。SPECT/CT融合了SPECT及CT的优势,解决了SPECT显像定位、定性不准确的难题,其诊断SAPHO综合征的准确率明显高于单纯SPECT,两者间的差异具有统计学意义,SPECT/CT可用于SAPHO综合征患者病灶的精准定位、辅助定性以及病灶代谢活性评价。但需要注意的是,Infinia VC Hawkeye 4型SPECT/CT仪配置的是低分辨率CT,其CT图像的分辨率远低于影像科诊断级CT,对于小病灶或复杂病变的图像显示模糊,定性诊断较困难,应用尚存在局限性。随着PET/CT装机数量的逐渐增加,其在SAPHO综合征中的应用国内外均有报道[17-18]。国内郝新忠等[16]报道了5例SAPHO综合征的PET/CT显像和临床分析结果,陆国秀等[19]报道了25例PET/CT联合骨显像对SAPHO综合征的诊断价值。骨显像的灵敏度高,易于发现PET/CT检查阴性的病灶,PET/CT有助于半定量分析炎症反应的程度,对病灶分期具有重要意义。
SAPHO综合征可以累及全身多部位骨骼,因此首先需与骨转移瘤相鉴别。骨转移瘤较少累及前上胸壁胸肋锁骨区,而SAPHO综合征的累及率较高,且因其发生于胸肋锁骨区典型的部位、具有典型的“牛头征”SPECT/CT表现并伴随皮肤损害,其诊断不难。需要特别注意的是临床上若不伴有皮肤损害,缺乏典型的“牛头征”,累及其他非典型部位者时,诊断需谨慎,应密切结合临床资料。其他需要与SAPHO综合征鉴别诊断的疾病包括慢性低毒力感染、银屑病关节炎、强直性脊柱炎、类风湿性关节炎等。
SAPHO综合征患者临床较少见,影像和核医学医师对该病尚缺乏足够的认识。SPECT/CT同时融合了SPECT及CT的优势,可以早期明确诊断,排除恶性肿瘤,对病灶的精准定位、更多隐匿病灶的发现以及病灶代谢活性的评价具有重要意义。
SPECT/CT骨显像对SAPHO综合征的诊断价值
Value of SPECT/CT bone imaging in the diagnosis of SAPHO syndrome
-
摘要:
目的探讨SPECT/CT骨显像在滑膜炎、痤疮、脓疱病、骨肥厚、骨髓炎(SAPHO)综合征诊断中的临床价值。 方法回顾性分析临床怀疑SAPHO综合征的11例患者的临床资料及SPECT/CT骨显像结果,所有患者均行99Tcm-MDP全身骨显像+局部断层显像及同机或异机CT扫描,获得SPECT全身骨显像和局部SPECT骨显像、CT显像、SPECT/CT融合显像图像。分析比较SPECT骨显像和SPECT/CT融合显像对SAPHO综合征诊断的准确率、灵敏度和特异度,组间准确率的比较采用χ2检验。 结果11例临床怀疑SAPHO综合征患者中,9例经穿刺组织病理或随访病情最终转归而确诊,另外2例为转移瘤。其中,SPECT诊断6例,共发现41个病灶出现放射性浓聚;SPECT/CT诊断9例,共发现44个病灶。SPECT骨显像的灵敏度、特异度和准确率分别为66.7%(6/9)、50.0%(1/2)和63.6%(7/11);SPECT/CT融合显像的灵敏度、特异度和准确率分别为100%(9/9)、50.0%(1/2)和90.9%(10/11),SPECT/CT融合显像对SAPHO综合症诊断的准确率明显高于单纯的SPECT显像,且差异具有统计学意义(χ2=11.82,P < 0.05)。 结论SPECT/CT的联合应用提高了对病灶解剖定位的准确率及骨显像特异度,可用于SAPHO综合征患者的病灶精准定位、早期诊断与鉴别诊断、更多隐匿病灶检出以及病灶代谢活性评价等,对SAPHO综合征的诊断有较高的临床价值。 -
关键词:
- 获得性骨肥大综合征 /
- 体层摄影术,发射型计算机,单光子 /
- 体层摄影术,X线计算机 /
- 骨显像
Abstract:ObjectivesTo discuss the clinical value of SPECT/CT bone imaging in the diagnosis of synovitis, acne, pustulosis, hyperostosis, and osteomyelitis (SAPHO) syndrome. MethodsThe clinical data and SPECT and SPECT/CT imaging results of 11 patients with suspected SAPHO syndrome were retrospectively analyzed. All patients underwent 99Tcm-MDP full-body bone imaging, local fault imaging, and CT scanning with the same or different machines. The accuracy, sensitivity, and specificity of the diagnosis of SAPHO syndrome through SPECT and SPECT/CT imaging were analyzed and compared. Data were analyzed through χ2 test. ResultsAmong 11 patients with suspected SAPHO syndrome, 9 underwent puncture pathology or follow-up for the definite diagnosis of their conditions. Two patients were diagnosed with metastatic tumors. In 6 patients with SPECT, 41 lesions exhibited radioactive concentration. Furthermore, 44 lesions were observed in 9 patients who were diagnosed through SPECT/CT. The sensitivity, specificity, and accuracy of SPECT and SPECT/CT imaging were 66.7%(6/9) and 100%(9/9), 50.0%(1/2) and 50.0%(1/2), 63.6%(7/11) and 90.9%(10/11), respectively. The diagnostic accuracy of SPECT/CT imaging for SAPHO syndrome was higher than that for pure SPECT. Moreover, the diagnostic accuracies of the two methods were significantly different(χ2=11.82, P < 0.05). ConclusionsThe combined application of SPECT/CT may improve the accuracy of identifying the anatomical orientations of lesions and the specificity of bone imaging. This method can be used for the precise localization of lesions, the identification and diagnosis of SAPHO in its early stages, the implicit detection of lesions, and the characterization of lesion metabolic activity. Therefore, the combined application of SPECT/CT diagnosis has high clinical value in the diagnosis of SAPHO syndrome. -
[1] Chamot AM, Benhamou CL, Kahn MF, et al. Acne-pustulosis-hyperostosis-osteitis syndrome. Results of a national survey. 85 cases[J]. Rev Rhum Mal Osteoartic, 1987, 54(3):187-196. [2] Pahlavan PS, Leslie WD. Multiple imaging findings in SAPHO syndrome[J]. Clin Nucl Med, 2008, 33(12):912-915. DOI:10.1097/RLU.0b013e31818c4eb1. [3] Hurtado-Nedelec M, Chollet-Martin S, Nicaise-Roland P, et al. Characterization of the immune response in the synovitis, acne, pustulosis, hyperostosis, osteitis (SAPHO) syndrome[J]. Rheumatology (Oxford), 2008, 47(8):1160-1167. DOI:10.1093/rheumatology/ken185. [4] Govoni M, Colina M, Massara A, et al. "SAPHO syndrome and infections"[J]. Autoimmun Rev, 2009, 8(3):256-259. DOI:10.1016/j.autrev.2008.07.030. [5] 孙洋, 孟悛非. SAPHO综合征的影像学表现[J].国外医学临床放射学分册, 2005, 28(2):93-95. DOI:10.3784/j.issn.1674-1897. 2005.02.007.
Sun Y, Meng QF. Imaging features of SAPHO syndrome[J]. Foreign Med Sci Clin Radiol Fascicle, 2005, 28(2):93-95. doi: 10.3784/j.issn.1674-1897.2005.02.007[6] Magrey M, Khan MA. New insights into synovitis, acne, pustulosis, hyperostosis, and osteitis (SAPHO) syndrome[J]. Curr Rheumatol Rep, 2009, 11(5):329-333. DOI:10.1007/s11926-009-0047-8. [7] Boutin RD, Resnick D. The SAPHO syndrome:an evolving concept for unifying several idiopathic disorders of bone and skin[J]. AJR Am J Roentgenol, 1998, 170(3):585-591. DOI:10.2214/ajr.170.3. 9490935. [8] Colina M, Lo Monaco A, Khodeir M, et al. Propionibacterium acnes and SAPHO syndrome:a case report and literature review[J]. Clin Exp Rheumatol, 2007, 25(3):457-460. [9] 王颖, 李亚明, 尹雅芙, 等. SAPHO综合征SPECT/CT显像1例报道并文献复习[J].中国临床医学影像杂志, 2013, 24(4):303-304. DOI:10.3969/j.issn.1008-1062.2013.04.027.
Wang Y, Li YM, Yin YF, et al. The diagnostic value of SPECT/CT for SAPHO syndrome:report of one case and review of literature[J].J Chin Clin Med Imaging, 2013, 24(4):303-304. doi: 10.3969/j.issn.1008-1062.2013.04.027[10] 刘记存, 陈勇, 崔建岭. SAPHO综合征的影像表现[J].中国医学影像技术, 2011, 27(8):1684-1687. DOI:10.13929/j.1003-3289. 2011.08.026.
Liu JC, Chen Y, Cui JL. Imaging features of SAPHO syndrome[J]. Chin J Med Imaging Technol, 2011, 27(8):1684-1687. doi: 10.13929/j.1003-3289.2011.08.026[11] Sallés M, Olivé A, Perez-Andres R, et al. The SAPHO syndrome:a clinical and imaging study[J]. Clin Rheumatol, 2011, 30(2):245-249. DOI:10.1007/s10067-010-1560-x. [12] Earwaker JW, Cotten A. SAPHO:syndrome or concept? Imaging findings[J]. Skeletal Radiol, 2003, 32(6):311-327. DOI:10.1007/s00256-003-0629-x. [13] Pichler R, Weiglein K, Schmekal B, et al. Bone scintigraphy using Tc-99m DPD and F18-FDG in a patient with SAPHO syndrome[J]. Scand J Rheumatol, 2003, 32(1):58-60. DOI:10.1080/030097403-10000436. [14] Freyschmidt J, Sternberg A. The bullhead sign:scintigraphic pattern of sternocostoclavicular hyperostosis and pustulotic arthroosteitis[J]. Eur Radiol, 1998, 8(5):807-812. DOI:10.1007/s003300050476. [15] Laredo JD, Vuillemin-Bodaghi V, Boutry N, et al. SAPHO syndrome:MR appearance of vertebral involvement[J]. Radiology, 2007, 242(3):825-831. DOI:10.1148/radiol.2423051222. [16] 郝新忠, 武志芳, 武萍, 等. SAPHO综合征18F-FDG PET/CT显像和临床分析[J].国际放射医学核医学杂志, 2015, 39(6):447-451, 457. DOI:10.3760/cma.j.issn.1673-4114.2015.06.003.
Hao XZ, Wu ZF, Wu P, et al. 18F-FDG PET/CT imaging and clinical features of SAPHO syndrome[J]. Int J Radiat Med Nucl Med, 2015, 39(6):447-451, 457. doi: 10.3760/cma.j.issn.1673-4114.2015.06.003[17] Patel CN, Smith JT, Rankine JJ, et al. F-18 FDG PET/CT can help differentiate SAPHO syndrome from suspected metastatic bone disease[J]. Clin Nucl Med, 2009, 34(4):254-257. DOI:10.1097/RLU. 0b013e31819a205c. [18] Abuhid IM, Silva LC, Martins GP, et al. Diagnosing SAPHO syndrome in suspected metastatic bone tumors[J]. Clin Nucl Med, 2010, 35(3):172-174. DOI:10.1097/RLU.0b013e3181cc6313. [19] 陆国秀, 郝珊瑚, 王志国, 等. PET-CT联合骨显像对SAPHO综合征的诊断价值[J].临床皮肤科杂志, 2014, 43(9):536-539. DOI:10.16761/j.cnki.1000-4963.2014.09.001.
Lu GX, Hao SH, Wang ZG, et al. The diagnostic value of PET-CT combined with bone imaging in SAPHO syndrome[J]. J Clin Dermatol, 2014, 43(9):536-539. doi: 10.16761/j.cnki.1000-4963.2014.09.001 -

 点击查看大图
点击查看大图
图(3)
计量
- 文章访问数: 3583
- HTML全文浏览量: 2474
- PDF下载量: 9