


-
肝细胞肝癌(hepatocellular carcinoma,HCC)是常见的恶性肿瘤之一,病死率较高。18F-FDG PET/CT显像常用于恶性肿瘤的诊断、临床分期及预后评估,但其诊断原发HCC的灵敏度不高,假阴性率可达40%~50%[1]。18F-FDG与11C-乙酸盐PET/CT显像具有一定程度的互补性,常用于HCC的诊断[2]、临床分期[3-4]及肝脏肿瘤的鉴别诊断[5-6]。先前关于18F-FDG及11C-乙酸盐双示踪剂在HCC患者中的应用研究中包含了低、中、高分化的HCC 3种不同分化类型,并未对特定的病理类型选择不同示踪剂进行显像[2, 7-8]。笔者仅对中、高分化HCC患者进行双示踪剂显像,初步探讨11C-乙酸盐单示踪剂PET/CT显像能否取代双示踪剂显像用于监测中、高分化HCC患者的复发与转移。
-
回顾性分析从2015年1月至2016年12月于我院行11C-乙酸盐和18F-FDG PET/CT躯干显像的10例中、高分化HCC患者。入选患者均为男性,年龄27~74岁,平均年龄(55.5±13.7)岁。所有患者均为手术或介入治疗后6~20个月的HCC患者,其中6例为中分化HCC,4例为高分化HCC。纳入标准:中、高分化HCC患者在病情监测过程中发现甲胎蛋白水平升高,临床怀疑复发或转移。排除标准:低分化HCC患者。入选患者一周内行18F-FDG和11C-乙酸盐PET/CT检查。所有患者最终通过病理或我院影像学检查确诊转移或复发。所有患者或家属对本研究均知情并签署了知情同意书。
-
18F-FDG和11C-乙酸盐均为我科合成,放化纯度大于95%,按中国药典标准规定行24 h细菌培养及凝胶法细菌内毒素检测(次日检测),结果均为阴性。患者空腹4~6 h,在安静环境中休息10~15 min,经静脉注射2.96~4.44 MBq/kg 18F-FDG后安静休息45~60 min,使用德国西门子Biograph 64型PET/CT行5床位躯干采集。CT的管电流为100 mAs,管电压为120 kV,旋转时间为0.5 s,螺距为0.9,层厚为5 mm。CT图像用于随后PET衰减校正。PET采用三维发射采集,2 min/床位。PET重建采用点扩散技术的迭代法(TureX),使用3次迭代和21个子集,图像矩阵为172 mm×172 mm,4 mm半高宽的高斯滤波,加散射校正。18F-FDG检查后1周内行11C-乙酸盐PET/CT检查。患者空腹4~6 h,经静脉注射2.96~4.44 MBq/kg 11C-乙酸盐,5 min后使用上述相同设备和方法行躯干采集。
-
由2位高级职称核医学医师在不知患者病理分级的情况下对PET/CT图像进行分析并测定病灶及本底SUVmax。SUVmax取2位医师所得数值的平均值。PET图像上代谢高于正常肝脏组织的病灶判定为阳性,低于或类似于正常肝脏组织的病灶判定为阴性。如2位医师意见不一致则通过共同讨论判定病灶阳性或阴性。PET显像未见放射性异常浓聚者,根据同机CT或其他影像学资料确定病灶位置,用视觉融合的方法在相对应部位勾画与病灶相同大小的ROI。
-
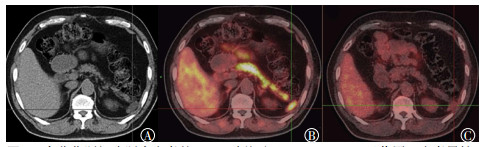
10例中、高分化HCC患者的临床资料及11C-乙酸盐、18F-FDG显像结果见表 1。11C-乙酸盐显像发现18个阳性病灶,灵敏度为100%(18/18);18F-FDG显像发现5个阳性病灶,灵敏度为27.8%(5/18);两种示踪剂同时发现5个阳性病灶(在4例中分化HCC患者中),11C-乙酸盐显像探测病灶的灵敏度与双示踪剂联合显像相同。18F-FDG显像发现2例中分化(图 1)和4例高分化HCC(图 2)病灶显像为阴性。11C-乙酸盐显像病灶的SUVmax为1.3~14.2,靶/本底比值(the ratio of target to background,T/B)为1.1~14.3;18F-FDG显像病灶的SUVmax为0.5~3.4,T/B为0.6~1.1。8例患者(13个病灶)病理证实为肿瘤复发或转移,2例患者(5个病灶)3个月后我院复查PET/CT或CT证实为转移。
序号 年龄 肝炎病史 AFP/
(μg/L)病理类型 病灶数目 病变位置 病变大小/
(cm×cm)11C-乙酸盐 18F-FDG SUVmax T/B 阳性(+)/
阴性(-)SUVmax T/B 阳性(+)/
阴性(-)1 46 + 263.56 中分化 2 肝内 2.7×2.0 4.0 1.2 + 3.4 1.1 + 肝内 4.3×2.4 4.4 1.3 + 3.4 1.1 + 2 51 + 102.82 中分化 2 肝内 1.3×0.9 5.7 1.8 + 2.4 0.9 - 肝内 2.7×2.0 5.1 1.6 + 2.8 1.1 + 3 69 + 97.1 高分化 1 肝内 1.0×0.8 3.9 1.1 + 1.8 0.6 - 4 56 + 223.62 中分化 1 肝内 9.0×6.8 6.0 1.4 + 2.5 0.9 - 5 74 + 69.81 高分化 1 肝内 9.8×7.7 14.2 3.2 + 3.3 0.9 - 6 53 + > 24 200 中分化 2 肝内 2.9×2.2 4.2 1.5 + 3.1 0.8 - 肝内 1.6×1.2 6.2 2.2 + 3.2 1.1 + 7 49 + 476.09 中分化 1 肝内 2.1×1.6 4.5 1.6 + 2.7 0.9 - 8 67 + 81.62 高分化 2 肝内 3.1×2.5 6.7 1.7 + 2.9 1 - 肝内 2.1×1.9 5.8 1.5 + 3 0.9 - 9 27 + 611.42 中分化 2 肝内 2.4×1.4 7.1 1.8 + 2.8 1 - 肝内 2.2×1.4 6.5 1.7 + 3 1.1 + 10 63 + 371.5 高分化 4 肝内 1.6×1.1 3.9 1.6 + 3 1 - 脾门区 3.0×1.6 4.3 14.3 + 0.6 1 - 腹膜后 1.5×1.3 5.5 9.2 + 0.5 0.8 - 小网膜 0.9×0.7 1.3 3.3 + 0.6 1 - 注:表中,“+”为阳性,为阴性;FDG:氟脱氧葡萄糖;PET/CT:正电子发射断层显像计算机体层摄影术;AFP:甲胎蛋白; SUVmax:最大标准化摄取值;T/B:靶/本底比值 表 1 10例男性中、高分化肝细胞肝癌患者的临床资料及11C-乙酸盐、18F-FDG PET/CT显像结果
Table 1. Clinical data and 11C-acetate and 18F-FDG PET/CT results of 10 male cases of moderately and highly differentiated hepatocellular carcinoma

图 1 中分化肝细胞肝癌患者的11C-乙酸盐及18F-FDG PET/CT显像图
Figure 1. 11C-acetate and 18F-FDG PET/CT imaging in patient with moderately differentiated hepatocellular carcinoma

图 2 高分化肝细胞肝癌患者的11C-乙酸盐及18F-FDG PET/CT显像图
Figure 2. 11C-acetate and 18F-FDG PET/CT imaging in patient with highly differentiated hepatocellular carcinoma
-
HCC在我国是常见的恶性肿瘤之一。及时且准确地判断HCC治疗后的残存、复发或转移情况直接关系到临床治疗方案的选择及患者预后。18F-FDG PET/CT显像在大多数恶性肿瘤的疗效监测及评估中发挥着越来越大的作用,但对HCC原发灶的诊断效果不佳,尤其是在高分化HCC患者中。18F-FDG PET/CT显像中18F-FDG在细胞内的浓聚程度取决于细胞内磷酸激酶活性和葡萄糖-6-磷酸酶活性之比,分化较好的肿瘤细胞内含有较高浓度的葡萄糖-6-磷酸酶,去磷酸化水平高,可以加速18F-FDG的细胞转出过程[9],因此,高分化HCC病灶细胞内18F-FDG的含量较低,常表现为假阴性。在对HCC转移灶的18F-FDG PET/CT显像研究中,Park等[4]发现18F-FDG比11C-乙酸盐更具优势;而Ho等[7]的研究结果表明对HCC转移灶应用11C-乙酸盐单示踪剂显像似乎有一定的优势。本研究结果与Ho等[7]的研究结果大致相同,在高分化HCC中,11C-乙酸盐显像发现8个病灶,而18F-FDG显像均为假阴性;在中分化HCC中,18F-FDG显像的阳性率也仅为50%,因此,对中、高分化HCC转移及复发病灶应用11C-乙酸盐与18F-FDG双示踪剂显像并没有明显的优势。
11C-乙酸盐作为氨基酸及甾醇合成的前体,可以从另一方面反映肿瘤代谢情况不受葡萄糖去磷酸化的影响,是一种很有潜力的正电子显像剂,已广泛应用于多种高分化、低度恶性的肿瘤显像中,可弥补18F-FDG显像的不足。乙酸盐参与细胞脂代谢,恶性肿瘤细胞脂类代谢比正常细胞活跃,11C-乙酸盐进入体内后较多地进入癌细胞中,其进入量与反映肿瘤增殖程度的脂肪及磷脂膜合成量呈正相关[10-11]。此外,11C-乙酸盐显像还可用于前列腺癌[12]及肾脏肿瘤[13]的诊断及分期。本研究中11C-乙酸盐PET/CT显像10例患者均为阳性,且总共发现18个病灶,对中、高分化HCC的复发与转移的探测灵敏度明显高于18F-FDG PET/CT显像,与双示踪剂联合显像灵敏度相同。
本研究仅针对治疗后高度怀疑复发与转移的中、高分化HCC患者进行双示踪剂显像,并未纳入低分化HCC患者。研究结果表明11C-乙酸盐显像可显著提高中、高分化HCC的复发与转移诊断的灵敏度,且推荐使用11C-乙酸盐显像用于监测中、高分化HCC的复发与转移。本研究的不足之处在于病例数相对较少,笔者所在课题组的下一步工作将继续对现有结论作进一步验证。
11C-乙酸盐PET/CT显像在中、高分化肝细胞肝癌复发与转移监测中的应用研究
Application of 11C-acetate PET/CT imaging in the detection of recurrence and metastasis of hepatocellular carcinoma with intermediate and high differentiation
-
摘要:
目的探讨11C-乙酸盐PET/CT显像在中、高分化肝细胞肝癌(HCC)复发与转移监测中的应用价值。 方法回顾性分析2015年1月至2016年12月行11C-乙酸盐和18F-FDG PET/CT躯干显像的10例中、高分化HCC男性患者,其中,中分化HCC 6例,高分化HCC 4例。患者经手术或介入治疗后,甲胎蛋白进行性升高,比较11C-乙酸盐和18F-FDG PET/CT的诊断价值。PET图像上代谢高于正常肝脏组织的病灶判定为阳性,低于或类似于正常肝脏组织的病灶判定为阴性。通过勾画感兴趣区计算病灶及本底最大标准化摄取值(SUVmax)及靶/本底比值(T/B)。所有患者最终通过病理或影像学检查确诊转移或复发。 结果11C-乙酸盐显像发现18个阳性病灶,灵敏度为100%(18/18);18F-FDG显像发现5个阳性病灶,灵敏度为27.8%(5/18);两种示踪剂同时发现5个阳性病灶(在4例中分化HCC患者中),11C-乙酸盐显像探测病灶的灵敏度与两种示踪剂联合显像相同。11C-乙酸盐显像病灶SUVmax为1.3~14.2,T/B为1.1~14.3;18F-FDG显像病灶SUVmax为0.5~3.4,T/B为0.6~1.1。8例患者(13个病灶)病理证实为肿瘤复发或转移,2例患者(5个病灶)3个月后复查PET/CT或CT证实为转移。 结论11C-乙酸盐显像可显著提高中、高分化HCC复发与转移诊断的灵敏度;推荐使用11C-乙酸盐显像用于监测中、高分化HCC的复发与转移。 -
关键词:
- 癌,肝细胞 /
- 氟脱氧葡萄糖F18 /
- 乙酸盐类 /
- 正电子发射断层显像计算机体层摄影术
Abstract:ObjectivesTo investigate the value of 11C-acetate PET/CT imaging in the detection of the recurrence and metastasis of hepatocellular carcinoma (HCC) with high or medium differentiation. MethodsA total of 10 patients who underwent surgical or interventional therapy, had moderately or highly differentiated HCC, underwent 11C-acetate and 18F-FDG PET/CT trunk imaging from January 2015 to December 2016 were retrospectively analyzed. Progressive increases in alpha fetoprotein were observed in the patients after the treatment. 11C-acetate and 18F-FDG PET/CT scan were performed on the patients in one week, and the diagnostic values of the two tracers were compared. In the PET images, the lesion was positive when the metabolic level of the lesion was higher than that of a normal liver tissue and negative when the metabolic level of the lesion was lower than or same as that of a normal liver tissue. The maximum standardized uptake value(SUVmax) and the ratio of target to background(T/B) were calculated by outlining the areas of interest. All patients were diagnosed with metastasis or recurrence by pathology or imaging examination. ResultsSix patients had moderately differentiated HCC and four patients had highly differentiated HCC. 11C-acetate imaging revealed 18 positive lesions, and the sensitivity was 100%(18/18). Five positive lesions were found in 18F-FDG images, and the sensitivity was 27.8%(5/18). Two tracers revealed five positive lesions (in four patients with moderately differentiated HCC). The sensitivity of 11C-acetate imaging to detect lesions was the same as that of double tracers combined imaging. The SUVmax range of 11C-acetate imaging was 1.3-14.2, and the range of T/B was 1.1-14.3. The SUVmax range of 18F-FDG imaging was 0.5-3.4, and the range of T/B was 0.6-1.1. Eight patients (13 lesions) were pathologically confirmed to have tumor recurrence or metastasis, and two patients (5 lesions) proved to be metastatic after 3 months of follow-up. Conclusions11C-acetate imaging can significantly improve the sensitivity of the diagnosis of recurrence and metastasis of moderately and highly differentiated HCC. 11C-acetate imaging is expected to replace 18F-FDG imaging in monitoring recurrence and metastasis in moderately and highly differentiated HCC. -
图 1 中分化肝细胞肝癌患者的11C-乙酸盐及18F-FDG PET/CT显像图
Figure 1. 11C-acetate and 18F-FDG PET/CT imaging in patient with moderately differentiated hepatocellular carcinoma
图 2 高分化肝细胞肝癌患者的11C-乙酸盐及18F-FDG PET/CT显像图
Figure 2. 11C-acetate and 18F-FDG PET/CT imaging in patient with highly differentiated hepatocellular carcinoma
表 1 10例男性中、高分化肝细胞肝癌患者的临床资料及11C-乙酸盐、18F-FDG PET/CT显像结果
Table 1. Clinical data and 11C-acetate and 18F-FDG PET/CT results of 10 male cases of moderately and highly differentiated hepatocellular carcinoma
序号 年龄 肝炎病史 AFP/
(μg/L)病理类型 病灶数目 病变位置 病变大小/
(cm×cm)11C-乙酸盐 18F-FDG SUVmax T/B 阳性(+)/
阴性(-)SUVmax T/B 阳性(+)/
阴性(-)1 46 + 263.56 中分化 2 肝内 2.7×2.0 4.0 1.2 + 3.4 1.1 + 肝内 4.3×2.4 4.4 1.3 + 3.4 1.1 + 2 51 + 102.82 中分化 2 肝内 1.3×0.9 5.7 1.8 + 2.4 0.9 - 肝内 2.7×2.0 5.1 1.6 + 2.8 1.1 + 3 69 + 97.1 高分化 1 肝内 1.0×0.8 3.9 1.1 + 1.8 0.6 - 4 56 + 223.62 中分化 1 肝内 9.0×6.8 6.0 1.4 + 2.5 0.9 - 5 74 + 69.81 高分化 1 肝内 9.8×7.7 14.2 3.2 + 3.3 0.9 - 6 53 + > 24 200 中分化 2 肝内 2.9×2.2 4.2 1.5 + 3.1 0.8 - 肝内 1.6×1.2 6.2 2.2 + 3.2 1.1 + 7 49 + 476.09 中分化 1 肝内 2.1×1.6 4.5 1.6 + 2.7 0.9 - 8 67 + 81.62 高分化 2 肝内 3.1×2.5 6.7 1.7 + 2.9 1 - 肝内 2.1×1.9 5.8 1.5 + 3 0.9 - 9 27 + 611.42 中分化 2 肝内 2.4×1.4 7.1 1.8 + 2.8 1 - 肝内 2.2×1.4 6.5 1.7 + 3 1.1 + 10 63 + 371.5 高分化 4 肝内 1.6×1.1 3.9 1.6 + 3 1 - 脾门区 3.0×1.6 4.3 14.3 + 0.6 1 - 腹膜后 1.5×1.3 5.5 9.2 + 0.5 0.8 - 小网膜 0.9×0.7 1.3 3.3 + 0.6 1 - 注:表中,“+”为阳性,为阴性;FDG:氟脱氧葡萄糖;PET/CT:正电子发射断层显像计算机体层摄影术;AFP:甲胎蛋白; SUVmax:最大标准化摄取值;T/B:靶/本底比值  下载: 导出CSV
下载: 导出CSV
-
[1] Ho CL, Yu SC, Yeung DW. 11C-acetate PET imaging in hepatocellular carcinoma and other liver masses[J]. J Nucl Med, 2003, 44(2):213-221. [2] Larsson P, Arvidsson D, Björnstedt M, et al. Adding 11C-acetate to 18F-FDG at PET Examination Has an Incremental Value in the Diagnosis of Hepatocellular Carcinoma[J]. Mol Imaging Radionucl Ther, 2012, 21(1):6-12. DOI:10.4274/Mirt.87. [3] Cheung TT, Ho CL, Lo CM, et al. 11C-acetate and 18F-FDG PET/CT for clinical staging and selection of patients with hepatocellular carcinoma for liver transplantation on the basis of Milan criteria:surgeon's perspective[J]. J Nucl Med, 2013, 54(2):192-200. DOI:10.2967/jnumed.112.107516. [4] Park JW, Kim JH, Kim SK, et al. A prospective evaluation of 18F-FDG and 11C-acetate PET/CT for detection of primary and metastatic hepatocellular carcinoma[J]. J Nucl Med, 2008, 49(12):1912-1921. DOI:10.2967/jnumed.108.055087. [5] Huo L, Dang Y, Lv J, et al. Application of dual phase imaging of 11C-acetate positron emission tomography on differential diagnosis of small hepatic lesions[J/OL]. PLoS One, 2014, 9(5): e96517[2018-01-12]. https: //www. ncbi. nlm. nih. gov/pmc/articles/PMC4015995. DOI: 10.1371/journal.pone.0096517. [6] Magini G, Farsad M, Frigerio M, et al. C-11 acetate does not enhance usefulness of F-18 FDG PET/CT in differentiating between focal nodular hyperplasia and hepatic adenoma[J]. Clin Nucl Med, 2009, 34(10):659-665. DOI:10.1097/RLU.0b013e3181b53488. [7] Ho CL, Chen S, Cheng TK, et al. PET/CT characteristics of isolated bone metastases in hepatocellular carcinoma[J]. Radiology, 2011, 258(2):515-523. DOI:10.1148/radiol.10100672. [8] Ho CL, Chen S, Yeung DW, et al. Dual-tracer PET/CT imaging in evaluation of metastatic hepatocellular carcinoma[J]. J Nucl Med, 2007, 48(6):902-909. DOI:10.2967/jnumed.106.036673. [9] Yoon KT, Kim JK, Kim DY, et al. Role of 18F-fluorodeoxyglucose positron emission tomography in detecting extrahepatic metastasis in pretreatment staging of hepatocellular carcinoma[J]. Oncology, 2007, 72 Suppl 1:S104-110. DOI:10.1159/000111715. [10] Yoshimoto M, Waki A, Yonekura Y, et al. Characterization of acetate metabolism in tumor cells in relation to cell proliferation:acetate metabolism in tumor cells[J]. Nucl Med Biol, 2001, 28(2):117-122. doi: 10.1016/S0969-8051(00)00195-5 [11] Salem N, Kuang Y, Corn D, et al.[(Methyl)1-11C]-acetate metabolism in hepatocellular carcinoma[J]. Mol Imaging Biol, 2011, 13(1):140-151. DOI:10.1007/s11307-010-0308-y. [12] Polanec SH, Andrzejewski P, Baltzer PAT, et al. Multiparametric[11C]Acetate positron emission tomography-magnetic resonance imaging in the assessment and staging of prostate cancer[J/OL]. PLoS One, 2017, 12(7): e0180790[2018-01-12]. https: //www. ncbi. nlm. nih. gov/pmc/articles/PMC5515396. DOI: 10.1371/journal.pone.0180790. [13] Ho CL, Chen S, Ho KM, et al. Dual-tracer PET/CT in renal angiomyolipoma and subtypes of renal cell carcinoma[J]. Clin Nucl Med, 2012, 37(11):1075-1082. DOI:10.1097/RLU.0b013e318266-cde2. -

 点击查看大图
点击查看大图

图(2)表(1)
计量
- 文章访问数: 2840
- HTML全文浏览量: 1835
- PDF下载量: 6