




-
非小细胞肺癌(non-small-cell lung cancer,NSCLC)占全部肺癌的80%,通过手术、放疗和药物的综合治疗,患者生存已得到明显改善[1]。对于行根治性切除术后病理分期为ⅢA-N2(pⅢA-N2)的NSCLC患者,术后辅助化疗可显著提高生存期[2-3],但局部区域复发率仍高达20%~40%[4-5]。在多种实体瘤的治疗中,术后放疗均可有效地杀灭潜在的亚临床病灶,提高局部控制率进而进一步改善生存[6-7]。对于pⅢA-N2 NSCLC患者,相关研究结果显示术后放疗(postoperative radiotherapy, PORT)虽能明显降低局部区域复发率,但对生存的影响仍不确定[8-13]。其原因可能是胸部放疗相关的心肺毒性降低了生存获益,这些不良反应可通过放疗技术的进步逐渐改善。此外,pⅢA-N2 NSCLC患者的异质性很大,可通过亚组分析确定能从PORT获益的亚组人群,达到精准治疗的目的,同时避免无生存获益的患者接受过度治疗。笔者回顾性分析804例ⅢA-N2 NSCLC患者的临床资料,依据简单的术前临床资料,筛选能从PORT获益的亚组人群。
-
① 肺部肿瘤经细胞学或病理学证实为NSCLC;②治疗前均有完善的头部MRI、颈部和腹部B超或CT、胸部CT或PET/CT、全身骨扫描分期检查资料,无远处转移病灶;③患者在我院接受肺部肿瘤根治切除手术,依据2009年第7版美国癌症联合委员会分期,术后病理分期为ⅢA-N2;④患者术后接受含铂类方案的化疗。
-
① 术前行新辅助化疗的患者;②镜下切缘阳性(R1)或术后肿瘤残存(R2)的患者;③其他部位恶性肿瘤病史(既往或同时),不包括可治愈的非黑色素瘤性皮肤癌和子宫颈原位癌;④未控的心脏疾病或者近6个月内发生心肌梗死;⑤有精神疾病史;⑥处于妊娠、哺乳期;⑦间质性肺炎或活动期肺纤维化;⑧活动性感染。
-
我院2006年1月至2015年12月收治的NSCLC根治术后pⅢA-N2患者中,符合入组标准的患者804例,其中男性475例、女性329例,年龄25~80岁,中位年龄56岁。通过增强CT或者PET/CT获取准确的临床淋巴结分期。CT上淋巴结短径≥10 mm或者PET/CT上淋巴结SUV>2.5定义为转移淋巴结。根据化疗后是否行PORT,将804例入组患者分为PORT组和单纯化疗组,其中PORT组276例,单纯化疗组528例。所有患者或其家属均于治疗前签署了知情同意书。
-
手术方式包括肺叶切除、楔形切除、袖状切除、双叶切除、全肺切除+纵隔淋巴结清扫或系统纵隔淋巴结取样术。术后化疗采用基于铂类的双药方案,另一种药物包括紫杉醇(百时美施贵宝(中国)投资有限公司)、多西他赛(江苏恒瑞医药股份有限公司)、培美曲塞、吉西他滨(江苏豪森药业股份有限公司)、长春瑞滨(齐鲁制药有限公司)。
-
患者取仰卧位,面罩或体膜固定身体,模拟定位CT(西门子,Somatom Definition AS,德国)扫描范围为颅底至腰2椎体水平,扫描层距5 mm。采用Pinnacle TPS软件(飞利浦,pinnacle 7.4f,荷兰)进行放疗靶区勾画及计划设计。靶区勾画综合手术前、后的影像学资料,临床靶体积主要包括手术残端、同侧肺门、同侧纵隔和隆凸下淋巴结区域。计划靶体积为临床靶体积外扩5 mm形成。计划靶体积的设计处方剂量为50~60 Gy,剂量分割为1.8~2.2 Gy/次,1次/d,5次/周。处方剂量至少覆盖95%的计划靶体积,且热点最高剂量限制在处方剂量的107%以内,脊髓最大剂量限制为≤45 Gy。使用三维适形或调强放疗技术进行计划设计。射线选择6 MV X射线,通过Pinnacle TPS软件获得剂量体积直方图等相关物理学参数。采用直线加速器(医科达,Agility,瑞典)进行放射治疗。
-
首程治疗结束后,2年内每3个月检查1次颈部和腹部B超或CT、胸部CT,2年后每6个月检查1次,5年后每年检查1次。每半年检查1次头部MRI,每年检查1次全身骨扫描。804例患者,失访66例,随访率为91.8%。
-
采用SPSS 22.0软件进行统计学分析。计数资料比较采用卡方检验,采用Log Rank法进行单因素预后分析,Cox回归进行多因素预后分析及亚组分析。生存分析采用Kaplan-Meier法,组间生存率比较采用Log Rank检验。P<0.05表示差异有统计学意义。
-
PORT组和单纯化疗组患者的中位年龄分别为54.5岁和57.0岁,PORT组 < 60岁的患者更多(χ2=15.48,P < 0.001);化疗周期数为3~4个的患者亦更多(χ2=18.42,P<0.001),差异均有统计学意义。其余一般临床资料两组间差异无统计学意义(χ2=0.48~4.28,均P>0.05)。两组患者的一般临床资料见表 1。
临床因素 总例数(%) 单纯化疗组(%) PORT组(%) χ2值 P值 性别 男性 475(59.1) 300(56.8) 175(63.4) 2.99 0.084 女性 329(40.9) 228(43.2) 101(36.6) 年龄/岁 <60 519(64.6) 315(59.7) 204(73.9) 15.48 <0.001 ≥60 285(35.4) 213(40.3) 72(26.1) 吸烟 否 394(49.0) 269(50.9) 125(45.3) 2.10 0.147 是 410(51.0) 259(49.1) 151(54.7) 术前T分期 T1 257(32.0) 167(31.6) 90(32.6) 4.28 0.369 T2 431(53.5) 288(54.5) 143(51.9) T3 74(9.2) 51(9.7) 23(8.3) T4 7(0.9) 3(0.6) 4(1.4) Tx 35(4.4) 19(3.6) 16(5.8) 术前N分期 N0 340(42.3) 221(41.9) 119(43.1) 0.48 0.924 N1 73(9.1) 49(9.3) 24(8.7) N2 379(47.1) 251(47.5) 128(46.4) Nx 12(1.5) 7(1.3) 5(1.8) 病理类型 鳞癌 197(24.5) 129(24.4) 68(24.6) 1.36 0.508 腺癌 554(68.9) 368(69.7) 186(67.4) 其他 53(6.6) 31(5.9) 22(8.0) 化疗周期数 1~2 64(8.0) 56(10.6) 8(2.9) 18.42 <0.001 3~4 658(81.8) 412(78.0) 246(89.1) ≥5 40(5.0) 30(5.7) 10(3.6) 不详 42(5.2) 30(5.7) 12(4.3) 注:表中,PORT:术后放疗;NSCLC:非小细胞肺癌。 表 1 PORT组和单纯化疗组804例NSCLC患者的一般临床资料比较
Table 1. Comparison of general clinical data between non-postoperative radiotherapy group and postoperative radiotherapy group of 804 non-small-cell lung cancer patients
全组患者化疗周期数中位数为4周期。化疗开始日期距离手术日期的中位值为1.1个月,放疗开始日期距化疗开始日期的中位值为3.5个月。计划靶体积的处方剂量中位值为50 Gy(30~64 Gy),单次剂量中位值为2 Gy/次(1.8~2.2 Gy/次)。
-
截至2017年6月30日,全组患者中位随访时间为32.07个月(2.50~133.98个月),中位生存时间为68.67个月,2年、5年总生存(overall survival,OS)分别为82.1%、54.5%,中位无病生存(disease-free survival, DFS)为19.84个月,中位无局部区域复发生存(locoregional recurrence-free survival, LRFS)为120.31个月,中位无远处转移生存(distant metastasis-free survival, DMFS)为30.52个月。
对与OS相关的多项临床因素(包括性别、年龄、吸烟状态、术前T分期、术前N分期、病理类型、化疗周期数、是否PORT)进行单因素分析,结果显示男性、年龄≥60岁、术前T分期增加、术前N分期为N1~N2、病理类型为非鳞癌非腺癌、化疗周期数为1~2、未行PORT是显著影响OS的不良预后因素(表 2)。
临床因素 例数(%) 中位生存
时间/月5年
OS/%χ2值 P值 性别 男性 475(59.1) 64.10 50.6 7.238 0.007 女性 329(40.9) 74.35 60.0 年龄/岁 <60 519(64.6) 85.29 58.7 9.131 0.003 ≥60 285(35.4) 55.29 46.7 吸烟 否 394(49.0) 68.67 55.9 2.720 0.099 是 410(51.0) 65.71 52.8 术前T分期 T1 257(32.0) 92.09 61.7 23.323 < 0.001 T2 431(53.6) 65.68 53.0 T3 74(9.2) 34.14 36.4 T4 7(0.9) - - Tx 35(4.4) 72.64 55.1 术前N分期 N0 340(42.3) 97.31 61.9 21.039 < 0.001 N1 73(9.1) 47.54 39.9 N2 379(47.1) 60.03 50.3 Nx 12(1.5) 68.67 58.3 病理类型 鳞癌 197(24.5) 91.14 55.7 18.024 < 0.001 腺癌 554(68.9) 68.67 54.9 其他 53(6.6) 34.04 38.0 化疗周期数 1~2 64(8.0) 33.68 33.4 21.134 < 0.001 3~4 658(81.8) 70.77 55.2 ≥5 40(5.0) - 63.9 不详 42(5.2) - 64.5 PORT 否 528(65.7) 64.10 50.8 5.253 0.022 是 276(34.3) 97.31 60.6 注:表中,pⅢA-N2:病理分期为ⅢA-N2;NSCLC:非小细胞肺癌;OS:总生存;PORT:术后放疗;“-”:无相关统计结果。 表 2 804例pⅢA-N2 NSCLC患者单因素预后分析结果
Table 2. Univariate analysis for overall survival of 804 pⅢA-N2 non-small-cell lung cancer patients
多因素分析结果显示性别、年龄、术前N分期、病理类型、是否PORT为OS相关的独立预后因素(表 3)。
影响因素 偏回归系数 偏回归系数标准误 Wald P值 OR值 OR值95%CI 性别 -0.418 0.183 5.196 0.023 0.658 0.460~0.943 年龄 -0.312 0.123 6.423 0.011 1.367 1.073~1.740 吸烟 -0.061 0.180 0.114 0.735 0.941 0.661~1.339 术前T分期 -0.114 0.059 3.719 0.054 1.121 0.998~1.259 术前N分期 -0.141 0.059 5.789 0.016 1.151 1.026~1.292 病理类型 -0.288 0.120 5.774 0.016 1.333 1.054~1.686 化疗周期数 -0.191 0.098 3.816 0.051 0.826 0.681~1.001 PORT -0.283 0.130 4.694 0.030 0.754 0.584~0.973 注:表中,pⅢA-N2:病理分期为ⅢA-N2;NSCLC:非小细胞肺癌;PORT:术后放疗。 表 3 804例pⅢA-N2 NSCLC患者Cox模型多因素预后分析结果
Table 3. Multivariate analysis for overall survival of 804 pⅢA-N2 non-small-cell lung cancer patients
-
PORT组和单纯化疗组的中位OS、中位DFS、中位LRFS、中位DMFS分别为97.31和64.10个月(χ2=5.253,P=0.022)、25.76和17.97个月(χ2=18.397, P < 0.001)、120.31和101.03个月(χ2=15.358, P < 0.001)、36.83和28.49个月(χ2=6.434, P=0.011),PORT组的各生存参数均显著优于单纯化疗组,且差异有统计学意义(表 4)。
组别 OS DFS LRFS DMFS 中位值/月 2年/% 5年/% 中位值/月 2年/% 5年/% 中位值/月 2年/% 5年/% 中位值/月 2年/% 5年/% 非PORT组 64.10 80.0 50.8 17.97 42.1 21.5 101.03 71.9 59.0 28.49 54.3 30.6 PORT组 97.31 86.1 60.6 25.76 53.1 36.7 120.31 83.2 73.6 36.83 60.1 42.8 χ2值 5.253 18.397 15.358 6.434 P值 0.022 < 0.001 < 0.001 0.011 注:表中,pⅢA-N2:病理分期为ⅢA-N2;NSCLC:非小细胞肺癌;PORT:术后放疗;OS:总生存;DFS:无病生存;LRFS:无局部区域复发生存;DMFS:无远处转移生存。 表 4 804例pⅢA-N2 NSCLC患者PORT与生存相关性的单因素分析结果
Table 4. Stratified analysis for survive of 804 pⅢA-N2 non-small-cell lung cancer patients according to postoperative radiotherapy
-
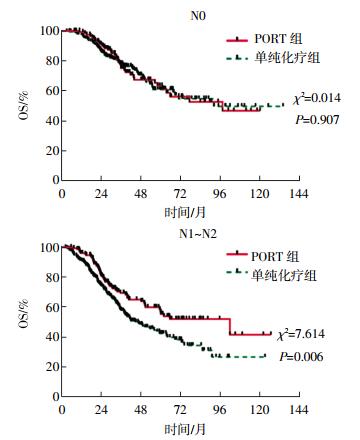
根据以下术前临床因素(包括性别、年龄、吸烟状态、肿瘤位置、术前T分期、术前N分期、术前分期、病理类型)进行预后因素的亚组分析,结果显示以下亚组行PORT能有OS获益(图 1),分别是:男性患者(HR:0.697,95%CI:0.513~0.947,P=0.021)(图 2),吸烟的患者(HR:0.648,95%CI:0.464~0.905,P=0.011)(图 3),术前N分期为N1~N2的患者(HR:0.640,95%CI:0.465~0.881,P=0.006)(图 4),术前分期为Ⅲ期的患者(HR:0.688,95%CI:0.484~0.980,P=0.038),以及病理类型为腺癌的患者(HR:0.726,95%CI:0.527~0.999,P=0.049)。

图 1 804例pⅢA-N2非小细胞肺癌患者PORT与生存相关性:术前临床因素亚组分析 图中,pⅢA-N2:病理分期为ⅢA-N2;PORT:术后放疗。
Figure 1. Correlation between postoperative radiotherapy and survival in 804 pⅢA-N2 NSCLC patients—subgroup analysis of preoperative clinical factors

图 2 PORT组和单纯化疗组pⅢA-N2非小细胞肺癌患者的OS曲线:不同性别的亚组分析 图中,OS:总生存;PORT:术后放疗;pⅢA-N2:病理分期为ⅢA-N2。
Figure 2. Overall survival curve for the postoperative radiothrapy and non-postoperative radiothrapy: subgroup analysis of different gender

图 3 PORT组和单纯化疗组pⅢA-N2非小细胞肺癌患者的OS曲线:不同吸烟状态的亚组分析 图中,OS:总生存;PORT:术后放疗;pⅢA-N2:病理分期为ⅢA-N2。
Figure 3. Overall survival curve for postoperative radiothrapy and non-postoperative radiothrapy: subgroup analysis of different smoking status

图 4 PORT组和单纯化疗组pⅢA-N2非小细胞肺癌患者的OS曲线:不同术前N分期亚组分析 图中,OS:总生存;PORT:术后放疗;pⅢA-N2:病理分期为ⅢA-N2。
Figure 4. Overall survival curve for postoperative radiothrapy and non-postoperative radiothrapy: subgroup analysis of different preoperative N staging
-
pⅢA-N2 NSCLC患者的术后化疗能明确改善生存,已成为此类患者术后的标准疗法。大量研究结果证实,PORT能显著提高局部控制率,但是否能提高生存期仍无明确结论。对9项行PORT的随机临床研究进行的荟萃分析[8]结果显示,PORT组(n=1056)和单纯手术组(n=1072)的2年OS分别为48%和55%,PORT组的生存率显著降低(P=0.001);进一步的亚组分析结果表明,对于Ⅰ~Ⅱ期和N0~N1期的患者,PORT会导致全组OS显著降低,但能轻度改善Ⅲ期和pN2期亚组患者的生存(差异无统计学意义)。上述研究中,使用落后的二维放疗技术导致了心肺毒性引起的病死率增高,抵消了放疗可能带来的生存获益。随着新放疗技术的逐渐普及,放疗的不良反应显著减少,PORT的价值再次引起关注。Lally等[9]基于监测(Surveillance)、流行病学(Epidemiology)与最终结果(End results)数据库(1988-2000年)的回顾性研究结果显示,PORT可显著改善N2期患者OS,5年OS由20%提高至27%。Douillard等[10]按照术后淋巴结转移状态进行分层的亚组分析结果也显示,术后放疗能显著改善pN2患者的生存,观察组的5年OS由17%提高至21%,术后化疗组由34%提高至47%。2011年Dai等[11]的回顾性研究包括了2003年1月至2005年12月我院收治的221例手术完全切除的pⅢA-N2 NSCLC患者,96例接受PORT的患者中有41例采用适形放疗,结果显示PORT能显著改善OS(P=0.046)、DFS(P=0.009)、LRFS(P=0.025)和DMFS(P=0.001),单因素和多因素分析结果均证实PORT能显著改善患者预后。但2007年Perry等[12]的随机对照研究结果显示,对于根治术后的pⅢA-N2 NSCLC患者,PORT不能显著提高无失败生存和OS。虽然此研究因入组太慢而提前结束,但其仍是至今发表的针对术后化疗后PORT是否能提高生存的唯一的随机研究。此外,欧洲开展的类似的Lung ART随机研究和由我院牵头的CNCI随机研究均尚在进行中。因此,针对pⅢA-N2 NSCLC患者的术后治疗,美国国立综合癌症网络并未把辅助化疗后的PORT作为Ⅰ类证据。2014年Patel等[13]发表的一项荟萃研究结果显示,将使用Co-60二维放疗技术的患者排除后,PORT能改善pⅢA-N2 NSCLC患者的局部控制和OS。Billiet等[14]发表的荟萃分析也得到了相同的结果。本研究中所有患者均使用三维或者调强放疗技术,PORT组的OS、DFS、LRFS、DMFS均显著优于单纯化疗组,多因素分析结果显示PORT是与OS相关的独立预后因素,这与大多数荟萃研究的结果一致。
pⅢA-N2 NSCLC是一组异质性较大的疾病,并非所有患者都能从PORT中获益,需要进一步筛选可获益的亚组人群以达到精确治疗的目的。多项回顾性研究分析了PORT对不同亚组患者的作用,进一步完善了这类患者的个体化治疗的相关信息。Sawyer等[15]回顾性分析发现,PORT能提高局部复发高危患者的局部控制率和生存;Matsuguma等[16]分析发现,多站N2的患者行PORT可以提高生存,而单站N2的患者无明显改善。Hui等[17]回顾性分析了2003年1月至2005年12月我院收治的221例术后pⅢA-N2 NSCLC患者,依据5种预后不良因素(吸烟指数≤400、术前N分期为N2、病理T分期为T3、病理类型为鳞癌、阳性淋巴结≥4)建立了一项预后指数(PORT-I),每个不良因素计1分,0~1分为低危,2分为中危,3~5分为高危,高危患者行PORT能显著改善OS(P = 0.000)、DFS(P=0.000)和LRFS(P=0.006),因此,对于高危患者强烈推荐PORT。
本研究中的亚组分析结果显示男性、吸烟、术前N分期为N1~N2、术前分期为Ⅲ期、病理类型为腺癌的患者行PORT可有OS获益,与Hui等[17]发表的回顾性分析结果有部分不同。究其原因在于Hui等[17]的研究纳入的2003年1月至2005年12月手术的221例患者中,包含了55例采用二维放疗技术的患者,而本研究纳入了2006年1月至2015年12月的804例患者,均采用三维或调强放疗技术,病例数以及放疗技术的差异,均可能导致结果不完全一致。McGovern等[18]分析了831例Ⅰ~Ⅲ期NSCLC患者的性别对放疗疗效的影响,结果显示女性的5年OS、无进展生存率和DMFS均明显高于男性,而本研究中男性患者行PORT能获益,可能与术后男性患者的恢复及放疗耐受性较女性更好有关。Vogelius等[19]发表的一项基于文献的荟萃分析结果显示,吸烟可减少放射性肺炎的发生(P=0.008),肺炎的发生率降低可能转化为一部分行放疗患者的生存获益,这可能是本研究中吸烟的患者PORT获益的原因之一。1997年Ruckdeschel等[20]根据纵隔镜下淋巴结转移数目提出将未手术的ⅢA-N2细分为4类,即ⅢA1~ⅢA4,2003年进一步修订为美国胸科医师学会的分类标准[21]。其中ⅢA1为术后病理发现的淋巴结转移;ⅢA2为术中发现单站淋巴结转移;ⅢA3为术前检查发现的单站或多站淋巴结转移,检查手段包括纵隔镜淋巴结活检、淋巴结活检或PET/CT;ⅢA4为纵隔大块或固定的多站淋巴结转移,不能行手术切除。本研究中术前N0的患者包括ⅢA1~ⅢA2,术前N1~N2等同于ⅢA3。与术前ⅢA1 ~ⅢA2相比,ⅢA3和临床Ⅲ期的患者具有更高的肿瘤负荷和远处转移趋势,即使肿瘤完全切除后,这部分患者仍具有较高的治疗失败率,预后更差[22],因此这部分患者行PORT可通过局部控制的增加转化为生存获益。Asamura等[23]报道了一项包括13 010例可切除肺癌患者的预后研究,其中部分腺癌患者进行了PORT,结果发现腺癌患者的预后更好;本研究结果显示腺癌患者行PORT有生存获益,再次佐证了这一结论。
综上所述,辅助化疗后行PORT能改善根治术后pⅢA-N2 NSCLC患者的OS、DFS、LRFS和DMFS。亚组分析结果发现部分术前临床因素具有预测PORT后有OS获益的亚组人群的价值,包括男性、吸烟、术前N分期为N1~N2、术前分期为Ⅲ期以及病理类型为腺癌的患者。基于本研究的结果,我们可以依据相关的术前临床资料,通过最简单有效的方法筛选出能通过PORT获益的亚组人群,有助于这类患者在术前的多学科讨论中明确综合治疗的模式,指导患者的下一步治疗。因本研究为回顾性研究,组间存在选择性偏倚等不平衡因素,需扩大样本量的前瞻性随机研究进一步证实。
术前临床因素预测pⅢA-N2非小细胞肺癌术后放疗获益人群的研究
Preoperative clinical risk factors in selecting patients with pathological ⅢA-N2 non-small-cell lung cancer benefiting from postoperative radiotherapy
-
摘要:
目的分析病理分期为ⅢA-N2(pⅢA-N2)的非小细胞肺癌(NSCLC)患者行手术+辅助化疗后,加或不加术后放疗(PORT)的疗效,从术前临床因素中筛选能从PORT中获益的亚组人群。 方法回顾性分析2006年1月至2015年12月行根治性手术的pⅢA-N2 NSCLC患者804例。其中,PORT组患者276例,单纯化疗组528例。通过增强CT或者PET/CT获取准确的临床淋巴结分期。CT上淋巴结短径≥10 mm或者PET/CT上淋巴结SUV>2.5定义为转移淋巴结。PORT使用三维适形或调强放疗技术,计划靶体积的设计处方剂量为50~60 Gy,剂量分割为1.8~2.2 Gy/次。采用Log Rank法进行单因素预后分析,Cox回归进行多因素预后分析及亚组分析,通过Kaplan-Meier法和Log Rank检验评估PORT对总生存(OS)、无病生存(DFS)、无局部区域复发生存(LRFS)和无远处转移生存(DMFS)的影响,并进行亚组分析。 结果全组患者的中位随访时间为32.07个月。2年、5年OS分别为82.1%、54.5%,中位DFS为19.84个月,中位LRFS为120.31个月,中位DMFS为30.52个月。行PORT显著改善了OS(χ2=5.253,P=0.022)、DFS(χ2=18.397,P < 0.001)、LRFS(χ2=15.358,P < 0.001)和DMFS(χ2=6.434,P=0.011),且差异均有统计学意义。单因素分析结果显示,男性、年龄≥60岁、术前T分期增加、术前N分期为N1~N2、病理类型为非鳞癌非腺癌、化疗周期为1~2、未行PORT是显著影响OS的不良预后因素。多因素分析结果显示性别、年龄、术前N分期、病理类型、是否PORT为OS相关的独立预后因素;行PORT有OS获益的亚组分别为男性(HR:0.697,95% CI:0.513~0.947,P=0.021)、吸烟(HR:0.648,95% CI:0.464~0.905,P=0.011)、术前N分期为N1~N2(HR:0.640,95% CI:0.465~0.881,P=0.006)、临床分期为Ⅲ期(HR:0.688,95% CI:0.484~0.980,P=0.038)以及病理类型为腺癌(HR:0.726,95% CI:0.527~0.999,P=0.049)的患者。 结论PORT能改善全组患者的OS、DFS、LRFS和DMFS。部分术前临床因素具有预测PORT后有OS获益的亚组人群的价值,包括男性、吸烟、术前N分期为N1~N2、临床分期为Ⅲ期以及病理类型为腺癌的患者。 Abstract:ObjectivePathological ⅢA-N2 non-small-cell lung cancer (pⅢA-N2 NSCLC) is a heterogeneous population, and the role of postoperative radiotherapy(PORT) after the adjuvant chemotherapy (ACT) in pⅢA-N2 NSCLC remains ambiguous. Not all pⅢA-N2 patients can benefit from PORT. This study was performed to identify the subgroup that can benefit from PORT after ACT. MethodsThis study included 804 pⅢA-N2 NSCLC patients completing radical resection and ACT from January 2006 to December 2015. The patients were divided into two groups:PORT group, patients who underwent PORT after radical resection and ACT; and NON-PORT group, control group of patients who only underwent radical resection and ACT. The PORT and NON-PORT groups consisted of 276 and 528 patients, respectively. Accurate clinical lymph node staging was obtained through contrast-enhanced CT and/or PET/CT. Lymph nodes measured in the short axis ≥ 10 mm on CT or SUV>2.5 on PET/CT were considered as metastases. Using 3-dimensional conformal radiation therapy or intensity modulated radiation therapy techniques, PORT was administered at 1.8-2.2 Gy per fraction to a prescription dose to the planning target volume of 50-60 Gy. Outcome measures included overall survival(OS), disease-free survival(DFS), locoregional recurrence-free survival(LRFS), and distant metastasis-free survival(DMFS). Kaplan-Meier, Log Rank test, and Cox regression were used to analyze survival data and identify prognostic factors. Statistically significant difference was set to P < 0.05. ResultsMedian follow-up time was 32.07 months. The 2-year and 5-year OS of the patients in the entire cohort were 82.1% and 54.5%, respectively. The median values of the DFS, LRFS, and DMFS were 19.84, 120.31, and 30.52 months, respectively. In the overall study cohort, the median values of the OS(97.31 months vs. 64.10 months, χ2=5.253, P=0.022), DFS (25.76 months vs. 17.97 months, χ2=18.397, P < 0.001), LRFS(120.31 months vs. 101.03 months, χ2=15.358, P < 0.001) and DMFS(36.83 months vs. 28.49 months, χ2=6.434, P=0.011) were significantly higher in the PORT group than in the NON-PORT group. Univariate analysis showed that the adverse prognostic factors which significantly affected OS were:male, age ≥ 60 years, advanced preoperative T staging, preoperative N1-N2, non-squamous carcinoma and non-adenocarcinoma, 1-2 chemotherapy cycles and NON-PORT. Multivariate Cox analyses revealed that factors independently associated with longer OS were PORT(HR=0.754, 95%CI=0.584-0.973, P=0.03), female, age < 60 years, preoperative clinical N0, clinic stage Ⅰ-Ⅱ, adenocarcinoma, or squamous carcinoma. Subgroup analysis indicated that several preoperative clinical factors could predict the population that would benefit from PORT after ACT. These factors included male(HR=0.697, 95%CI=0.513-0.947, P=0.021), smoking patient(HR=0.648, 95%CI=0.464-0.905, P=0.011), preoperative clinical N1-N2(HR=0.640, 95%CI=0.465-0.881, P=0.006), clinic stage Ⅲ(HR=0.688, 95%CI=0.484-0.980, P=0.038), and adenocarcinoma(HR=0.726, 95%CI=0.527-0.999, P=0.049). ConclusionsPORT after ACT could significantly improve the 5-year OS, DFS, LRFS, and DMFS in pⅢA-N2 NSCLC patients. Moreover, PORT could improve the 5-year OS of the subgroups with the following characteristics:male, smoking patient, preoperative clinical N1-N2, clinic stage Ⅲ, and adenocarcinoma. -
Key words:
- Carcinoma, non-small-cell lung /
- Radiotherapy /
- Chemotherapy /
- Therapeutic evaluation
-
图 1 804例pⅢA-N2非小细胞肺癌患者PORT与生存相关性:术前临床因素亚组分析 图中,pⅢA-N2:病理分期为ⅢA-N2;PORT:术后放疗。
Figure 1. Correlation between postoperative radiotherapy and survival in 804 pⅢA-N2 NSCLC patients—subgroup analysis of preoperative clinical factors
图 2 PORT组和单纯化疗组pⅢA-N2非小细胞肺癌患者的OS曲线:不同性别的亚组分析 图中,OS:总生存;PORT:术后放疗;pⅢA-N2:病理分期为ⅢA-N2。
Figure 2. Overall survival curve for the postoperative radiothrapy and non-postoperative radiothrapy: subgroup analysis of different gender
图 3 PORT组和单纯化疗组pⅢA-N2非小细胞肺癌患者的OS曲线:不同吸烟状态的亚组分析 图中,OS:总生存;PORT:术后放疗;pⅢA-N2:病理分期为ⅢA-N2。
Figure 3. Overall survival curve for postoperative radiothrapy and non-postoperative radiothrapy: subgroup analysis of different smoking status
图 4 PORT组和单纯化疗组pⅢA-N2非小细胞肺癌患者的OS曲线:不同术前N分期亚组分析 图中,OS:总生存;PORT:术后放疗;pⅢA-N2:病理分期为ⅢA-N2。
Figure 4. Overall survival curve for postoperative radiothrapy and non-postoperative radiothrapy: subgroup analysis of different preoperative N staging
表 1 PORT组和单纯化疗组804例NSCLC患者的一般临床资料比较
Table 1. Comparison of general clinical data between non-postoperative radiotherapy group and postoperative radiotherapy group of 804 non-small-cell lung cancer patients
临床因素 总例数(%) 单纯化疗组(%) PORT组(%) χ2值 P值 性别 男性 475(59.1) 300(56.8) 175(63.4) 2.99 0.084 女性 329(40.9) 228(43.2) 101(36.6) 年龄/岁 <60 519(64.6) 315(59.7) 204(73.9) 15.48 <0.001 ≥60 285(35.4) 213(40.3) 72(26.1) 吸烟 否 394(49.0) 269(50.9) 125(45.3) 2.10 0.147 是 410(51.0) 259(49.1) 151(54.7) 术前T分期 T1 257(32.0) 167(31.6) 90(32.6) 4.28 0.369 T2 431(53.5) 288(54.5) 143(51.9) T3 74(9.2) 51(9.7) 23(8.3) T4 7(0.9) 3(0.6) 4(1.4) Tx 35(4.4) 19(3.6) 16(5.8) 术前N分期 N0 340(42.3) 221(41.9) 119(43.1) 0.48 0.924 N1 73(9.1) 49(9.3) 24(8.7) N2 379(47.1) 251(47.5) 128(46.4) Nx 12(1.5) 7(1.3) 5(1.8) 病理类型 鳞癌 197(24.5) 129(24.4) 68(24.6) 1.36 0.508 腺癌 554(68.9) 368(69.7) 186(67.4) 其他 53(6.6) 31(5.9) 22(8.0) 化疗周期数 1~2 64(8.0) 56(10.6) 8(2.9) 18.42 <0.001 3~4 658(81.8) 412(78.0) 246(89.1) ≥5 40(5.0) 30(5.7) 10(3.6) 不详 42(5.2) 30(5.7) 12(4.3) 注:表中,PORT:术后放疗;NSCLC:非小细胞肺癌。  下载: 导出CSV
下载: 导出CSV
表 2 804例pⅢA-N2 NSCLC患者单因素预后分析结果
Table 2. Univariate analysis for overall survival of 804 pⅢA-N2 non-small-cell lung cancer patients
临床因素 例数(%) 中位生存
时间/月5年
OS/%χ2值 P值 性别 男性 475(59.1) 64.10 50.6 7.238 0.007 女性 329(40.9) 74.35 60.0 年龄/岁 <60 519(64.6) 85.29 58.7 9.131 0.003 ≥60 285(35.4) 55.29 46.7 吸烟 否 394(49.0) 68.67 55.9 2.720 0.099 是 410(51.0) 65.71 52.8 术前T分期 T1 257(32.0) 92.09 61.7 23.323 < 0.001 T2 431(53.6) 65.68 53.0 T3 74(9.2) 34.14 36.4 T4 7(0.9) - - Tx 35(4.4) 72.64 55.1 术前N分期 N0 340(42.3) 97.31 61.9 21.039 < 0.001 N1 73(9.1) 47.54 39.9 N2 379(47.1) 60.03 50.3 Nx 12(1.5) 68.67 58.3 病理类型 鳞癌 197(24.5) 91.14 55.7 18.024 < 0.001 腺癌 554(68.9) 68.67 54.9 其他 53(6.6) 34.04 38.0 化疗周期数 1~2 64(8.0) 33.68 33.4 21.134 < 0.001 3~4 658(81.8) 70.77 55.2 ≥5 40(5.0) - 63.9 不详 42(5.2) - 64.5 PORT 否 528(65.7) 64.10 50.8 5.253 0.022 是 276(34.3) 97.31 60.6 注:表中,pⅢA-N2:病理分期为ⅢA-N2;NSCLC:非小细胞肺癌;OS:总生存;PORT:术后放疗;“-”:无相关统计结果。
下载: 导出CSV
表 3 804例pⅢA-N2 NSCLC患者Cox模型多因素预后分析结果
Table 3. Multivariate analysis for overall survival of 804 pⅢA-N2 non-small-cell lung cancer patients
影响因素 偏回归系数 偏回归系数标准误 Wald P值 OR值 OR值95%CI 性别 -0.418 0.183 5.196 0.023 0.658 0.460~0.943 年龄 -0.312 0.123 6.423 0.011 1.367 1.073~1.740 吸烟 -0.061 0.180 0.114 0.735 0.941 0.661~1.339 术前T分期 -0.114 0.059 3.719 0.054 1.121 0.998~1.259 术前N分期 -0.141 0.059 5.789 0.016 1.151 1.026~1.292 病理类型 -0.288 0.120 5.774 0.016 1.333 1.054~1.686 化疗周期数 -0.191 0.098 3.816 0.051 0.826 0.681~1.001 PORT -0.283 0.130 4.694 0.030 0.754 0.584~0.973 注:表中,pⅢA-N2:病理分期为ⅢA-N2;NSCLC:非小细胞肺癌;PORT:术后放疗。
下载: 导出CSV
表 4 804例pⅢA-N2 NSCLC患者PORT与生存相关性的单因素分析结果
Table 4. Stratified analysis for survive of 804 pⅢA-N2 non-small-cell lung cancer patients according to postoperative radiotherapy
组别 OS DFS LRFS DMFS 中位值/月 2年/% 5年/% 中位值/月 2年/% 5年/% 中位值/月 2年/% 5年/% 中位值/月 2年/% 5年/% 非PORT组 64.10 80.0 50.8 17.97 42.1 21.5 101.03 71.9 59.0 28.49 54.3 30.6 PORT组 97.31 86.1 60.6 25.76 53.1 36.7 120.31 83.2 73.6 36.83 60.1 42.8 χ2值 5.253 18.397 15.358 6.434 P值 0.022 < 0.001 < 0.001 0.011 注:表中,pⅢA-N2:病理分期为ⅢA-N2;NSCLC:非小细胞肺癌;PORT:术后放疗;OS:总生存;DFS:无病生存;LRFS:无局部区域复发生存;DMFS:无远处转移生存。
下载: 导出CSV
-
[1] Reck M, Heigener DF, Mok T, et al. Management of non-small-cell lung cancer: recent developments[J]. Lancet, 2013, 382(9893):709-719. DOI:10.1016/S0140-6736(13)61502-0. [2] Arriagada R, Dunant A, Pignon JP, et al. Long-term results of the international adjuvant lung cancer trial evaluating adjuvant Cisplatin-based chemotherapy in resected lung cancer[J]. J Clin Oncol, 2010, 28(1):35-42. DOI:10.1200/JCO.2009.23.2272. [3] NSCLC Meta-analyses Collaborative Group, Arriagada R, Auperin A, et al. Adjuvant chemotherapy, with or without postoperative radiotherapy, in operable non-small-cell lung cancer: two meta-analyses of individual patient data[J]. Lancet, 2010, 375(9722):1267-1277. DOI:10.1016/S0140-6736(10)60059-1. [4] Le PC. Role of postoperative radiotherapy in resected non-small cell lung cancer:a reassessment based on new data[J]. Oncologist, 2011, 16(5):672-681. DOI:10.1634/theoncologist. 2010-0150. [5] Winton T, Livingston R, Johnson D, et al. Vinorelbine plus cisplatin vs. observation in resected non-small-cell lung cancer[J]. N Engl J Med, 2005, 352(25):2589-2597. DOI:10.1056/NEJMoa043623. [6] Belkacémi Y, Azria D. New tools in adjuvant breast cancer radiotherapy[J]. Bull Cancer, 2007, 94(4):389-397. DOI:10.1684/bdc.2007.0230. [7] Ramsey S, Tepper JE. Rectal cancer radiotherapy[J]. Cancer J, 2007, 13(3):204-209. DOI:10.1097/PPO.0b013e318074def2. [8] PORT Meta-analysis Trialists Group. Postoperative radiotherapy in non-small-cell lung cancer:systematic review and meta-analysis of individual patient data from nine randomised controlled trials[J]. Lancet, 1998, 352(9124):257-263. DOI:10.1016/S0140-6736(98)06341-7. [9] Lally BE, Zelterman D, Colasanto JM, et al. Postoperative radiotherapy for stage Ⅱ or Ⅲ non-small-cell lung cancer using the surveillance, epidemiology, and end results database[J]. J Clin Oncol, 2006, 24(19):2998-3006. DOI:10.1200/JCO.2005.04.6110. [10] Douillard JY, Rosell R, De Lena M, et al. Adjuvant vinorelbine plus cisplatin versus observation in patients with completely resected stage IB-ⅢA non-small-cell lung cancer (Adjuvant Navelbine International Trialist Association[ANITA]): a randomised controlled trial[J]. Lancet Oncol, 2006, 7(9):719-727. DOI:10.1016/S1470-2045(06)70804-X. [11] Dai H, Hui Z, Ji W, et al. Postoperative radiotherapy for resected pathological stage ⅢA-N2 non-small cell lung cancer: a retrospective study of 221 cases from a single institution[J]. Oncologist, 2011, 16(5):641-650. DOI:10.1634/theoncologist.2010-0343. [12] Perry MC, Kohman LJ, Bonner JA, et al. A phase Ⅲ study of surgical resection and paclitaxel/carboplatin chemotherapy with or without adjuvant radiation therapy for resected stage Ⅲ non-small-cell lung cancer:Cancer and Leukemia Group B 9734[J]. Clin Lung Cancer, 2007, 8(4):268-272. DOI:10.3816/CLC.2007.n.005. [13] Patel SH, Ma Y, Wernicke AG, et al. Evidence supporting contemporary post-operative radiation therapy(PORT) using linear accelerators in N2 lung cancer[J]. Lung Cancer, 2014, 84(2):156-160. DOI:10.1016/j.lungcan.2014.02.016. [14] Billiet C, Decaluwé H, Peeters S, et al. Modern post-operative radiotherapy for stage Ⅲ non-small cell lung cancer may improve local control and survival: a meta-analysis[J]. Radiother Oncol, 2014, 110(1):3-8. DOI:10.1016/j.radonc.2013.08.011. [15] Sawyer TE, Bonner JA, Gould PM, et al. Effectiveness of postoperative irradiation in stage ⅢA non-small cell lung cancer according to regression tree analyses of recurrence risks[J]. Ann Thorac Surg, 1997, 64(5):1402-1407. DOI:10.1016/S0003-4975(97)00908-9. [16] Matsuguma H, Nakahara R, Ishikawa Y, et al. Postoperative radiotherapy for patients with completely resected pathological stage ⅢA-N2 non-small cell lung cancer:focusing on an effect of the number of mediastinal lymph node stations involved[J]. Interact Cardiovasc Thorac Surg, 2008, 7(4):573-577. DOI:10.1510/icvts.2007. 174342. [17] Hui Z, Dai H, Liang J, et al. Selection of proper candidates with resected pathological stage ⅢA-N2 non-small cell lung cancer for postoperative radiotherapy[J]. Thorac Cancer, 2015, 6(3):346-353. DOI:10.1111/1759-7714.12186. [18] McGovern SL, Liao Z, Bucci MK, et al. Is sex associated with the outcome of patients treated with radiation for non-small cell lung cancer?[J]. Cancer, 2009, 115(14):3233-3242. DOI:10.1002/cncr.24361. [19] Vogelius IR, Bentzen SM. A literature-based meta-analysis of clinical risk factors for development of radiation induced pneumonitis[J]. Acta Oncol, 2012, 51(8):975-983. DOI:10.3109/0284186X.2012. 718093. [20] Ruckdeschel JC. Combined modality therapy of non-small cell lung cancer[J]. Semin Oncol, 1997, 24(4):429-439. [21] Robinson LA, Wagner H, Ruckdeschel JC. Treatment of stage ⅢA non-small cell lung cancer[J]. Chest, 2003, 123(1 Suppl):202S-220S. DOI:10.1378/chest.123.1_suppl.2023. [22] Yoshino I, Yoshida S, Miyaoka E, et al. Surgical outcome of stage ⅢA-cN2/pN2 non-small-cell lung cancer patients in Japanese lung cancer registry study in 2004[J]. J Thorac Oncol, 2012, 7(5):850-855. DOI:10.1097/JTO.0b013e31824c945b. [23] Asamura H, Goya T, Koshiishi Y, et al. A Japanese Lung Cancer Registry study: prognosis of 13, 010 resected lung cancers[J]. J Thorac Oncol, 2008, 3(1):46-52. DOI:10.1097/JTO.0b013e31815 e8577. -

 点击查看大图
点击查看大图

计量
- 文章访问数: 3432
- HTML全文浏览量: 2516
- PDF下载量: 2