


 下载:
下载:


-
海绵状血管瘤是一种良性血管畸形,并不是真正的肿瘤。骨海绵状血管瘤好发于脊柱及颅骨,在脊柱中多发生于椎体,约占脊柱血管瘤的5%~12%,占脊柱肿瘤的4%[1-4]。椎体海绵状血管瘤可侵犯周围组织,延伸到硬膜内、外腔,形成椎管内硬膜内、外海绵状血管瘤[5]。MRI通常表现为T1WI低信号或等信号,T2WI高信号或等信号,增强扫描时明显强化[4, 6]。由于海绵状血管瘤血管腔内有血栓的钙化或机化,CT扫描表现为瘤体内点片状钙化灶及增厚的骨小梁,此为海绵状血管瘤特征性指标,对海绵状血管瘤的诊断具有很高的灵敏度。18F-FDG PET显像提示海绵状血管瘤是一种18F-FDG低摄取的良性肿瘤[7]。有研究报道,海绵状血管瘤18F-FDG PET的SUVmax<2.5[8]。
-
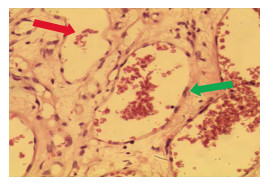
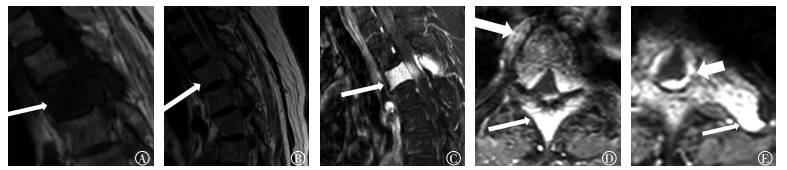
患者女性,69岁,因“双下肢乏力4月余,加重伴疼痛、活动受限一周”入院,无发热等不适。既往无慢性病、肿瘤及传染病病史。体格检查:T3~T4椎体明显压痛、叩击痛,T4椎体平面以下感觉减退,双侧髂腰肌、股四头肌、股三头肌肌力及足背伸背屈、右侧踇背伸背屈、右侧踇跖屈肌肌力低于4级,双侧踇跖背伸肌力下降,约为3级。双下肢腱反射亢进,双侧髌阵挛(-),双侧踝阵挛(-),双侧巴彬斯基征(+)。肛周感觉减退,肛门松弛,收缩力差,可容二指。双上肢肌张力及腱反射正常。血清学检查:白细胞为11.15×109/L(正常值为3.5×109/L~9.5×109/L),中性粒细胞百分数为91.1%(正常值为40%~75%);超敏C反应蛋白为11.86 mg/L(正常值为<3.3 mg/L),红细胞沉降率为63 mm/h(正常值为0~15 mm/h)。肿瘤标志物检查:糖类抗原CA125、细胞角蛋白19片段、甲胎蛋白、癌胚抗原、生长激素、胃泌素释放肽前体、神经原特异烯醇化酶、糖类抗原CA72-4、糖类抗原CA15-3、糖类抗原CA19-9均为阴性。影像学检查,胸椎MRI示T3椎体及附件呈T1、T2稍长或等信号,增强扫描后强化明显,未见骨质破坏,相应水平椎管内硬膜下见团块状占位病变,信号及强化程度与椎体病变相似,椎管变窄,考虑为恶性肿瘤(图 1)。18F-FDG PET/CT检查示:T3椎体及附件密度不均匀,内部骨质结构紊乱,似有分隔,并见多发粗大点状高密度影,相应水平椎体后方见片状稍高密度影致椎管变窄,18F-FDG代谢与其余椎体一致,SUVmax为2.4,考虑为良性病变,海绵状血管瘤可能性大(图 2)。因患者出现明显的脊髓损伤症状,T5椎体平面以下不全瘫痪,且呈进行性加重,已有手术指征,患者行后路T3椎体肿瘤探查切除+脊髓减压钛笼支撑植骨融合钉棒系统内固定术。术后CT示:T1~T5椎体呈术后改变,T3椎体缺如,其前正中位置可见网状致密影,周围见包裹性积液(图 3)。病理检查结果示:T3椎体病灶内可见异常血管聚集成丛状,血管腔内有大量红细胞,符合海绵状血管瘤(图 4)。

图 1 患者女性,69岁,胸椎MRI图

图 2 患者女性,69岁,胸椎18F-FDG PET/CT显像图

图 3 患者女性,69岁,术后胸椎CT显像图

图 4 患者女性,69岁,胸椎海绵状血管瘤病理图(苏木精-伊红染色,×20)
-
本例海绵状血管瘤累及椎体、椎体附件、周围组织并延伸到椎管内侵及硬脊膜,病变范围广泛,引起脊髓压迫症状,MRI增强扫描后明显强化,因此误诊为恶性肿瘤。转移瘤、淋巴瘤、神经源性肿瘤、结核等病变也可以出现相似的MRI表现,因此需要进一步鉴别。椎体转移瘤有原发灶、椎体骨质破坏及周围软组织肿块,MRI表现为T1WI稍低或等信号,T2WI稍高或等信号,强化程度较海绵状血管瘤弱,很少像海绵状血管瘤呈均匀一致性强化,CT可见低密度的骨质破坏区及周围软组织肿块,增强扫描后呈明显不均匀强化[9],18F-FDG PET同时显示原发灶及转移瘤,转移瘤与原发灶的代谢基本一致。淋巴瘤可局限于椎管内,也可通过椎间孔向椎旁生长,破坏邻近椎体、椎板和肋骨,形成巨大软组织肿块,MRI表现为T1WI低信号,T2WI呈稍高或等信号,增强扫描后可呈中度-显著强化,CT对软组织肿块的显示不如MRI,但有利于骨质破坏及病灶内死骨的显示[10],淋巴瘤的18F-FDG PET代谢明显高于海绵状血管瘤,并同时显示椎体外远处病变,有助于鉴别[11]。Yunoki等[5]报道了一例哑铃状的海绵状血管瘤,哑铃状脊柱肿瘤伴椎间孔扩大通常是神经源性肿瘤,但海绵状血管瘤椎间孔一般不扩大,虽然哑铃状的海绵状血管瘤极其罕见,但也应注意鉴别。此外,海绵状血管瘤还应与结核鉴别,结核在椎体破坏的同时,容易累及椎间盘[12],本例MRI平扫及增强扫描椎间盘未见明确受累,尽管白细胞稍增高,但病灶区皮肤温度不高,并无全身的感染症状,患者无结核病史,MRI表现结合病史不难排除结核,但结核具有渗出、增生和坏死3种基本病理改变,也会出现不同的影像学表现[11],因此鉴别比较困难,应结合实验室检查。
18F-FDG PET/CT显像低代谢结合CT特异性的点状钙化灶对本例海绵状血管瘤的术前诊断并不困难。对于海绵状血管瘤与恶性肿瘤的鉴别,PET/CT具有灵敏度高的优势,既可以观察到CT特征性的点状钙化灶,又可以结合全身代谢情况与其他疾病进行鉴别。尽管MRI对软组织的分辨率较高,对周围软组织病变及椎管内病变显示清晰,但对海绵状血管瘤的诊断缺乏特异性,容易误诊。因此,当MRI显示病灶累及椎体、椎体附件、椎管及周围组织且病灶明显强化,又没有明确的椎体破坏,怀疑恶性肿瘤时,应结合PET/CT对诸如海绵状血管瘤等良性病变进行鉴别诊断。
MRI误诊的椎体海绵状血管瘤18F-FDG PET/CT显像一例
18F-FDG PET/CT findings of a thoracic vertebral cavernous hemangioma: a case of MRI misdiagnosis
-
摘要: 笔者报道了一例双下肢乏力4月余,加重伴疼痛、活动受限一周的病例。MRI显示病灶累及胸3椎体、椎体附件和周围组织,并延伸到椎管内硬脊膜,增强后病变明显强化,MRI因病变范围广且增强后明显强化,考虑为恶性肿瘤。而18F-FDG PET低代谢结合CT点状、栅栏状钙化灶和椎体骨质无破坏,考虑为海绵状血管瘤;且术后病理因病灶内见异常血管聚集成丛状,血管腔内有大量红细胞,诊断为海绵状血管瘤。文献复习加深了对椎体海绵状血管瘤的认识,其可累及椎体、椎体附件,甚至延伸到椎管内和(或)周围组织。海绵状血管瘤是一种血管畸形,MRI增强后呈明显强化,但是PET显像则呈低代谢。当MRI显示病变范围广伴明显强化,而椎体无骨质破坏,怀疑恶性肿瘤时,应结合PET/CT对诸如海绵状血管瘤等良性病变进行鉴别诊断。Abstract: We report a 69-year-old female with nearly 4 months of bilateral lower limb weakness and about 1 week of limited activity and pain. MRI of the thoracolumbar spine revealed that the lesion was mainly on the vertebral body and the corresponding intraspinal, epidural, and paravertebral soft tissues. In the Gd-enhanced images, the lesion was highly apparent and was diagnosed as a malignant tumor. However, the punctate bone density was increased upon PET/CT and 18F-FDG uptake was low. Furthermore, PET/CT imaging showed a cavernous hemangioma, and this was confirmed by histological examination of the tumor. The understanding of the cavernous hemangioma was deepened by literature review. A cavernous hemangioma can involve the vertebral body and vertebral appendages, and can even extend into the spinal canal and surrounding tissues. Cavernous hemangioma is a benign vascular malformation. The Gd-enhanced imaging is a valuable enhancement tool. Moreover, PET showed low 18F-FDG uptake. When the MRI lesions are widespread and obvious, malignancy should not be ruled out. Furthermore, PET/CT should be used for the differential diagnosis of benign lesions, such as cavernous hemangioma.
-
Key words:
-
[1] Cha JG, Yoo JH, Kim HK, et al. PET/CT and MRI of intra-osseous haemangioma of the tibia[J/OL]. Br J Radiol, 2012, 85(1012): e94-e98[2017-03-05]. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3486666/pdf/bjr-85-e094.pdf. DOI: 10.1259/bjr/35251836. [2] Matsumoto Y, Takahashi Y, Haraguchi A, et al. Intraosseous hemangioma arising in the clavicle[J]. Skeletal Radiol, 2014, 43(1):89-93. DOI:10.1007/s00256-013-1715-3. [3] Khalatbari MR, Abbassioun K, Amirjmshidi A. Solitary spinal epidural cavernous angioma:report of nine surgically treated cases and review of the literature[J]. Eur Spine J, 2013, 22(3):542-547. DOI:10.1007/s00586-012-2526-2. [4] Tan S, Kurt A, Okutan O, et al. CT findings of a thoracic vertebral hemangioma presenting with acute neurological symptoms[J].Turk Neurosurg, 2011, 21(1):113-115. [5] Yunoki M, Suzuki K, Uneda A, et al. A case of dumbbell-shaped epidural cavernous angioma in the lumbar spine[J]. Surg Neurol Int, 2015, 6(Suppl 10):S309-312.DOI:10.4103/2152-7806.159378. [6] Ciurea ME, Bondari S, Stoica LE, et al. Role of MRI in the diagnosis and evaluation of cavernous hemangioma of the arm[J]. J Med Life, 2014, 7(1):46-50. [7] Ko SW, Park JG. Cavernous hemangioma of the ilium mimicking aggressive malignant bone tumor with increased activity on 18F-FDG PET/CT[J]. Korean J Radiol, 2013, 14(2):294-298. DOI:10.3348/kjr.2013.14.2.294. [8] Shin JH, Lee HK, Rhim SC, et al. Spinal epidural cavernous hemangioma:MR findings[J]. J Comput Assist Tomogr, 2001, 25(2):257-261. DOI:10.1097/00004728-200103000-00019. [9] 赵鑫福.椎管内硬膜外海绵状血管瘤MRI表现[J].中国实用医药, 2015, 10(3):118-119. DOI:10.14163/j.cnki.11-5547/r.2015.03.080.
Zhao XF. MRI findings of epidural cavernous hemangioma in the spinal canal[J]. China Prac Med, 2015, 10(3):118-119. doi: 10.14163/j.cnki.11-5547/r.2015.03.080[10] Yang L, Liu Z, Su L, et al. Primary bone lymphoplasmacytic lymphoma presenting with spinal cord compression:a case report[J]. Turk J Hematol, 2013, 30(4):409-412. DOI:10.4274/Tjh.2012. 0072. [11] 金民山, 张俊, 姜一逸. 18F-PET/CT在不明原发灶肿瘤中的临床应用价值[J].国际放射医学核医学杂志, 2017, 41(2):94-97. DOI:10.3760/cma.jssn.1673-4114.2017.02.003.
Jin MS, Zhang J, Jiang YY. Clinical value of 18F-FDG PET/CT in cancer of unknown primary[J]. Int J Radiat Med Nucl Med, 2017, 41(2):94-97. doi: 10.3760/cma.jssn.1673-4114.2017.02.003[12] Park HS, Song YJ. Multiple tuberculoma involving the brain and spinal cord in a patient with miliary pulmonary tuberculosis[J]. J Korean Neurosurg Soc, 2008, 44(1):36-39. DOI:10.3340/jkns.2008.44.1.36. -

 点击查看大图
点击查看大图
图(4)
计量
- 文章访问数: 3894
- HTML全文浏览量: 2680
- PDF下载量: 6