


-
宫颈癌是女性常见的恶性肿瘤之一,近十几年来我国宫颈癌的发病率和病死率在逐年升高[1]。放疗是治疗宫颈癌的主要手段之一,各期均可选择放疗。对于宫颈癌术后具有高危复发因素的患者,行术后盆腔放疗可以降低复发风险和延长无进展生存时间[2]。宫颈癌术后盆腔调强放疗(intensity-modulated radiotherapy,IMRT)是目前常用的外照射放疗技术,在疗效和不良反应方面优于常规放疗和三维适形放疗[3-4]。
容积旋转调强放疗(volumetric modulated arc radiotherapy,VMAT)是一种新的调强方法,最早由Yu[5]在1995年提出,Otto[6]于2008年对其算法进行改进,并开始用于临床。与IMRT相比,VMAT用于宫颈癌术后盆腔放疗在剂量学上是否更具优势?我们比较了不同弧度的VMAT计划与5野IMRT(5-field IMRT,5F-IMRT)计划之间的剂量学差异,现报道如下。
-
回顾性分析2015年5月至2016年12月我院放疗科的10例宫颈癌患者术后盆腔外照射的5F-IMRT计划资料。患者年龄34~61岁,中位年龄48岁;按2009年国际妇产科学联盟(FIGO)分期[7]均为Ⅰb~Ⅱa期;手术方式均为全子宫+双侧附件切除术+盆腔淋巴结清扫术,术后有复发高危因素。所有患者均于检查前签署了放疗知情同意书。
-
患者取仰卧位,真空垫或体膜固定体位,CT模拟定位机(SOMATOM,德国西门子)行增强扫描,扫描层厚为5 mm,层间距为5 mm,层数70~80,扫描范围为腰3椎体上缘至坐骨结节下2 cm。然后将CT扫描图像传入Eclipse治疗计划系统(美国瓦里安)。
-
在Eclipse治疗计划系统上进行靶区勾画,临床靶区包括阴道残端、部分阴道及盆腔淋巴结引流区(部分髂总、髂外、髂内、宫旁、闭孔、骶前)。计划靶区(plan target volume,PTV)为临床靶区各个方向外放0.5~1.0 cm。同时勾画小肠(包括结肠)、直肠、膀胱和股骨头等危及器官。
-
靶区处方剂量为2 Gy/次,共25次,总剂量为50 Gy。要求至少95%的PTV达到处方剂量,PTV外不出现≥110%的剂量热点。照射野危及器官限量:小肠V40(小肠受照40 Gy的体积百分比)≤50%;直肠和膀胱V50(直肠和膀胱受照50 Gy的体积百分比)≤50%;股骨头V50(股骨头受照50 Gy的体积百分比)≤5%。
-
在Eclipse治疗计划系统上对10例宫颈癌术后患者设计单弧VMAT和双弧VMAT放疗计划。单弧VMAT:顺时针179°~181°;双弧VMAT:顺时针179°~181°,逆时针181°~179°。5F-IMRT机架角度数为70°、125°、180°、235°、290°。均采用6 MV-X线照射。
-
PTV剂量学参数包括最大剂量(Dmax)、平均剂量(Dmean)、最小剂量(Dmin)、适形度指数(conformity index,CI)、均匀性指数(homogeneity index,HI)和加速器跳数(monitor unit,MU)。CI计算公式为:CI=(TVRI /TV)×(TVRI /VRI),TVRI为处方剂量包括的靶区体积,TV为靶体积,VRI为处方剂量包括的总体积,CI值在0到1之间,CI值越大表明靶区适形度越高。HI计算公式为:HI=(D2%-D98%)/D50%,D2%为靶区最大近似剂量,D98%为靶区最小近似剂量,D50%近似靶区平均剂量,HI值越小说明靶区剂量分布越均匀。危及器官剂量学参数包括:最大剂量(Dmax)和平均剂量(Dmean),以及接受10、20、30、40、50 Gy照射剂量的体积占总体积的百分比。
-
采用SPSS22.0统计学软件进行分析,计量资料采用x± s表示,数据符合正态分布且方差齐。组间比较采用单因素方差分析检验,组间两两比较采用LSD检验。P < 0.05表示差异有统计学意义。
-
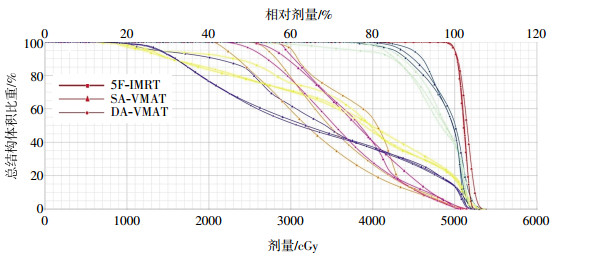
5F-IMRT、单弧VMAT和双弧VMAT 3种放疗计划均能满足靶区处方剂量的要求(图 1)。3种放疗计划的Dmax、Dmean、CI和HI之间的差异有统计学意义(F=24.102、13.710、5.919、11.045,均P < 0.05)。3种放疗计划的Dmin的差异无统计学意义(F=3.323,P>0.05)。单弧VMAT和双弧VMAT计划的MU明显少于5F-IMRT计划,差异有统计学意义(F=295.138,P < 0.05)(表 1)。

图 1 5F-IMRT、单弧VMAT和双弧VMAT 3种放疗技术靶区的剂量体积直方图
Figure 1. The dose-volume histogram of targets of 5F-IMRT, SA-VMAT and DA-VMAT plans
放疗技术 Dmax /cGy Dmin /cGy Dmean /cGy CI HI MU 5F-IMRT 5275.14±31.11 4601.58±106.86 5096.05±8.52 0.88±0.04 0.13±0.03 1315.70±139.77 单弧VMAT 5468.76±102.01 4504.43±113.37 5149.94±38.26 0.80±0.083 0.19±0.04 0455.00±57.40 双弧VMAT 5328.61±32.72 4596.35±51.77 5107.91±14.77 0.87±0.04 0.14±0.01 0444.70±50.73 F值 24.102 3.323 13.710 5.919 11.045 295.138 P值 0.000 0.051 0.000 0.007 0.000 0.000 注:表中,5F-IMRT:5野调强放疗;VMAT:容积旋转调强放疗;Dmax:最大剂量;Dmin:最小剂量;Dmean:平均剂量;CI:适形度指数;HI:均匀性指数;MU:加速器跳数。 表 1 5F-IMRT、单弧VMAT和双弧VMAT 3种放疗技术靶区剂量学参数比较(x± s)
Table 1. Comparison of dosimetric parameters for targets in 5F-IMRT, SA-VMAT and DA-VMAT plans(x± s)
-
5F-IMRT、单弧VMAT和双弧VMAT 3种放疗计划均能满足危及器官的剂量要求。由表 2可知,对于小肠的参数Dmax,5F-IMRT和双弧VMAT计划优于单弧VMAT,差异有统计学意义(F=16.069,P < 0.05);3种计划的Dmean差异无统计学意义(F=0.074,P>0.05)。对于直肠的参数Dmax,5F-IMRT和双弧VMAT计划优于单弧VMAT,差异有统计学意义(F=7.521,P < 0.05);3种计划的Dmean差异无统计学意义(F=2.184,P>0.05)。对于膀胱的参数Dmax,5F-IMRT和双弧VMAT计划优于单弧VMAT,差异有统计学意义(F=13.966,P < 0.05);对于参数Dmean,5F-IMRT优于单弧VMAT和双弧VMAT,差异有统计学意义(F=10.021,P < 0.05)。对于左、右股骨头,3种计划的Dmax差异无统计学意义(F=0.194、0.341,均P>0.05);对于参数Dmean,单弧VMAT和双弧VMAT优于5F-IMRT,差异有统计学意义(F=12.149、8.712,均P < 0.05)。
危及器官 剂量学参数 5F-IMRT 单弧VMAT 双弧VMAT F值 P值 小肠 Dmax 5168.85±44.69 5358.57±106.28 5228.83±65.29 16.069 0.000 Dmean 2884.12±436.96 2954.05±387.78 2907.72±411.52 0.074 0.929 直肠 Dmax 5200.55±38.97 5301.88±86.25 5233.60±41.15 7.521 0.003 Dmean 4635.31±177.42 4772.79±151.70 4743.27±132.06 2.184 0.132 膀胱 Dmax 5217.79±37.58 5393.39±125.03 5257.88±33.84 13.966 0.000 Dmean 4304.59±210.11 4627.95±119.32 4545.79±161.80 10.021 0.001 左股骨头 Dmax 4632.40±234.83 4557.97±269.56 4589.41±297.05 0.194 0.825 Dmean 3296.81±156.96 2785.82±292.91 2796.42±316.43 12.149 0.000 右股骨头 Dmax 4807.94±131.72 4834.58±266.90 4763.11±161.94 0.341 0.714 Dmean 3439.86±178.90 3023.92±463.04 2867.44±234.52 8.712 0.001 注:表中,5F-IMRT:5野调强放疗;VMAT:容积旋转调强放疗;Dmax:最大剂量;Dmean:平均剂量。 表 2 5F-IMRT、单弧VMAT和双弧VMAT 3种放疗技术危及器官剂量学参数比较[(x± s)/cGy]
Table 2. Comparison of dosimetric parameters for organs at risk in 5F-IMRT, SA-VMAT and DA-VMAT plans[(x± s)/cGy]
-
由表 3可知,5F-IMRT、单弧VMAT和双弧VMAT 3种放疗计划在小肠和直肠V10、V20、V30、V40、V50中的差异均无统计学意义(F=0.010~1.731,均P>0.05)。3种计划在膀胱V50中的差异无统计学意义(F=2.061,P>0.05);在膀胱V20、V30、V40中,5F-IMRT优于单弧VMAT和双弧VMAT,差异有统计学意义(F=5.142、20.095、7.387,均P < 0.05)。3种计划在左股骨头V40中的差异无统计学意义(F=2.650,P>0.05);对于左股骨头参数V20和V30,单弧和双弧VMAT优于5F-IMRT,差异有统计学意义(F=3.717、16.040,均P < 0.05)。3种计划在右股骨头V10、V20中的差异无统计学意义(F=2.043、2.984,均P>0.05);对于右股骨头参数V30和V40,单弧和双弧VMAT优于5F-IMRT,差异有统计学意义(F=10.873、7.791,均P < 0.05)。
危及器官 剂量学参数 5F-IMRT 单弧VMAT 双弧VMAT F值 P值 小肠 V10 093.27±7.31 092.87±7.12 092.86±7.24 0.010 0.990 V20 071.34±11.44 070.62±10.16 068.36±10.30 0.213 0.809 V30 041.14±13.54 044.71±12.06 043.96±11.11 0.235 0.792 V40 024.85±12.16 028.53±11.63 026.98±12.49 0.233 0.793 V50 006.07±3.27 009.43±4.67 007.47±4.09 1.731 0.196 直肠 V10 100.00±0.00 100.00±0.00 100.00±0.00 - - V20 100.00±0.00 100.00±0.00 100.00±0.00 - - V30 099.29±1.62 099.89±0.34 100.00±0.00 1.594 0.222 V40 089.62±11.70 095.57±5.63 095.20±5.38 1.686 0.204 V50 019.85±8.68 029.43±16.39 024.55±10.78 1.495 0.242 膀胱 V10 100.00±0.00 100.00±0.00 100.00±0.00 - - V20 098.30±2.37 100.00±0.00 100.00±0.00 5.142 0.013 V30 090.73±5.54 099.10±1.57 099.36±1.66 20.095 0 V40 072.84±10.82 088.29±4.64 083.58±10.78 7.387 0.003 V50 020.35±7.51 027.76±10.98 021.10±8.07 2.061 0.147 左股骨头 V10 100.00±0.00 100.00±0.00 100.00±0.00 - - V20 099.45±1.34 089.84±10.67 089.47±11.93 3.717 0.038 V30 067.56±13.65 034.29±15.33 034.46±16.29 16.040 0.000 V40 010.53±5.82 004.67±6.23 005.64±6.28 2.650 0.089 V50 100.00±0.00 100.00±0.00 100.00±0.00 - - 右股骨头 V10 100.00±0.00 099.87±.27 100.00±0.00 2.043 0.149 V20 100.00±0.00 089.13±16.28 091.22±8.33 2.984 0.067 V30 074.68±14.70 050.65±23.24 039.19±12.21 10.873 0.000 V40 020.15±9.92 013.33±8.49 006.39±3.44 7.791 0.002 V50 100.00±0.00 100.00±0.00 100.00±0.00 - - 注:表中,Vn:小肠受照n Gy的体积百分比,n=10、20、30、40、50;5F-IMRT:5野调强放疗;VMAT:容积旋转调强放疗;-:无数值。 表 3 5F-IMRT、单弧VMAT和双弧VMAT 3种放疗技术危及器官剂量学参数比较[(x± s)/%]
Table 3. Comparison of dosimetric parameters for organs at risk in 5F-IMRT, SA-VMAT and DA-VMAT plans[(x± s)/%]
-
宫颈癌术后盆腔IMRT是目前常用的外照射放疗技术,在疗效和不良反应方面优于常规放疗和三维适形放疗,但其治疗时间相对较长。有文献报道,延长治疗时间可以修复肿瘤细胞DNA、增加肿瘤的增殖概率,导致肿瘤控制概率降低[8]。体外照射宫颈癌细胞,随着照射时间延长,肿瘤细胞的存活率会逐步增高[9]。MU减少,即减少了散射,正常组织的散射量也减少,理论上降低了第二原发肿瘤的发生率[10]。
VMAT技术是一种新的调强方式,可以通过调整多叶光栅的形状和输出剂量率配合机架的旋转,在较短的时间内对靶区进行剂量强度调制,提高了靶区的生物效应和治疗效率[11]。
宫颈癌术后外照射放疗靶区形状不规则,变化较大,其周围又有众多危及器官;另外,患者在治疗时需要憋小便,治疗时间过长增加了患者不适感,增加了不自主运动,可能引起摆位误差。能否利用VMAT技术达到IMRT相同的剂量学要求,同时减少MU和缩短治疗时间?宫颈癌术后外照射是否可以应用VMAT技术进行,不仅能达到IMRT的剂量学要求,同时又能减少MU和治疗时间?不少学者针对以上问题进行了研究,如杨波等[12]对比了宫颈癌术后固定野调强放疗(FF-IMRT)和容积调强弧形治疗(VIMAT)计划的剂量学差异,FF-IMRT计划采用9野均分共面照射,VIMAT计划采用2个全弧照射;与9野IMRT比较,VIMAT计划PTV的95%覆盖度增加(t=9.84,P=0.000)、最大剂量(Dmax)降低(t=-3.51,P=0.005)、CI变差(t=5.93,P=0.000);正常组织保护方面VIMAT计划略好于FF-IMRT;与9野IMRT比较,VIMAT计划MU减少57%(t=-40.54,P=0.000)。杨国姿等[13]比较了双弧VMAT(RapidArc)与7野固定野动态IMRT两种宫颈癌术后放疗的剂量学参数及急性不良反应发生率,发现RapidArc靶区剂量适形度较高(t=3.13,P < 0.05),但均匀性略低(t=-4.25,P < 0.05);RapidArc计划股骨头V20和V30均低(t=2.56、2.34,P < 0.05);RapidArc计划MU减少52.1%,治疗时间缩短46.8%;两组急性不良反应发生率差异无统计学意义。可见双弧VMAT计划达到了或略优于IMRT计划的要求,并且减少了MU并缩短了治疗时间。在宫颈癌根治性放疗中取得了同样的研究结果[14-15]。
临床上治疗患者是为了达到最大的增益比,理论上单弧VMAT或减少IMRT的野数势必也能降低MU和缩短治疗时间,这样双弧VMAT计划是否还能具有优势?因此,我们分析了单弧VMAT、双弧VMAT和5F-IMRT计划之间的剂量学差异。研究结果显示,单弧VMAT、双弧VMAT和5F-IMRT计划均能满足靶区处方剂量的要求,在靶区Dmax、Dmean、CI和HI上,双弧VMAT与5F-IMRT放疗计划相当,单弧VMAT计划最差。单弧VMAT和双弧VMAT计划的MU明显少于5F-IMRT计划。在危及器官保护方面,从小肠、直肠和膀胱Dmax参数来看,双弧VMAT与5F-IMRT计划相当,单弧VMAT计划最差。膀胱V20、V30和V40,5F-IMRT优于单弧VMAT和双弧VMAT,差异有统计学意义。对于左股骨头参数V20和V30,单弧和双弧VMAT优于5F-IMRT,差异有统计学意义。对于右股骨头参数V30和V40,单弧和双弧VMAT优于5F-IMRT,差异有统计学意义。
此外,有研究发现,双弧VMAT计划不仅能更好地保护照射野里的正常组织,对周边组织的辐射剂量也较小[16]。增加IMRT的野数,是否能得到好的剂量学的优势?Sharfo等[17]研究发现宫颈癌12野和20野IMRT计划质量优于单弧和双弧VMAT计划,但是治疗时间长。
在实际工作中,对于个体患者来说,最佳治疗技术的选择取决于治疗计划质量和治疗时间之间的权衡。综上所述,宫颈癌术后放疗,双弧VMAT计划在靶区剂量学参数上与5F-IMRT计划相当,单弧VMAT计划较差。在危及器官保护方面,3种计划各有优势,但VMAT计划MU明显减少,可以提高治疗效率,值得临床进一步研究。
宫颈癌术后容积旋转调强放疗与5野调强放疗计划的剂量学比较
Dosimetric comparison between volumetric modulated arc radiotherapy and five fields intensity-modulated radiation therapy for postoperative cervical carcinoma
-
摘要:
目的比较宫颈癌术后容积旋转调强放疗(VMAT)与5野调强放疗(5F-IMRT)计划的剂量学差异,并在危及器官保护方面进行分析。 方法选择10例宫颈癌术后放疗的5F-IMRT计划,按相同的剂量限制对每例患者行单弧VMAT和双弧VMAT计划设计,比较3种计划的靶区剂量、适形度指数、均匀性指数、危及器官剂量及加速器跳数。组间比较采用单因素方差分析检验,组间两两比较采用LSD检验。 结果单弧VMAT和双弧VMAT均能满足靶区处方剂量的要求,在靶区最大剂量、平均剂量、适形度指数和均匀性指数上,双弧VMAT与5F-IMRT计划相当,单弧VMAT计划最差,差异有统计学意义(F=24.102、13.710、5.919、11.045,均P < 0.05);靶区最小剂量比较,3种计划差异无统计学意义(F=3.323,P>0.05)。单弧VMAT和双弧VMAT计划的加速器跳数明显少于5F-IMRT计划,差异有统计学意义(F=295.138,P < 0.05)。对于小肠、直肠和膀胱的参数最大剂量,双弧VMAT与5F-IMRT计划相当,单弧VMAT计划最差,差异有统计学意义(F=16.069、7.521、13.966,均P < 0.05)。对于膀胱的参数V20、V30和V40(V表示受照剂量体积百分比),5F-IMRT优于单弧VMAT和双弧VMAT,差异有统计学意义(F=5.142、20.095、7.387,均P < 0.05)。对于左股骨头参数V20和V30,单弧和双弧VMAT优于5F-IMRT,差异有统计学意义(F=3.717、16.040,均P < 0.05)。对于右股骨头参数V30和V40,单弧和双弧VMAT优于5F-IMRT,差异有统计学意义(F=10.873、7.791,均P < 0.05)。 结论宫颈癌术后放疗,双弧VMAT计划在靶区剂量学参数上与5F-IMRT计划相当,单弧VMAT计划较差。在危及器官保护方面,3种计划各有优势,但VMAT计划的加速器跳数明显减少,可以提高治疗效率,值得进一步研究。 Abstract:ObjectiveTo determine the dosimetric differences between volumetric modulated arc radiotherapy(VMAT) an five fields intensity-modulated radiation therapy(5F-IMRT) for postoperative cervical cancer. MethodsTen patients with postoperative cervical carcinoma were enrolled in this study. Single arc VMAT, double arc VMAT, and 5F-IMRT plans were generated for these patients. Dose of target, conformal index (CI), homogeneity index (HI), organs at risk and monitor units (MU) were analyzed. The measurement data were analyzed by single factor analysis of variance, and an LSD test was performed in both two groups. ResultsSingle arc and double arc VMAT plans both satisfied the clinical dosimetriy requirements. No significant difference was observed between the VMAT and 5F-IMRT plans with respect to the maximum dose(Dmax) of the target, mean dose(Dmean), CI, and HI. Compared with these plans, the single arc VMAT was weaker and significantly different with respect to the above-mentioned variables (F=24.102, 13.710, 5.919, 11.045, all P < 0.05). There is no significant difference between the 3 plans of the minimum dose of the target (F=3.323, P>0.05). The MU values o f the single arc and double arc VMAT plans were significantly lower than that of 5F-IMRT(F=295.138, P>0.05). Meanwhile, significant difference was observed between the Dmax values of the small intestine, rectum, and bladder for double arc VMAT plan, single arc VMAT plan and those of the 5F-IMRT plan(F=16.069, 7.521, 13.966, all P < 0.05). The bladder V20, V30 and V40 for 5F-IMRT were better than those of the single arc and double arc VMAT, and the differences were significant(F=5.142, 20.095, 7.387, all P < 0.05). The left femoral head V20 and V30 for single arc and double arc VMAT plan was superior to that of 5F-IMRT, and the differences were statistically significant (F=3.717, 16.040, both P < 0.05). The right femoral head V30 and V40 for single arc and double arc VMAT plan was superior to that of 5F-IMRT, and the differences were statistically significant (F=10.873, 7.791, both P < 0.05). ConclusionsCompared with 5F-IMRT, the double arc VMAT achieved equal dosimetric parameters with fewer MU. In terms of organ at risk protection, the three plans have their own advantages, but the MU of the VMAT plan is significantly reduced, which can improve the treatment efficiency and worth further study. -
图 1 5F-IMRT、单弧VMAT和双弧VMAT 3种放疗技术靶区的剂量体积直方图
Figure 1. The dose-volume histogram of targets of 5F-IMRT, SA-VMAT and DA-VMAT plans
表 1 5F-IMRT、单弧VMAT和双弧VMAT 3种放疗技术靶区剂量学参数比较(x± s)
Table 1. Comparison of dosimetric parameters for targets in 5F-IMRT, SA-VMAT and DA-VMAT plans(x± s)
放疗技术 Dmax /cGy Dmin /cGy Dmean /cGy CI HI MU 5F-IMRT 5275.14±31.11 4601.58±106.86 5096.05±8.52 0.88±0.04 0.13±0.03 1315.70±139.77 单弧VMAT 5468.76±102.01 4504.43±113.37 5149.94±38.26 0.80±0.083 0.19±0.04 0455.00±57.40 双弧VMAT 5328.61±32.72 4596.35±51.77 5107.91±14.77 0.87±0.04 0.14±0.01 0444.70±50.73 F值 24.102 3.323 13.710 5.919 11.045 295.138 P值 0.000 0.051 0.000 0.007 0.000 0.000 注:表中,5F-IMRT:5野调强放疗;VMAT:容积旋转调强放疗;Dmax:最大剂量;Dmin:最小剂量;Dmean:平均剂量;CI:适形度指数;HI:均匀性指数;MU:加速器跳数。  下载: 导出CSV
下载: 导出CSV
表 2 5F-IMRT、单弧VMAT和双弧VMAT 3种放疗技术危及器官剂量学参数比较[(x± s)/cGy]
Table 2. Comparison of dosimetric parameters for organs at risk in 5F-IMRT, SA-VMAT and DA-VMAT plans[(x± s)/cGy]
危及器官 剂量学参数 5F-IMRT 单弧VMAT 双弧VMAT F值 P值 小肠 Dmax 5168.85±44.69 5358.57±106.28 5228.83±65.29 16.069 0.000 Dmean 2884.12±436.96 2954.05±387.78 2907.72±411.52 0.074 0.929 直肠 Dmax 5200.55±38.97 5301.88±86.25 5233.60±41.15 7.521 0.003 Dmean 4635.31±177.42 4772.79±151.70 4743.27±132.06 2.184 0.132 膀胱 Dmax 5217.79±37.58 5393.39±125.03 5257.88±33.84 13.966 0.000 Dmean 4304.59±210.11 4627.95±119.32 4545.79±161.80 10.021 0.001 左股骨头 Dmax 4632.40±234.83 4557.97±269.56 4589.41±297.05 0.194 0.825 Dmean 3296.81±156.96 2785.82±292.91 2796.42±316.43 12.149 0.000 右股骨头 Dmax 4807.94±131.72 4834.58±266.90 4763.11±161.94 0.341 0.714 Dmean 3439.86±178.90 3023.92±463.04 2867.44±234.52 8.712 0.001 注:表中,5F-IMRT:5野调强放疗;VMAT:容积旋转调强放疗;Dmax:最大剂量;Dmean:平均剂量。
下载: 导出CSV
表 3 5F-IMRT、单弧VMAT和双弧VMAT 3种放疗技术危及器官剂量学参数比较[(x± s)/%]
Table 3. Comparison of dosimetric parameters for organs at risk in 5F-IMRT, SA-VMAT and DA-VMAT plans[(x± s)/%]
危及器官 剂量学参数 5F-IMRT 单弧VMAT 双弧VMAT F值 P值 小肠 V10 093.27±7.31 092.87±7.12 092.86±7.24 0.010 0.990 V20 071.34±11.44 070.62±10.16 068.36±10.30 0.213 0.809 V30 041.14±13.54 044.71±12.06 043.96±11.11 0.235 0.792 V40 024.85±12.16 028.53±11.63 026.98±12.49 0.233 0.793 V50 006.07±3.27 009.43±4.67 007.47±4.09 1.731 0.196 直肠 V10 100.00±0.00 100.00±0.00 100.00±0.00 - - V20 100.00±0.00 100.00±0.00 100.00±0.00 - - V30 099.29±1.62 099.89±0.34 100.00±0.00 1.594 0.222 V40 089.62±11.70 095.57±5.63 095.20±5.38 1.686 0.204 V50 019.85±8.68 029.43±16.39 024.55±10.78 1.495 0.242 膀胱 V10 100.00±0.00 100.00±0.00 100.00±0.00 - - V20 098.30±2.37 100.00±0.00 100.00±0.00 5.142 0.013 V30 090.73±5.54 099.10±1.57 099.36±1.66 20.095 0 V40 072.84±10.82 088.29±4.64 083.58±10.78 7.387 0.003 V50 020.35±7.51 027.76±10.98 021.10±8.07 2.061 0.147 左股骨头 V10 100.00±0.00 100.00±0.00 100.00±0.00 - - V20 099.45±1.34 089.84±10.67 089.47±11.93 3.717 0.038 V30 067.56±13.65 034.29±15.33 034.46±16.29 16.040 0.000 V40 010.53±5.82 004.67±6.23 005.64±6.28 2.650 0.089 V50 100.00±0.00 100.00±0.00 100.00±0.00 - - 右股骨头 V10 100.00±0.00 099.87±.27 100.00±0.00 2.043 0.149 V20 100.00±0.00 089.13±16.28 091.22±8.33 2.984 0.067 V30 074.68±14.70 050.65±23.24 039.19±12.21 10.873 0.000 V40 020.15±9.92 013.33±8.49 006.39±3.44 7.791 0.002 V50 100.00±0.00 100.00±0.00 100.00±0.00 - - 注:表中,Vn:小肠受照n Gy的体积百分比,n=10、20、30、40、50;5F-IMRT:5野调强放疗;VMAT:容积旋转调强放疗;-:无数值。
下载: 导出CSV
-
[1] 胡尚英, 郑荣寿, 赵方辉, 等. 1989至2008年中国女性子宫颈癌发病率和死亡趋势分析[J].中国医学科学院学报, 2014, 36(2):119-125. DOI:10.3881/j.issn.1000-503X.2014.02.001.
Hu SY, Zheng RS, Zhao FH, et al. Trend analysis of cervical cancer incidence and mortality rates in Chinese women duri[J]. Acta Academiae Medicinae Sinicae, 2014, 36(2):119-125. doi: 10.3881/j.issn.1000-503X.2014.02.001[2] Rotman M, Sedlis A, Piedmonte MR, et al. A phase Ⅲ randomized trial of postoperative pelvic irradiation in Stage IB cervical carcinoma with poor prognostic features:follow-up of a gynecologic oncology group study[J]. Int J Radiat Oncol Biol Phys, 2006, 65(1):169-176. DOI:10.1016/j.ijrobp.2005.10.019.、 [3] 金华, 马翔宇, 周丽静, 等.调强放疗在早期子宫颈癌术后阴道残端复发治疗中的价值[J].肿瘤研究与临床, 2014, 26(4):238-240. DOI:10.3760/cma.j.issn.1006-9801.2014.04.007.
Jin H, Ma XY, Zhou LJ, et al. Evaluation of the intensity modulated radiotherapy in early stage cervical cancer with vaginal stump recurrence after surgery[J]. Cancer Res Clin, 2014, 26(4):238-240. doi: 10.3760/cma.j.issn.1006-9801.2014.04.007[4] 穆鹏, 李联崑, 贾海清.宫颈癌术后调强放疗与三维适形放疗的对比研究[J].实用医院临床杂志, 2015, 12(2):49-51, 52. DOI:10.3969/j.issn.1672-6170.2015.02.018.
Mu P, Li LK, Jia HQ. A comparative study on three-dimensional conformal radiotherapy and intensity modulated radiotherapy in the treatment of postoperative cervical cancer[J]. Pract J Clin Med, 2015, 12(2):49-51, 52. doi: 10.3969/j.issn.1672-6170.2015.02.018[5] Yu CX. Intensity-modulated arc therapy with dynamic multileaf collimation:an alternative to tomotherapy[J]. Phys Med Biol, 1995, 40(9):1435-1449. doi: 10.1088/0031-9155/40/9/004 [6] Otto K. Volumetric modulated arc therapy:IMRT in a single gantry arc[J]. Med Phys, 2008, 35(1):310-317. DOI:10.1118/1.2818738. [7] Pecorelli S. Revised FIGO staging for carcinoma of the vulva, cervix, and endometrium[J]. Int J Gynaecol Obstet, 2009, 105(2):103-104. DOI:10.1016/j.ijgo.2009.02.012. [8] Wang JZ, Li XA, D'Souza WD, et al. Impact of prolonged fraction delivery times on tumor control:a note of caution for intensity-modulated radiation therapy (IMRT)[J]. Int J Radiat Oncol Biol Phys, 2003, 57(2):543-552. doi: 10.1016/S0360-3016(03)00499-1 [9] Moiseenko V, Duzenli C, Durand RE. In vitro study of cell survival following dynamic MLC intensity-modulated radiation therapy dose delivery[J]. Med Phys, 2007, 34(4):1514-1520. DOI:10.1118/1.2712044. [10] Guckenberger M, Richter A, Krieger T, et al. Is a single arc sufficient in volumetric-modulated arc therapy(VMAT) for complex-shaped target volumes?[J]. Radiother Oncol, 2009, 93(2):259-265. DOI:10.1016/j.radonc.2009.08.015. [11] Shaffer R, Nichol AM, Vollans E, et al. A comparison of volumetric modulated arc therapy and conventional intensity-modulated radiotherapy for frontal and temporal high-grade gliomas[J]. Int J Radiat Oncol Biol Phys, 2010, 76(4):1177-1184. DOI:10.1016/j.ijrobp.2009.03.013. [12] 杨波, 庞廷田, 孙显松, 等.宫颈癌术后盆腔容积调强弧形治疗与固定野调强放疗计划的剂量学研究[J].中华放射肿瘤学杂志, 2012, 21(6):543-546. DOI:10.3760/cma.j.issn.1004-4221. 2012. 06.018.
Yang B, Pang TT, Sun XS, et al. Dosimetric study of volumetric intensity-modulated arc therapy and fixed field intensity-modulated radiotherapy for cervix cancer[J]. Chin J Radiat Oncol, 2012, 21(6):543-546. doi: 10.3760/cma.j.issn.1004-4221.2012.06.018[13] 杨国姿, 潘振宇, 夏文明, 等.容积旋转调强与固定野动态调强在宫颈癌术后放疗的剂量学比较[J].中华放射医学与防护杂志, 2014, 34(1):37-40. DOI:10.3760/cma.j.issn.0254-5098. 2014. 01.010.
Yang GZ, Pan ZY, Xia WM, et al. Dosimetric comparison and clinical application of RapidArc and intensity-modulated radiotherapy for postoperative radiotherapy of cervical cancer[J]. Chin J Radiol Med Prot, 2014, 34(1):37-40. doi: 10.3760/cma.j.issn.0254-5098.2014.01.010[14] 吴丽丽, 谢文佳, 张武哲, 等.宫颈癌根治性放疗旋转容积调强技术及固定野动态调强放疗技术的剂量学差异[J].中国老年学杂志, 2014, 34(10):2617-2620. DOI:10.3969/j.issn.1005-9202. 2014.10.001.
Wu LL, Xie WJ, Zhang WZ, et al. Dosimetric study of volumetric modulated radiotherapy in cervical cancer treated with definitive radiotherapy[J]. Chin J Gerontol, 2014, 34(10):2617-2620. doi: 10.3969/j.issn.1005-9202.2014.10.001[15] 康梅, 权循凤, 李兵兵, 等.宫颈癌容积调强与固定野动态调强放疗技术的剂量学比较[J].安徽医学, 2016, 37(4):398-402. DOI:10.3969/j.issn.1000-0399.2016.04.005.
Kang M, Quan XF, Li BB, et al. Dosimetric study of volumetric-modulated arc radiotherapy and fixed field-intensity modulated radiation therapy for cervix neoplasms[J]. Anhui Med J, 2016, 37(4):398-402. doi: 10.3969/j.issn.1000-0399.2016.04.005[16] Jia MX, Zhang X, Yin C, et al. Peripheral dose measurements in cervical cancer radiotherapy: a comparison of volumetric modulated arc therapy and step-and-shoot IMRT techniques[J/OL]. Radiat Oncol, 2014, 9: 61[2017-10-15]. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3996072. DOI: 10.1186/1748-717X-9-61. [17] Sharfo AW, Voet PW, Breedveld S, et al. Comparison of VMAT and IMRT strategies for cervical cancer patients using automated planning[J]. Radiother Oncol, 2015, 114(3):395-401. DOI:10.1016/j.radonc.2015.02.006. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 2952
- HTML全文浏览量: 1925
- PDF下载量: 6