



-
随着电子计算机技术及医学工程的快速进步,螺旋CT的发展也日新月异,近年来,更高排螺旋CT、新宝石CT及能谱CT的应用使得多排螺旋CT在颅颈部血管的临床应用中得以广泛开展并日臻成熟。检索相关文献,基于颅颈联合CT血管成像(CT angiography,CTA)的技术应用及临床应用的论文颇多[1~4],但缺少关于规范颅颈联合照像格式的文章。全国各大医院均在进行颅颈联合CTA检查,但是照相格式五花八门,杂乱无章,在实际工作中延长了医师的影像判读时间,延误了患者的治疗时间窗。本文旨在提出一种颅颈联合CTA照相格式进行讨论,以期同道在进行此类检查后能规范照像格式,使临床医师特别是介入科医师看到的后处理图像一目了然、有章可循。
-
采用美国GE公司Lightspeed 64 VCT及AW4.6工作站,日本SONY up-df500干式热敏洗片机,北京LOCUS LD医学影像纸介质激光打印系统。
-
随机抽取2016年1月至3月影像号尾数为“9”的三门峡市中心医院影像科颅颈联合CTA图像30例(A组)及河南省人民医院影像科颅颈联合图像30例(B组)。其中,B组照相格式实例见图 1、图 2;A组照相格式实例见图 3。

图 1 河南省人民医院颅颈联合 CT 血管造影照相格式实例一 图中, A: CT 容积重建像; B: CT 多平面重建像; C: 颅内血管容积 重建像。
Figure 1. Example of the photographic format of craniocervical CT angiography in Henan Provincial People's Hospital. A: Volume rendering images; B: Multiplanar reconstruction images; C: Volume reconstruction images of intracranial vasculars.

图 2 河南省人民医院颅颈联合 CT 血管造影照相格式实例二 图中, A: CT 容积重建像; B: CT 多平面重建像; C: CT 容积重建像(黑白)。
Figure 2. Another example of the photographic format of craniocervical CT angiography in Henan Provincial People's Hospital. A: Volume rendering images; B: Multiplanar reconstruction images; C: Monochrome volume reconstruction images.

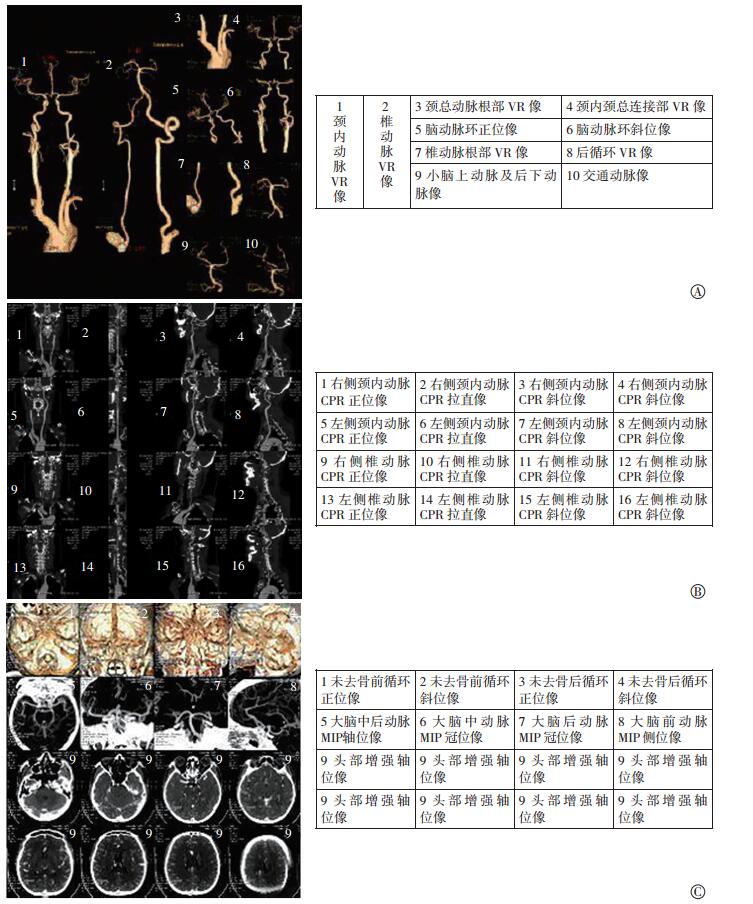
图 3 三门峡市中心医院颅颈联合 CT 血管造影照相格式实例 图中, A、 B、 C 中左侧图像分别为头颈部 VR 像、 CPR 像和 MIP 像,右侧表格为与左侧图像一一对应的文字介绍; VR: 容积重建; CPR: 血管曲面重建; MIP: 最大密度投影。
Figure 3. Example of the photographic format of craniocervical CT angiography in Sanmenxia Central Hospital. A: Volume rendering images of craniocervical blood vessels; B: Curved plannar reconstruction images of craniocervical blood vessels; C: Maximum density projection images of craniocervical blood vessels. The right forms are text description that correspond to the left images.
-
请河南省人民医院3名介入科主任医师及三门峡市中心医院2名介入科副主任医师采用5分法分别对A组、B组图像进行主观评价。评价的标准为:5分,图像有次序,表述清楚,血管定位快速准确;4分,图像较有次序,表述较清楚,血管定位较快速准确;3分,图像较有次序,表述较清楚,血管定位准确;2分,图像较有次序,表述较清楚,血管定位较准确;1分,图像无次序,表述不清楚,血管定位困难[5]。各分值的确定由医师根据情况主观确定,30例图像评分每一项取平均值,精确到小数点后2位数。
-
采用SPSS 12.0软件对数据进行统计学分析。A组和B组图像的次序满意得分、表述清楚得分、血管快速定位得分、准确度得分用均数±标准差表示,定量资料符合正态分布并方差齐采用两两比较t检验,P < 0.01表示差异有统计学意义。
-
A组及B组的照片格式满意度、血管快速准确定位得分的对照情况见表 1。A组的照片格式满意度得分为(4.70±0.23)分,B组为(3.00±1.23)分,两者比较差异有统计学意义(t=6.30,P < 0.01);A组的血管定位快速准确度得分为(4.82±0.15)分,B组为(3.00±1.13)分,两者比较差异有统计学意义(t=7.01,P < 0.01)。
组别 照片格式满意度 血管快速定位准确度 图像次序满意度得分 表述清楚得分 血管快速定位得分 定位准确度得分 A组 医师一 2.72 2.00 2.80 2.00 医师二 2.68 2.12 2.78 2.16 医师三 2.75 2.05 2.81 2.15 医师四 2.78 2.08 2.82 1.98 医师五 2.69 1.99 2.77 1.99 B组 医师一 1.51 1.51 1.51 1.51 医师二 1.45 1.49 1.47 1.52 医师三 1.52 1.48 1.49 1.51 医师四 1.51 1.49 1.50 1.53 医师五 1.49 1.48 1.52 1.51 平均 A组 4.70±0.23 4.82±0.15 B组 3.00±1.23a 3.00±1.13b 注: 表中, A 组为三门峡市中心医院影像科颅颈联合 CT 血管成像图像; B 组为河南省人民医院影像科颅颈联合 CT 血管成像图像。 a: 与 A 组比较差异有统计学意义(t = 6.30, P < 0.01); b: 与 A 组比较, 差异有统计学意义(t = 7.01, P < 0.01)。 表 1 两组的照片格式满意度、 血管快速准确定位得分对照表
Table 1. Scores of the photographic format satisfaction versus scores of positioning speed and accuracy of the blood vessels
图 1头颈部血管无整体观,动脉环旋转无规范,未见血管MPR拉直像,不利于观察血管腔内细节。图 1血管MPR像较少,VR黑白像与彩色像重复,对临床无意义。图 3对以上几点能较好解决,利于临床医师快速阅读。
图 3中A所示为血管容积再现(volume rendering,VR)像,第1、2幅较大图像清晰显示前后循环,临床医师对颅颈部血管的先天变异、起源、走形异常、狭窄、扩张等异常病变可清晰观察;第7幅图像显示颈总动脉及椎动脉根部狭窄情况;第4、5、6及8、9、10为多方位旋转像,分别显示了颈内动脉及椎基底动脉的情况,在需显示动脉瘤、狭窄等严重情况时可酌情删减其他图像。此照片的排版格式较好地解决了血管图像显示较小的问题,并通过规范化的格式使临床医师在快速阅读患者的CTA图像中能有的放矢。
图 3中B所示为血管曲面重建(curved plannar reconstruction,CPR)像,分别显示了左侧颈总(内)动脉、右侧颈总(内)动脉、左侧椎动脉、右侧椎动脉的情况,需要指出的是,在观察到明确狭窄的部位时,我们将每行的最后一幅图像替换为轴位像,以显示斑块的性质及狭窄的程度,并测量CT值。此照片的排版格式使医师一目了然,较好地减少了因排版混乱可能造成的左右方向差错的问题。
图 3中C第一行为未去骨VR像,可以较好地观察血管的解剖位置;第二行为最大密度投影(maximum intensity projection,MIP)像[6],在观察钙化斑块及穿支动脉时优点明显;后两行为头部轴位像。当需要特殊表述重点部位血管及病变的情况时,可酌情删减最后两行图像,增加诸如CT仿真内窥镜、表面重现像等图像。图 3中C为A、B较好的补充。
-
规范颅颈联合CTA照相格式非常必要。检索国内近年的医学文献,未见有关于CT片照相格式的报道[7-8]。虽然同一医院的医师经过较长时间的磨合及交流可以大致看懂图像所反映的疾病信息,可一旦有外院的医师读片时,仍会耗费一定的时间才能读懂胶片信息,这就浪费了宝贵的治疗时间,所以笔者认为规范颅颈联合CTA后处理图像格式非常必要,且意义重大[9],只有在临床工作中规范了照相格式,才能节省检查时间,避免错误,并使更多的临床医师能读懂胶片上的信息。推而广之,如果全国的头颈联合CTA照相格式能统一,那将大大减少医师的劳动量,并能节省更多的时间用于患者的治疗。
技术的进步是为了更好地服务于诊断,有规律的、可重复的照片模式经过实践证明可以快速让绝大多数影像科医师及临床医师了解病情,确定病因,迅速制定进一步的治疗方案,为患者的治疗提供了宝贵的时间。本研究经过不同医院的多名医师、教授的验证,对比其他医院的照片格式,得到了满意的效果,获得了较高的评价。
我们检索近5年的文献,有关头颈联合CTA照相格式方面的研究未见报道。我们通过科室集体商议,反复修改,并广泛征询神经内科、介入科等相关科室人员的意见及上级医院影像科高年资教授的意见,形成了现有的头颈血管CTA照相排版模式。另外为了使临床包括介入科医师能更好地了解图像所表述的意义,我们以表格形式制作并印发了照片排版中每幅图像的文字介绍,使图像和文字一一对应,并与临床医师简单沟通后,大多数临床医师很快就能接受并读懂胶片信息。
在日常CTA后处理工作中,经常遇到诸如烟雾病、血管发育畸形等病例,不能完全按此格式照相[10-11],笔者认为,特殊情况需特殊处理,在长时间地应用规范的后处理图像后,临床医师也熟悉了照相的规范,在发现一两个不能进行标准化照相的病例时也能很快发现并理解,提示临床医师注意此例患者的不同之处。
在工作实践中,我们发现不同厂家提供的照片排版的格式不尽相同,不一定都有本研究中使用的格式,但笔者相信,这是一个简单的软件问题;很多医院也有多台不同的后处理工作站,可以通过多种工作站之间的数据共享、PACS工作站的照相模式互补、软件升级等方法解决。
我们无意规范国内颅颈联合CTA照相格式,仅提出三门峡市中心医院影像科使用的照相模式分享给各位同道,这种模式在日常工作中的确起到了事半功倍的效果,获得了国内多位介入科医师的好评。依此类推,我们还规范了冠脉CTA、肾动脉CTA、主动脉CTA、下肢动脉CTA的照相格式,并在运用了彩色胶片后,使显示内容更加立体形象,取得了满意的效果。客观来说,每一种照相模式都有它的优劣性,笔者也恳请同道能对本照相格式提出批评指正,使它更规范,更利于临床阅读。
规范颅颈联合CT血管成像照相格式的临床意义
Clinical significance of standardizing the photographic format of craniocervical CTA
-
摘要:
目的探讨规范颅颈联合CT血管成像(CTA)后处理图像对临床的意义。 方法收集30例河南省三门峡市中心医院影像科(A组)和30例河南省人民医院影像科(B组)的颅颈联合CTA后处理图像,分别对图像的次序、表述、快速准确定位等方面进行主观评价,以上各项得分的两组间比较采用t检验。 结果两组图像在照片格式满意度和血管定位快速准确度方面的差异均有统计学意义(t=6.30和7.01,均P < 0.01),说明采用A组的颅颈联合CTA照相格式较B组在快速准确定位某一血管病变方面有明显的优点。 结论规范颅颈联合CTA照相格式对提高临床包括介入科医师的判读效率、减少差错率的效果明显。 -
关键词:
- 血管造影术 /
- 体层摄影术, X线计算机 /
- 颅颈联合 /
- 照相格式
Abstract:Objective To explore the clinical significance of standardizing the post -processing photos of craniocervical CT angiography(CTA). Methods Post-processing photos of craniocervical CTA of 30 cases in Sanmenxia central hospital and 30 cases in Henan provincial people's hospital were collected and divided into two groups(group A and group B). The image sequence, expression, and rapid and accurate positioning were evaluated subjectively, and the t-test was used in the two groups. Results The photographic format satisfaction, positioning speed and accuracy of the blood vessels were statistically significant in the two groups (t=6.30 and 7.01, both P < 0.01). This result illustrated that the photographic format of craniocervical CTA for the rapid and accurate localization of a vascular lesion is more advantageous in group A than in group B. Conclusion Standardizing the craniocervical CTA photographic format could shorten the interpretation time of clinicians and obviously reduce the error rate. -
Key words:
- Angiography /
- Tomography, X-ray computed /
- Craniocervical /
- Photographic format
-
图 1 河南省人民医院颅颈联合 CT 血管造影照相格式实例一 图中, A: CT 容积重建像; B: CT 多平面重建像; C: 颅内血管容积 重建像。
Figure 1. Example of the photographic format of craniocervical CT angiography in Henan Provincial People's Hospital. A: Volume rendering images; B: Multiplanar reconstruction images; C: Volume reconstruction images of intracranial vasculars.
图 2 河南省人民医院颅颈联合 CT 血管造影照相格式实例二 图中, A: CT 容积重建像; B: CT 多平面重建像; C: CT 容积重建像(黑白)。
Figure 2. Another example of the photographic format of craniocervical CT angiography in Henan Provincial People's Hospital. A: Volume rendering images; B: Multiplanar reconstruction images; C: Monochrome volume reconstruction images.
图 3 三门峡市中心医院颅颈联合 CT 血管造影照相格式实例 图中, A、 B、 C 中左侧图像分别为头颈部 VR 像、 CPR 像和 MIP 像,右侧表格为与左侧图像一一对应的文字介绍; VR: 容积重建; CPR: 血管曲面重建; MIP: 最大密度投影。
Figure 3. Example of the photographic format of craniocervical CT angiography in Sanmenxia Central Hospital. A: Volume rendering images of craniocervical blood vessels; B: Curved plannar reconstruction images of craniocervical blood vessels; C: Maximum density projection images of craniocervical blood vessels. The right forms are text description that correspond to the left images.
表 1 两组的照片格式满意度、 血管快速准确定位得分对照表
Table 1. Scores of the photographic format satisfaction versus scores of positioning speed and accuracy of the blood vessels
组别 照片格式满意度 血管快速定位准确度 图像次序满意度得分 表述清楚得分 血管快速定位得分 定位准确度得分 A组 医师一 2.72 2.00 2.80 2.00 医师二 2.68 2.12 2.78 2.16 医师三 2.75 2.05 2.81 2.15 医师四 2.78 2.08 2.82 1.98 医师五 2.69 1.99 2.77 1.99 B组 医师一 1.51 1.51 1.51 1.51 医师二 1.45 1.49 1.47 1.52 医师三 1.52 1.48 1.49 1.51 医师四 1.51 1.49 1.50 1.53 医师五 1.49 1.48 1.52 1.51 平均 A组 4.70±0.23 4.82±0.15 B组 3.00±1.23a 3.00±1.13b 注: 表中, A 组为三门峡市中心医院影像科颅颈联合 CT 血管成像图像; B 组为河南省人民医院影像科颅颈联合 CT 血管成像图像。 a: 与 A 组比较差异有统计学意义(t = 6.30, P < 0.01); b: 与 A 组比较, 差异有统计学意义(t = 7.01, P < 0.01)。  下载: 导出CSV
下载: 导出CSV
-
[1] Röther J, Jonetz-Mentzel L, Fiala A, et al. Hemodynamic assessment of acute stroke using dynamic single-slice computed tomographic perfusion imaging[J]. Arch Neurol, 2000, 57(8):1161-1166. DOI:10.1001/archneur.57.8.1161. [2] Koenig M, Klotz E, Luka B, et al. Perfusion CT of the brain:diagnostic approach for early detection of ischemic stroke[J]. Radiology, 1998, 209(1):85-93. DOI:10.1148/radiology.209.1. 9769817. [3] Koenig M, Kraus M, Theek C, et al. Quantitative assessment of the ischemic brain by means of perfusion-related parameters derived from perfusion CT[J]. Stroke, 2001, 32(2):431-437. DOI:10.1161/01.STR.32.2.431. [4] 满晓, 冷振璞, 庞在英, 等. CT灌注成像联合CT血管造影诊断超早期缺血性脑血管病的价值[J].临床神经病学杂志, 2004, 17(2):89-91. DOI:10.3969/j.issn.1004-1648.2004.02.004.
Man X, Leng ZP, Pang ZY, et al. The value of combined application of CT perfusion imaging and CT angiography in the diagnosis of hyperacute ischemic cerebrovascular disease[J]. J Clin Neurol, 2004, 17(2):89-91. doi: 10.3969/j.issn.1004-1648.2004.02.004[5] 刘玉明, 陈锋, 唐小锋, 等.改良64层CT颅颈联合动脉成像技术的临床价值[J].中华临床医师杂志:电子版, 2010, 4(9):1617-1622. DOI:10.3969/cma.j.issn.1674-0785.2010.09.029.
Liu YM, Chen F, Tang XF, et al. Cinical value of modified 64-slice CT angiography technique in brain and neck combined artery imaging[J]. Chin J Clinicians(Electronic Edition), 2010, 4(9):1617-1622. doi: 10.3969/cma.j.issn.1674-0785.2010.09.029[6] 徐俊, 林江, 蒋黛蒂.颅颈联合CT血管成像检查进展[J].临床放射学杂志, 2011, 30(5):761-764. DOI:10.13437/j.cnki.jcr.2011. 05.015.
Xu J, Lin J, Jiang DD, et al. Latest advances of craniocervical CTA[J]. J Clin Radiol, 2011, 30(5):761-764.. doi: 10.13437/j.cnki.jcr.2011.05.015[7] Yu S, Zhang L, Zheng J, et al. A comparison of adaptive iterative dose reduction 3D and filtered back projection in craniocervical CT angiography[J/OL]. Clin Radiol, 2017, 72(1):96.e1-96.e6[2017-07-04]. http://www.sciencedirect.com/science/article/pii/S0009926016303233?via%3Dihub.DOI:10.1016/j.crad.2016.08.004. [8] 陈钰, 朱元利, 薛华丹, 等.第3代双源CT 70 kV管电压和20~25 ml对比剂模式下行头颈联合CT血管成像在体质量小于75 kg人群中的效果[J].中国医学科学院学报, 2017, 39(1):4-11. DOI:10.3881/j.issn.1000-503X.2017.01.002.
Chen Y, Zhu YL, Xue HD, et al. Third-generation dual-source CT for head and neck CT angiography with 70 kV tube voltage and 20-25 ml contrast medium in patients with body weight lower than 75 kg[J]. Acta Acad Med Sin, 2017, 39(1):4-11. doi: 10.3881/j.issn.1000-503X.2017.01.002[9] 张军, 王剑虹, 刘军, 等.头颈联合CT血管造影在头颈动脉狭窄中的应用[J].中国医学计算机成像杂志, 2013, 19(2):97-101. DOI:10.3969/j.issn.1006-5741.2013.02.001.
Zhang J, Wang JH, Liu J, et al. Applications of standardized examination protocol of multiple-slice spiral CT angiography in intracranial and cervical arteries[J]. Chin Comput Med Imag, 2013, 19(2):97-101. doi: 10.3969/j.issn.1006-5741.2013.02.001[10] 唐翠松, 汤光宇, 李伟, 等.头颈联合CTA对动脉成窗变异的评价[J].临床放射学杂志, 2012, 31(6):790-793. DOI:10.13437/j.cnki.jcr.2012.06.008.
Tang CS, Tang GY, Li W, et al. The application of cranio-cervical CT angiography in the evaluation of intracranial and cervical arterial fenestration[J]. J Clin Radiol, 2012, 31(6):790-793. doi: 10.13437/j.cnki.jcr.2012.06.008[11] 孟庆涛, 郑穗生, 李军, 等. MSCTA对永存颈动脉-椎基底动脉吻合的诊断价值[J].实用放射学杂志, 2014, 30(5):880-882.
Meng QT, Zheng SS, Li J, et al. The value of MSCTA in the diagnosis of persistent carotid-vertebralbasilar arartery anastomoses[J]. J Pract Radiol, 2014, 30(5):880-882. -

 点击查看大图
点击查看大图

计量
- 文章访问数: 2786
- HTML全文浏览量: 1707
- PDF下载量: 2