


-
临床工作中,孤立性肺结节(solitary pulmonary nodule,SPN)的影像诊断和鉴别诊断一直是难点,18F-FDG PET/CT作为最有效的鉴别SPN的检查手段,仍然存在一些不足。 18F-FDG PET/CT显像诊断结节的良恶性是根据肿瘤组织葡萄糖代谢差异来判断的,但18F-FDG属非特异性肿瘤显像剂,对一些炎症组织(如结核性肉芽肿、结节病)会产生假阳性结果。常规18F-FDG PET/CT显像单纯依靠SUVmax判断肺结节良恶性的灵敏度、特异度及准确率较低,且假阳性率及假阴性率较高,结合18F-FDG PET/CT延迟显像后,仍有部分病变难以鉴别。近年来,有学者寻找除18F-FDG PET/CT以外的其他影像学方法来弥补其不足,如高分辨率CT(high resolution computed tomography,HRCT)及11C-胆碱(choline,11C-CHO)显像[1]。本研究探讨了常规18F-FDG PET/CT、18F-FDG双时相PET/CT、HRCT及11C-CHO PET/CT多模态显像对SPN的诊断价值,现报道如下。
-
选取2008年1月至2015年6月在我院临床诊断的SPN 28例,其中男性17例、女性11例,年龄33~84岁,平均年龄(60.8±10.5)岁。
入选标准:肺实质内直径≤30 mm的圆形或椭圆形单发肺内肿块,无远处转移,且不伴有肺门和纵隔淋巴结肿大、肺不张、胸腔积液或肺炎,未接受放、化疗,有长期临床随访结果或明确的病理诊断。
剔除标准:肺实质内多发结节,直径>30 mm的单发肺内肿块,体格检査或辅助检査发现有远处转移者,曾接受放、化疗。
28例SPN患者的结节分布:10例位于左上肺,6例位于右上肺,2例位于右中肺,2例位于右下肺,8例位于左下肺。 所有患者均于检查前签署了知情同意书,该研究获得了我院伦理委员会的批准。
-
PET/CT扫描仪为美国GE公司的Discover ST PET/CT仪,18F-FDG及11C-CHO由我院PET/CT中心的美国GE公司回旋加速器生产,放化纯>95%,并经无菌、无热原、细菌内毒素检测合格。
所有患者均于18F-FDG PET/CT扫描前禁食6 h以上,注射前空腹血糖水平控制在正常范围内,于病变对侧静脉注射18F-FDG(5.55 MBq/kg),嘱患者静卧约45 min,排空膀胱后行PET/CT全身显像(扫描范围从颅顶至股骨上段,根据患者的身高扫描 6 ~ 8个床),扫描完成后行肺部HRCT扫描,2 h后行肺部延迟显像。隔日注射11C-CHO(5.55 MBq/kg),10 min后行肺局部显像,PET和CT图像传送到xeleris工作站进行图像融合。
-
由2位核医学科副主任及以上医师共同阅片,诊断意见有分歧时,另请一位主任医师阅片,两位或以上医师意见一致时方可作出诊断。
PET显像图的判断以SUVmax作为半定量指标,以SPN最大截面勾画ROI,18F-FDG及11C-CHO 均以SUVmax≥2.5为阳性。
双时相显像根据以下公式计算SUVmax变化率:
△SUVmax = (SUVDelay - SUVNormal)/SUVNormal×100%
公式中,SUVDelay为延迟显像SUVmax,SUVNormal为常规显像SUVmax。
18F-FDG PET/CT延迟显像SUVmax上升≥10%为恶性病变(阳性),下降或上升<10%为良性病变(阴性)。
HRCT图像评判恶性结节的标准为:结节边界清晰并具有两项及两项以上征象者(包括分叶征、短细毛刺、胸膜尾征、支气管充气征、血管集束征、空泡征)。
当18F-FDG、11C-CHO PET/CT显像阳性且HRCT结节呈恶性表现时,临床诊断为恶性SPN(阳性);当18F-FDG、11C-CHO PET/CT显像阴性且HRCT结节呈良性表现时,临床诊断为良性SPN(阴性);当18F-FDG PET/CT阳性、11C-CHO PET/CT阴性、HRCT结节呈良性表现时诊断良性SPN可能性较大;当18F-FDG PET/CT阴性、11C-CHO PET/CT阳性、HRCT结节呈恶性表现时诊断恶性SPN可能性较大。
-
对所有病例进行随访,以显像诊断是否符合临床随访及病理检查结果作为判断标准。临床随访时间为12个月。
-
采用SPSS19.0软件进行统计学分析。根据诊断标准,计算18F-FDG PET/CT、18F-FDG双时相PET/CT、11C-CHO PET/CT及11C-CHO+18F-FDG双时相PET/CT+HRCT的准确率、灵敏度(真阳性率)、特异度(真阴性率)。计算患者18F-FDG和11C-CHO的SUVmax及分析良恶性结节分叶、毛刺、胸膜尾征、血管集束征之间的差异,计量数据均以均数 ± 标准差表示,符合正态分布和方差齐性,组间SUVmax的比较采用t检验,计数资料采用χ2检验。P < 0.05表示差异有统计学意义。
-
28例SPN患者中,经病理或临床随访确诊,有肺癌17例,结核7例,结节病4例。
常规18F-FDG PET/CT 显像确诊21 例,其中5 例腺癌、8 例鳞癌、1 例鳞腺癌为真阳性,4 例结核和3 例结节病为真阴性。4 例患者因SUVmax≥2.5 而出现假阳性,病理证实有3 例结核、1 例结节病。3 例SUVmax < 2.5 假阴性患者,穿刺病理证实1例高分化腺癌(图 1中A)、2 例高分化鳞癌,二者病变直径均小于15 mm。常规18F-FDG PET/CT显像结果的准确率为75.0%,灵敏度(真阳性率)为82.4%,特异度(真阴性率)为63.6%(表 1)。

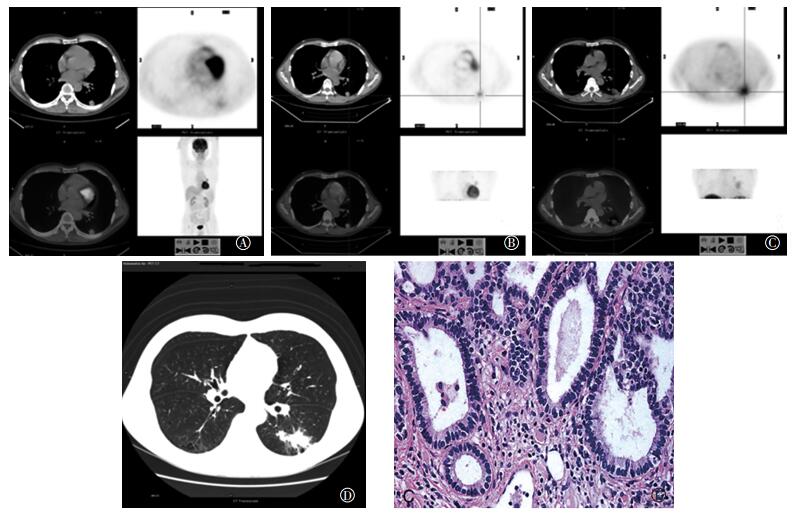
图 1 左肺下叶后基底段孤立性肺结节的 18F-FDG PET/CT 常规全身显像、 肺局部延迟显像、 11C-胆碱 PET/CT 肺局部显像、 肺高分辨率 CT 和病理图 患者男性, 65 岁, 间歇性咳嗽 3 个月余, 无明显咯痰、 咯血, 就诊呼吸内科, 门诊 CT 发现左肺下叶背段小结节影, 为确诊结节性质, 行 PET/CT 检查。 图中, A: 18F-FDG PET/CT 图, CT 图示左肺下叶后基底段直径约 2.1 cm 结节影, CT 值 23~42 Hu, PET 图示相应部位显像剂摄取增高, SUVmax 约 1.8; B: 18F-FDG PET/CT 延迟显像图, PET 图示相应部位显像剂摄取增高, SUVmax 约 2.4, 滞留指数为 33%;C: 11C-胆碱 PET/CT 图, PET 图示相应部位显像剂摄取增高, SUVmax 约 2.8; D: 高分辨率 CT 图, 示结节见分叶征、 短细毛刺、 胸膜尾征、支气管充气征、 血管集束征、 空泡征; E: 术后病理图, 左下肺腺癌(苏木精-伊红染色, ×200)。
Figure 1. The 18F-FDG PET/CT normal imaging, 18F-FDG PET/CT delay imaging, 11C-CHO PET/CT imaging, HRCT imaging and pathology of the left lower lobe posterior basal section solitary pulmonary lesion
显像方式 准确度 灵敏度(真阳性率) 特异度(真阴性率) 18F-FDG PET/CT 75.0(21/28) 82.4(14/17) 63.6(7/11) 18F-FDG 双时相 PET/CT 85.7(24/28) 88.9(16/18) 80.0(8/10) 11C-CHO PET/CT 82.1(23/28) 82.3(14/17) 81.8(9/11) 11C-CHO+18F-FDG 双时相 PET/CT+HRCT 96.4(27/28) 90.0(9/10) 91.7(11/12) 注: 表中, CHO: 胆碱; HRCT: 高分辨率 CT。 表 1 28 例孤立性肺结节患者 4 种显像方法的灵敏度、 特异度、 准确率比较(%)
Table 1. 28 patients with socitary pulmonary nodule were compared through true positive rate, negative rate and accuracy by 4 imagings(%)
18F-FDG双时相PET/CT(常规显像+延迟显像)确诊24例(肺癌16例、良性病8例),研究结果显示18例SPN 延迟显像2 h时,SPN 的延迟显像△SUVmax较早期常规显像的SUVmax上升≥10%(13.7%±3.1%)而诊断为恶性病变(图 1中B)。4 例结核患者因常规显像SUVmax≥2.5疑似恶性的患者中3 例患者SUVmax 降低或升高未达10%而考虑为良性病。3例结节病和2例结核常规显像和延迟显像SUVmax < 2.5考虑良性病。4例误诊患者,其中2例诊断为恶性的SPN,穿刺活检为良性(1例结核,1例结节病),误诊原因可能与病变处于增殖活跃期有关。2例诊断为良性病变的SPN,1例观察6个月结节体积增大,手术后病理为肺泡细胞癌,与病变呈磨玻璃影有关。1例误诊为结核,抗结核无效,活检为结节病。 常规显像+延迟显像结果的准确率为85.7%,灵敏度(真阳性率)为88.9%,特异度(真阴性率)为80.0%(表 1)。
11C-CHO PET/CT显像确诊23 例,其中21 例11C-CHO PET/CT与18F-FDG PET/CT显像结果均一致,且恶性与良性病变比较,SUVmax明显增高,差异有统计学意义(表 2);4 例18F-FDG SUVmax≥2.5 患者中有2 例11C-CHO SUVmax < 2.5,病理证实1 例结核、1 例结节病。3例18F-FDG SUVmax < 2.5而11C-CHO SUVmax≥2.5的患者中1例随访或活检均为良性,可能与良性病变细胞膜增殖较快有关,2例为恶性(图 1中C)。11C-CHO PET/CT显像结果的准确率为82.1%,灵敏度(真阳性率)为82.3%,特异度(真阴性率)为81.8%(表 1)。
显像剂 肺癌(n=17) 良性病变(n=11) t P值 18F-FDG 5.29±2.75 2.20±1.23 10.57 0.00 11C-CHO 3.28±1.76 0.81±0.79 13.19 0.00 注: 表中, CHO: 胆碱。 表 2 28 例孤立性肺结节患者 18F-FDG PET/CT 和 11C-CHO PET/CT 的 SUVmax 比较
Table 2. 28 patients were compared through SUVmax by 18F-FDG PET/CT and 11C-CHO PET/CT
11C-CHO+18F-FDG双时相PET/CT+HRCT确诊27 例(肺癌16例,结核7例,结节病4例),与常规18F-FDG PET/CT显像比较,4 例18F-FDG PET/CT显像结果SUVmax≥2.5的SPN患者中均无HRCT恶性表现;3 例18F-FDG PET/CT显像结果SUVmax < 2.5的SPN患者中,2例有两个以上HRCT 恶性表现(图 1中D),病理结果确诊为恶性(图 1中E),误诊1 例有HRCT 恶性表现,但病理结果为良性,可能与结核处于活跃期,血供较丰富有关。11C-CHO+18F-FDG双时相PET/CT+HRCT显像结果的准确率为96.4%,灵敏度(真阳性率)为90.0%,特异度(真阳性率)为91.7%(表 1)。所有患者的HRCT特征比较详见表 3。
分类 分叶 毛刺征 胸膜尾征 支气管充气征 血管集束征 空泡征 肺癌(n=17) 13 3 6 4 3 1 良性(n=11) 1 0 1 7 0 2 χ2 9.27 10.36 14.31 4.50 17.52 1.05 P值 <0.05 <0.05 <0.05 >0.05 <0.05 >0.05 表 3 28 例孤立性肺结节患者高分辨率 CT 特征比较
Table 3. 28 patients were compared through high resolution CT
-
肺癌是最常见的恶性肿瘤之一。2012年全球肺癌新发病例和死亡病例高居各种恶性肿瘤前位,占当年全部恶性肿瘤发病和死亡例数的13.2%和19.4%[2],肺癌的发生与吸烟、大气污染、石棉等环境暴露因素密切相关。近年来我国经济发展迅速,随着工业化和城市化进程的不断加快,我国居民的生活环境和生活方式发生了剧烈变化,肺癌在我国的发病率也呈显著上升趋势。2015年卫生统计数据显示,肺癌的发病率和病死率均占我国恶性肿瘤首位[3]。
肺癌的生存率与肺癌是否能早期诊断、早期治疗密切相关,肺癌的早期表现之一为SPN,目前评价SPN的影像学方法包括胸部X片、CT、MRI及PET/CT等。胸部X片因其密度分辨力低而且有影像上的重叠,心脏后方的病变和小的病变不易观察,误诊及漏诊率较高。近年来,低剂量CT的应用一方面增加了肺结节被筛查出的可能,如美国国立癌症研究所公布低剂量螺旋CT用于肺癌筛查可有效降低20%的肺癌病死率;另一方面被筛查出的肺结节定性诊断仍是难点,特别是 SPN,其病理类型、生长方式、局部播散方式复杂,影像学征象表现为多种多样,尽管包含如炎性假瘤等良性病变,但有30%~40% 的SPN为恶性结节[4]。单纯CT形态学诊断SPN的灵敏度、特异度、准确率较低[5]。
SPN的诊断及鉴别诊断一直是临床难题,随着18F-FDG PET/CT越来越多地用于肺部良恶性病变的鉴别[6],且被推荐用于3~30 mm的SPN的定性诊断[7],SPN的诊断准确率大幅提高。据文献报道,18F-FDG PET/CT显像诊断SPN的灵敏度可达82%,特异度为60%[8]。本研究中,单次18F-FDG PET/CT显像对SPN诊断的准确率为75.0%,灵敏度为82.4%,特异度为63.6%,与相关文献报道一致;假阳性病例与其他文献报道的炎症增殖性病变18F-FDG摄取增高一致[9];假阴性患者与病灶小(直径<15 mm)及呈毛玻璃样改变有关,需结合HRCT综合分析,减少假阴性。
由于SPN直径较小(直径≤30 mm),且18F-FDG并非特异性显像剂,部分良性SPN的SUVmax≥2.5,与恶性SPN较难鉴别,部分国内外学者认为18F-FDG双时相PET/CT显像能够提高诊断SPN的灵敏度和准确率,对SPN的鉴别诊断有重要价值[10-11],双时相PET/CT显像主要原理是恶性肿瘤18F-FDG持续摄取增高且在肿瘤内滞留时间长,良性病变是暂时18F-FDG摄取增高,但滞留时间较短,大多数学者认为恶性肿瘤摄取18F-FDG平均峰时在注射后4 h,而良性肿瘤及炎性病变的摄取峰时在注射后 0.5 h,且随着时间的延长,良性病变的 SUVmax减小[12]。本研究结果显示28例SPN患者中有18例SPN 延迟显像2 h 时,SUVmax较早期常规显像上升>10%,其中17例诊断为恶性SPN,与病理结果一致,1例SUVmax≥2.5的SPN患者延迟显像SUVmax升高>10%,但穿刺结果为结核,可能是因为这类良性肉芽肿性病变含有大量的类上皮细胞、郎罕氏巨细胞及淋巴细胞成分,这些细胞的葡萄糖代谢旺盛,18F-FDG摄取较高,因此导致结果的假阳性[13]。4 例结核患者因常规显像SUVmax≥2.5疑似恶性的患者中3 例患者SUVmax 降低或升高未达10%而考虑为良性病变,临床随访12个月或穿刺活检证实为良性SPN。18F-FDG双时相PET/CT显像对SPN诊断的准确率为85.7%,灵敏度为88.9%,特异度为80.0%,准确率及灵敏度较常规显像明显提高。这与国内外文献的报道一致[14-16]。
除肿瘤外,正常组织及一些良性病变也可摄取18F-FDG,给临床SPN的鉴别诊断带来了一定的困难。随着正电子标记药物的研发,11C-CHO对某些肿瘤(如前列腺癌、脑瘤和膀胱癌等)的鉴别诊断价值明显优于18F-FDG[17],滕学鹏等[18]的研究结果显示,肺部恶性占位病变的2种显像剂SUVmax均明显高于良性占位,两者间的差异有统计学意义;本研究也将11C-CHO应用于SPN的鉴别诊断,结果显示,18F-FDG SUVmax在良、恶性SPN中的差异有统计学意义(t = 10.57,P < 0.05),而11C-CHO SUVmax在良、恶性SPN中的差异也具有统计学意义(t =13.19,P < 0.05),与文献报道一致。滕学鹏等[18]的研究结果显示,11C-CHO PET/CT对肺部病变诊断的灵敏度为88.39%、特异度为80.95%、准确率为85.20%。本研究中的结果显示,11C-CHO PET/CT对SPN诊断的灵敏度为82.3%、特异度为81.8%、准确率为82.3%,较文献报道稍低,可能与本研究中的对象为SPN(直径≤30 mm)有关。在本研究中,有21例SPN患者的18F-FDG PET/CT与11C-CHO PET/CT显像结果均一致,4例18F-FDG SUVmax≥2.5患者中有2例11C-CHO SUVmax <2.5,病理证实为1例结核、1例结节病,此结果表明,11C-CHO对18F-FDG诊断较困难的病例是有益的补充。
18F-FDG在肿瘤局部异常浓聚是恶性肿瘤的重要标志,但18F-FDG PET/CT检查方法不具特异性,会出现一定假阳性和假阴性,分化较好和生长缓慢的肿瘤或结节直径<10 mm的恶性肿瘤可出现假阴性,尤以毛玻璃影为著,有些穿刺活检结果为腺癌,但影像表现无18F-FDG摄取。HRCT检查可准确反映SPN的位置、形态、结节内密度、结节与周围组织的关系,因此,HRCT可对部分结节的性质作出判断。陶鑫等[19]研究表明,分叶、毛刺、胸膜尾征、血管集束征是恶性病变的征象,圆形、表面光滑及钙化是良性病变的征象。本研究结果显示,良恶性结节分叶、毛刺、胸膜尾征、血管集束征之间的差异有统计学意义。
大量报道提示,PET/CT在SPN诊断方面是目前最准确的鉴别诊断工具,但仍有假阳性和假阴性[20],应通过多模态显像(11C-CHO+18F-FDG双时相 PET/CT+HRCT)来寻找诊断SPN的最佳手段。本研究中多模态显像确诊的27例患者与常规18F-FDG PET/CT显像比较,4例SUVmax≥2.5的SPN无HRCT恶性表现;2例SUVmax<2.5的SPN有两个以上HRCT恶性表现;1例SUVmax<2.5的SPN有HRCT恶性表现,病理结果为良性。该结果显示,多模态显像诊断的灵敏度为90.0%、特异度为91.7%、准确率为96.4%,因此,多模态显像是诊断SPN的最好手段之一。
综上所述,多模态显像可弥补常规PET/CT检查中的某些不足,达到应用上的优势互补。多种显像剂和双时相结合HRCT综合分析,大大提高了诊断SPN的灵敏度、特异度及准确率,在鉴别SPN的良恶性方面更具优势,可用以指导临床诊治,避免不必要的手术给患者带来精神及经济上的负担。
11C-胆碱与18F-FDG双时相PET/CT显像结合高分辨率CT在孤立性肺结节鉴别诊断中的应用
Application of 11C-CHO and 18F-FDG dual-phase PET/CT imaging combined with high-resolution computed tomography in differential diagnosis of solitary pulmonary nodules
-
摘要:
目的比较11C-胆碱(11C-CHO)PET/CT、18F-FDG双时相PET/CT、常规18F-FDG PET/CT、11C-CHO+18F-FDG双时相PET/CT显像结合高分辨率CT(HRCT)4种方法对鉴别诊断孤立性肺结节(SPN)良恶性的价值。 方法对28例SPN患者进行18F-FDG PET/CT显像(注药后l h显像,2 h行延迟显像)和11C-CHO PET/CT显像(于注药10 min后进行)。PET图像判断以SPN最大截面勾画ROI,计算SUVmax作为半定量指标,SUVmax ≥ 2.5为阳性,18F-FDG PET/CT延迟显像SUVmax上升10%为恶性病变(阳性),下降或升高 < 10%为良性病变(阴性)。HRCT以是否有分叶征、短细毛刺、胸膜尾征、支气管充气征、血管集束征、空泡征为分析良恶性的指征。所有病例进行临床综合分析及随访,以影像诊断是否符合临床随访及病理结果作为判断标准。组间SUVmax的比较采用t检验;计数资料的比较采用χ2检验。 结果 28例SPN患者中,病理或临床随访诊断发现肺癌17例,结核7例,结节病4例。常规18F-FDG PET/CT显像确诊21例,18F-FDG双时相PET/CT显像确诊24例,11C-CHO PET/CT显像确诊23例,11C-CHO +18F-FDG双时相PET/CT+HRCT确诊27例。28例患者良恶性结节的18F-FDG及11C-CHO PET/CT的SUVmax比较,差异有统计学意义(t=10.57和13.19,均P < 0.05)。良恶性结节分叶、毛刺、胸膜尾征、血管集束征之间的差异有统计学意义(χ2=9.27、10.36、14.31和17.52,均P < 0.05)。11C-CHO+18F-FDG双时相PET/CT+HRCT联合显像的灵敏度为81.8%,特异度为94.1%,准确率为96.4%,明显高于非联合显像。 结论 11C-CHO+18F-FDG双时相PET/CT+HRCT能较好地鉴别SPN的良恶性,三者联合能提高对SPN的诊断率。 -
关键词:
- 孤立性肺结节 /
- 胆碱 /
- 氟脱氧葡萄糖F18 /
- 正电子发射断层显像术 /
- 体层摄影术, X线计算机
Abstract:Objective To compare choline (11C-CHO) PET/CT, conventional 18F-FDG PET/CT, 18F-FDG double-phase PET/CT, and 11C-CHO PET/CT +18F-FDG double-phase PET/CT imaging combined with high-resolution computed tomography(HRCT) to determine whether differential diagnosis value for solitary pulmonary nodules (SPN) is benign or malignant. Methods This study included 28 patients who were clinically diagnosed with SPN. Patients were injected with 18F-FDG then subjected to PET/CT scan after 1 and 2 h and were injected with 11C-CHO then subjected to PET/CT scan again after 10 min. PET images were analyzed by SPN maximum section ROI and SUVmax as a semi-quantitative index, wherein values higher than 2.5 are considered positive for SPN. SUVmax in routine were compared with that in delayed 18F-FDG PET/CT imaging, wherein an increase of more than 10% indicates malignant lesions (positive), whereas a decrease or increase by less than 10% indicates benign lesions (negative). Benign or malignant lesion were analyzed with lobulation, short spiculation and pleural tail sign, air bronchogram, vascular convergence sign, and vacuole sign in HRCT imaging. All cases were analyzed and clinically followed-up. Imaging diagnoses were compared with pathological results or clinical follow -up. SUVmax comparisons between groups were tested by t-test and the enumeration data were compared by analysis of variance. Results Twenty -eight patients were pathologically diagnosed and clinically followed-up. Seventeen patients were diagnosed with lung cancer, seven with tuberculosis, and four with sarcoidosis. Twenty patients were confirmed by routine 18F-FDG PET/CT imaging, 24 by double-phase 18F-FDG PET/CT imaging, 23 by routine 11C-CHO PET/CT imaging, and 27 by 11C -CHO PET/CT + 18F -FDG double -phase PET/CT + HRCT. 18F -FDG and 11C -CHO SUVmax in benign or malignant nodules in 28 patients were analyzed. Differences were statistically significant(t=10.57 and 13.19, both P < 0.05). A significant difference exists between benign and malignant nodules in the leaf, burr, pleural tail sign, and vascular bundle sign(χ2=9.27, 10.36, 14.31, and 17.52, all P < 0.05). The sensitivity, specificity and accuracy of 11C -CHO +18F -FDG dual phase PET/CT +HRCT were 90.0%, 91.7% and 96.4%, significantly higher than that of the others uncombined imaging. Conclusion 11C-CHO PET/CT + 18F-FDG dual-phase PET/CT+HRCT can determine whether SPN is benign or malignant. Combine the three scan models will improve diagnostic efficiency of SPN. -
图 1 左肺下叶后基底段孤立性肺结节的 18F-FDG PET/CT 常规全身显像、 肺局部延迟显像、 11C-胆碱 PET/CT 肺局部显像、 肺高分辨率 CT 和病理图 患者男性, 65 岁, 间歇性咳嗽 3 个月余, 无明显咯痰、 咯血, 就诊呼吸内科, 门诊 CT 发现左肺下叶背段小结节影, 为确诊结节性质, 行 PET/CT 检查。 图中, A: 18F-FDG PET/CT 图, CT 图示左肺下叶后基底段直径约 2.1 cm 结节影, CT 值 23~42 Hu, PET 图示相应部位显像剂摄取增高, SUVmax 约 1.8; B: 18F-FDG PET/CT 延迟显像图, PET 图示相应部位显像剂摄取增高, SUVmax 约 2.4, 滞留指数为 33%;C: 11C-胆碱 PET/CT 图, PET 图示相应部位显像剂摄取增高, SUVmax 约 2.8; D: 高分辨率 CT 图, 示结节见分叶征、 短细毛刺、 胸膜尾征、支气管充气征、 血管集束征、 空泡征; E: 术后病理图, 左下肺腺癌(苏木精-伊红染色, ×200)。
Figure 1. The 18F-FDG PET/CT normal imaging, 18F-FDG PET/CT delay imaging, 11C-CHO PET/CT imaging, HRCT imaging and pathology of the left lower lobe posterior basal section solitary pulmonary lesion
表 1 28 例孤立性肺结节患者 4 种显像方法的灵敏度、 特异度、 准确率比较(%)
Table 1. 28 patients with socitary pulmonary nodule were compared through true positive rate, negative rate and accuracy by 4 imagings(%)
显像方式 准确度 灵敏度(真阳性率) 特异度(真阴性率) 18F-FDG PET/CT 75.0(21/28) 82.4(14/17) 63.6(7/11) 18F-FDG 双时相 PET/CT 85.7(24/28) 88.9(16/18) 80.0(8/10) 11C-CHO PET/CT 82.1(23/28) 82.3(14/17) 81.8(9/11) 11C-CHO+18F-FDG 双时相 PET/CT+HRCT 96.4(27/28) 90.0(9/10) 91.7(11/12) 注: 表中, CHO: 胆碱; HRCT: 高分辨率 CT。  下载: 导出CSV
下载: 导出CSV
表 2 28 例孤立性肺结节患者 18F-FDG PET/CT 和 11C-CHO PET/CT 的 SUVmax 比较
Table 2. 28 patients were compared through SUVmax by 18F-FDG PET/CT and 11C-CHO PET/CT
显像剂 肺癌(n=17) 良性病变(n=11) t P值 18F-FDG 5.29±2.75 2.20±1.23 10.57 0.00 11C-CHO 3.28±1.76 0.81±0.79 13.19 0.00 注: 表中, CHO: 胆碱。
下载: 导出CSV
表 3 28 例孤立性肺结节患者高分辨率 CT 特征比较
Table 3. 28 patients were compared through high resolution CT
分类 分叶 毛刺征 胸膜尾征 支气管充气征 血管集束征 空泡征 肺癌(n=17) 13 3 6 4 3 1 良性(n=11) 1 0 1 7 0 2 χ2 9.27 10.36 14.31 4.50 17.52 1.05 P值 <0.05 <0.05 <0.05 >0.05 <0.05 >0.05
下载: 导出CSV
-
[1] 李昕, 王晴文, 姚树展, 等. 11C-胆碱PET/CT显像在肺癌中的应用价值及其机理的研究[J].医学影像学杂志, 2012, 22(4):546-551. DOI:10.3969/j.issn.1006-9011.2012.04.010.
Li X, Wang QW, Yao SZ, et al. The research of 11C-choline PET/CT imaging and choline metabolism on lung cancer[J]. J Med Imaging, 2012, 22(4):546-551. doi: 10.3969/j.issn.1006-9011.2012.04.010[2] Torre LA, Bray F, Siegel RL, et al. Global cancer statistics, 2012[J]. CA Cancer J Clin, 2015, 65(2):87-108. DOI:10.3322/caac.21262. [3] Chen W, Zheng R, Baade PD, et al. Cancer statistics in China, 2015[J]. CA Cancer J Clin, 2016, 66(2):115-132. DOI:10.3322/caac.21338. [4] 李培秀, 徐晓磊, 都日娜, 等.恶性孤立性肺结节螺旋CT与PET/CT分析[J].医疗卫生装备, 2016, 37(8):84-86. DOI:10.7687/J.ISSN1003-8868.2016.08.084.
Li PX, Xu XL, Du RN, et al. Spiral CT and PET/CT manifestations of malignant solitary pulmonary nodules[J]. Chin Med Equip J, 2016, 37(8):84-86. doi: 10.7687/J.ISSN1003-8868.2016.08.084[5] 林洁, 郑祥武, 殷薇薇, 等. PET/CT双时相显像对孤立性肺结节诊断价值的ROC曲线分析[J].肿瘤学杂志, 2015, 21(4):292-296. DOI:10.11735/j.issn.1671-170X.2015.04.B008.
Lin J, Zheng XW, Yin WW, et al. The ROC analysis of dual time point PET/CT imaging in diagnosis of solitary pulmonary nodule[J]. J Chin Oncol, 2015, 21(4):292-296. doi: 10.11735/j.issn.1671-170X.2015.04.B008[6] Yilmaz F, Tastekin G. Sensitivity of 18F-FDG PET in evaluation of solitary pulmonary nodules[J/OL]. Int J Clin Exp Med, 2015, 8(1):45-51[2017-04-10]. http://www.ncbi.nlm.nih.gov/pubmed/25784973. [7] Gould MK, Donington J, Lynch WR, et al. Evaluation of individuals with pulmonary nodules:when is it lung cancer? Diagnosis and management of lung cancer, 3rd ed:American College of Chest Physicians evidence-based clinical practice guidelines[J/OL]. Chest, 2013, 143(5 Suppl):e93S-e120S[2017-04-10]. https://www.ncbi.nlm.nih.gov/pubmed/23649456.DOI:10.1378/chest.12-2351. [8] Ohno Y, Nishio M, Koyama H, et al. Solitary pulmonary nodules:comparison of dynamic First-Pass contrast-enhanced perfusion Area-Detector CT, dynamic First-Pass contrast-enhanced Mr imaging, and FDG PET/CT[J]. Radiology, 2015, 274(2):563-575. DOI:10.1148/radiol.14132289. [9] 李文婵, 陈敏, 姚稚明, 等.肺单发结核瘤18F-FDG PET/CT误诊分析[J].中国医学影像学杂志, 2016, 24(10):737-740, 745. DOI:10.3969/j.issn.1005-5185.2016.10.006.
Li WC, Chen M, Yao ZM, et al. Misdiagnosis of 18F-FDG PET/CT in Single Pulmonary Tuberculoma[J]. Chin J Med Imaging, 2016, 24(10):737-740, 745. doi: 10.3969/j.issn.1005-5185.2016.10.006[10] 李文婵, 姚稚明, 屈婉莹, 等. SUV小于2.5的孤立性肺结节18F-FDG PET/CT诊断价值初探[J].医学研究杂志, 2011, 40(9):47-51. DOI:10.3969/j.issn.1673-548X.2011.09.016.
Li WC, Yao ZM, Qu WY, et al. 18F-FDG PET/CT characterization of solitary pulmonary nodules with an initial average standard uptake value less than 2.5[J]. J Med Res, 2011, 40(9):47-51. doi: 10.3969/j.issn.1673-548X.2011.09.016[11] Schillaci O. Use of dual-point fluorodeoxyglucose imaging to enhance sensitivity and specificity[J]. Semin Nucl Med, 2012, 42(4):267-280. DOI:10.1053/j.semnuclmed.2012.02.003. [12] 姚稚明, 屈婉莹, 刘甫庚, 等. 18F-FDG PET/CT双时相显像对孤立性肺结节的诊断价值[J].中华核医学杂志, 2007, 27(1):5-7. DOI:10.3760/cma.j.issn.2095-2848.2007.01.002.
Yao ZM, Qu WY, Liu FG, et al. The clinical value of dual time point 18F-FDG PET/CT in diagnosis of solitary pulmonary nodule[J]. Chin J Nucl Med, 2007, 27(1):5-7. doi: 10.3760/cma.j.issn.2095-2848.2007.01.002[13] Li Y, Su M, Li F, et al. The value of 18F-FDG-PET/CT in the differential diagnosis of solitary pulmonary nodules in areas with a high incidence of tuberculosis[J]. Ann Nucl Med, 2011, 25(10):804-811. DOI:10.1007/s12149-011-0530-y. [14] De Wever W, Verschakelen J, Coolen J. Role of imaging in diagnosis, staging and follow-up of lung cancer[J]. Curr Opin Pulm Med, 2014, 20(4):385-392. DOI:10.1097/MCP. 0000000000000066. [15] Schillaci O. Use of dual-point fluorodeoxyglucose imaging to enhance sensitivity and specificity[J]. Semin Nucl Med, 2012, 42(4):267-280. DOI:10.1053/j.semnuclmed.2012.02.003. [16] 吴涛, 崔坤炜, 张娟, 等.双时相18F-FDG PET/CT显像对肺部病变良恶性的鉴别诊断价值[J].安徽医学, 2016, 37(11):1393-1396. DOI:10.3969/j.issn.1000-0399.2016.11.021.
Wu T, Cui KW, Zhang J, et al. Diagnostic value of Double-phase 18F-FDG PET/CT in benign and malignant pulmonary lesions[J].Anhui Med J, 2016, 37(11):1393-1396. doi: 10.3969/j.issn.1000-0399.2016.11.021[17] 娜仁花, 柴黎明, 居热提·阿扎提, 等. 11C-胆碱PET/CT显像在前列腺癌诊断中对18F-FDG的补充价值[J].中国临床医学影像杂志, 2016, 27(11):799-803. DOI:10.3969/j.issn.1008-1062.2016. 11.011.
Na RH, Chai LM, Jureti AZT, et al. Added value of 11C-choline PET/CT imaging to 18F-FDG PET/CT in primary prostate cancer[J]. J Chin Clin Med Imaging, 2016, 27(11):799-803. doi: 10.3969/j.issn.1008-1062.2016.11.011[18] 滕学鹏, 董伟, 刘立恒, 等. PET-CT 11C-胆碱和18F-FDG显像剂联合对肺占位病变鉴别诊断价值分析[J].中华肿瘤防治杂志, 2012, 19(15):1177-1179, 1183.
Teng XP, Dong W, Liu LH, et al. Joint value analysis of 11C-choline and 18F-FDG PET-CT in pulmonary occupying lesions diagnosis[J]. Chin J Cancer Prev Treat, 2012, 19(15):1177-1179, 1183.[19] 陶鑫, 赵志梅, 刘颖华, 等.孤立性肺结节HRCT征象概率分析的初步研究[J].现代诊断与治疗, 2009, 20(4):196-199. DOI:10.3969/j.issn.1001-8174.2009.04.002.
Tao X, Zhao ZM, Liu YH, et al. Preliminary study on probability analysis of HRCT features of solitary pulmonary nodules[J]. Mod Diagn Treat, 2009, 20(4):196-199. doi: 10.3969/j.issn.1001-8174.2009.04.002[20] Jeong SY, Lee KS, Shin KM, et al. Efficacy of PET/CT in the characterization of solid or partly solid solitary pulmonary nodules[J]. Lung Cancer, 2008, 61(2):186-194. DOI:10.1016/j.lungcan.2007.12.021. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 3109
- HTML全文浏览量: 2015
- PDF下载量: 6