


-
多层螺旋CT(multislice CT,MSCT)灌注扫描能准确反映组织微循环情况,对肿瘤良恶性鉴别、治疗效果和预后评估等均有重要的价值[1]。虽然获取时间-密度灌注曲线和灌注指标是MSCT灌注扫描后处理的基本操作,但是获取灌注参数之前,必须选定入选动脉和ROI。然而,如何选定入选动脉和ROI仍没有一致的观点[2-4],且该类研究在国内罕有报道。在国外有关腮腺肿瘤的少数研究中,通过对比颈内动脉(internal carotid artery,ICA)和颈外动脉(external carotid artery,ECA)作为入选动脉时的灌注参数值,推荐使用ICA作为入选动脉[2-3],而其他同类研究却未发现两者之间存在差异性[5]。此外,ROI采样面积的选择,可能因为ROI内组织较大的不均质性、存在临近血管的影响等而影响灌注结果[3-4],目前尚未对不同的ROI采样面积选择进行深入对比分析,以致ROI的大小是否影响灌注结果仍不明。因此,我们通过探讨不同入选动脉和ROI大小等对灌注参数的影响,明确其对腮腺肿瘤MSCT灌注扫描结果的影响,为以后类似灌注后处理分析提供更准确和科学的分析方法。
-
收集2015年1月至2016年5月在我科行腮腺肿瘤MSCT灌注扫描患者17例,在行灌注功能后处理前,剔除出现明显运动伪影2例、假牙伪影影响肿瘤层面图像2例和颈内动脉栓塞1例,最终共12例纳入研究,基本情况见表 1。其中,女性5例、男性7例,年龄30~64岁,平均年龄为(47.0±8.8)岁;12例患者中腺淋巴瘤5例、非腺淋巴瘤7例(其中,腮腺癌2例、多形性腺瘤3例、炎性淋巴结1例、Mikulicz病1例)。本研究经过佛山市第一人民医:伦理委员会委员批准。入选患者在实施灌注扫描前均签署了知情同意书。
病例编号 性别 年龄 病变位置 病理诊断 1 女 45 左侧腮腺 腮腺癌 2 女 44 左侧腮腺 多形性腺瘤 3 女 30 右侧腮腺 腮腺癌 4 女 31 左测腮腺 Mikulicz 5 男 47 双测腮腺 腺淋巴瘤 6 男 51 双测腮腺 腺淋巴瘤 7 男 35 右测腮腺 多形性腺瘤 8 男 59 左侧腮腺 腺淋巴瘤 9 男 56 双侧腮腺 腺淋巴瘤 10 男 44 左侧腮腺 炎性淋巴结 11 女 57 右侧腮腺 多形性腺瘤 12 男 64 左侧腮腺 腺淋巴瘤 表 1 12例入选腮腺肿瘤患者的基本情况
Table 1. Clinical data of 12 cases of parotid tumor patients
-
采用Philips公司256层Brilliance iCT扫描仪,所有患者行常规MSCT平扫后即行CT灌注扫描。灌注扫描层面包括腮腺全貌,高压注射器经右肘静脉快速注入20 mL生理盐水,然后注入40~60 mL对比剂(碘必乐300 mg I/mL),用20~30 mL生理盐水再次冲管,注射速度5 mL/s。注射对比剂后即开始动态容积扫描,扫描参数:80 kV、120 mA;11~35 s行动脉期间隔扫描;35~60 s行静脉期间隔扫描,间隔时间5 s;动态扫描获得15个容积数据,共375帧图像, 采集数据输入EBW后处理工作站。所有患者入选动脉选择均与腮腺病变同侧,当肿瘤为双侧腮腺同时发生者,选择病变较明显一侧进行研究。
-
使用Philips后处理工作站(EBW 4.5)自带的Perfusion软件进行数据处理,在所观察的层面分别选择与肿瘤同侧的ICA、ECA和颈总动脉(commoncarotid artery,CCA)作为入选动脉,肿瘤ROI选择为60 mm2,避开肿瘤坏死和囊变区以及邻近血管。自动获取灌注结果,记录肿瘤血流量(blood flow,BF)、血容量(blood volume,BV)和增强幅度(peakenhancement index,PEI)。在选择ECA作为入选动脉的基础上,分别记录采样面积为60 mm2、80%瘤体面积(S80%)和全瘤面积(S100%)共3种不同ROI时的BF(mL·min-1·100g-1)、BV(mL /100 g)和PEI(Hu)参数值。
-
采用SPSS13.0软件进行统计学分析。所有灌注参数值(BF、BV和PEI)均用“均数±标准差”表示。在肿瘤ROI不变的前提下,对比不同入选动脉所获得的灌注参数值;选定ECA为入选动脉后,对比不同ROI采样面积时获得的灌注参数值,不同组间灌注参数值(BF、BV和PEI)采用方差分析。对腺淋巴瘤和非腺淋巴瘤灌注参数进行正态分布和方差齐性检验后,采用t检验比较组间差异。P<0.05表示差异有统计学意义。
-
当肿瘤ROI采样面积固定为60 mm2,分别选取ECA、ICA和CCA为入选动脉时,BF、BV和PEI在各组之间的差异无统计学意义(F=0.012、0.007和0.233,均P>0.05),详见表 2。当选择ECA为入选动脉进行后处理分析,肿瘤ROI采样面积分别取60 mm2、S80%和S100%时,BF、BV和PEI在各组之间的差异亦无统计学意义(F=0.220、0.033和0.283,均P>0.05)(表 3)
入选动脉 BF/(mL·min-1·100g-1) BV/(mL/100 g) PEI/Hu ECA 54.88±30.45 29.83±15.44 51.53±18.39 ICA 50.09±26.70 26.39±8.210 52.07±18.54 CCA 51.74±27.06 28.35±12.44 52.44±19.09 F值 0.012 0.007 0.233 P值 0.914 0.993 0.793 注:表中,ECA:颈外动脉;ICA:颈内动脉;CCA:颈总动脉;BF:血流量;BV:血容量;PEI:增强幅度。 表 2 肿瘤ROI面积为60 mm2时不同入选动脉对灌注参数值的影响(x±s)
Table 2. Results of perfusion parameters on different input arteries selected(ROI: 60 mm2)(x±s)
ROI采样
面积BF/(mL·min-1·100g-1) BV/(mL/100 g) PEI/Hu 60 mm2 54.96±30.42 29.83±15.44 51.61±18.34 S80% 48.22±27.35 28.58±15.05 47.73±18.87 S100% 48.74±25.01 28.32±15.52 46.67±16.56 F值 0.220 0.033 0.283 P值 0.804 0.968 0.755 注:表中,BF:血流量;BV:血容量;PEI:增强幅度;S80%:80%瘤体面积;S100%:全瘤面积。 表 3 ECA为入选动脉时肿瘤不同ROI采样面积对灌注参数值的影响(x±s)
Table 3. Results of perfusion parameters in different size of ROI(external carotid artery was the input artery)(x±s)
-
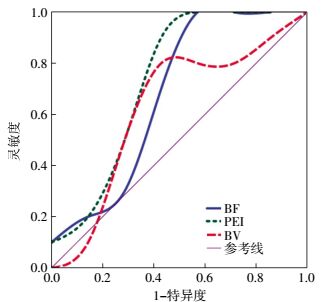
选择ECA为入选动脉、ROI取60mm2时,腺淋巴瘤组的BF和PEI均高于非腺淋巴瘤组,且两组之间的差异具有统计学意义(t=2.453和2.516,均P<0.05);而腺淋巴瘤组的BV虽然高于非腺淋巴瘤组,但两组之间的差异不具有统计学意义(t=0.428,P>0.05)(表 4)。表 5、图 1中的受试者工作特征曲线(receiveroperatingcharacteristiccurve,ROC)显示,在腺淋巴瘤诊断中,当BF取值为34.99mL·min-1·1 100 g-1时,诊断灵敏度达100%,而特异度最低(52.4%);总体上PEI对腺淋巴瘤具有较高的诊断效能,ROC曲线下面积为0.762,高于BF和BV;当PEI取值为41.53 Hu时,诊断腺淋巴瘤的灵敏度和特异度分别为86.7%和66.7%。图 2中的ROC曲线显示,选择ECA为入选动脉、ROI采样面积为S80%时,PEI诊断腺淋巴瘤的效能最高。
组别 例数 BF/
(mL·min-1·100 g-1)BV/
(mL/100 g)PEI/
Hu腺淋巴瘤组 5 61.50±18.99 30.05±12.92 57.85±14.10 非腺淋巴瘤组 7 42.88±29.62 28.09±16.45 42.11±15.32 t值 2.453 0.428 2.516 P值 0.040 0.700 0.030 注:表中,BF:血流量;BV:血容量;PEI:增强幅度。 表 4 腮腺腺淋巴瘤组与非腺淋巴瘤组BF、BV和PEI灌注参数值的对比分析
Table 4. Comparative analysis of blood flow, blood volume, andpeak enhancement index values of adenolymphoma and nonadenolymphoma
灌注参数 ROC曲线下面积 基准值 灵敏度/% 特异度/% BF 0.686 34.99 100.0 52.4 BV 0.616 23.87 066.7 71.4 PEI 0.762 41.53 086.7 66.7 注:表中,ROC:受试者工作特征曲线;BF:血流量;BV:血容量;PEI:增强幅度。 表 5 BF、BV和PEI对腺淋巴瘤的诊断效能分析
Table 5. Diagnostic efficiencies of blood flow, blood volume andpeak enhancement index for adenolymphoma diagnosis

图 1 入选动脉为ECA、病灶ROI采样面积为60 mm2时BF、BV和PEI对腺淋巴瘤的诊断效能(ROC曲线)图中, ECA:颈外动脉;BF:血流量;BV:血容量;PEI:增强幅度;ROC:受试者工作特征曲线。
Figure 1. Receiver operating characteristic curve of blood flow, blood volume and peak enhancement index with external carotidartery selected as input artery and ROI size of 60 mm2

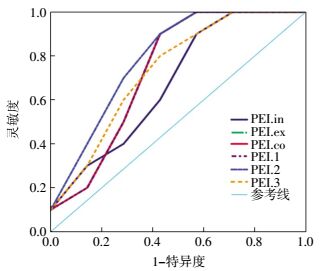
图 2 不同入选动脉和病灶ROI采样面积下PEI诊断效能(ROC曲线)图中, PEI.ex, PEI.co和PEI.1具有相同的诊断效能, 其ROC曲线重叠。In=ICA;ex=ECA;co=CCA;1:ROI=60 mm2;2:ROI=S80%;3:ROI=S100%;ROC:受试者工作特征曲线;ICA:颈内动脉;ECA:颈外动脉;CCA:颈总动脉;PEI:增强幅度。
Figure 2. Receiver operating characteristic curve of peak enhancement index with different input arteries and ROI sizes
-
MSCT灌注技术在头颈部肿瘤中的应用逐渐增多。目前,关于灌注后处理入选动脉的选择仍没有统一的观点。不同研究中ECA和ICA均有作为入选动脉进行灌注后处理分析,甚至在同一研究中亦有同时采用ECA和ICA作为入选动脉进行后处理,以获取BF、BV和PEI等灌注参数值的报道[2-3]。既往较多研究分别对ECA和ICA作为入选动脉而获取的灌注参数值进行对比分析,发现两者在BF、BV、平均通过时间和达峰时间等参数之间的差异并不具有统计学意义[2-4];但是Miracle等[2]和Tawfik等[3]建议选用ECA作为入选动脉,认为ECA管径较大,容易识别且垂直走行,能减少容积效应的影响。我们在ECA和ICA的基础上,加入了CCA进行对比研究,结果显示,在肿瘤ROI采样面积(60 mm2)相同的基础上,三者作为入选动脉所获取的BF、BV和PEI之间的差异均无统计学意义,这与以往的研究结果相符[2-3, 5]。但与ECA相比,CCA具有更大的管径且更容易识别。就本研究结果而言,笔者认为CCA作为入选动脉更适合,但应根据肿瘤所在位置和层面包括的血管断面进行选择。
我们针对腮腺肿瘤进行研究,对腺淋巴瘤组和非腺淋巴瘤组在肿瘤ROI采样面积一致的前提下,比较ECA、ICA和CCA作为入选动脉时PEI对腺淋巴瘤的诊断效能。结果显示,当ECA和CCA作为入选动脉时,PEI具有更高的诊断效能。因此,我们推测,对腮腺腺淋巴瘤的诊断或许选择ECA或CCA作为入选动脉更合适。
既往研究均提及,在勾画病灶的ROI时应避开囊变和坏死区以及邻近血管等组织,但就ROI采样面积而言,尚无统一的方法和建议[3, 5]。目前,ROI勾画多采用固定面积法和面积比例法。前者固定ROI的采样面积而不考虑肿瘤的大小,如Bisdas等[6]在腮腺灌注研究中选择ROI采样面积为40 mm2,Miracle等[2]的研究选择ROI采样面积为25~35 mm2。这种固定ROI采样面积的方法能精准获取研究者所需要的ROI。而在面积比例法中,王平仲等[7]认为ROI采样面积不应小于90%瘤体面积(S90%),而我们的既往研究[8]和Tawfik等[3]则认为,选择的ROI采样面积不应小于S80%。这种比例法勾画ROI采样面积的方法能更客观、准确地反映肿瘤整体的灌注情况。此外,尚有研究未对ROI勾画进行具体说明[9]。本研究结果显示,当入选动脉固定(ECA)时,病灶ROI分别取60 mm2、S80%和S100%,所得到的各灌注参数值(BF、BV和PEI)之间的差异无统计学意义。可见,如何选择ROI,以及ROI采样面积的大小可能不会影响腮腺肿瘤MSCT灌注结果,但仍需加大样本量进一步验证。
由于本研究中的肿瘤病灶无较大的囊变和坏死区,仅局部表现为小囊变,因此,不能评估当肿瘤病灶内存在较大囊变和坏死区、ROI面积取S80%和S100%时,是否会影响灌注参数值及其影响程度。这是本研究的不足之处。而我们在鉴别诊断腺淋巴瘤和非腺淋巴瘤中,病灶ROI均采样S80%时,PEI有较高的诊断效能,ROC曲线下面积为0.762。另外,对腺淋巴瘤组和非腺淋巴瘤组灌注参数进行对比分析发现,前者BF和PEI均高于后者,且差异具有统计学意义,这与以往研究结果相符[7-8]。该差异性主要原因可能是由于腺淋巴瘤组织含有丰富的毛细血管所致;而BV在腺淋巴瘤组较高,但两组之间的差异不具有统计学意义,这与以往研究结果不一致[8, 10]。我们认为,原因可能是由于本研究纳入样本量较小所致。
综上所述,MSCT灌注扫描在腮腺肿瘤的诊断和鉴别诊断中,入选动脉和病灶ROI选择对BF、BV和PEI等灌注参数值的影响差异均不具有统计学意义,可按实际情况自由选择。但本研究结果显示,在腺淋巴瘤的鉴别诊断中,选择ECA为入选动脉、ROI取S80%时,PEI具有较高的诊断效能。但由于本研究的纳入样本量较少,需要进一步增大样本量和多中心的深入研究。
腮腺肿瘤MSCT灌注扫描结果:入选动脉和病灶ROI选择的影响
MSCT perfusion of parotid tumor:the effect of arterial input and region of interest selection
-
摘要:
目的探讨入选动脉和病灶ROI选择对腮腺肿瘤多层螺旋CT(MSCT)灌注扫描结果的影响。 方法使用Philips ADW4.5工作站自带的灌注扫描软件对12例腮腺肿瘤患者进行MSCT灌注后处理分析。记录选择不同入选动脉和病灶ROI时的血流量(BF)、血容量(BV)和增强幅度(PEI)等灌注参数;采用方差分析法分析并比较上述各组参数值;采用独立样本t检验比较腺淋巴瘤和非腺淋巴瘤灌注参数之间的差异性。 结果选取颈外动脉(ECA)、颈内动脉(ICA)和颈总动脉(CCA)为入选动脉时,BF、BV和PEI值在各组之间的差异无统计学意义(F=0.012、0.007和0.233,均P>0.05);当肿瘤取不同面积ROI时,上述各灌注参数值之间的差异同样不具有统计学意义(F=0.220、0.033和0.283,均P>0.05)。选择ECA作为入选动脉、ROI为80%瘤体面积(S80%)时,PEI对腺淋巴瘤的鉴别诊断效能最高。 结论入选动脉和病灶ROI的大小对腮腺肿瘤灌注结果无明显影响;但选择ECA作为入选动脉、ROI取S80%可能有助于提高腮腺腺淋巴瘤的诊断效能。 -
关键词:
- 腮腺肿瘤 /
- 腺淋巴瘤 /
- 体层摄影术, 螺旋计算机 /
- 感兴趣区
Abstract:ObjectiveTo evaluate the effect of arterial input and ROI selection on the perfusion CT parameters of parotid tumors. MethodsA deconvolution-based software(Philips ADW4.5) was used to perform perfusion calculations on 12 parotid tumor patients. Blood flow(BF), blood volume(BV), and peak enhancement index(PEI) of different arterial inputs and ROI selection were recorded. These values were compared using one-way ANOVA. Independent sample t-test was performed to compare the values of adenolymphoma and non-adenolymphoma. ResultsNo significant difference was observed among BF, BV, and PEI obtained when external carotid artery(ECA), internal carotid artery(ICA), and common carotid artery(CCA) were used as input arteries(F=0.012, 0.007 and 0.233, all P>0.05). Similarly, no significant difference was observed among the perfusion parameters of different ROIs of lesions(F=0.220, 0.033, and 0.283, all P>0.05). When ECA was selected as arterial input, the area of ROI was approximately S80%, and PEI had the best diagnostic effect for adenolymphoma differential diagnosis. ConclusionsArterial input selection and area of ROI had no significant effect on perfusion CT calculation of parotid tumor. However, ECA and S80% of ROI selected for perfusion post-processing might facilitate parotid adenolymphoma diagnosis. -
Key words:
- Parotid neoplasms /
- Adenolymphoma /
- Tomography, spiral computed /
- Region of interest
-
图 1 入选动脉为ECA、病灶ROI采样面积为60 mm2时BF、BV和PEI对腺淋巴瘤的诊断效能(ROC曲线)图中, ECA:颈外动脉;BF:血流量;BV:血容量;PEI:增强幅度;ROC:受试者工作特征曲线。
Figure 1. Receiver operating characteristic curve of blood flow, blood volume and peak enhancement index with external carotidartery selected as input artery and ROI size of 60 mm2
图 2 不同入选动脉和病灶ROI采样面积下PEI诊断效能(ROC曲线)图中, PEI.ex, PEI.co和PEI.1具有相同的诊断效能, 其ROC曲线重叠。In=ICA;ex=ECA;co=CCA;1:ROI=60 mm2;2:ROI=S80%;3:ROI=S100%;ROC:受试者工作特征曲线;ICA:颈内动脉;ECA:颈外动脉;CCA:颈总动脉;PEI:增强幅度。
Figure 2. Receiver operating characteristic curve of peak enhancement index with different input arteries and ROI sizes
表 1 12例入选腮腺肿瘤患者的基本情况
Table 1. Clinical data of 12 cases of parotid tumor patients
病例编号 性别 年龄 病变位置 病理诊断 1 女 45 左侧腮腺 腮腺癌 2 女 44 左侧腮腺 多形性腺瘤 3 女 30 右侧腮腺 腮腺癌 4 女 31 左测腮腺 Mikulicz 5 男 47 双测腮腺 腺淋巴瘤 6 男 51 双测腮腺 腺淋巴瘤 7 男 35 右测腮腺 多形性腺瘤 8 男 59 左侧腮腺 腺淋巴瘤 9 男 56 双侧腮腺 腺淋巴瘤 10 男 44 左侧腮腺 炎性淋巴结 11 女 57 右侧腮腺 多形性腺瘤 12 男 64 左侧腮腺 腺淋巴瘤  下载: 导出CSV
下载: 导出CSV
表 2 肿瘤ROI面积为60 mm2时不同入选动脉对灌注参数值的影响(x±s)
Table 2. Results of perfusion parameters on different input arteries selected(ROI: 60 mm2)(x±s)
入选动脉 BF/(mL·min-1·100g-1) BV/(mL/100 g) PEI/Hu ECA 54.88±30.45 29.83±15.44 51.53±18.39 ICA 50.09±26.70 26.39±8.210 52.07±18.54 CCA 51.74±27.06 28.35±12.44 52.44±19.09 F值 0.012 0.007 0.233 P值 0.914 0.993 0.793 注:表中,ECA:颈外动脉;ICA:颈内动脉;CCA:颈总动脉;BF:血流量;BV:血容量;PEI:增强幅度。
下载: 导出CSV
表 3 ECA为入选动脉时肿瘤不同ROI采样面积对灌注参数值的影响(x±s)
Table 3. Results of perfusion parameters in different size of ROI(external carotid artery was the input artery)(x±s)
ROI采样
面积BF/(mL·min-1·100g-1) BV/(mL/100 g) PEI/Hu 60 mm2 54.96±30.42 29.83±15.44 51.61±18.34 S80% 48.22±27.35 28.58±15.05 47.73±18.87 S100% 48.74±25.01 28.32±15.52 46.67±16.56 F值 0.220 0.033 0.283 P值 0.804 0.968 0.755 注:表中,BF:血流量;BV:血容量;PEI:增强幅度;S80%:80%瘤体面积;S100%:全瘤面积。
下载: 导出CSV
表 4 腮腺腺淋巴瘤组与非腺淋巴瘤组BF、BV和PEI灌注参数值的对比分析
Table 4. Comparative analysis of blood flow, blood volume, andpeak enhancement index values of adenolymphoma and nonadenolymphoma
组别 例数 BF/
(mL·min-1·100 g-1)BV/
(mL/100 g)PEI/
Hu腺淋巴瘤组 5 61.50±18.99 30.05±12.92 57.85±14.10 非腺淋巴瘤组 7 42.88±29.62 28.09±16.45 42.11±15.32 t值 2.453 0.428 2.516 P值 0.040 0.700 0.030 注:表中,BF:血流量;BV:血容量;PEI:增强幅度。
下载: 导出CSV
表 5 BF、BV和PEI对腺淋巴瘤的诊断效能分析
Table 5. Diagnostic efficiencies of blood flow, blood volume andpeak enhancement index for adenolymphoma diagnosis
灌注参数 ROC曲线下面积 基准值 灵敏度/% 特异度/% BF 0.686 34.99 100.0 52.4 BV 0.616 23.87 066.7 71.4 PEI 0.762 41.53 086.7 66.7 注:表中,ROC:受试者工作特征曲线;BF:血流量;BV:血容量;PEI:增强幅度。
下载: 导出CSV
-
[1] Mazzei MA, Preda L, Cianfoni A, et al. CT perfusion:technical developments and current and future applications[J/OL]. Biomed Res Int, 2015, 2015:397521[2017-02-17]. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4324810.DOI:10.1155/2015/397521" target="_blank">10.1155/2015/397521">https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4324810.DOI:10.1155/2015/397521. [2] Miracle AC, Rezaei A, Gandhi D, et al. CT perfusion of the neck:internal carotid artery versus external carotid artery as the reference artery[J]. AJNR Am J Neuroradiol, 2009, 30(8):1598-1601. DOI:10.3174/ajnr.A1531. [3] Tawfik AM, Razek AA, Elsorogy LG, et al. Perfusion CT of head and neck cancer:effect of arterial input selection[J]. AJR Am J Roentgenol, 2011, 196(6):1374-1380. DOI:10.2214/AJR.10.5343. [4] Petralia G, Preda L, Raimondi S, et al. Intra-and interobserver agreement and impact of arterial input selection in perfusion CT measurements performed in squamous cell carcinoma of the upper aerodigestive tract[J]. AJNR Am J Neuroradiol, 2009, 30(6):1107-1115. DOI:10.3174/ajnr.A1540. [5] Rumboldt Z, Al-Okaili, Deveikis JP. Perfusion CT for head and neck tumors:pilot study[J]. AJNR Am J Neuroradiol, 2005, 26(5):1178-1185. [6] Bisdas S, Baghi M, Wagenblast J, et al. Differentiation of benign and malignant parotid tumors using deconvolution-based perfusion CT imaging:feasibility of the method and initial results[J]. Eur J Radiol, 2007, 64(2):258-265. DOI:10.1016/j.ejrad.2007.02.032. [7] 王平仲, 余强, 石慧敏, 等. CT灌注诊断腮腺肿瘤的临床价值评价[J].上海口腔医学, 2005, 14(6):573-577. DOI:10.3969/j.issn.1006-7248.2005.06.006.
Wang PZ, Yu Q, Shi HM, et al. Diagnostic value of CT perfusion for parotid gland tumors[J]. Shanghai J Stomatol, 2005, 14(6):573-577. doi: 10.3969/j.issn.1006-7248.2005.06.006[8] Xu ZF, Rong F, Yu T, et al. Pleomorphic adenoma versus warthin tumor of the parotid gland:diagnostic value of CT perfusion imaging and its pathologic explanation[J]. J Tumor, 2016, 4(2):419-425. DOI:10.17554/j.issn.1819-6187.2016.04.74. [9] Dong Y, Lei GW, Wang SW, et al. Diagnostic value of CT perfusion imaging for parotid neoplasms[J/OL]. Dentomaxillofac Radiol, 2014, 43(1):20130237[2017-02-17]. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3887482.DOI:10.1259/dmfr.20130237" target="_blank">10.1259/dmfr.20130237">https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3887482.DOI:10.1259/dmfr.20130237. [10] Sumi M, Van Cauteren M, Sumi T, et al. Salivary gland tumors:use of intravoxel incoherent motion MR imaging for assessment of diffusion and perfusion for the differentiation of benign from malignant tumors[J]. Radiology, 2012, 263(3):770-777. DOI:10. 1148/radiol. 12111248. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 2898
- HTML全文浏览量: 1824
- PDF下载量: 2