


 下载:
下载:
-
随着我国人口的老龄化,60岁以上人群骨质疏松症总患病率明显升高,尤其是老年绝经后女性[1-3]。胸腰椎椎体压缩性骨折是骨质疏松症较为常见且严重的后果之一。一旦发生椎体压缩性骨折,将会对患者的生活及经济状况造成明显的影响,包括较高的病死率、持续的背部疼痛、生活质量的下降以及较高的医疗费用支出等。因此,对椎体压缩性骨折进行积极预防以及早期诊断具有重要的临床意义。在近几年的研究中,全身骨显像在骨质疏松症和良恶性椎体骨折、新鲜椎体与陈旧椎体的鉴别诊断中显现了一定的价值[4]。Ap Dafydd等[5]报道了用骨显像与MRI诊断急性、亚急性及陈旧性骨折的一致性为63%,且两者在经皮穿刺椎体成形术及椎体球囊扩张后凸成形术前具有指导意义。目前关于骨显像在骨质疏松性椎体骨折的治疗方案选择方面的应用价值研究尚少。我们回顾性分析了2012年11月至2016年10月因骨质疏松导致的压缩性骨折而就诊于我院的81例绝经后女性,评估99Tcm-MDPSPECT/CT骨显像及其半定量分析指标在绝经后女性骨质疏松性胸腰椎椎体压缩性骨折临床治疗方案的选择中的增益价值。
-
选取2012年11月至2016年10月因轻微外伤或日常活动导致胸腰背部疼痛而就诊于我院,最终诊断为骨质疏松性胸腰椎椎体压缩性骨折的绝经后女性患者81例,年龄49~91岁,平均年龄(71.86±9.59)岁,平均绝经时间(22.41±10.01)年。通过骨密度测定、外科手术、胸腰椎MRI、胸腰椎X射线检查或随访证实为骨质疏松引起的椎体压缩性骨折,并排除其他器质性病变包括肿瘤、炎症、结核等。本研究经本院医学伦理委员会批准。所有患者或其家属均于检查前签署了知情同意书。
-
采用SIEMENS公司生产的Symbia T 16型双探头SPECT/CT检查仪进行骨显像。肘静脉注射99Tcm-MDP 740~1110 MBq后3 h排空膀胱,行全身骨显像及局部SPECT/CT断层融合显像,采用低能高分辨率准直器。全身图像以双探头前后位采集,采集速度为13 cm/min;局部SPECT/CT断层融合图像以病灶部位为中心,先采集SPECT断层图像,然后采集CT图像,再利用专用软件进行图像融合。
-
所有图像均由2名具有副主任医师职称以上的核医学医师独立对图像进行诊断分析,只有二者诊断意见一致时方可认为资料有效;二者意见不一致时,则视为资料无效。首先观察全身图像中出现较均一放射性核素浓聚的椎体个数,再在同机CT融合图像中根据核素浓集部位定位骨折椎体节段。同时在CT图像中观察椎体形态,包括压缩变、双凹变以及楔形变,观察椎体是否存在成骨性或溶骨性改变以及椎体周围脓肿等征象,并结合临床病史鉴别椎体肿瘤及椎体感染性骨病变。利用ROI技术在矢状位断层图像上勾画病灶椎体(T)及与其相邻的正常椎体(NT),测量二者的放射性计数并计算比值,即T/NT值,分别勾画3次,取3次测量值的平均值。
-
将所收集病例根据椎体是否在99Tcm-MDPSPECT/CT骨显像后进行手术分成两组,一组为手术组,包括行经皮穿刺椎体成形术及椎体球囊后凸成形术的患者,另一组为非手术组。
-
使用SPSS19.0统计学软件分析数据,原始数据均服从正态分布和方差齐性。采用两独立样本t检验进行手术组与非手术组骨折椎体半定量指标T/NT值总体均数比较,P<0.05为差异有统计学意义。
-
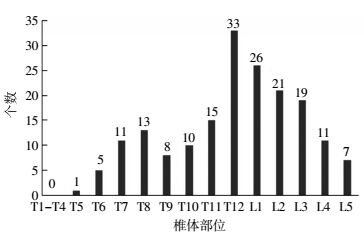
所有81例患者中共检出180个胸腰椎椎体骨折,其中以第12胸椎最常见,共33个(18.33%,33/180);其次为第1腰椎,共26个(14.44%,26/180);之后为第2腰椎、第3腰椎及第11胸椎,所占比例分别为11.66%(21/180)、10.55%(19/180)、8.33%(15/180)(图 1)。

图 1 绝经后女性骨质疏松患者180个胸腰椎椎体压缩性骨折分布
Figure 1. Distribution of 180 fragile fractures of thoracic and lumbarvertebrae in postmenopausal women with osteoporosis
在所有骨折椎体中,手术组椎体骨折110个,T/NT值为2.44±0.84;非手术组椎体骨折70个,T/NT值为1.04±0.14,两组间差异具有统计学意义(t=13.654,P<0.05)。在所有骨折椎体中,单发椎体骨折为36例(图 2),而多发椎体骨折为45例(图 3)
另外还发现椎体以外骨折,包括肋骨骨折29例(图 4)、椎体附件骨折2例、骶骨骨折2例、耻骨骨折1例。经过随访证实手术组患者大多数取得了不错的治疗效果,尤其以背部疼痛缓解明显,而非手术组患者经过保守治疗后症状也得到了相应改善。

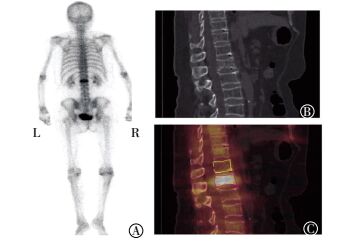
图 2 单发椎体压缩性骨折99Tcm-MDP SPECT/CT骨显像图像。患者女性, 55岁, 无诱因腰部疼痛不适3 d, 变换体位时加重, 诊断为野重度骨质疏松、第1腰椎压缩性骨折冶。入:行野经皮椎体成形术冶后症状明显缓解。图中, A:99TcmMDP骨显像全身后位图, 可见第1腰椎椎体显像剂均匀性分布浓聚影;B:同机CT断层图, 可见第1腰椎椎体双凹性改变;C:99Tcm-MDP SPECT/CT融合图, 黄色线条勾画椎体为病灶椎体邻近椎体第12胸椎, 红色线条勾画椎体为病灶椎体第1腰椎, 病灶椎体与邻近椎体的放射性计数比值T/NT值为3.45。
Figure 2. Images of single vertebral compression fracture with 99TcmMDP SPECT/CT bone imaging

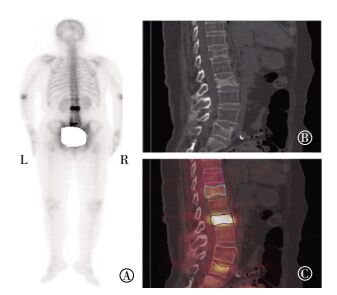
图 3 多发椎体压缩性骨折99Tcm-MDP SPECT/CT骨显像图像。患者女性, 63岁, 腰背部疼痛伴活动受限, 近日逐渐加重。对第2、5腰椎行野经皮椎体成形术冶, 术后症状明显缓解。图中, A:99Tcm-MDP骨显像全身后位图, 可见第12胸椎显像剂分布轻度增高, 第2腰椎均匀性显像剂浓聚影, 第5腰椎局部均匀性显像剂浓聚影;B:同机CT断层矢状位图, 可见第12胸椎及第2、5腰椎压缩性改变;C:99Tcm-MDPSPECT/CT融合图, 可见第12胸椎显像剂轻度增高, 第2、5腰椎均匀性显像剂浓聚影, 粉红色、墨绿色及橙色线条勾画椎体为病灶邻近的正常椎体, 分别对应为第11胸椎及第1、4腰椎, 浅蓝色、深蓝色及深红色线条勾画椎体为病灶椎体, 分别对应为第12胸椎及第2、5腰椎;第12胸椎及第2、5腰椎与邻近椎体的放射性计数比值T/NT值分别为1.08、5.22及1.68。
Figure 3. Images of multiple vertebral compression fractures with99Tcm-MDP SPECT/CT bone imaging

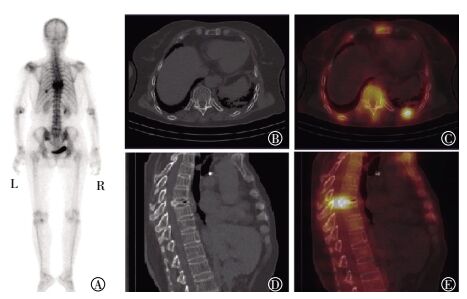
图 4 椎体压缩性骨折合并肋骨骨折99Tcm-MDP SPECT/CT骨显像图像。患者女性, 66岁, 诊断为第8胸椎重度压缩性骨折伴左侧第9后肋骨折。图中, A:99Tcm-MDP骨显像全身后位图, 可见第8腰椎均匀性显像剂浓聚影, 左侧第9后肋点状显像剂浓聚影;B:同机CT断层图, 可见左侧第9后肋骨皮质中断不连续;C:99Tcm-MDP SPECT/CT融合图, 可见左侧第9后肋骨皮质中断伴显像剂分布浓聚;D:同机CT断层矢状位图, 可见第8胸椎椎体重度压缩变扁, 骨皮质尚完整, 并可见气体影;E:99Tcm-MDP SPECT/CT矢状位融合图, 可见第8胸椎椎体中后柱显像剂分布明显浓聚。
Figure 4. Images of vertebral compression fracture combined with rib fracture with99Tcm-MDP SPECT/CT bone imaging
-
本研究结果显示,在所有绝经后骨质疏松患者中发生的胸腰椎椎体骨折主要以第12胸椎及第1腰椎为主,这与Wang等[6]的研究结果一致,最主要的原因可能与第12胸椎及第1腰椎界于灵活度差与灵活度高的椎体之间有关。此结果提示,在临床上如果患者仅是低位椎体疼痛也应给予足够的重视,明确其是否合并第12胸椎及第1腰椎椎体骨折。
在临床上,绝经后女性骨质疏松患者椎体发生压缩性骨折时的治疗方案选择存在较大的差异。陈旧椎体骨折不伴有任何症状时无需特殊的治疗,但已有椎体骨折的患者发生再次椎体骨折的概率将大大升高[6-7],因此对于这部分患者需要积极干预骨质疏松,预防椎体再次骨折。而对于急性和亚急性椎体骨折伴或不伴有明显腰背部疼痛的患者的治疗方式主要包括经皮椎体成形术、经皮椎体后凸成形术、经皮椎体球囊扩张成形术[8-9]。因此,椎体压缩性骨折治疗前的评估具有重要意义。
MRI检查是临床常用的诊断椎体压缩性骨折的影像学方法,能够更好地了解椎体压缩性骨折发生时是否存在椎间盘、脊髓、韧带等病变[10]。但对于年龄较大的患者,有时会由于身体内安放有金属支架、心脏起搏器、不能承受MRI检查时的噪音等原因而不能进行[11]。而99Tcm-MDP SPECT/CT骨显像不受这些因素影响,并可在显示椎体压缩性骨折的同时,一次性地显示全身骨骼代谢及解剖结构。99Tcm-MDP SPECT/CT骨显像主要与骨相应部位的血流供应情况、代谢活跃程度等因素有关。椎体压缩性骨折的骨组织局部血流量增加、骨盐代谢旺盛以及成骨细胞功能增强,可聚集相对多的显像剂,典型骨显像图像表现为压缩性较均一的异常显像剂浓聚,在SPECT/CT断层图像上表现为椎体高度减低、形态失常,包括椎体压缩性改变、楔形变以及双凹变,不伴骨质破坏。本研究结果发现,110个骨扫描后行手术治疗的骨折椎体的T/N值明显高于70个未行手术治疗的骨折椎体。Ap Dafydd等[5]在回顾性研究中将骨折椎体对99Tcm-MDP的摄取分为轻度摄取、中度摄取以及明显摄取,结果发现在所有最终经过手术治疗的65例压缩性骨折患者中有56例为99Tcm-MDP中度摄取及明显摄取,即中度摄取及明显摄取的压缩性骨折椎体占全部手术治疗患者的86%。因此,对绝经后女性骨质疏松性椎体骨折尤其是不能行MRI检查的患者,99Tcm-MDP SPECT/CT骨显像提供了很好的影像学资料,对临床具有一定的参考价值。
此外,99Tcm-MDP SPECT/CT全身骨显像还可以发现胸腰椎椎体骨折以外其他部位同时存在的骨折,包括肋骨骨折、骶骨骨折以及椎体附件骨折等。有研究表明,骨质疏松性椎体压缩性骨折合并肋骨骨折是引起持续胸痛的主要原因[12-13]。因此对于绝经后女性骨质疏松患者发生椎体骨折时要注意是否合并上述部位的骨折,而常规胸腰椎平片、CT以及MRI往往会忽略这点。99Tcm-MDP SPECT/CT全身骨显像能够有效地诊断全身骨骼疾病,发现椎体以外的病变,具有灵敏度高、定位准确、价格便宜等优点,且与胸腰椎平片、CT以及MRI相比在诊断全身骨骼疾病方面存在明显的优势[11]。Masala等[14]研究发现,99Tcm-MDP骨显像与MRI对4个月以内椎体骨折的诊断具有较好的一致性,但是对于超过4个月的椎体骨折99Tcm-MDP骨显像具有较高的准确率。原因是放射性核素摄取在骨折椎体上最高可存在12个月之久。99Tcm-MDP骨显像是一项通过放射性摄取对骨质疏松椎体病变作出高灵敏度、功能性、定量分析的检查。放射性摄取反映了骨转化过程,标志着骨折愈合过程。且随着99Tcm-MDP骨显像同机融合CT的应用,一次显像可同时显示功能图像与解剖图像,可直观地观察椎体形态、密度、骨质变化等内容,较单纯全身骨显像提高了诊断准确率。
综上所述,本研究结果提示99Tcm-MDP SPECT/CT全身骨显像及其半定量分析在绝经后女性骨质疏松性胸腰椎骨折椎体治疗方案的选择方面具有一定的临床指导意义,与此同时还能够及时发现其他部位是否合并骨折。但临床上椎体骨折是否需要手术治疗,不仅需要参考影像学检查结果,包括99Tcm-MDP SPECT/CT以及MRI等,还要综合考虑年龄、是否合并严重心肺疾病、是否合并严重的腰背部疼痛等客观因素,以及不可预知的主观因素等。因此,后续我们将扩大研究病例数,结合其他因素进一步研究99Tcm-MDP SPECT/CT全身骨显像及其定量分析指标的临床指导意义。
99Tcm-MDP SPECT/CT骨显像在绝经后女性骨质疏松性胸腰椎椎体骨折中的增益价值
Incremental values of 99Tcm-MDP bone scan in postmenopausal women with osteoporotic thoracolumbar vertebral fractures
-
摘要:
目的研究99Tcm-MDP SPECT/CT骨显像及其半定量分析指标在绝经后女性骨质疏松性胸腰椎椎体骨折中的增益价值。 方法回顾性分析2012年11月至2016年10月因轻微外伤或日常活动导致胸腰背部疼痛而就诊,最终诊断为骨质疏松性胸腰椎椎体压缩性骨折的绝经后女性患者81例。选取SPECT/CT矢状位融合断层图像,利用ROI技术重复勾画病灶椎体(T)及与其相邻的正常椎体(NT),并计算病灶椎体与正常椎体的放射性计数比值,即T/NT值。将所收集病例根据椎体是否在99Tcm-MDP SPECT/CT骨显像后进行手术分成两组,一组为手术组,包括行经皮穿刺椎体成形术及椎体球囊后凸成形术的患者,另一组为非手术组。对两组T/NT值采用两独立样本t检验进行统计学分析。 结果(1)手术组共计110个椎体,T/NT值为2.44±0.84;非手术组共计70个椎体,T/NT值为1.04±0.14,两组T/NT值的差异有统计学意义(t=13.654,P < 0.05)。(2)发现椎体以外骨折,包括肋骨骨折29例、椎体附件骨折2例、骶骨骨折2例、耻骨骨折1例。 结论99Tcm-MDP SPECT/CT骨显像及其半定量分析指标在指导绝经后女性骨质疏松性胸腰椎椎体压缩性骨折临床治疗方案的选择和其他部位是否有骨折的诊断中具有一定的参考价值。 -
关键词:
- 骨质疏松, 绝经后 /
- 胸椎 /
- 腰椎 /
- 99m锝美罗酸盐 /
- 体层摄影术, 发射型计算机, 单光子 /
- 体层摄影术, X线计算机 /
- 椎体骨折
Abstract:ObjectiveTo assess incremental values of 99Tcm-MDP SPECT/CT bone scan imaging by semi-quantitative analysis indexes for osteoporotic thoracolumbar vertebral fractures in postmenopausal women. MethodsThis retrospective study enrolled 81 postmenopausal women patients diagnosed and treated for back pain from November 2012 to October 2016. All patients were diagnosed with osteoporotic thoracolumbar vertebral compression fractures. All patients underwent 99Tcm-MDP SPECT/CT bone imaging, and techniques for ROI were repeatedly applied to draw sagittal imaging sites of regional uptake in ROI, to record the number of radioactive counting of lesions (T) and adjacent normal vertebral sagittal imaging (NT), and to calculate T/NT ratio. Patients were divided into two groups. One group was treated by vertebroplasty or kyphoplasty after 99Tcm-MDP SPECT/CT bone imaging, and the other was treated with conservative treatment. T/NT ratios of the two groups were statistically analyzed. ResultsA total of 110 vertebral fractures were treated by vertebroplasty or kyphoplasty after 99Tcm-MDP SPECT/CT bone imaging, and 70 vertebral fractures were treated with conservative treatment. T/NT ratio of fractures reached 2.44±0.84 and 1.04±0.14, respectively (t=13.654, P < 0.05), after treatment with vertebroplasty or kyphoplasty; and conservative treatment. Some concurrent lesions which were absent in X-ray or MRI were detected by SPECT/CT, for example, 29 rib fractures and 2 sacrum fractures. Conclusion99Tcm-MDP SPECT/CT bone imaging by semi-quantitative analysis can effectively guide treatment of vertebral compression fractures. -
图 1 绝经后女性骨质疏松患者180个胸腰椎椎体压缩性骨折分布
Figure 1. Distribution of 180 fragile fractures of thoracic and lumbarvertebrae in postmenopausal women with osteoporosis
图 2 单发椎体压缩性骨折99Tcm-MDP SPECT/CT骨显像图像。患者女性, 55岁, 无诱因腰部疼痛不适3 d, 变换体位时加重, 诊断为野重度骨质疏松、第1腰椎压缩性骨折冶。入:行野经皮椎体成形术冶后症状明显缓解。图中, A:99TcmMDP骨显像全身后位图, 可见第1腰椎椎体显像剂均匀性分布浓聚影;B:同机CT断层图, 可见第1腰椎椎体双凹性改变;C:99Tcm-MDP SPECT/CT融合图, 黄色线条勾画椎体为病灶椎体邻近椎体第12胸椎, 红色线条勾画椎体为病灶椎体第1腰椎, 病灶椎体与邻近椎体的放射性计数比值T/NT值为3.45。
Figure 2. Images of single vertebral compression fracture with 99TcmMDP SPECT/CT bone imaging
图 3 多发椎体压缩性骨折99Tcm-MDP SPECT/CT骨显像图像。患者女性, 63岁, 腰背部疼痛伴活动受限, 近日逐渐加重。对第2、5腰椎行野经皮椎体成形术冶, 术后症状明显缓解。图中, A:99Tcm-MDP骨显像全身后位图, 可见第12胸椎显像剂分布轻度增高, 第2腰椎均匀性显像剂浓聚影, 第5腰椎局部均匀性显像剂浓聚影;B:同机CT断层矢状位图, 可见第12胸椎及第2、5腰椎压缩性改变;C:99Tcm-MDPSPECT/CT融合图, 可见第12胸椎显像剂轻度增高, 第2、5腰椎均匀性显像剂浓聚影, 粉红色、墨绿色及橙色线条勾画椎体为病灶邻近的正常椎体, 分别对应为第11胸椎及第1、4腰椎, 浅蓝色、深蓝色及深红色线条勾画椎体为病灶椎体, 分别对应为第12胸椎及第2、5腰椎;第12胸椎及第2、5腰椎与邻近椎体的放射性计数比值T/NT值分别为1.08、5.22及1.68。
Figure 3. Images of multiple vertebral compression fractures with99Tcm-MDP SPECT/CT bone imaging
图 4 椎体压缩性骨折合并肋骨骨折99Tcm-MDP SPECT/CT骨显像图像。患者女性, 66岁, 诊断为第8胸椎重度压缩性骨折伴左侧第9后肋骨折。图中, A:99Tcm-MDP骨显像全身后位图, 可见第8腰椎均匀性显像剂浓聚影, 左侧第9后肋点状显像剂浓聚影;B:同机CT断层图, 可见左侧第9后肋骨皮质中断不连续;C:99Tcm-MDP SPECT/CT融合图, 可见左侧第9后肋骨皮质中断伴显像剂分布浓聚;D:同机CT断层矢状位图, 可见第8胸椎椎体重度压缩变扁, 骨皮质尚完整, 并可见气体影;E:99Tcm-MDP SPECT/CT矢状位融合图, 可见第8胸椎椎体中后柱显像剂分布明显浓聚。
Figure 4. Images of vertebral compression fracture combined with rib fracture with99Tcm-MDP SPECT/CT bone imaging
-
[1] 中华医学会骨质疏松和骨矿盐疾病分会.原发性骨质疏松症诊治指南(2011年)[J].中华骨质疏松和骨矿盐疾病杂志, 2011, 4(1):2-17. DOI:10.3969/j.issn.1674-2591.2011.01.002.
Chinese Society of Osteoporosis and Bone Mineral Reseasch. The guidelines for diagnosis and treatment of primary osteoporosis(2011)[J]. Chin J Osteoporosis & Bone Miner Res, 2011, 4(1):2-17. doi: 10.3969/j.issn.1674-2591.2011.01.002[2] Gerdhem P. Osteoporosis and fragility fractures:Vertebral fractures[J]. Best Pract Res Clin Rheumatol, 2013, 27(6):743-755. DOI:10.1016/j.berh.2014.01.002. [3] Bazzocchi A, Spinnato P, Fuzzi F, et al. Vertebral fracture assessment by new dual-energy X-ray absorptiometry[J]. Bone, 2012, 50(4):836-841. DOI:10.1016/j.bone.2012.01.018. [4] Zhang Y, Shi H, Cheng D, et al. Added value of SPECT/spiral CT versus SPECT in diagnosing solitary spinal lesions in patients with extraskeletal malignancies[J]. Nucl Med Commun, 2013, 34(5):451-458. DOI:10.1097/MNM.0b013e32835fa552. [5] Ap Dafydd D, Salem S, Zerizer I, et al. The value of combined assessment of vertebral fractures with 99Tcm MDP scintigraphy and MRI in selecting and planning percutaneous vertebroplasty[J]. Nucl Med Commun, 2014, 35(7):755-761. DOI:10.1097/MNM.0000000000000110. [6] Wang H, Li C, Xiang Q, et al. Epidemiology of spinal fractures among the elderly in Chongqing, China[J]. Injury, 2012, 43(12):2109-2116. DOI:10.1016/j.injury.2012.04.008. [7] Black DM, Rosen CJ. Postmenopausal osteoporosis[J]. N Engl J Med, 2016, 374(21):2096-2097. DOI:10.1056/NEJMc1602599. [8] Mattie R, Laimi K, Yu S, et al. Comparing percutaneous vertebroplasty and conservative therapy for treating osteoporotic compression fractures in the thoracic and lumbar spine:a systematic review and Meta-Analysis[J]. J Bone Joint Surg Am, 2016, 98(12):1041-1051. DOI:10.2106/JBJS.15.00425. [9] Suzuki N, Ogikubo O, Hansson T. Previous vertebral compression fractures add to the deterioration of the disability and quality of life after an acute compression fracture[J]. Eur Spine J, 2010, 19(4):567-574. DOI:10.1007/s00586-009-1162-y. [10] Cahueque M, Cobar A, Zuñiga C, et al. Management of burst fractures in the thoracolumbar spine[J]. J Orthop, 2016, 13(4):278-281. DOI:10.1016/j.jor.2016.06.007. [11] Iqbal B, Currie GM, Wheat JM, et al. The incremental value of SPECT/CT in characterizing solitary spine lesions[J]. J Nucl Med Technol, 2011, 39(3):201-207. DOI:10.2967/jnmt.111.088351. [12] Jun DS, An BK, Yu CH, et al. Practical use of bone scan in patients with an osteoporotic vertebral compression fracture[J]. J Korean Med Sci, 2015, 30(2):194-198. DOI:10.3346/jkms.2015.30.2.194. [13] Barrett-Connor E, Nielson CM, Orwoll E, et al. Epidemiology of rib fractures in older men:Osteoporotic Fractures in Men(MrOS) prospective cohort study[J/OL]. BMJ, 2010, 340:c1069[2017-01-04]. http://www.bmj.com/content/340/bmj.c1069.long.DOI:10.1136/bmj.c1069" target="_blank">10.1136/bmj.c1069">http://www.bmj.com/content/340/bmj.c1069.long.DOI:10.1136/bmj.c1069. [14] Masala S, Schillaci O, Massari F, et al. MRI and bone scan imaging in the preoperative evaluation of painful vertebral fractures treated with vertebroplasty and kyphoplasty[J]. In Vivo, 2005, 19(6):1055-1060. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 2997
- HTML全文浏览量: 2007
- PDF下载量: 11