


-
子宫颈癌是在全球妇女中发病率仅次于乳腺癌的妇科恶性肿瘤[1-2],且多数患者就诊时已处于中晚期,体外照射联合腔内治疗是中晚期宫颈癌的经典放疗方法。IMRT因能给予靶区更好适形的剂量照射,减少周围正常组织的受量,被广泛应用于宫颈癌的盆腔外照射中[3-5]。近距离腔内放疗是中晚期根治性放疗中的一个重要组成部分,但在患者接受腔内后装照射时,因为肿瘤的解剖位置异常或消退不明显,导致腔内后装陡峭的剂量曲线并不能包绕整个靶区,或是患者因害怕后装带来的痛苦和恐惧,而抵触腔内治疗。在IMRT基础上对肿瘤进行同步推量调强放疗(simultaneous integrated boost-intensity modulated radiation therapy,SIB-IMRT),可以在给予盆腔较低剂量照射的同时,给予转移淋巴结、原发宫颈肿瘤及宫旁受浸组织高剂量照射,在不延长外照射治疗时间的前提下使肿瘤局部单次剂量和总剂量提高,从而有望减少腔内后装的应用次数,减轻患者对后装治疗的恐惧[6-7]。本研究回顾性分析277例中晚期宫颈癌患者资料,以IMRT作为对照,观察SIB-IMRT的不良反应和远期疗效,探讨SIB-IMRT治疗中晚期宫颈癌的安全性及可行性。
-
2009年1月至2015年6月在我院肿瘤科接受根治性放疗同期化疗的中晚期宫颈癌患者,随访成功者277例,卡氏评分≥80,患者无明显放化疗禁忌,平均年龄(52.7±9.77)岁。按照国际妇产科联盟分期标准进行分期,Ⅱb期165例、Ⅲ期97例、Ⅳ期15例。277例患者中鳞癌262例、腺癌12例、腺鳞癌2例、宫颈小细胞癌1例。所有患者实行同步放化疗,其中70例行IMRT,207例行SIB-IMRT。化疗方案为铂类+紫杉醇类,放疗开始前使用紫杉醇类135 mg/m2(1次/d,第1天)+顺铂或奈达铂75 mg/m2(1次/d,第1天),诱导化疗一次。放疗正式开始后,使用顺铂或奈达铂40 mg/m2每周一次单药同步化疗,其中使用顺铂者79例,奈达铂者198例。本研究入组患者均签署知情同意书。两组不同放疗方式患者的一般临床资料分布与可比性见表 1。
临床因素 调强放疗 同步推量调强放疗 χ2值 P值 例数 百分比/% 例数 百分比/% 年龄 ≤53岁 35 50.0 129 62.3 3.287 0.070 >53岁 35 50.0 78 37.7 临床分期 Ⅱb期 38 54.3 127 61.4 1.085 0.298 Ⅲ~Ⅳ期 32 45.7 80 38.6 病理类型 鳞癌 66 94.3 196 94.7 0.016 0.898 非鳞癌 4 5.7 11 5.3 治疗前淋巴结状态 阳性 18 25.7 60 29.0 0.277 0.599 阴性 52 74.3 147 71.0 化疗周期数 1~3个 25 35.7 71 34.3 0.046 0.830 4~6个 45 64.3 136 65.7 化疗方案 顺铂类 36 51.4 43 20.8 24.110 0.000 奈达铂类 34 48.6 164 79.2 表 1 277例中晚期宫颈癌患者的临床资料分组分布与比较
Table 1. Distribution and comparison of clinical data of 277 patients with advanced cervical cancer
-
根据国际辐射单位与测量委员会(ICRU)62号报告,确定肿瘤靶区体积(gross tumor volume,GTV)为CT或MRI上的可见肿瘤,包括宫颈病灶及宫旁受浸范围,同步推量的靶区(GTV-SIB)定义为GTV减去浸及膀胱、直肠的肿瘤体积。临床靶区体积包括GTV外放0.5 cm的范围、阴道上段1/3、宫旁及相应淋巴结引流区(闭口、骶前、髂内外、髂总)。将临床靶区体积外放0.5 cm获得计划靶区体积(planning target volume,PTV)。所有患者遵医嘱于定位前1 h排空膀胱,并饮水500 mL。定位时均采用仰卧位,使用胸腹体膜固定。放疗计划由美国Varian公司eclipse10.0工作站制定,能量选择6 MV X射线。IMRT组及SIB-IMRT组患者采用七野均分等中心照射,照射角度为0°、50°、100°、150°、210°、260°、310°。两组计划的PTV单次处方剂量为1.8~2.0 Gy,照射25~28次,总剂量为50.0~50.4 Gy,PTV覆盖均达到95%。SIB-IMRT组中194例患者GTV(GTVtotal)单次处方剂量为2.0~2.1 Gy,照射28次,总剂量为56.0~58.0 Gy。SIB-IMRT组中另13例患者在GTV外缘向内缩1 cm的区域内,给予单次处方剂量2.0 Gy,总处方剂量56.0 Gy;而在靠近GTV中心区域(GTVcenter)给予高剂量照射(单次处方剂量2.3 Gy,总处方剂量64.0 Gy),从而形成GTV由外到内逐渐递增的剂量分布。危及器官的剂量设定为直肠V50<40%、膀胱V50<40%、小肠V50<10%、股骨头V50<5%。放疗计划传输到Varian 21EX加速器,使用Varian公司的OBI系统图像配准软件进行实时影像采集,完成精确摆位,每周一次,共5次。治疗前患者遵循与其定位时相同的膀胱充盈方法。患者自外照射3周后每周加1次后装治疗,A点(解剖位置位于宫颈口上2 cm,宫颈轴线旁2 cm)6.0 Gy/次。患者全盆腔(外照+后装)剂量以等效2.0 Gy(equivalent dose in 2.0 Gy fraction,EQD2)计算,公式如下:$EQD_{2}=n·d· \frac{{({\rm d}+α/β)}}{{(2+α/β)}}$。其中,肿瘤α/β=10.0 Gy,d为分次剂量,n为分次数,IMRT组患者接受4~5次后装治疗(此时A点EQD2=E外照+E后装=81.6~90.0 Gy,其中,E外照为49.6~50.0 Gy,E后装为32.0~40.0 Gy),SIB-IMRT组患者接受3~4次后装治疗(此时A点EQD2=E外照+E后装=80.0~90.0 Gy,其中,E外照为56.0~58.0 Gy,E后装为24.0~32.0 Gy)。
-
(1)不良反应:急性期反应包括急性放射性膀胱炎、直肠炎及骨髓抑制;远期反应包括远期放射性膀胱炎、直肠炎、骨髓抑制、肠梗阻、下肢水肿、肾积水等。相关急慢性不良反应根据美国肿瘤放射治疗协作组织(RTOG)分级标准记录。(2)生存情况:计算患者1年及3年总生存率(overall survival,OS)。
-
使用SPSS22.0软件行Kaplan-Meier法计算患者OS;使用Cox法行患者生存多因素(包括患者年龄、分期、病理类型、治疗前淋巴结状态及化疗周期数)预后分析;对患者一般资料及不良反应的比较行χ2检验。P < 0.05表示差异有统计学意义。
-
记录患者2级及以上急性与远期骨髓抑制、直肠炎、膀胱炎,结果详见表 2。IMRT组和SIB-IMRT组患者直肠及膀胱的急性毒性反应(χ2=0.306、0.971,P均 > 0.05)和远期毒性反应(χ2=0.014、0.381,P均 > 0.05)发生率的差异无统计学意义;SIB-IMRT组急性骨髓抑制发生率比IMRT组高,且差异有统计学意义(χ2=5.898,P < 0.05);两组患者的远期骨髓抑制、下肢水肿、肾积水及肠梗阻的发生率差异无统计学意义(χ2=2.259、0.740、0.141和1.492,P均 > 0.05)。在SIB-IMRT组中,两种不同GTV推量方式患者间急性及远期不良反应的发生率差异无统计学意义(χ2=0.000~1.497,P均 > 0.05)(表 3)。
不良反应 调强放疗 同步推量调强放疗 χ2值 P值 例数 百分比/% 例数 百分比/% 急性骨髓抑制 50 71.4 175 84.5 5.898 0.015 急性直肠炎 14 20.0 48 23.2 0.306 0.580 急性膀胱炎 3 4.3 16 7.7 0.971 0.324 远期骨髓抑制 3 5.6 3 1.4 2.259 0.133 远期直肠炎 7 13.0 21 10.1 0.014 0.906 远期膀胱炎 1 1.4 6 2.9 0.381 0.537 下肢水肿 1 1.9 1 0.6 0.740 0.390 肾积水 1 1.9 2 1.2 0.141 0.707 肠梗阻 2 3.7 2 1.2 1.492 0.222 表 2 接受调强放疗与同步推量调强放疗的中晚期宫颈癌患者的急性及远期不良反应比较
Table 2. Comparison of acute and long-term toxicities in patients with advanced cervical cancer receiving IMRT and simultaneous integrated boost-intensity modulated radiation therapy
不良反应 GTVcenter GTVtotal χ2值 P值 例数 百分比/% 例数 百分比/% 急性骨髓抑制 11 84.6 164 85.0 0.000 0.994 急性直肠炎 3 23.1 45 23.2 0.000 0.992 急性膀胱炎 0 0.0 16 8.2 1.161 0.281 远期骨髓抑制 0 0.0 3 18.8 0.191 0.662 远期直肠炎 0 0.0 21 13.1 1.497 0.221 远期膀胱炎 0 0.0 6 3.8 0.389 0.533 下肢水肿 0 0.0 1 0.5 0.067 0.795 肾积水 0 0.0 2 1.0 0.135 0.713 肠梗阻 0 0.0 2 1.0 0.135 0.713 注:表中,对GTVcenter给予单次处方剂量2.3 Gy,总处方剂量64 Gy;对GTVtotal给予单次处方剂量2 Gy,总处方剂量56 Gy;GTV:肿瘤靶区体积。 表 3 207例不同GTV推量方式调强放疗的中晚期宫颈癌患者的急性及远期不良反应比较
Table 3. Comparison of acute and long-term toxicities in 207 cases of patients with advanced cervical cancer receiving different simultaneous integrated boost-intensity modulated radiation therapy
-
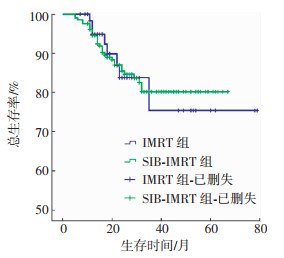
所有患者均完成了放疗。截至2016年7月,所有患者随访时间为9~82个月(中位时间为26个月)。两组患者的生存曲线见图 1。IMRT组及SIB-IMRT组患者1年OS分别为100%和99.5%,3年OS为75.0%和84.7%。两组患者的1年及3年OS差异无统计学意义(χ2=0.339、0.674,P均 > 0.05)。SIB-IMRT组中两种不同GTV推量方式患者的1年OS差异无统计学意义(χ2=0.067,P > 0.05)。随访期间有7例患者出现照射部位局部复发,复发时间为11~16个月(中位时间为13个月);50例患者出现远处转移,主要位于腹膜后、肝、肺、左侧锁骨上等位置,转移时间为2~35个月(中位时间为13个月);47例患者死亡,均为肿瘤所致。
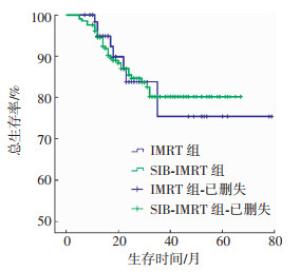
图 1 接受调强放疗(70例)与同步推量调强放疗(207例)的中晚期宫颈癌患者的总生存曲线比较 图中,SIB-IMRT:同步推量调强放疗。
Figure 1. Comparison of overall survival curves in patients with advanced cervical cancer receiving IMRT and simultaneous integrated boost-intensity modulated radiation therapy
-
将患者年龄、分期、病理类型、治疗前淋巴结状态、化疗周期数纳入Cox多因素分析模型,分别对所有入组患者和SIB-IMRT组患者进行多因素分析,结果发现年龄和疗前淋巴结状态是影响所有入组患者(χ2=7.971和15.938,P均 < 0.05)及SIB-IMRT组患者(χ2=7.503和10.048,P均 < 0.05)生存的预后影响因素。
-
子宫颈癌在全球妇女中的发病率呈逐年上升趋势,且很多患者就诊时已处于中晚期,体外照射联合腔内后装治疗是中晚期宫颈癌患者首选的治疗方法。近距离腔内放疗是中晚期根治性放疗中的一个重要组成部分,外照射结束后需要通过高剂量腔内后装来追加剂量,这种放疗模式使得局部晚期宫颈癌的生存率显著提高[8]。中晚期患者中部分肿瘤体积偏大,由于后装放射源位置固定,常造成后装剂量对偏大肿瘤覆盖不足,同时由于后装治疗实施困难,也常使患者因惧怕疼痛而放弃后装治疗。
外照射调强技术的发展在提高靶区受照剂量分布适形度的同时,也降低了周围危及器官的受照剂量,从而为靶区外照射剂量的提升创造了可能。这使得很多学者开始关注SIB-IMRT在中晚期宫颈癌应用中的可行性[9-11]。正常器官移动的不确定性是SIB-IMRT技术在临床中进一步应用的最大限制[12]。Macchia等[13]对局部晚期宫颈癌患者进行术前放疗前瞻性分析,发现给予GTV-SIB单次处方剂量2.25 Gy、总处方剂量45 Gy的SIB-IMRT是可行且安全的。Marnitz等[6]探讨了螺旋断层SIB-IMRT在宫颈癌中应用的早期不良反应,发现给予GTV-SIB单次处方剂量2.12 Gy、总处方剂量59.36 Gy时,40例患者的急性不良反应并未明显增加。这些结果表明GTV推量单次在2.25 Gy以下是可行的。
考虑到膀胱和直肠毗邻GTV,本研究中对GTV-SIB的推量是GTV减去浸及膀胱、直肠的肿瘤体积,并给予GTV常规分割剂量2.0 Gy,低于Macchia及Marnitz给定的处方剂量。放疗过程中通过每周一次的锥形束CT扫描进行靶区变化的追踪和定位。对IMRT和SIB-IMRT两组患者的临床观察发现,两组患者直肠及膀胱的急性毒性反应和远期毒性反应的发生率差异无统计学意义;而IMRT组患者急性骨髓抑制的发生率明显低于SIB-IMRT组,主要是因为IMRT组中接受血液毒性较低的顺铂[14]化疗的患者比例明显高于SIB-IMRT组(χ2=24.110,P < 0.05),而两组患者毗邻骨盆的PTV处方剂量一致,因此认为急性骨髓抑制的发生率受放疗技术差异的影响不大,本研究中SIB-IMRT技术在中晚期宫颈癌患者的放疗实施中是安全的。
在患者生存状况方面,相比IMRT组,本研究中SIB-IMRT组患者的1年及3年OS差异无统计学意义,证明SIB-IMRT组通过增加肿瘤外照射剂量来减少一次腔内后装次数,实现相同肿瘤控制率的方法是可行的。另外,本研究对13例患者进行GTV中心区域高剂量同步推量放疗的探索,结果发现两种不同GTV推量方式下患者的急性期和1年的远期放疗不良反应的发生率差异均无统计学意义,当然对于该技术的临床观察仍需长期的追踪。
本研究对患者预后因素分析发现,年龄和疗前淋巴结状态是影响所有入组患者及SIB-IMRT组患者生存的共同预后因素,表明年龄和疗前淋巴结阳性是中晚期宫颈癌患者生存的预后高危因素。
本研究中IMRT组患者急性及慢性直肠炎的发生率分别为20.0%和13.0%,这与采用相同IMRT技术的Du等[3](19.3%和14.1%)和Gandhi等[15](31.8%和13.6%)的结果相似,且本研究出现的急性及慢性膀胱炎的发生率还略低(分别为4.3%和1.4%)。另外,对本研究IMRT组患者进行生存率分析发现,患者1年及3年OS分别为100%和75%,这与Du等[3](90.7%和82.5%)和Gandhi等[15](27个月生存率为85.7%)的研究结果类似。IMRT组在不良反应和生存情况上均与国外文献类似,表明本研究中对照组的数据是可靠的。不足之处是本研究中IMRT组比SIB-IMRT组病例数偏少,后期将继续增加IMRT组病例数以完善研究。
综上所述,外照射同步推量GTV至单次剂量2.00~2.07 Gy、总剂量56~58 Gy的调强技术在中晚期宫颈癌的根治性放疗中是安全可行的,该技术可以减少后装治疗的次数,从而减轻患者后装治疗的不适及痛苦。对于中晚期宫颈癌患者,SIB-IMRT是一种可尝试的外照射技术。
中晚期宫颈癌患者调强放疗与同步推量调强放疗预后比较
Clinical effects of IMRT and simultaneous integrated boost-intensity modulated radiation therapy: a comparative study of 277 patients with advanced cervical cancer
-
摘要:
目的 探讨同步推量调强放疗(SIB-IMRT)技术治疗中晚期宫颈癌患者的不良反应、远期疗效及相关预后因素。 方法 回顾性分析2009年1月至2015年6月收治的277例中晚期未手术的宫颈癌患者,其中70例行IMRT,207例行SIB-IMRT。比较中晚期宫颈癌患者行IMRT与SIB-IMRT后的不良反应,并进行远期疗效及预后因素分析。采用Kaplan-Meier法计算生存率,Cox法行多因素预后分析。 结果 IMRT组与SIB-IMRT组的随访率均为100%。与IMRT相比,SIB-IMRT未增加患者直肠及膀胱的急性毒性反应(χ2=0.306和0.971,P均>0.05)和远期毒性反应(χ2=0.014和0.381,P均>0.05)。IMRT组及SIB-IMRT组患者1年总生存率(OS)分别为100%和99.5%,3年OS分别为75.0%和84.7%,差异无统计学意义(χ2=0.339和0.674,P均>0.05)。患者年龄和治疗前淋巴结状态是所有入组患者(χ2=7.971和15.938,P均 < 0.05)及SIB-IMRT组患者(χ2=7.503和10.048,P均 < 0.05)生存的预后影响因素。 结论 初步结果表明SIB-IMRT技术安全可行,且可以减少后装治疗次数,减轻患者后装治疗的不适及痛苦。对于中晚期宫颈癌患者,SIB-IMRT是一种可尝试的外照射技术。 Abstract:Objective To explore the toxicity, long-term overall survival(OS), and prognostic factors in advanced cervical cancer treated with IMRT and simultaneous integrated boost-intensity modulated radiation therapy(SIB-IMRT). Methods A retrospective analysis was performed on 277 patients with advanced cervical cancer. These patients were admitted from January 2009 to June 2015. Among the 277 patients, 70 patients received IMRT, and 207 patients received SIB-IMRT. Toxicities, survival rates, and prognostic factors were compared between the two groups. The Kaplan-Meier method was used to calculate the survival rates, and the Cox model was used for multivariate prognostic analysis. Results The follow-up rate was 100% in both the IMRT and SIB-IMRT groups. Compared with IMRT, SIB-IMRT showed no significant differences in acute proctitis and cystitis toxicities(χ2=0.306, 0.971, both P>0.05), as well as in long-term toxicity(χ2=0.014, 0.381, both P>0.05). The 1-year OS rates for the IMRT and SIB-IMRT groups were 100% and 99.5%, respectively, and the 3-year OS rates were 75.0% and 84.7%, correspondingly(χ2=0.339, 0.674, both P>0.05). The age and status of the pretreatment lymph nodes were the prognostic factors for all patients(χ2=7.971, 15.938, both P < 0.05), including the SIB-IMRT group(χ2=7.503, 10.048, both P < 0.05) in terms of OS. Conclusion Results indicated that SIB-IMRT can feasibly treat advanced cervical cancer. SIB-IMRT is a promising alternative treatment for patients who are not fit for brachytherapy treatment; this method also helps to reduce treatment fractions. Hence, SIB-IMRT is a recommended external beam technology for cervical cancer treatment. -
图 1 接受调强放疗(70例)与同步推量调强放疗(207例)的中晚期宫颈癌患者的总生存曲线比较 图中,SIB-IMRT:同步推量调强放疗。
Figure 1. Comparison of overall survival curves in patients with advanced cervical cancer receiving IMRT and simultaneous integrated boost-intensity modulated radiation therapy
表 1 277例中晚期宫颈癌患者的临床资料分组分布与比较
Table 1. Distribution and comparison of clinical data of 277 patients with advanced cervical cancer
临床因素 调强放疗 同步推量调强放疗 χ2值 P值 例数 百分比/% 例数 百分比/% 年龄 ≤53岁 35 50.0 129 62.3 3.287 0.070 >53岁 35 50.0 78 37.7 临床分期 Ⅱb期 38 54.3 127 61.4 1.085 0.298 Ⅲ~Ⅳ期 32 45.7 80 38.6 病理类型 鳞癌 66 94.3 196 94.7 0.016 0.898 非鳞癌 4 5.7 11 5.3 治疗前淋巴结状态 阳性 18 25.7 60 29.0 0.277 0.599 阴性 52 74.3 147 71.0 化疗周期数 1~3个 25 35.7 71 34.3 0.046 0.830 4~6个 45 64.3 136 65.7 化疗方案 顺铂类 36 51.4 43 20.8 24.110 0.000 奈达铂类 34 48.6 164 79.2  下载: 导出CSV
下载: 导出CSV
表 2 接受调强放疗与同步推量调强放疗的中晚期宫颈癌患者的急性及远期不良反应比较
Table 2. Comparison of acute and long-term toxicities in patients with advanced cervical cancer receiving IMRT and simultaneous integrated boost-intensity modulated radiation therapy
不良反应 调强放疗 同步推量调强放疗 χ2值 P值 例数 百分比/% 例数 百分比/% 急性骨髓抑制 50 71.4 175 84.5 5.898 0.015 急性直肠炎 14 20.0 48 23.2 0.306 0.580 急性膀胱炎 3 4.3 16 7.7 0.971 0.324 远期骨髓抑制 3 5.6 3 1.4 2.259 0.133 远期直肠炎 7 13.0 21 10.1 0.014 0.906 远期膀胱炎 1 1.4 6 2.9 0.381 0.537 下肢水肿 1 1.9 1 0.6 0.740 0.390 肾积水 1 1.9 2 1.2 0.141 0.707 肠梗阻 2 3.7 2 1.2 1.492 0.222
下载: 导出CSV
表 3 207例不同GTV推量方式调强放疗的中晚期宫颈癌患者的急性及远期不良反应比较
Table 3. Comparison of acute and long-term toxicities in 207 cases of patients with advanced cervical cancer receiving different simultaneous integrated boost-intensity modulated radiation therapy
不良反应 GTVcenter GTVtotal χ2值 P值 例数 百分比/% 例数 百分比/% 急性骨髓抑制 11 84.6 164 85.0 0.000 0.994 急性直肠炎 3 23.1 45 23.2 0.000 0.992 急性膀胱炎 0 0.0 16 8.2 1.161 0.281 远期骨髓抑制 0 0.0 3 18.8 0.191 0.662 远期直肠炎 0 0.0 21 13.1 1.497 0.221 远期膀胱炎 0 0.0 6 3.8 0.389 0.533 下肢水肿 0 0.0 1 0.5 0.067 0.795 肾积水 0 0.0 2 1.0 0.135 0.713 肠梗阻 0 0.0 2 1.0 0.135 0.713 注:表中,对GTVcenter给予单次处方剂量2.3 Gy,总处方剂量64 Gy;对GTVtotal给予单次处方剂量2 Gy,总处方剂量56 Gy;GTV:肿瘤靶区体积。
下载: 导出CSV
-
[1] 张瑾, 吴玉梅, 孔为民, 等.763例Ⅲ期宫颈癌不同放疗方法的疗效分析[J].中华放射肿瘤学杂志, 2008, 17(5):364-367. DOI:10.3321/j.issn:1004-4221.2008.05.009.
Zhang J, Wu YM, Kong WM, et al.Treatment results of different radiotherapy for 763 patients with advanced cervical cancer[J].Chin J Radiat Oncol, 2008, 17(5):364-367. doi: 10.3321/j.issn:1004-4221.2008.05.009[2] 黄建敏, 潘莉萍, 李冬雪.PET和PET-CT在宫颈癌中的应用价值[J].国际放射医学核医学杂志, 2007, 31(2):112-114. DOI:10.3760/cma.j.issn.1673-4114.2007.02.016.
Huang JM, Pan LP, Li DX.The application of PET and PET-CT in cervical cancer[J].Int J Radiat Med Nucl Med, 2007, 31(2):112-114. doi: 10.3760/cma.j.issn.1673-4114.2007.02.016[3] Du XL, Tao J, Sheng XG, et al.Intensity-modulated radiation therapy for advanced cervical cancer:a comparison of dosimetric and clinical outcomes with conventional radiotherapy[J].Gynecol Oncol, 2012, 125(1):151-157. DOI:10.1016/j.ygyno.2011.12.432. [4] Chen CC, Lin JC, Jan JS, et al.Definitive intensity-modulated radiation therapy with concurrent chemotherapy for patients with locally advanced cervical cancer[J].Gynecol Oncol, 2011, 122(1):9-13. DOI:10.1016/j.ygyno.2011.03.034. [5] Zhang G, Fu C, Zhang Y, et al.Extended-field intensity-modulated radiotherapy and concurrent cisplatin-based chemotherapy for postoperative cervical cancer with common iliac or para-aortic lymph node metastases:a retrospective review in a single institution[J].Int J Gynecol Cancer, 2012, 22(7):1220-1225. DOI:10.1097/IGC.0b013e3182643b7c. [6] Marnitz S, Köhler C, Burova E, et al.Helical tomotherapy with simultaneous integrated boost after laparoscopic staging in patients with cervical cancer: analysis of feasibility and early toxicity[J/OL].Int J Radiat Oncol Biol Phys, 2012, 82(2): e137-e143[2016-09-13].http://www.sciencedirect.com/science/acticle/pii/S0360301610036382. DOI: 10.1016/j.ijrobp.2010.10.066. [7] Vandecasteele K, De Neve W, De Gersem W, et al.Intensity-modulated arc therapy with simultaneous integrated boost in the treatment of primary irresectable cervical cancer.Treatment planning, quality control, and clinical implementation[J].Strahlenther Onkol, 2009, 185(12):799-807. DOI:10.1007/s00066-009-1986-8. [8] Koh WY, Lim K, Tey J, et al.Outcome of 6 fractions of 5.3 Gray HDR brachytherapy in combination with external beam radiotherapy for treatment of cervical cancer[J].Gynecol Oncol, 2013, 131(1):93-98. DOI:10.1016/j.ygyno.2013.07.102. [9] Boyle J, Craciunescu O, Steffey B, et al.Methods, safety, and early clinical outcomes of dose escalation using simultaneous integrated and sequential boosts in patients with locally advanced gynecologic malignancies[J].Gynecol Oncol, 2014, 135(2):239-243. DOI:10.1016/j.ygyno.2014.08.037. [10] Marnitz S, Stromberger C, Kawagan-Kagan M, et al.Helical tomotherapy in cervical cancer patients:simultaneous integrated boost concept:technique and acute toxicity[J].Strahlenther Onkol, 2010, 186(10):572-579. DOI:10.1007/s00066-010-2121-6. [11] Guerrero M, Li XA, Ma L, et al.Simultaneous integrated intensity-modulated radiotherapy boost for locally advanced gynecological cancer:radiobiological and dosimetric considerations[J].Int J Radiat Oncol Biol Phys, 2005, 62(3):933-939. DOI:10.1016/j.ijrobp.2004.11.040. [12] Harris EE, Latifi K, Rusthoven C, et al.Assessment of organ motion in postoperative endometrial and cervical cancer patients treated with intensity-modulated radiation therapy[J].Int J Radiat Oncol Biol Phys, 2011, 81(4):E645-E650. DOI:10.1016/j.ijrobp.2011.01.054. [13] Macchia G, Cilla S, Deodato F, et al.Intensity-modulated extended-field chemoradiation plus simultaneous integrated boost in the pre-operative treatment of locally advanced cervical cancer: a dose-escalation study[J/OL].Br J Radiol, 2015, 88(1055): 20150385[2016-09-13].https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4743458. DOI: 10.1259/bjr.20150385. [14] 朱卫国, 于长华, 李涛, 等.国产奈达铂用于宫颈癌同步放化疗的剂量递增试验[J].中华肿瘤杂志, 2011, 33(7):525-526. DOI:10.3760/cma.j.issn.0253-3766.2011.07.011.
Zhu WG, Yu CH, Li T, et al.Dose escalation of domestic nedaplatin used in concurrent chemoradiotherapy for cervical cancer[J].Chin J Oncol, 2011, 33(7):525-526. doi: 10.3760/cma.j.issn.0253-3766.2011.07.011[15] Gandhi AK, Sharma DN, Rath GK, et al.Early clinical outcomes and toxicity of intensity modulated versus conventional pelvic radiation therapy for locally advanced cervix carcinoma:a prospective randomized study[J].Int J Radiat Oncol Biol Phys, 2013, 87(3):542-548. DOI:10.1016/j.ijrobp.2013.06.2059. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 2849
- HTML全文浏览量: 1825
- PDF下载量: 4