


-
在我国,食管鳞癌占所有食管癌的95%以上,且绝大多数发生于胸段食管,而淋巴结转移是食管癌最常见的转移途径,淋巴结转移枚数是食管癌患者重要的独立负性预后因子,与患者的生存时间呈负相关[1-4]。第7版美国癌症联合委员会食管癌分期中规定,从锁骨上区到腹腔干均为区域淋巴结,1~2枚区域淋巴结转移为N1,3~6枚转移为N2,≥7枚转移为N3[5]。因此术前准确判断淋巴结是否转移至关重要。本研究对18F-FDG PET/CT显像与增强CT在术前胸段食管鳞癌淋巴结转移诊断中的准确率进行评价,现报道如下。
-
选取我院2010年10月至2016年1月经病理证实且未患过其他恶性肿瘤的胸段食管鳞癌患者54例,男性46例、女性8例,年龄41~73岁,平均(59.4±8.7)岁。同期(术前一周内)行18F-FDG PET/CT及增强CT检查,所有患者或家属均于检查前签署了知情同意书。术后病理淋巴结分期为N0期22例、N1期24例、N2期7例、N3期1例。胸上段、胸中段及胸下段食管鳞癌例数分别为8、34和12例。
-
采用荷兰Philips公司生产的Gemini TF 64 PET/CT仪,18F-FDG由日本住友公司HM-10回旋加速器生产,放化纯度>95%。患者检查前禁食6 h以上,控制血糖范围在3.9~7.5 mmol/L。经静脉注射185~370 MBq 18F-FDG后,安静休息约60 min,排尿后仰卧位上机扫描。CT扫描采集条件为120 kV、200 mA,矩阵512×512,层厚5 mm,然后以1 min/床位的速度采集从颅底至股骨上段的PET图像。采用三维模式采集,应用CT数据进行衰减校正,在EBW2.0后处理工作站上将PET图像和CT图像进行融合,分别得到横断面、矢状面及冠状面的PET、CT及PET/CT融合图像。
-
采用东芝16层螺旋CT机(Aquilion/M16型),行食管CT平扫及增强扫描,扫描范围包括下颈部、胸部及上腹部,扫描参数为管电压120 kV,管电流采用自动毫安,层厚5 mm,增强扫描采用非离子型对比剂经肘静脉注射,剂量为70~90 mL/s。获得图像分别在纵隔窗和肺窗下观察,并结合1.0 mm层厚轴位源图像行多平面重建。
-
所有患者均行经胸食管癌切除术,常规2野或3野淋巴结清扫,术式取决于肿瘤位置和术前影像学检查所示阳性淋巴结位置,术中对切取的淋巴结行常规切片以作病理学检查。术后根据手术和病理学资料对每组淋巴结与术前影像信息进行比较。
-
参考食管癌淋巴结分组标准,即1R组为右锁骨上淋巴结,1L组为左锁骨上淋巴结,2R组为右上气管旁淋巴结,2L组为左上气管旁淋巴结,3P组为上段食管旁淋巴结,4R组为右下气管旁淋巴结,4L组为左下气管旁淋巴结,5组为主肺动脉窗淋巴结,6组为前纵隔淋巴结,7组为隆突下淋巴结,8M组为中段食管旁淋巴结,8L组为下段食管旁淋巴结,9组为下肺韧带淋巴结,10R组为右气管支气管淋巴结,10L组为左气管支气管淋巴结,11R组为右肺叶间淋巴结,11L组为左肺叶间淋巴结,15组为横隔淋巴结,16组为贲门周围淋巴结,17组为胃左动脉旁淋巴结,18组为肝总动脉旁淋巴结,19组为脾动脉旁淋巴结,20组为腹腔动脉旁淋巴结[6]。
-
对18F-FDG PET/CT显像结果进行视觉分析和半定量分析,在PET图像上找出局灶性浓聚灶,浓聚程度高于纵隔则为阳性,低于纵隔则为阴性,在PET/CT融合图像上确定是否为阳性淋巴结并精确定位,分组参照文献[6]。选择所有阳性显像病灶横断面放射性摄取程度最高层面,以病灶大小的90%为ROI,计算机自动计算SUV,结合病灶的边界、形态及密度进行判断。将病灶边界清晰、形态规则、密度均匀且SUV>2.5作为恶性病变的诊断标准,如果边界不清晰、形态不规则或者密度不均匀伴有钙化,即使SUV>2.5也视为阴性。同时记录肿大淋巴结短径。增强CT阳性淋巴结的诊断标准为淋巴结短径>10 mm或者增强扫描后呈薄壁环状强化。分别统计18F-FDG PET/CT和增强CT对胸段食管癌淋巴结转移的灵敏度、特异度及准确率,应用SPSS13.0软件对二者诊断效能的相关数据进行χ2检验。统计所有肿大淋巴结短径,将其分为3组(≤5 mm、5~10 mm及≥10 mm),采用χ2检验比较两种显像方法的诊断准确率。P < 0.05表示差异有统计学意义。
-
54例患者共切取并分离淋巴结186枚,均经病理证实,其中转移淋巴结77枚,非转移淋巴结109枚。
18F-FDG PET/CT诊断淋巴结转移65枚(典型病例见图 1中A),其中假阳性5枚(5组、11L组、17组各1枚,7组2枚,典型病例见图 1中B),PET/CT图像显示淋巴结边界清晰,SUV均>2.6,但病理证实纤维组织内见钙化,为良性;诊断良性淋巴结121枚,其中假阴性17枚(1R组、2L组、4R组、8M组各1枚,2R组3枚,8L组4枚,16组6枚,典型病例见图 1中C),除16组1枚(短径12 mm,伴囊变,SUV=2.2,病理证实为转移淋巴结,见图 1中D)和8M组1枚(短径10 mm,位于中段食管旁,与食管病灶融合,见图 1中E)外,其余淋巴结短径均≤5 mm,SUV均<2.5,病理证实均为转移淋巴结。增强CT诊断淋巴结转移58枚,其中假阳性27枚(10R组9枚,10L组6枚,11L组3枚,5组、6组、7组各2枚,11R组、4R组、8M组各1枚),短径均≥10 mm,病理证实为良性;诊断良性淋巴结128枚,其中假阴性46枚(1R组、3P组、4L组、11L组和10L组各1枚,17组、8M组和7组各2枚,1L组、2L组和10R组各3枚,16组5枚,4R组6枚,8L组7枚,2R组8枚),短径均<10 mm,病理证实为转移淋巴结(表 1)。由表 1可见,胸段食管鳞癌淋巴结转移主要位于2R组、4R组、8M组、8L组、16组和17组;18F-FDG PET/CT显像假阴性主要位于2R组(3枚)、8L组(4枚)和16组(6枚)。
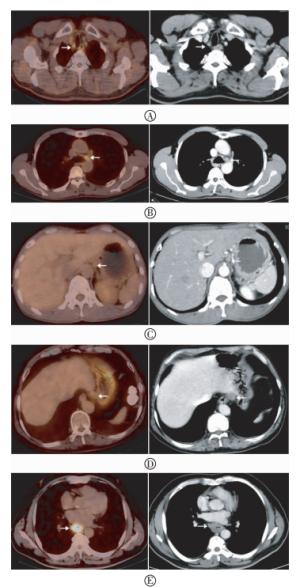
图 1 胸段食管鳞癌患者18F-FDG PET/CT与增强CT显像图图中,A:2R组淋巴结(箭头所示),直径5 mm,PET/CT融合图像放射性异常摄取,SUVmax=3.4,增强CT图像相应部位淋巴结为假阴性;B:5组淋巴结(箭头所示),短径5 mm,SUVmax=3.2,PET/CT显示为假阳性,增强CT为真阴性,病理证实为良性;C:16组淋巴结(箭头所示),直径5 mm,PET/CT融合图像无放射性摄取,增强CT图像相应部位淋巴结边界欠清晰,病理证实为转移淋巴结;D:16组淋巴结伴囊变(箭头所示),短径12 mm,PET/CT融合图像无放射性摄取,显示为假阴性,而增强CT呈环形轻度强化,显示为真阳性淋巴结;E:原发灶旁8M组淋巴结(箭头所示),由于原发灶对显像剂的摄取掩盖了淋巴结的放射性摄取,故PET/CT未发现病灶,而增强CT该部位淋巴结为真阳性,短径10 mm。
Figure 1. Representative images of 18F-FDG PET/CT and enhanced CT in detecting metastatic lymph nodes of thoracic esophageal squamous cell carcinoma
组别 18F-FDG PET/CT 增强CT 合计 转移淋巴结占比[(n/77)/%] 真阳性 假阳性 真阴性 假阴性 真阳性 假阳性 真阴性 假阴性 1R组 1 0 2 1 1 0 2 1 4 2.6 1L组 3 0 6 0 0 0 6 3 9 3.9 2R组 15 0 12 3 10 0 12 8 30 23.4 2L组 3 0 6 1 1 0 6 3 10 5.2 3P组 1 0 2 0 0 0 2 1 3 1.3 4R组 6 0 7 1 1 1 6 6 14 9.1 4L组 2 0 0 0 1 0 0 1 2 2.6 5组 1 1 10 0 1 2 9 0 12 1.3 6组 0 0 7 0 0 2 5 0 7 0 7组 4 2 5 0 2 2 5 2 11 5.2 8M组 4 0 3 1 3 1 2 2 8 6.5 8L组 3 0 1 4 0 0 1 7 8 9.1 9组 0 0 1 0 0 0 1 0 1 0 10R组 4 0 12 0 1 9 3 3 16 5.2 10L组 1 0 11 0 0 6 5 1 12 1.3 11R组 0 0 6 0 0 1 5 0 6 0 11L组 1 1 8 0 0 3 6 1 10 1.2 15组 0 0 0 0 0 0 0 0 0 0 16组 1 0 1 6 2 0 1 5 8 9.1 17组 8 1 2 0 6 0 3 2 11 10.4 18组 2 0 0 0 2 0 0 0 2 2.6 19组 0 0 1 0 0 0 1 0 1 0 20组 0 0 1 0 0 0 1 0 1 0 合计 60 5 104 17 31 27 82 46 186 100 表 1 18F-FDG PET/CT与增强CT诊断不同组别胸段食管鳞癌肿大淋巴结及病理检查结果(例)
Table 1. Results of 18F-FDG PET/CT and enhanced CT in diagnosing different groups of lymph nodes of thoracic esophageal squamous cell carcinoma compared with the histopathological results
18F-FDG PET/CT诊断淋巴结转移的灵敏度、特异度和准确率分别为77.9%(60/77)、95.4%(104/109)和88.2%(164/186),均高于增强CT的40.3%(31/77)、75.2%(82/109)和60.8%(113/186),且二者差异有统计学意义(χ2=24.04、15.77和36.77,P均 < 0.01)。
短径≤5 mm的淋巴结47枚,18F-FDG PET/CT正确诊断35枚,准确率为74.5%,增强CT正确诊断37枚,准确率为78.7%,二者差异无统计学意义(χ2=0.24,P>0.05);短径5~10 mm和≥10 mm淋巴结分别为81枚、58枚,18F-FDG PET/CT正确诊断分别为75枚、54枚,准确率分别为92.6%、93.1%,增强CT正确诊断分别为47枚、29枚,准确率分别为58.0%、50.0%,18F-FDG PET/CT和增强CT的诊断差异均有统计学意义(χ2=26.03和26.47,P均 < 0.01)。
从整体上看,18F-FDG PET/CT诊断胸段食管鳞癌淋巴结分期正确42例(77.8%)、错误12例(22.2%);增强CT正确29例(53.7%)、错误25例(46.3%)(表 2)。18F-FDG PET/CT联合增强CT诊断可修正3例N分期,准确率提高至83.3%(45/54)。
分期 18F-FDG PET/CT 增强CT 正确分期 N0 21 15 N1 16 10 N2 4 4 N3 1 0 提高分期 N0→N1 1 4 N0→N2 0 3 N1→N2 2 3 降低分期 N1→N0 6 11 N2→N0 2 1 N2→N1 1 2 N3→N2 0 1 表 2 18F-FDG PET/CT与增强CT诊断胸段食管鳞癌N分期及病理对照结果(例)
Table 2. Results of 18F-FDG PET/CT and enhanced CT in diagnosing the N stage of thoracic esophageal squamous cell carcinoma
-
食管癌好发淋巴结转移,食管淋巴引流主要是以纵行方向为主,纵行淋巴管数量是横行淋巴管数量的6倍。胸段食管癌转移多先转移到肿瘤相应部位食管旁淋巴结,胸上段食管癌多沿食管旁淋巴结向颈部淋巴结转移;胸中段食管癌则既有向上到胸上段食管旁、气管旁、颈深及锁骨上淋巴结转移,也可向下转移到贲门旁、胃左血管旁等胃周淋巴结;胸下段食管癌则以下行淋巴结转移居多,呈现上下双向跳跃式转移的特点[7]。本组病例中胸段食管癌食管旁淋巴结转移以8M组、8L组为主,向上以跳跃出现在2R组及4R组常见,向下以16组及17组常见,符合食管癌淋巴结的转移规律。
食管癌淋巴结转移是影响患者预后的最重要因素之一,食管癌术前淋巴结分期关系到综合治疗方案的选择和疗效的评估,准确的淋巴结分期是提高食管癌手术切除率及术后生存率的重要保证。因此术前准确判断淋巴结是否转移至关重要。目前对食管癌的淋巴结转移大多根据CT、MRI或超声内镜等解剖影像来确定[8]。但是这些影像检查仍存在较多的假阳性和假阴性结果[9],即临床上经常会出现增大的淋巴结并非转移淋巴结,而转移淋巴结并不肿大的情况。因此,单从淋巴结在解剖影像学上表现的大小来判断食管癌的淋巴结转移还存在不足。增强CT作为最常用的食管癌术前检查方法,其在T分期上的诊断价值已得到普遍认可[10];但在N分期上,其准确率普遍不高,相关资料显示其灵敏度、特异度及准确率分别介于8.0%~84.0%、60.0%~99.0%及45.0%~96.0%[9, 11-12]。本研究结果也介于上述范围,>10 mm的淋巴结除了由肿瘤转移引起外还可以由炎症或反应性增生造成,而<10 mm的淋巴结也经常存在转移灶,这导致CT以短径大小来判断淋巴结是否转移存在很大的局限性,无法对肿大淋巴结进行定性,造成增强CT对N分期的诊断准确率偏低,本研究中增强CT诊断胸段食管鳞癌淋巴结分期的准确率仅为53.7%。而18F-FDG PET/CT诊断淋巴结转移不仅以淋巴结大小、形态来判断,还结合分子代谢改变为依据,是集解剖与功能影像特点于一体的检查方法。本研究18F-FDG PET/CT诊断淋巴结转移的灵敏度、特异度及准确率分别为77.9%、95.4%及88.2%,与文献[13]的77.8%、92.9%及84.4%及文献[14]的74.7%、97.2%、92.0%报道相近,但灵敏度却低于文献[15]的86.2%与文献[16]的83.1%,这与本研究中假阴性淋巴结有15枚短径均≤5 mm有关,转移淋巴结内肿瘤细胞较少,对18F-FDG的摄取相对较少,部分转移的小淋巴结受PET空间分辨率的限制或部分容积效应的影响无法清晰显示[16],从而降低了N分期。本组研究还有一例淋巴结呈现囊变坏死而无放射性浓聚。这些情况除了结合增强CT,还应按淋巴结具体分组提示临床淋巴结肿大,以便有目的地进行清扫。
由于18F-FDG是非肿瘤特异显像剂,各种非特异性炎症所致的淋巴结肿大常出现放射性浓聚,尤其是老年患者对称性的肺门淋巴结肿大及其放射性浓聚,易使N分期增高,这些淋巴结边界欠清晰、伴有钙盐沉积,诊断中应将这类淋巴结视为良性,可降低假阳性率。本研究据此诊断仍有5枚假阳性淋巴结,虽然边界清晰,但病理证实是纤维组织内伴钙盐沉积,此时应多结合临床及既往病史、职业史加以分析。虽然本研究中18F-FDG PET/CT诊断胸段食管鳞癌N分期的准确率达到77.8%,但却与本研究54例患者中N0期较多,而N2、N3期较少,手术取出的淋巴结也偏少有关,因此仍有待更大、更均衡的样本研究。
总之,融合了功能显像与解剖显像特点的18F-FDG PET/CT在胸段食管鳞癌淋巴结转移中的诊断价值高于以解剖显像为诊断基础的增强CT,具有较高的临床应用价值。
18F-FDG PET/CT在胸段食管鳞癌淋巴结转移中的诊断价值
Value of 18F-FDG PET/CT in detecting metastatic lymph nodes of thoracic esophageal squamous cell carcinoma
-
摘要:
目的 探讨18F-FDG PET/CT在胸段食管鳞癌淋巴结转移中的诊断价值,并与增强CT及术后病理结果进行对比。 方法 胸段食管鳞癌患者54例,术前一周内行18F-FDG PET/CT和增强CT扫描,术后以病理学诊断为“金标准”,比较两种显像方法对胸段食管鳞癌淋巴结转移的灵敏度、特异度、准确率及不同短径范围的诊断准确率。应用SPSS13.0软件进行四格表χ2检验。 结果 手术共切取肿大淋巴结186枚,均经病理证实,其中淋巴结转移77枚,18F-FDG PET/CT诊断淋巴结转移的灵敏度、特异度及准确率分别为77.9%(60/77)、95.4%(104/109)和88.2%(164/186),增强CT分别为40.3%(31/77)、75.2%(82/109)和60.8%(113/186),二者诊断效能差异有统计学意义(χ2=24.04、15.77和36.77,P均 < 0.01)。对于短径>5 mm(5~10 mm及≥10 mm)的淋巴结,18F-FDG PET/CT诊断的准确率高于增强CT,且差异有统计学意义(χ2=26.03和26.47,P均 < 0.01);对于短径≤5 mm的淋巴结,二者间诊断的准确率差异无统计学意义(χ2=0.24,P>0.05)。 结论 18F-FDG PET/CT在胸段食管鳞癌淋巴结转移中具有较高的诊断价值,对于短径>5 mm的淋巴结优势明显。 -
关键词:
- 食管肿瘤 /
- 正电子发射断层显像术 /
- 体层摄影术, X线计算机 /
- 氟脱氧葡萄糖F18 /
- 淋巴结转移 /
- 短径
Abstract:Objective To analyze the diagnostic value of 18F-FDG PET/CT and enhanced CT in detecting metastatic lymph nodes of thoracic esophageal squamous cell carcinoma. Methods Fifty-four patients with thoracic esophageal squamous cell carcinoma underwent both 18F-FDG PET/CT and enhanced CT before surgery within a week. All lesions were confirmed histopathologically as the golden standard. The sensitivity, specificity, and accuracy of the two imaging modalities were compared. In addition, the diagnostic accuracy of the two methods in detecting metastatic lymph nodes having different diameters in patients with thoracic esophageal squamous cell carcinoma was evaluated. Theχ2-test was used with SPSS 13.0. Results A total of 186 lymph node specimens, including 77 specimens of metastases, were extracted and confirmed by pathology. The sensitivity, specificity, and accuracy of 18F-FDG PET/CT were 77.9%(60/77), 95.4%(104/109), 88.2%(164/186), respectively, whereas those of enhanced CT were 40.3%(31/77), 75.2%(82/109), and 60.8%(113/186), respectively. All values were statistically significant(χ2=24.04, 15.77, and 36.77, all P < 0.01). The diagnostic accuracy of 18F-FDG PET/CT is significantly better than that of enhanced CT in the group of R>5 mm (χ2=26.03 and 26.47, both P < 0.01) without the group of R≤5 mm(χ2=0.24, P>0.05). Conclusion 18F-FDG PET/CT has a great value in detecting metastatic lymph nodes of thoracic esophageal squamous cell carcinoma, especially lymph nodes that are R>5 mm. -
图 1 胸段食管鳞癌患者18F-FDG PET/CT与增强CT显像图图中,A:2R组淋巴结(箭头所示),直径5 mm,PET/CT融合图像放射性异常摄取,SUVmax=3.4,增强CT图像相应部位淋巴结为假阴性;B:5组淋巴结(箭头所示),短径5 mm,SUVmax=3.2,PET/CT显示为假阳性,增强CT为真阴性,病理证实为良性;C:16组淋巴结(箭头所示),直径5 mm,PET/CT融合图像无放射性摄取,增强CT图像相应部位淋巴结边界欠清晰,病理证实为转移淋巴结;D:16组淋巴结伴囊变(箭头所示),短径12 mm,PET/CT融合图像无放射性摄取,显示为假阴性,而增强CT呈环形轻度强化,显示为真阳性淋巴结;E:原发灶旁8M组淋巴结(箭头所示),由于原发灶对显像剂的摄取掩盖了淋巴结的放射性摄取,故PET/CT未发现病灶,而增强CT该部位淋巴结为真阳性,短径10 mm。
Figure 1. Representative images of 18F-FDG PET/CT and enhanced CT in detecting metastatic lymph nodes of thoracic esophageal squamous cell carcinoma
表 1 18F-FDG PET/CT与增强CT诊断不同组别胸段食管鳞癌肿大淋巴结及病理检查结果(例)
Table 1. Results of 18F-FDG PET/CT and enhanced CT in diagnosing different groups of lymph nodes of thoracic esophageal squamous cell carcinoma compared with the histopathological results
组别 18F-FDG PET/CT 增强CT 合计 转移淋巴结占比[(n/77)/%] 真阳性 假阳性 真阴性 假阴性 真阳性 假阳性 真阴性 假阴性 1R组 1 0 2 1 1 0 2 1 4 2.6 1L组 3 0 6 0 0 0 6 3 9 3.9 2R组 15 0 12 3 10 0 12 8 30 23.4 2L组 3 0 6 1 1 0 6 3 10 5.2 3P组 1 0 2 0 0 0 2 1 3 1.3 4R组 6 0 7 1 1 1 6 6 14 9.1 4L组 2 0 0 0 1 0 0 1 2 2.6 5组 1 1 10 0 1 2 9 0 12 1.3 6组 0 0 7 0 0 2 5 0 7 0 7组 4 2 5 0 2 2 5 2 11 5.2 8M组 4 0 3 1 3 1 2 2 8 6.5 8L组 3 0 1 4 0 0 1 7 8 9.1 9组 0 0 1 0 0 0 1 0 1 0 10R组 4 0 12 0 1 9 3 3 16 5.2 10L组 1 0 11 0 0 6 5 1 12 1.3 11R组 0 0 6 0 0 1 5 0 6 0 11L组 1 1 8 0 0 3 6 1 10 1.2 15组 0 0 0 0 0 0 0 0 0 0 16组 1 0 1 6 2 0 1 5 8 9.1 17组 8 1 2 0 6 0 3 2 11 10.4 18组 2 0 0 0 2 0 0 0 2 2.6 19组 0 0 1 0 0 0 1 0 1 0 20组 0 0 1 0 0 0 1 0 1 0 合计 60 5 104 17 31 27 82 46 186 100  下载: 导出CSV
下载: 导出CSV
表 2 18F-FDG PET/CT与增强CT诊断胸段食管鳞癌N分期及病理对照结果(例)
Table 2. Results of 18F-FDG PET/CT and enhanced CT in diagnosing the N stage of thoracic esophageal squamous cell carcinoma
分期 18F-FDG PET/CT 增强CT 正确分期 N0 21 15 N1 16 10 N2 4 4 N3 1 0 提高分期 N0→N1 1 4 N0→N2 0 3 N1→N2 2 3 降低分期 N1→N0 6 11 N2→N0 2 1 N2→N1 1 2 N3→N2 0 1
下载: 导出CSV
-
[1] Wijnhoven BP, Tran KT, Esterman AA, et al.An evaluation of prognostic factors and tumor staging of resected carcinoma of the esophagus[J].Ann Surg, 2007, 245(5):717-725. DOI:10.1097/01.sla.0000251703.35919.02. [2] Chen J, Zhu J, Pan J, et al.Postoperative radiotherapy improved survival of poor prognostic squamous cell carcinoma esophagus[J].Ann Thorac Surg, 2010, 90(2):435-442. DOI:10.1016/j.athoracsur.2010.04.002. [3] 陈元美, 陈俊强, 朱坤寿, 等.淋巴结转移数目与胸段食管鳞癌根治术预后关系[J].中华胸心血管外科杂志, 2014, 30(2):76-78. DOI:10.3760/cma.j.issn.1001-4497.2014.02.004.
Chen YM, Chen JQ, Zhu KS, et al.The relationship between number of metastatic lymph node and prognosis of thoracic-esophageal cancer patients treated with radical resection[J].Chin J Thorac Cardiovasc Surg, 2014, 30(2):76-78. doi: 10.3760/cma.j.issn.1001-4497.2014.02.004[4] 李菲, 黄俊星, 张俊.18F-FDG PET/CT在食管癌中的临床应用[J].国际放射医学核医学杂志, 2016, 40(4):282-286. DOI:10.3760/cma.j.issn.1673-4114.2016.04.009.
Li F, Huang JX, Zhang J.The clinical application of 18F-FDG PET/CT in esophageal cancer[J].Int J Radiat Med Nucl Med, 2016, 40(4):282-286. doi: 10.3760/cma.j.issn.1673-4114.2016.04.009[5] Rice TW, Blackstone EH, Rusch VW.7th edition of the AJCC Cancer Staging Manual:esophagus and esophagogastric junction[J].Ann Surg Oncol, 2010, 17(7):1721-1724.DOI10.1245/s10434-010-1024-1. doi: 10.1245/s10434-010-1024-1 [6] Rusch VW, Asamura H, Watanabe H, et al.The IASLC lung cancer staging project:a proposal for a new international lymph node map in the forthcoming seventh edition of the TNM classification for lung cancer[J].J Thorac Oncol, 2009, 4(5):568-577. DOI:10.1097/JTO.0b013e3181a0d82e. [7] 黄伟鹏, 许建生, 陈洁容, 等.胸段食管癌淋巴结转移分布特征的螺旋CT表现[J].中国临床医学影像杂志, 2009, 20(4):236-239. DOI:10.3969/j.issn.1008-1062.2009.04.003.
Huang WP, Xu JS, Chen JR, et al.CT features of lymph node metastases of thoracic esophageal carcinoma[J].J Chin Clin Med Imaging, 2009, 20(4):236-239. doi: 10.3969/j.issn.1008-1062.2009.04.003[8] Pennathur A, Gibson MK, Jobe BA, et al.Oesophageal carcinoma[J].Lancet, 2013, 381(9864):400-412. DOI:10.1016/S0140-6736(12)60643-6. [9] 王秀芳, 郑玄中, 靳宏星.食管癌淋巴结转移影像诊断方法及进展[J].肿瘤研究与临床, 2009, 21(5):356-358. DOI:10.3760/cma.j.issn.1006-9801.2009.05.027.
Wang XF, Zheng XZ, Jin HX.Imaging diagnosis methods and progress for lymph node metastasis in esophageal carcinoma[J].Cancer Res Clin, 2009, 21(5):356-358. doi: 10.3760/cma.j.issn.1006-9801.2009.05.027[10] Ohashi S, Miyamoto S, Kikuchi O, et al.Recent advances from basic and clinical studies of esophageal squamous cell carcinoma[J].Gastroenterology, 2015, 149(7):1700-1715. DOI:10.1053/j.gastro.2015.08.054. [11] 姚沛旭, 许建生, 黄伟鹏, 等.容积CT和重建技术对食管癌术前评分法N分期的研究[J].中国CT和MRI杂志, 2007, 5(2):22-24. DOI:10.3969/j.issn.1672-5131.2007.02.008.
Yao PX, Xu JS, Huang WP, et al.A study of integrated scoring system by spiral CT volume scan and reconstruction on preoperative N staging of esophageal carcinoma[J].Chin J CT MRI, 2007, 5(2):22-24. doi: 10.3969/j.issn.1672-5131.2007.02.008[12] Yoon YC, Lee KS, Shim YM, et al.Metastasis to regional lymph nodes in patients with esophageal squamous cell carcinoma:CT versus FDG PET for presurgical detection-prospective study[J].Radiology, 2003, 227(3):764-770. DOI:10.1148/radiol.2281020423. [13] Kato H, Kuwano H, Nakajima M, et al.Comparison between positron emission tomography and computed tomography in the use of the assessment of esophageal carcinoma[J].Cancer, 2002, 94(4):921-928. DOI:10.1002/cncr.10330. [14] Tan R, Yao SZ, Huang ZQ, et al.Combination of FDG PET/CT and contrast-enhanced MSCT in detecting lymph node metastasis of esophageal cancer[J].Asian Pac J Cancer Prev, 2014, 15(18):7719-7724. DOI:10.7314/APJCP.2014.15.18.7719. [15] 姚树展, 刘松涛, 韩广秀, 等.PET/CT在胸段食管癌诊断与淋巴分期中的应用价值[J].医学影像学杂志, 2009, 19(7):835-838. DOI:10.3969/j.issn.1006-9011.2009.07.015.
Yao SZ, Liu ST, Han GX, et al.The applicable value of PET/CT in diagnosing and lymphatic staging for thoracic esophageal cancer[J].J Med Imaging, 2009, 19(7):835-838. doi: 10.3969/j.issn.1006-9011.2009.07.015[16] 谭茹, 朱仁娟, 葛全序, 等.18F-FDG PET/CT和增强MSCT评价食管癌淋巴结转移[J].中华核医学杂志, 2007, 27(6):356-359. DOI:10.3760/cma.j.issn.2095-2848.2007.06.012.
Tan R, Zhu RJ, Ge QX, et al.The application of 18F-FDG PET/CT and contrast enhanced MSCT in detecting metastatic lymph nodes in esophageal cancer[J].Chin J Nucl Med, 2007, 27(6):356-359. doi: 10.3760/cma.j.issn.2095-2848.2007.06.012 -

 点击查看大图
点击查看大图

计量
- 文章访问数: 3012
- HTML全文浏览量: 1654
- PDF下载量: 3