


 下载:
下载:

-
骨恶性淋巴瘤是一种淋巴结外的恶性淋巴瘤,可发生于任何年龄,男性发病者多于女性,约为1.3:1。骨恶性淋巴瘤可分为原发性骨淋巴瘤和继发性骨淋巴瘤,病理上又可分为霍奇金淋巴瘤和非霍奇金淋巴瘤。原发性骨淋巴瘤临床少见,传统X射线诊断存在一定困难;继发性骨淋巴瘤是淋巴瘤结外侵犯的重要部位之一,直接影响到淋巴瘤的分期、预后及治疗。传统断层影像(CT、MRI)对继发性骨淋巴瘤多有分析报道,但对其18F-FDG PET/CT的影像学表现的报道较少,本研究旨在探讨继发性骨淋巴瘤在18F-FDG PET/CT显像中的影像学特点,现报道如下。
-
收集2012年4月至2015年6月在我院行PET/CT检查,并经骨、淋巴结或肿块活检行病理学检查及免疫组化证实的淋巴瘤患者共46例(霍奇金淋巴瘤6例、非霍奇金淋巴瘤40例),均诊断为继发性骨淋巴瘤,其中,男性25例、女性21例,年龄7~77岁,中位年龄49岁。46例中骨活检3例(活检部位分别为右侧胫骨、右侧髂骨及L4椎体),余43例行髂棘穿刺,证实为骨淋巴瘤25例,阴性18例(经化疗后复查PET/CT,原高代谢灶活性明显减低)。
-
PET/CT仪型号为Discovery LS16(美国GE公司),18F由我科Minitrace回旋加速器(美国GE公司)生产,18F-FDG由Tracelab FXFN全自动合成装置(美国GE公司)合成,放射化学纯度 > 95%。
-
所有患者签署相关知情同意书后,于检查前禁食6 h以上,检查当日空腹血糖浓度控制在3.9~6.1 mmol/L。18F-FDG注射剂量为3.70~4.81 MBq/kg,注药后患者平卧休息45~60 min后采集图像。CT采集条件为管电压120 kV,管电流130~160 mA,层厚5.0 mm,显像范围为颅顶部至双侧大腿上段。PET体部采集为二维模式,3.5~4.0 min/床位,头部采集为三维模式,10 min/床位。PET数据通过Xeleris工作站配套软件利用CT图像信息进行衰减校正,采用有序子集最大期望值迭代法进行图像重建,层厚5.0 mm。
-
分别分析病变部位、数目以及骨质变化的CT、PET及融合图像,测量各病灶SUVmax及骨穿部位(髂棘)SUVmax。所有图像均由2位有经验的核医学科医师共同阅片诊断。
-
继发性骨淋巴瘤的影像学表现多样,可分为浸润型、溶骨型、硬化型和混合型等[1]。这几种类型可依照如下标准划分:首先,病灶为高代谢灶,以病灶SUV高于纵隔血池判定为代谢增高。其次,①骨髓浸润型:CT图像提示骨质无明显改变,而PET图像提示代谢增高;②溶骨型:表现为浸润性或“虫蚀样”破坏,骨内可见斑片状破坏透亮区,边缘不清楚;③硬化型:表现为骨质密度的局限增高;④混合型:表现为溶骨性骨质破坏区内有散在的斑片状、絮状致密影或破坏区周围形成不规则、密度不均匀的骨硬化[2]。
-
常规行单侧髂棘穿刺活检、骨髓病理组织学及免疫组化检查。
-
采用SPSS19.0软件进行统计学分析,将骨髓穿刺结果分为阴性和阳性两组,分别记录两组18F-FDG PET/CT显像相应穿刺部位(髂棘)SUV,采用P-P图与Q-Q图验证两组SUV是否符合正态分布,并进行独立样本t检验,P < 0.05表示差异具有统计学意义。同时,绘制穿刺部位SUV诊断继发性骨淋巴瘤的受试者工作特征曲线(receiver operating characteristic curve,ROC),根据曲线下面积值评价其诊断价值。根据Youden指数计算最佳诊断临界值(cut-off值)、灵敏度和特异度。
-
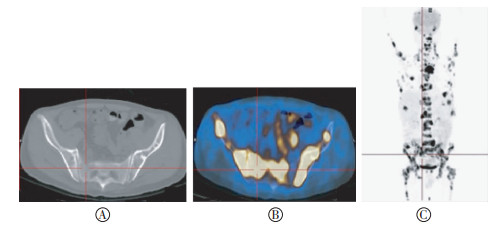
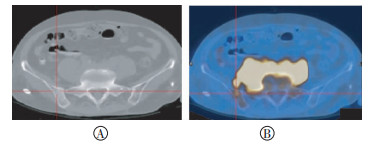
本组46例继发性骨淋巴瘤患者的18F-FDG PET/CT显像结果显示骨质异常表现可分为:(1)骨髓浸润型31例(67.40%),全身弥漫性或局部骨髓代谢活性增高,病灶的最高SUVmax可达18.3,全身弥漫者代谢以中轴骨及骨盆为明显,同层面CT均未见骨质密度异常(图 1)。(2)混合型10例(21.80%),其中,①伴骨髓浸润型9例(19.57%),CT表现为溶骨型、硬化型及骨髓浸润型并存,部分病灶骨质密度异常增高,部分病灶表现为溶骨性骨质破坏(图 2),伴有或不伴有软组织肿块影,有1例伴有膨胀型骨质破坏,同层面PET提示代谢增高,SUVmax为26.6,部分病灶局部代谢明显增高,SUVmax为17.9,同层面CT未见骨质密度异常表现;②不伴骨髓浸润型1例(2.17%),为单发病灶,位于右侧髂骨,CT表现为单骨内破坏和硬化并存,破坏区边缘或分隔硬化,周围伴有软组织肿块影,SUVmax为16.0。(3)硬化型3例(6.52%),均为单发,分别位于右侧锁骨、左侧髋臼、T7椎体,CT图像表现为骨质密度呈斑点状、结节状异常增高,右侧锁骨病灶伴有软组织密度影,同层面PET提示代谢增高,SUVmax分别为21.0、12.2、3.0(图 3)。(4)溶骨型2例(4.34%),CT表现为不同程度溶骨性骨质破坏,边缘无硬化、增生,破坏区周围伴有软组织密度肿块影,同层面PET提示代谢不同程度增高。溶骨型2例中1例单发于右侧髂骨,伴软组织密度影,SUVmax为26.7(图 4);1例为多发病灶(位于左侧顶骨、右侧髂骨、左侧髋臼及左侧第2前肋),各病灶均伴有软组织密度影,其中左侧第2前肋及右侧髂骨病灶呈膨胀型改变,表现为骨皮质膨大、变薄,SUVmax为8.5。本组46例中,伴溶骨型共3例(6.52%,包括混合型中1例),伴硬化型共9例(19.57%,包括混合型中6例),混合型共10例(21.74%),伴骨髓浸润型40例(86.96%,包括混合型中9例)。
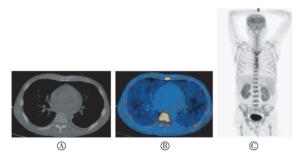
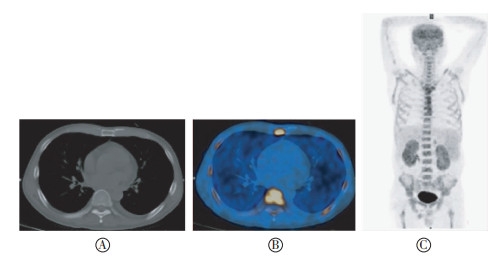
图 1 患者男性,59岁,B细胞淋巴瘤,骨髓浸润型。图中,A:CT图像;B:18F-FDG PET/CT融合图像;C:全身最大密度投影图像。图像显示病灶表现为全身弥漫性分布,CT图像示骨质未见明显改变。
Figure 1. B cell lymphoma in a 59-year-old man, bone marrow infiltration type
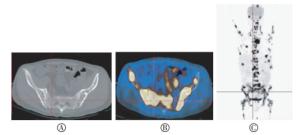
图 2 患者男性,45岁,滤泡性淋巴瘤伴弥漫性大B细胞淋巴瘤,混合型。图中,A:CT图像;B:18F-FDG PET/CT融合图像;C:全身最大密度投影图像。图像见全身多发异常浓聚灶,CT见不同类型的骨质异常改变并存。
Figure 2. Follicular lymphoma with diffuse large B cell lymphoma in a 45-year-old man, mixed type
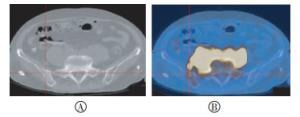
图 3 患者女性,77岁,外周T细胞淋巴瘤,硬化型。图中,A:CT图像;B:18F-FDG PET/CT融合图像。CT示右侧髂骨见局部骨质呈骨质硬化型改变,PET显像呈高摄取,SUVmax为21.0。
Figure 3. Peripheral T cell lymphoma in a 77-year-old woman, sclerosis type
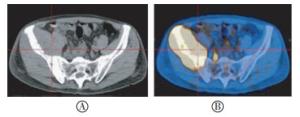
图 4 患者男性,65岁,弥漫性大B细胞淋巴瘤,溶骨型。图中,A:CT图像;B:18F-FDG PET/CT融合图像。CT示右侧髂骨见骨质破坏伴软组织肿块影,PET显像呈高摄取,SUVmax为26.7。
Figure 4. Diffuse large B cell lymphoma in a 65-year-old man, osteolysis type
-
本组46例患者中,病灶全身弥漫性分布18例(39.13%),均为骨髓浸润型;多发18例(39.13%),其中溶骨型1例,骨髓浸润型8例,混合型9例;单发10例(21.74%),其中溶骨型1例,骨质硬化型3例,混合型1例,骨髓浸润型5例。
-
本组46例患者中,肱骨、股骨均受累23例(50.00%),SUV max为1.1~17.9;肱骨、股骨均无受累14例(30.43%),均为骨髓浸润型表现;单纯肱骨受累5例(10.87%),SUVmax为1.9~6.6;单纯股骨受累4例(8.70%),SUVmax为1.7~2.3。
-
骨髓穿刺阳性组SUV为4.60±2.73,阴性组为1.92±1.60,两组SUV符合正态分布,行独立样本t检验,t=4.036,P < 0.001,差异有统计学意义,表明骨髓穿刺阳性组的SUV高于阴性组。
-
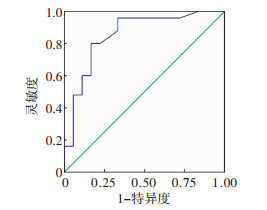
穿刺部位SUV诊断继发性骨淋巴瘤的ROC(图 5)结果显示,穿刺部位SUV诊断继发性骨淋巴瘤的曲线下面积值为0.856(95%CI:0.734~0.977),当SUV大于cut-off值2.35时,其诊断继发性骨淋巴瘤的特异度和灵敏度分别为83.3%和80.0%。
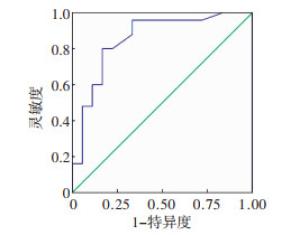
图 5 穿刺部位SUV诊断继发性骨淋巴瘤的受试者工作特征曲线
Figure 5. Receiver operating characteristic curve of SUV in the puncture sites in the diagnosis of secondary bone lymphoma
-
继发性骨淋巴瘤为结外骨髓受侵,可发生于霍奇金淋巴瘤或非霍奇金淋巴瘤,全身骨骼均可受累,以中轴骨多见[3],通常提示淋巴瘤骨髓广泛浸润(Ⅳ期),约占所有非霍奇金淋巴瘤的20%~40%。骨淋巴瘤是一种少见的结外恶性淋巴瘤,占骨原发恶性肿瘤的3%,占结外淋巴瘤的5%[1]。本组46例继发性骨淋巴瘤骨质破坏类型呈多样化,但存在一定的特征性,以骨髓浸润型最为多见[占86.96%(包括混合型中的9例)],病灶分布范围以多发或全身弥漫分布为多见(各占39.13%)。当病灶表现为溶骨性骨质破坏时,多数伴有软组织肿块(本组2例溶骨坏型均伴有软组织肿块影)。文献报道18F-FDG PET/CT无论是对霍奇金淋巴瘤还是非霍奇金淋巴瘤骨髓受侵,均有较高的特异度或灵敏度,在CT无骨质密度异常改变未能检出病灶的情况下,PET能够显示出更多骨髓受侵病灶[4]。本研究中,伴肱骨或股骨受累32例(69.57%),肱骨和股骨同时受累23例(占50.00%),均为骨髓浸润型表现,可能成为继发性骨淋巴瘤的影像学特点之一,但目前尚未查阅到相关文献。由于骨淋巴瘤的发病率低,本研究所收集的病例数有限,有待进一步积累、增加样本量进行深入研究。
长期以来,骨髓活检是诊断淋巴瘤骨髓浸润的主要方法,但是淋巴瘤浸润骨髓有时可表现为局灶性分布,骨髓穿刺结果受取材部位限制及标本量的影响,可能出现假阴性。既往亦有文献报道,PET/CT对非霍奇金淋巴瘤骨髓浸润的检出率高于骨髓穿刺[5-6]。本组研究中,有18例骨髓穿刺阴性,该组穿刺部位(髂棘)的SUV明显低于阳性组,ROC提示当SUV大于cut-off值2.35时,其诊断继发性骨淋巴瘤的特异度和灵敏度分别为83.3%和80.0%,说明穿刺部位阳性率与该部位SUV呈正相关,故18F-FDG PET/CT显示的高代谢部位对骨髓穿刺部位的选择具有指导意义。有报道称,对于PET/CT诊断为阳性,并且局灶性浸润的侵袭性非霍奇金淋巴瘤患者,可以在PET/CT引导下进行骨髓穿刺[7]。
结合以上影像学特点及相关性分析,18F-FDG PET/CT在继发性骨淋巴瘤的诊断和鉴别诊断上具有相对优势。需与继发性骨淋巴瘤进行鉴别诊断的疾病包括:(1)原发性骨淋巴瘤。目前公认的原发性骨淋巴瘤的诊断标准为:①肿瘤首发部位在骨骼;②临床和其他辅助检查如影像学检查未发现骨骼外其他部位淋巴瘤;③在骨内病灶确诊为淋巴瘤后6个月,骨外仍未发现其他淋巴瘤病灶;④病理组织形态学和免疫组化证实[8]。分析原发性骨淋巴瘤和继发性骨淋巴瘤的PET/CT表现具有重要的临床意义,明确原发性抑或继发性骨淋巴瘤是临床选用合适的治疗手段及判断预后的关键。继发性骨淋巴瘤是骨外淋巴瘤的晚期浸润或直接侵犯,属于Ⅳ期,而原发性骨淋巴瘤属于Ⅰ期,两者的治疗疗效及预后存在很大差别,但在组织学上很难将两者区分[9-10],PET/CT对除骨骼外其他病灶的显示有利于鉴别,如对全身多发高代谢淋巴结、其他部位肿块或肝脾肿大等淋巴瘤浸润的判定具有较高价值,同时,可有效帮助分期及评估疗效[11]。(2)多发性骨髓瘤。该病发病年龄较大,以多发型为多见,常见“钻孔样”、“虫蚀样”骨质破坏,边缘清楚,硬化少见,且伴骨髓浸润、累及肱骨和(或)股骨者鲜有,可同时结合病史及相关实验室检查进行鉴别。(3)骨转移瘤。该病可表现为溶骨性骨质破坏、骨质硬化或混合型等,溶骨性破坏可伴有膨胀性改变,但骨髓浸润型较少见,股骨、肱骨受累者亦不常见,且大多有原发肿瘤的症状,部分可伴有肿瘤标志物水平升高,18F-FDG PET/CT可显示原发灶。
继发性骨淋巴瘤的18F-FDG PET/CT影像学表现
Analysis on 18F-FDG PET/CT imaging characteristics in secondary bone lymphoma
-
摘要:
目的 探讨继发性骨淋巴瘤在18F-FDG PET/CT显像中的影像学特点。 方法 对2012年4月至2015年6月行全身18F-FDG PET/CT显像的46例继发性骨淋巴瘤患者的PET/CT影像学表现进行回顾性分析。并将骨髓穿刺结果分为阳性和阴性两组,对两组显像相应穿刺部位(髂棘)SUV进行独立样本t检验,同时绘制穿刺部位SUV诊断继发性骨淋巴瘤的受试者工作特征曲线(ROC)。 结果 46例继发性骨淋巴瘤患者中,霍奇金淋巴瘤6例、非霍奇金淋巴瘤40例;单发10例,多发18例,全身弥漫分布18例。46例患者骨质异常表现多样,其中,骨髓浸润型31例(67.40%)、混合型10例(21.74%)、硬化型3例(6.52%)、溶骨型2例(4.34%)。46例患者中肱骨或股骨受累32例(69.57%),均为骨髓浸润型表现。骨髓穿刺阳性组及阴性组SUV独立样本t检验结果显示t=4.036,P < 0.001,提示两组差异有统计学意义。穿刺部位SUV诊断继发性骨淋巴瘤的ROC曲线结果显示SUV诊断界值为2.35,其诊断继发性骨淋巴瘤的特异度和灵敏度分别为83.3%和80.0%。 结论 继发性骨淋巴瘤的18F-FDG PET/CT影像学表现存在一定的特征性,在该病的诊断与鉴别诊断中具有重要的临床价值,且对骨髓穿刺部位的选择具有指导意义。 -
关键词:
- 氟脱氧葡萄糖F18 /
- 正电子发射断层显像术 /
- 体层摄影术, X线计算机 /
- 继发性骨淋巴瘤
Abstract:Objective To investigate the 18F-FDG PET/CT imaging characteristics in secondary bone lymphoma. Methods A total of 46 patients with 18F-FDG PET/CT imaging of secondary bone lymphoma from April 2012 to June 2015 were selected; the PET/CT imaging characteristics were retrospectively analyzed. The patients were divided according to the results of their bone marrow biopsies:negative and positive groups. The SUV of the biopsy sites in 18F-FDG PET/CT imaging between the two groups were compared by independent sample t test, and the receiver operating characteristic curve(ROC) of the SUV in the puncture sites in the diagnosis of secondary bone lymphoma was drawn. Results The 46 cases of secondary bone lymphoma included 6 cases of Hodgkin's lymphoma and 40 cases of non-Hodgkin's lymphoma. The cases comprised 10 cases of single bone lesion, 18 cases of multiple bone lesions, and 18 cases of diffuse bone lesions in the whole body. The bone densities of the 46 cases were abnormal with the following conditions:31 cases of bone marrow infiltration type(67.40%), 10 cases of mixed type(21.74%), 3 cases of sclerosis type(6.52%), and 2 cases of osteolysis type(4.34%); 32 cases of humeral or femoral involvement(69.57%) with the bone marrow infiltration type was included. The independent sample t-test in the negative and positive groups showed a t value of 4.036, P < 0.001, revealing that the difference was statistically significant. The ROC curve of the SUV in the puncture sites in the diagnosis of secondary bone lymphoma showed a cut-off value of 2.35; the specificity and sensitivity of the diagnosis of secondary bone lymphoma were 83.3% and 80.0%, respectively. Conclusions The PET/CT imaging features of secondary bone lymphoma showed certain characteristics that are important and of clinical value to the diagnosis and differential diagnosis of secondary bone lymphoma, thus revealing that it has instructional significance for choosing biopsy sites. -
图 1 患者男性,59岁,B细胞淋巴瘤,骨髓浸润型。图中,A:CT图像;B:18F-FDG PET/CT融合图像;C:全身最大密度投影图像。图像显示病灶表现为全身弥漫性分布,CT图像示骨质未见明显改变。
Figure 1. B cell lymphoma in a 59-year-old man, bone marrow infiltration type
图 2 患者男性,45岁,滤泡性淋巴瘤伴弥漫性大B细胞淋巴瘤,混合型。图中,A:CT图像;B:18F-FDG PET/CT融合图像;C:全身最大密度投影图像。图像见全身多发异常浓聚灶,CT见不同类型的骨质异常改变并存。
Figure 2. Follicular lymphoma with diffuse large B cell lymphoma in a 45-year-old man, mixed type
图 3 患者女性,77岁,外周T细胞淋巴瘤,硬化型。图中,A:CT图像;B:18F-FDG PET/CT融合图像。CT示右侧髂骨见局部骨质呈骨质硬化型改变,PET显像呈高摄取,SUVmax为21.0。
Figure 3. Peripheral T cell lymphoma in a 77-year-old woman, sclerosis type
图 4 患者男性,65岁,弥漫性大B细胞淋巴瘤,溶骨型。图中,A:CT图像;B:18F-FDG PET/CT融合图像。CT示右侧髂骨见骨质破坏伴软组织肿块影,PET显像呈高摄取,SUVmax为26.7。
Figure 4. Diffuse large B cell lymphoma in a 65-year-old man, osteolysis type
-
[1] 李营.骨恶性淋巴瘤的影像学分析[J].微创医学, 2012, 7(6):630-632. DOI:10.3969/j.issn.1673-6575.2012.06.024.
Li Y. Imaging analysis of malignant lymphoma of bone[J].J Minim Invasive Med, 2012, 7(6):630-632. doi: 10.3969/j.issn.1673-6575.2012.06.024[2] 范娇娇, 崔建岭.原发性骨淋巴瘤的临床、病理及影像研究进展[J].国际医学放射学杂志, 2016, 39(2):171-174. DOI:10.19300/j.2016.Z3658.
Fan JJ, Cui JL.Advances in clinical, pathological and imaging research in primary lymphoma of bone[J].Int J Med Radiol, 2016, 39(2):171-174. doi: 10.19300/j.2016.Z3658[3] 高晓玉, 刑伟.以肋骨侵犯为首发的儿童骨淋巴瘤一例[J].中国医学计算机成像杂志, 2014, 20(3):299-300.
Gao XY, Xing W.Lymphoma of bone with initial presentation as a cervical rib mass[J].Chin Comput Med Imag, 2014, 20(3):299-300.[4] 李中泉, 谢丽璇, 张海捷, 等.骨淋巴瘤的18F-FDG PET/CT表现[J].临床军医杂志, 2015, 43(2):189-191, 199. DOI:10.3969/j.issn.1671-3826.2015.02.26.
Li ZQ, Xie LX, Zhang HJ, et al.Characteristics of 18F-FDG PET/CT imaging in bone lymphoma[J].Chin J Med Offic, 2015, 43(2):189-191, 199. doi: 10.3969/j.issn.1671-3826.2015.02.26[5] Schaefer NG, Strobel K, Taverna C, et al.Bone involvement in patients with lymphoma:the role of FDG-PET/CT[J].Eur J Nucl Med Mol Imaging, 2007, 34(1):60-67. DOI:10.1007/s00259-006-0238-8. [6] Pelosi E, Penna D, Douroukas A, et al.Bone marrow disease detection with FDG-PET/CT and bone marrow biopsy during the staging of malignant lymphoma:results from a large multicentre study[J].Q J Nucl Med Mol Imaging, 2011, 55(4):469-475. [7] 岳进, 苏丽萍.全身MRI与PET/CT在淋巴瘤骨髓浸润诊断及预后中的作用[J].国际放射医学核医学杂志, 2016, 40(1):50-54. DOI:10.3760/cma.j.issn.1673-4114.2016.01.010.
Yue J, Su LP.Function of whole-body MRI and PET/CT in the diagnosis and prognosis of lymphoma with bone marrow infiltration[J].Int J Radiat Med Nucl Med, 2016, 40(1):50-54. doi: 10.3760/cma.j.issn.1673-4114.2016.01.010[8] 刘玉林, 陈宪, 付荣, 等.骨淋巴瘤的CT、MRI表现[J].中国肿瘤影像学, 2009, 2(3):68-71. DOI:10.3969/j.issn.1009-4393.2009.14.016.
Liu YL, Chen X, Fu R, et al.CT and MRI imaging of bone lymphoma[J].Chin J Oncoradiol, 2009, 2(3):68-71. doi: 10.3969/j.issn.1009-4393.2009.14.016[9] 罗泽斌, 陈晓东, 黄泽光.原发性骨淋巴瘤影像学诊断及鉴别诊断[J].实用放射学杂志, 2012, 28(10):1599-1603. DOI:10.3969/j.issn.1002-1671.2012.10.029.
Luo ZB, Chen XD, Huang ZG.Imaging diagnosis and differential diagnosis of primary bone lymphoma[J].J Pract Radiol, 2012, 28(10):1599-1603. doi: 10.3969/j.issn.1002-1671.2012.10.029[10] 陈桂美, 李先玉.骨原发性淋巴瘤的影像学诊断与鉴别诊断[J].江西医药, 2015, 50(12):1345-1347. DOI:10.3969/j.issn.1006-2238.2015.12.013.
Chen GM, Li XY.Imaging diagnosis and differential diagnosis of primary bone lymphoma[J].Jiangxi Med J, 2015, 50(12):1345-1347. doi: 10.3969/j.issn.1006-2238.2015.12.013[11] 王全师, 吴湖炳, 王明芳, 等.18F-FDG显像对淋巴瘤分期及疗效评价的价值[J].中华核医学杂志, 2004, 24(1):8-10. DOI:10.3760/cma.j.issn.2095-2848.2004.01.003.
Wang QS, Wu HB, Wang MF, et al.18F-FDG PET imaging for staging and treatment evaluation in lymphoma[J].Chin J Nucl Med, 2004, 24(1):8-10. doi: 10.3760/cma.j.issn.2095-2848.2004.01.003 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 2874
- HTML全文浏览量: 1811
- PDF下载量: 5