



-
目前,精准肝脏外科已经普遍被业内学者认识[1-2],右半肝活体肝移植(live donor liver transplantation,LDLT)术前对供肝的精准评估关系着移植肝的预后及供体的恢复。IQQA®-Liver肝脏CT影像解读分析系统提供了一个高自动化、全方位、即时、定量分析的综合平台,支持医师快速实时地对动态多期肝脏影像进行肝脏、肝段、病灶、血管(包括肝动脉、肝静脉、肝门脉)的分割、标记、容积测量以及相互空间关系的定量评估。本文分析了92例LDLT供体的临床资料,从右半肝体积评估及肝静脉引流域入手,评估IQQA-Liver三维系统在肝移植术精准手术选择中的临床价值。
-
2011年1月至2014年5月,在我院东方器官移植中心行右半肝LDLT手术的供体共92例,包括男性73例、女性19例,年龄21~59岁,平均(34.3±1.4)岁,体重43~93 kg,平均(68.89±4.82)kg。所有供者均经过询问临床病史、体格检查、超声及实验室检查,签署知情同意书,自愿捐肝并经医院伦理委员会审核批准,在术前1周内完成多层螺旋CT扫描,行移植肝带肝中静脉(middle hepatic vein,MHV)术式者59例,不带MHV术式者33例。
-
与供体相对应的92例受体中,男性64例、女性28例,年龄23~71岁,平均(47.5±2.1)岁,体重42.5~117 kg,平均(77.29±3.65)kg。92例受体患原发病的情况为乙肝后肝硬化38例,合并肝癌12例;丙肝后肝硬化32例,合并肝癌8例;原发性肝癌5例;原发酒精性肝硬化8例;隐源性肝硬化4例;原发性硬化性胆管炎2例;肝豆状核变性2例;胆汁淤积性肝硬化1例。
-
采用美国GE Light speed QX/i16排螺旋CT对所有供体行腹部平扫及增强扫描,管电压120 kV,管电流260 mA,扫描层厚10 mm,螺距1.375:1。采用高压注射器经肘前静脉注入非离子型对比剂欧乃派克(350 mgI/ml),注射流率为3 ml/s,剂量为1.5 ml/kg。门脉流入期延迟时间为40~45 s,门脉期60~75 s。每份原始数据均重建为2.0 mm层厚、1.25 mm间隔。
-
将原始数据分别传送到GE ADW4.2工作站及IQQA®-Liver肝脏CT影像解读分析系统(美国EDDA科技公司),由两名经验丰富的影像诊断医师分别测量一次,取平均值为最终肝体积。
-
在GE ADW4.2工作站选取门脉期,从肝顶开始每4层圆滑勾画肝轮廓,把肝门区门静脉、下腔静脉、大的肝裂等结构排除在外,然后计算得出CT全肝体积(CTV 全)。同样方法以MHV中线(下腔静脉与胆囊窝长轴)为界勾画右半肝轮廓,得出CT右半肝体积(CTV)。
-
载入原始数据到IQQA-Liver肝脏CT影像解读分析系统,系统自动根据肝脏解剖位置及肝脏密度勾画出每层的肝实质轮廓,手动修正,将大结构排除在外,结束修改得到全肝体积(IQQAV 全)。在全肝轮廓基础上以MHV为界,用可调节曲面或手动切割功能进行自动化肝脏分割得到右半肝体积,用IQQA体积表示(IQQAV)。分别标记门静脉右支、左支、Ⅳ段支(图 1中A),得出门脉右支流域体积(right portal vein territorial volume,RPVTV),相当于术中阻断门脉及肝动脉血流时沿缺血线所得的右半肝体积。

图 1 IQQA-Liver门脉及肝静脉流域图中,A:门脉右支及Ⅳ段支的流域;B:肝静脉Ⅴ、Ⅷ、Ⅳ段属支流域。
Figure 1. Territorial volume of portal vein and hepatic vein by IQQA-Liver
-
由两名有经验的医师同时进行观察,主要观察并测定手术切面周围(Ⅴ、Ⅷ、Ⅳ段)的肝右静脉(right hepatic vein,RHV)、MHV属支及肝右后下静脉(inferior right hepatic vein,IRHV)的直径、走行。在IQQA-Liver肝脏CT影像解读分析系统上利用血管标记功能标记肝静脉主干及Ⅴ、Ⅷ、Ⅳ段属支,得出各属支的相互空间关系及相应流域(图 1中B),统计手术切面相关静脉直径,计算静脉直径与流域的相关性。依据术中切面选择及血管重建或假设重建情况计算相应右半肝体积为有效的功能肝体积(efficient functional hepatic volume,EFHV),其是受体可有效利用的部分,是RHV引流域与重建属支引流域体积之和。
-
术中取出供体右半肝后,灌入UW液(the University of Wisconsin solution),去除附着肝门结构和附属韧带组织,约20 min后,称重,用供肝质量除以肝密度(1 g/ml),计算得到术中体积(intraoperative volume,IOV)。
-
计算手动法、半自动法、门脉流域法计算的右半肝体积及EFHV、IOV与相应受体体重比值,即GRWR,并进行分级。
-
利用SPSS17.0软件进行统计学分析,所有计量资料用$\bar x \pm s$表示,符合正态分布进行配对t检验,非正态分布进行配对的秩和检验,并对组间数据进行两两相关性分析,P≤0.05表示差异有统计学意义。
-
手动法、半自动法测量全肝体积(CTV 全和IQQAV 全)分别为(1356.36±217.81)cm3和(1368.05±220.78)cm3,二者相关系数为0.96,P≤0.01,二者高度相关。手动法、半自动法测量右半肝体积(CTV和IQQAV)分别为(858.06±154.95)cm3和(847.81±155.14)cm3,二者相关系数为0.93,P≤0.01,二者高度相关。RPVTV、EFHV及IOV的平均值及范围见表 1。IQQAV与IOV、CTV与IOV、RPVTV与IOV、EFHV与IOV的相关系数分别为0.82、0.81、0.77、0.81,P均 < 0.01。
组别 例数 $\bar x \pm s$ 最小值 最大值 CTV 全 92 1356.36±217.81 755.77 1897.51 IQQAV 全 92 1368.05±220.78 722.22 1949.78 CTV 92 858.06±154.95 459.88 1188.14 IQQAV 92 847.81±155.14 465.88 1220.03 IOV 92 726.37±124.33 380.00 1132.00 RPVTV 92 789.52±148.44 507.72 1250.57 EFHV 92 822.29±154.79 405.52 1038.43 注:表中,CTV 全为手动法测量的全肝体积;IQQAV 全为半自动法测量的全肝体积;CTV为手动法测量的右半肝体积;IQQAV为半自动法测量的右半肝体积;IOV为术中体积;RPVTV为门脉右支流域体积;EFHV为有效的功能肝体积。 表 1 不同体积测量方法所得的全肝体积及右半肝体积的平均值范围(cm3)
Table 1. The total hepatic volume and right hemihepatic volume measured by 5 methods followed(cm3)
-
计算5种右半肝体积与其相应受体体重的比值,得到相应的GRWR,以0.8%、1.0%为界进行分级,结果见表 2及表 3。
组别 $\bar x \pm s$ 最小值 最大值 IOV-GRWR 1.01±0.21 0.68 1.85 CTV-GRWR 1.23±0.37 0.74 2.20 IQQAV-GRWR 1.22±0.37 0.78 2.26 RPVTV-GRWR 1.26±0.37 0.84 2.13 EFHV-GRWR 1.14±0.18 0.77 1.50 注:表中,IOV为术中体积;CTV为手动法测量的右半肝体积;IQQAV为半自动法测量的右半肝体积;RPVTV为门脉右支流域体积;EFHV为有效的功能肝体积;GRWR为移植物/受体体重比。 表 2 5种右半肝体积与相应受体体重比的平均值及范围(%)
Table 2. The graft-to-recipient body weight ratio from 5 methods followed(%)
组别 <0.8% 0.8%~1.0% >1.0% IOV-GRWR 9 47 36 CTV-GRWR 1 22 69 IQQAV-GRWR 1 20 71 EFHV-GRWR 2 25 65 RPVTV-GRWR 0 29 63 注:表中,IOV为术中体积;CTV为手动法测量的右半肝体积;IQQAV为半自动法测量的右半肝体积;RPVTV为门脉右支流域体积;EFHV为有效的功能肝体积;GRWR为移植物/受体体重比。 表 3 5组GRWR分级及相应例数
Table 3. Grades of GRWR and homologous mumber of cases
-
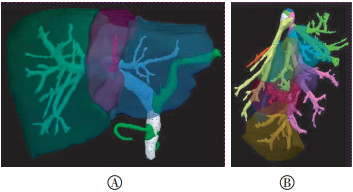
92例供肝手术切面相关血管共254支,包括MHV属支104支,RHV属支93支,IRHV属支57支,254支静脉直径为(4.10±1.72)mm,相应流域体积为(54.70±44.21)cm3,其相关系数为0.73,P≤0.01(图 2)。
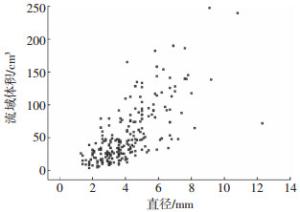
图 2 254支静脉直径与流域体积相关性的散点图
Figure 2. Scatter diagram about relativity between hepatic vein diameter and homologous territorial volume
-
本研究共59例选择扩大右半肝移植术(带MHV),33例选择右半肝移植术(不带MHV)。对比术中结果,行不带MHV术式的33例患者中,MHV属支<3 mm者4支,无重建;3~5 mm者18支,7支重建;5~7 mm者18支,17支重建,1支5 mm者未重建;≥7 mm者17支,均重建,其中1支搭桥。
CT手动法、IQQA半自动法及EFHV所计算的GRWR分别有1、1、2例<0.8%,CTV-GRWR最小值为0.74%,此受者的IQQAV-GRWR为0.85%,手术方式为带MHV术式,术后两周内肝功能恢复欠佳,经积极治疗,一个月后肝功能恢复正常。
IQQAV-GRWR最小值为0.78%的受者亦行带MHV术式,其对应的CTV-GRWR为0.81%,术中损坏膈肌致血气胸,术后10 d胆红素升高,肝功能持续下降,于术后7周再次行原位尸体肝移植,发现肿瘤种植转移,术中室颤,最后死亡。
EFHV-GRWR最小值为0.77%的受者术中MHV 5段、8段各一支(直径分别为5.7、4.2 mm)以冷保存的髂血管与受者肝中、肝左静脉共同开口搭桥吻合;RHV与受者RHV吻合,术后肝功能未见异常,伤口愈合良好后出院。EFHV-GRWR为0.79%的受者行带MHV术式,并重建肝右后下静脉,术后恢复良好。
-
手术前的精准评估越来越被外科医师认可[3],成为手术是否成功的必要条件。肝移植精准手术评估的要点主要包括:①确定手术方式,决定将MHV切给受者还是留给供者;②确定供肝EFHV和留给供者的剩余功能性肝体积;③确定肝切面相关脉管的分支数目、直径、走行长度、距离、变异情况等,同时了解MHV及IRHV的引流域。④确定需要切除、重建或搭桥的管道及相关术中注意事项。手术是否成功取决于两个基本因素:足够大的移植肝以满足受体代谢需要,足够大的残肝以让供者顺利渡过肝再生期。若供者剩余肝脏体积过小,也可能发生小肝综合征[4],文献报道世界范围内已经有19例供者死亡[5-6]。因此必须筛选合适的供者并精准评估供肝质量、体积、血管、胆管情况。CT和MRI是准确的肝体积测量方法[7],而新技术及新软件的进展也让评估越来越准确。
-
CT手动法的准确率高,具有可操作性及可重复性,但费时费力,得出的肝脏三维图像不够平滑。而半自动法多是利用软件处理原始多层螺旋CT图像,辅以影像医师修改,如日本的Virtual Place Lexus[8],德国的HepaVision[9]等。本研究中IQQA-Liver三维系统得出全肝体积及右半肝体积过程只需8~15 min,远短于手动法(约60 min)。并且IQQAV与IOV的相关性比CTV更好,分析可能是因为半自动法避免了人为操作误差,平滑性好,且仅需1次描绘,也有利于避免误差。
右半肝切除术中,门脉右支、右肝动脉分别阻断,此时可见肝脏表面的左右肝的缺血界面,再以此为标记进行切肝[10];RPVTV即模拟术中夹闭门脉右支及肝右动脉后的缺血右半肝。Wang等[11]研究利用门脉右支及左支的最大直径估算右半肝体积也是基于门脉左、右支的血流分布。因此RPVTV、EFHV与IOV均具有良好相关性,反映了模拟手术切面的可行性。
IOV计算是假设肝密度为1 g/ml,赖彦华等[1]研究亦参照1 ml肝体积重量为1 mg。而Lemke等[12]获取了16例右半肝LDLT中实测供肝体积及质量数据,证实平均肝实质密度是1.1172 g/ml。Radtke等[13]研究中发现人肝组织在0.9%NaCl中沉入水底,提示人肝组织的密度应 > 1.00 g/ml。另外,由于移植肝在称重时内部液体基本流失,高渗性UW液的灌注使得肝组织脱水,导致IOV与质量比术前小。一般带MHV的肝实质切面在MHV的左侧,并保留大约0.5 cm厚的肝实质以保护MHV[14];而不带MHV的切面为沿MHV右缘1 cm,延伸至上腔静脉到胆囊窝底[15],因此不带MHV的术式本来就比术前测量肝体积小,Marcos等[16]报道模拟切线和实际切肝线2 cm的偏移就会造成200 g肝组织的差异,这也是术前所测体积比IOV大的原因之一。
行右半肝LDLT时,手术切面大致沿夹闭肝右动脉及门静脉右支后的缺血线走行,即在MHV附近,应准确评估Ⅷ、Ⅴ段的MHV属支,由于Ⅷ、Ⅴ段亦存在RHV属支,使得LDLT术后Ⅷ、Ⅴ段静脉回流得以代偿,从而保证这部分的肝组织功能,因此应同时评估供肝到Ⅷ、Ⅴ段MHV及RHV属支,便于外科医师估计术后侧支循环生成的可能。IRHV要从下腔静脉分离,由于手术技巧等原因,静脉直径需足够大以方便重建,如>5 mm[17],因此其流域也面临着淤血问题,这对GRWR较小的移植肝,即“SFSG(small-for-size grafts)”非常重要,应保留较大的IRHV以保护右半肝的静脉引流。
右半肝LDLT中MHV的取舍是一直存在争论的焦点问题[18]。对于不带MHV的术式,医师在术前对移植肝内可能存在肝静脉淤血区域和范围进行精准预测,可以作为术中决策是否需重建肝静脉的依据[10]。由于手术技巧等原因,目前临床医师往往根据静脉属支的管径来决定是否需要重建,认为静脉直径需>5 mm[17],本研究发现静脉直径与引流域存在一定的相关性,但并非完全呈正比,一方面与血管在肝脏中的分布有关,另一方面也跟各属支走行长度及与根部距离有关。本研究结合静脉流域分析计算EFHV,为临床精准评估供肝体积提供重要参考,如果RHV的引流域足够大,满足GRWR > 0.8%,应将MHV留给供者;如果肝左静脉引流域 > 全肝体积的30%,应将MHV分配给移植物[19];对于GRWR < 0.8%、肝左静脉引流区域 < 全肝体积的30%的供者,应进一步计算MHV各分支的流域体积,如果在保证MHV引流域充分利用的情况下,能够满足GRWR > 0.8%和剩余肝脏体积 > 30%,应将MHV主干留给供者,对移植物中的MHV分支采取血管搭桥等方式进行重建。本研究与Sano等[20]的研究结果相同。
IQQA-Liver三维系统可以模拟手术切面,还原肝切面周围脉管结构的真实立体解剖构象,辅助术者进行术前规划、虚拟切割和风险评估,可以精确计算每一支血管的流域体积,进而准确计算分配给受者的供肝体积及供者剩余肝脏体积,显著提高外科医师的三维阅片水平和空间构象能力,这对于术前评估手术风险、制定手术计划具有重要意义。
IQQA-Liver对右半肝活体肝移植供肝体积及引流域精准评估的临床价值
Clinical significance of IQQA-Liver in the evaluation of liver volume and hepatic vein territory before live donor liver transplantation with a right lobe graft
-
摘要:
目的 探讨IQQA-Liver三维系统对右半肝活体肝移植(LDLT)术前精准评估肝体积及引流域的实用价值。 方法 分别以手动法及半自动法测量92例供体全肝体积(CTV 全、IQQAV 全)及右半肝体积(CTV、IQQAV),测定门脉右支引流域体积(RPVTV),模拟肝切面及静脉重建方案计算有效的功能肝体积(EFHV),并将这4种术前体积分别与术中体积(IOV)进行对比,采用组间数据配对t检验及组间数据两两相关分析进行数据处理,以P≤0.05为差异有统计学意义。统计分析肝静脉各属支直径与相应引流域的相关性。 结果 CTV 全与IQQAV 全分别为(1356.36±217.81)cm3和(1368.05±220.78)cm3,二者相关系数为0.96;CTV与IQQAV分别为(858.06±154.95)cm3和(847.81±155.14)cm3,二者相关系数为0.93。IOV为(726.37±124.33)cm3,RPVTV为(789.52±148.44)cm3,EFHV为(822.29±154.79)cm3。IQQAV与IOV、CTV与IOV、RPVTV与IOV、EFHV与IOV的相关系数分别为0.82、0.81、0.77、0.81,P均 < 0.01。254支手术切面相关血管直径与相应引流域的相关系数为0.73,P≤0.01。 结论 半自动法所测体积与IOV的相关性良好,肝静脉各属支的直径不能完全反映引流域体积,术前应计算EFHV,为临床提供更精准的术前评估。 Abstract:Objective To investigate the clinical significance of an IQQA-Liver three dimensional system in the evaluation of hepatic volume and hepatic venous drainage territory before live donor liver transplantation(LDLT) with a right lobe graft. Methods The total hepatic volume and right hemihepatic volume of 92 donors were determined with IQQA semiautomatic method(IQQAVtotal and IQQAV) and traditional CT manual method(CTVtotal and CTV). Right portal vein territorial volume(RPVTV) of 92 donors were determined, and efficient functional hepatic volume(EFHV) were obtained by simulating hepatic section and venous reconstruction schedule. The preoperative right hemihepatic volume obtained via four methods were compared with the intraoperative volume(IOV) in LDLT and then evaluated through paired t test and correlation analysis between interclass data. P≤0.05 was considered statistically significant. The relationship of the diameter and the territorial volume of 254 hepatic vein were analyzed. Results The correlation coefficients were 0.96 for CTVtotal and IQQAVtotal and 0.93 for CTV and IQQAV. The correlation coefficients were 0.82, 0.81, 0.77, and 0.81 for IQQAV, CTV, RPVTV, EFHV, and IOV, respectively. The correlation coefficient was 0.73 between the diameter and territorial volume of the hepatic vein(P≤0.01). Conclusions The hemihepatic volume obtained through IQQA-Liver was associated with IOV. However, the diameter of the tributaries of the hepatic vein cannot completely represent homologous territorial volume. EFHV should be calculated to evaluate a patient′s status before operation is performed. -
图 1 IQQA-Liver门脉及肝静脉流域图中,A:门脉右支及Ⅳ段支的流域;B:肝静脉Ⅴ、Ⅷ、Ⅳ段属支流域。
Figure 1. Territorial volume of portal vein and hepatic vein by IQQA-Liver
图 2 254支静脉直径与流域体积相关性的散点图
Figure 2. Scatter diagram about relativity between hepatic vein diameter and homologous territorial volume
表 1 不同体积测量方法所得的全肝体积及右半肝体积的平均值范围(cm3)
Table 1. The total hepatic volume and right hemihepatic volume measured by 5 methods followed(cm3)
组别 例数 $\bar x \pm s$ 最小值 最大值 CTV 全 92 1356.36±217.81 755.77 1897.51 IQQAV 全 92 1368.05±220.78 722.22 1949.78 CTV 92 858.06±154.95 459.88 1188.14 IQQAV 92 847.81±155.14 465.88 1220.03 IOV 92 726.37±124.33 380.00 1132.00 RPVTV 92 789.52±148.44 507.72 1250.57 EFHV 92 822.29±154.79 405.52 1038.43 注:表中,CTV 全为手动法测量的全肝体积;IQQAV 全为半自动法测量的全肝体积;CTV为手动法测量的右半肝体积;IQQAV为半自动法测量的右半肝体积;IOV为术中体积;RPVTV为门脉右支流域体积;EFHV为有效的功能肝体积。  下载: 导出CSV
下载: 导出CSV
表 2 5种右半肝体积与相应受体体重比的平均值及范围(%)
Table 2. The graft-to-recipient body weight ratio from 5 methods followed(%)
组别 $\bar x \pm s$ 最小值 最大值 IOV-GRWR 1.01±0.21 0.68 1.85 CTV-GRWR 1.23±0.37 0.74 2.20 IQQAV-GRWR 1.22±0.37 0.78 2.26 RPVTV-GRWR 1.26±0.37 0.84 2.13 EFHV-GRWR 1.14±0.18 0.77 1.50 注:表中,IOV为术中体积;CTV为手动法测量的右半肝体积;IQQAV为半自动法测量的右半肝体积;RPVTV为门脉右支流域体积;EFHV为有效的功能肝体积;GRWR为移植物/受体体重比。
下载: 导出CSV
表 3 5组GRWR分级及相应例数
Table 3. Grades of GRWR and homologous mumber of cases
组别 <0.8% 0.8%~1.0% >1.0% IOV-GRWR 9 47 36 CTV-GRWR 1 22 69 IQQAV-GRWR 1 20 71 EFHV-GRWR 2 25 65 RPVTV-GRWR 0 29 63 注:表中,IOV为术中体积;CTV为手动法测量的右半肝体积;IQQAV为半自动法测量的右半肝体积;RPVTV为门脉右支流域体积;EFHV为有效的功能肝体积;GRWR为移植物/受体体重比。
下载: 导出CSV
-
[1] 赖彦华, 董家鸿, 段伟东, 等.精准肝脏外科技术在活体肝移植供肝切取中的应用[J].中华外科杂志, 2015, 53(5):328-334. DOI:10. 3760/cma.j.issn. 0529-5815. 2015. 05. 003.
Lai YH, Dong JH, Duan WD, et al. Clinical application of precise liver surgery techniques for donor hepatectomy in living donor liver transplantation[J]. Chin J Surg, 2015, 53(5):328-334. doi: 10.3760/cma.j.issn.0529-5815.2015.05.003.[2] Qiu Y, Zhu X, Zhu R, et al. The clinical study of precise hemihepatectomy guided by middle hepatic vein[J]. World J Surg, 2012, 36(10):2428-2435. DOI:10. 1007/s00268-012-1662-5. [3] 王学栋.计算机辅助手术规划系统在精准肝脏外科中的应用研究[D].济南: 山东大学, 2013.
Wang XD. Application of computer assisted surgical planning system in precise liver surgery[D]. Jinan: Shandong University, 2013.[4] 蒋文涛, 沈中阳, 孙超, 等.预防活体肝移植后肝小体积综合征的综合措施[J].中华器官移植杂志, 2013, 34(1):17-19. DOI:10. 3760/cma.j.issn. 0254-1785. 2013. 01. 005.
Jiang WT, Shen ZY, Sun C, et al. Procedures to prevent development of small-for-size syndrome during living donor liver transplantation[J]. Chin J Organ Transplant, 2013, 34(1):17-19. doi: 10.3760/cma.j.issn.0254-1785.2013.01.005.[5] Trotter JF, Adam R, Lo CM, et al. Documented deaths of hepatic lobe donors for living donor liver transplantation[J]. Liver Transpl, 2006, 12(10):1485-1488. DOI:10. 1002/lt. 20875. [6] Coelho JC, De Freitas AC, Matias JE, et al. Donor complications including the report of one death in right-lobe living-donor liver transplantation[J]. Dig Surg, 2007, 24(3):191-196. DOI:10. 1159/000102898. [7] 李艳艳, 牟玲, 于文娟, 等.肝移植中全肝体积的CT和磁共振影像学测量准确性的荟萃分析[J].中华器官移植杂志, 2015, 36(2):97-101. DOI:10. 3760/cma.j.issn. 0254-1785. 2015. 02. 008.
Li YY, Mou L, Yu WJ, et al. The accuracy of CT and MR estimating whole liver volume:a meta-analysis[J]. Chin J Organ Transplant, 2015, 36(2):97-101. doi: 10.3760/cma.j.issn.0254-1785.2015.02.008.[8] Uchida K, Taniguchi M, Shimamura T, et al. Three-dimensional computed tomography scan analysis of hepatic vasculatures in the donor liver for living donor liver transplantation[J]. Liver Transpl, 2010, 16(9):1062-1068. DOI:10. 1002/lt. 22109. [9] Radtke A, Sotiropoulos GC, Sgourakis G, et al. "Anatomical" versus "territorial" belonging of the middle hepatic vein:virtual imaging and clinical repercussions[J]. J Surg Res, 2011, 166(1):146-155. DOI:10. 1016/j.jss. 2009. 07. 042. [10] 夏雷, 夏强.肝脏外科技术进展[J].国际外科学杂志, 2014, 41(4):282-284. DOI:10. 3760/cma.j.issn. 1673-4203. 2014. 04. 022.
Xia L, Xia Q. Progress in liver surgical techniques[J]. Int J Surg, 2014, 41(4):282-284. doi: 10.3760/cma.j.issn.1673-4203.2014.04.022.[11] Wang F, Pan KT, Chu SY, et al. Preoperative estimation of the liver graft weight in adult right lobe living donor liver transplantation using maximal portal vein diameters[J]. Liver Transpl, 2011, 17(4):373-380. DOI:10. 1002/lt. 22274. [12] Lemke AJ, Brinkmann MJ, Pascher A, et al. Accuracy of the CT-estimated weight of the right hepatic lobe prior to living related liver donation(LRLD) for predicting the intraoperatively measured weight of the graft[J]. Rofo, 2003, 175(9):1232-1238. DOI:10. 1055/s-2003-41938. [13] Radtke A, Sotiropoulos GC, Nadalin S, et al. Preoperative volume prediction in adult living donor liver transplantation:how much can we rely on it?[J]. Am J Transplant, 2007, 7(3):672-679. DOI:10. 1111/j. 1600-6143. 2006. 01656.x. [14] 范上达, 卢宠茂, 王伟林, 等.成人-成人间活体右半肝移植[J].肝胆外科杂志, 1999, 7(3):174-177.
Fan SD, Lu CM, Wang WL, et al. Adult-to-adult living donor liver transplantation using right lobe grafts[J]. J Hepatobiliary Surg, 1999, 7(3):174-177.[15] Pannu HK, Maley WR, Fishman EK. Liver transplantation:preoperative CT evaluation[J]. Radiographics, 2001, 21(suppl 1):S133-146. DOI:http://dx.doi.org/10.1148/radiographics.21.suppl_1.g01oc03s133 [16] Marcos A, Orloff M, Mieles L, et al. Functional venous anatomy for right-lobe grafting and techniques to optimize outflow[J]. Liver Transpl, 2001, 7(10):845-852. DOI:10. 1053/jlts. 2001. 27966. [17] Sugawara Y, Makuuchi M, Sano K, et al. Vein reconstruction in modified right liver graft for living donor liver transplantation[J]. Ann Surg, 2003, 237(2):180-185. DOI: 10. 1097/01.SLA. 0000048444. 40498. AD. [18] Radtke A, Schroeder T, Molmenti EP, et al. The "territorial belonging" of the middle hepatic vein:a troublesome dilemma in adult live donor liver transplantation--anatomical evidence based on virtual 3-dimensional-computed tomography-imaging reconstructions[J]. Eur J Med Res, 2006, 11(2):66-72. [19] 丁恩慈, 蒋文涛, 季倩, 等.活体肝移植术前评估肝静脉引流域的临床价值[J].中华器官移植杂志, 2012, 33(10):606-610. DOI:10. 3760/cma.j.issn. 0254-1785. 2012. 10. 009.
Ding EC, Jiang WT, Ji Q, et al. Clinical value of hepatic vein drainage territory evaluation before LDLT with right lobe graft[J]. Chin J Organ Transplant, 2012, 33(10):606-610. doi: 10.3760/cma.j.issn.0254-1785.2012.10.009.[20] Sano K, Makuuchi M, Miki K, et al. Evaluation of hepatic venous congestion:proposed indication criteria for hepatic vein reconstruction[J]. Ann Surg, 2002, 236(2):241-247. DOI:10. 1097/01. SLA. 0000021845. 89475. 00. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 2776
- HTML全文浏览量: 1472
- PDF下载量: 7