


-
盆底痉挛综合征(spastic pelvic floor syndrome,SPFS)的患者用力排粪时,盆底肌肉收缩不协调,从而导致不协调性排粪困难[1-2]。女性患者因盆腔生理解剖结构复杂,除表现为耻骨直肠肌相对肥厚、力排状态下肛直角减小外,常伴有多盆腔器官脱垂[3]。目前,动态MRI已在女性SPFS的评估中得到广泛应用,但对于合并疾病的诊断存在一定的假阴性,影响了术前评估及术后疗效评价的准确性。本研究旨在探讨直肠内注入模拟粪便的盆底动态MRI在女性SPFS患者影像学评估中的诊断优势。
-
回顾性分析2009年7月至2013年12月于我院肛肠外科诊断为SPFS并接受盆底动态MRI检查的53例女性患者的影像学资料。患者年龄14~78岁,平均年龄(52.7±15.8)岁,均符合RomeⅢ中关于功能性便秘及出口梗阻型便秘的诊断标准[2],并且均经结肠镜、下消化道造影或排粪造影检查排除结直肠器质性病变。
-
患者于检查前2~3 h采用甘油灌肠剂清洁直肠,检查前1 h开始储存尿液,以使膀胱处于半充盈状态。所有患者均采用我院自行设计的注入超声耦合剂的高顺应性球囊来模拟粪便,以反映盆底运动。检查时患者采用仰卧位,膝关节及髋关节屈曲,近似截石位,并多次训练做力排动作(Valsalva动作),以达到最佳用力排便状态。
-
采用德国西门子公司3.0 T超导型磁共振成像系统及8通道相控阵体部线圈。静态扫描快速自旋回波T2加权序列(重复时间5000 ms、回波时间86 ms、矩阵320×320、激励2次、层厚3 mm、间隔0.5 mm),并采集盆腔斜冠状面、斜矢状面和斜轴面图像。直肠内插入已注入超声耦合剂的胃管(用于标记肛管),并于阴道内注入约10 ml的超声耦合剂,然后行真实稳态进动快速成像序列多相位动态扫描,采集盆腔正中矢状面力排相(18个时相、共扫描25 s),最后取出标记胃管,插入自制球囊,囊内注入超声耦合剂(注入量以患者产生轻度便意为准,一般为80~100 ml),嘱患者尽力将球囊排出,进行正中矢状面力排相扫描(恢复时间最小、翻转角70°、视野33、矩阵矢状面256×224、冠状面256×256、激励2次、矢状面层厚4 mm、矢状面间隔0.5 mm、冠状面层厚6 mm、冠状面间隔2 mm、90个时相、扫描时间83 s)。
-
盆底动态MRI示肛直角为肛管长轴与直肠后壁的夹角,静息相时约为108°~127°,力排相时肛直角增大,提肛相时肛直角减小,角度变化为15°~20°。SPFS患者力排相时耻骨直肠肌痉挛性收缩,肛直角减小。利用动态MRI测量SPFS患者力排相(注入模拟粪便前、后)肛直角大小,可以反映耻骨直肠肌的放松程度。将耻尾线作为参照标志线[4],即从耻骨联合下缘延续到骶尾骨最后一节关节处。利用动态MRI测量SPFS患者力排相(注入模拟粪便前、后)各解剖标志线(包括膀胱颈、阴道后穹窿、肛门直肠结合部)至参考标志线纵垂线的距离,可以反映各器官的脱垂程度[5-10]。盆底器官脱垂分期为:轻度,即力排相盆底器官位于耻尾线下 < 3 cm;中度,即力排相盆底器官位于耻尾线下3~6 cm;重度,即力排相盆底器官位于耻尾线下 > 6 cm[11-13]。直肠前膨出分3度:轻度,即力排相直肠前壁向前呈囊袋状突出,其深度超过正常直肠前壁边界以远的垂直距离 < 2.0 cm;中度,即力排相直肠前壁向前呈囊袋状突出,其深度超过正常直肠前壁边界以远的垂直距离为2.0~4.0 cm;重度,即力排相直肠前壁向前呈囊袋状突出,其深度超过正常直肠前壁边界以远的垂直距离 > 4.0 cm[14]。会阴体下降诊断为力排相肛直肠结合部与耻尾线的垂直连线 > 5 cm。测量和诊断由低年资医师和有20年以上影像诊断经验的高年资医师分别进行,对于有分歧的诊断,互相商议达成一致。
-
采用SPSS 20.0软件进行数据的录入和分析。研究球囊注入前、后肛直角变化的二分类配对资料,比较采用McNemar检验,研究球囊注入前、后盆底器官脱垂的多分类等级配对资料比较采用配对秩和检验。P < 0.05表示差异有统计学意义。
-
利用直肠内模拟粪便注入后的动态MRI检查发现,53例SPFS患者均表现为耻骨直肠肌痉挛性反向收缩,其中24例[年龄27~78岁,平均年龄(55.2±12.4)岁]伴发多盆腔器官脱垂,包括11例直肠前膨出,3例膀胱脱垂、子宫颈或阴道穹窿脱垂、会阴体下降并直肠前膨出,2例膀胱脱垂、子宫颈或阴道穹窿脱垂并会阴体下降,2例膀胱脱垂,2例膀胱脱垂并直肠前膨出,1例膀胱脱垂、子宫颈或阴道穹窿脱垂并直肠前膨出,1例膀胱脱垂并子宫颈或阴道穹窿脱垂,1例直肠前膨出并会阴体下降,1例膀胱脱垂并会阴体下降;另外29例为单纯SPFS患者[年龄14~76岁,平均年龄(50.7±18.1)岁],未合并其他盆腔脏器脱垂。
利用盆底动态MRI技术观察比较SPFS患者直肠内模拟粪便注入前、后力排相的肛直角变化,结果见图 1。资料进行配对χ2检验,差异无统计学意义(χ2=0.603,P=0.219)(表 1)。相比直肠内模拟粪便注入后的盆底动态MRI,未注入的力排相分别有18.0%(9/50)膀胱脱垂、6.1%(3/49)子宫或阴道穹窿脱垂、32.7%(17/52)直肠前膨出及14.6%(7/48)会阴体下降诊断为阴性。利用盆底动态MRI技术观察比较直肠内模拟粪便注入前、后力排相的会阴体下降、膀胱脱垂、子宫颈或阴道穹窿脱垂、直肠前膨出程度,结果见图 2、图 3。资料进行定性资料配对秩和检验,差异均有统计学意义(Z=-2.646、-2.714、-2.449、-3.947,P=0.008、0.000、0.007、0.014)(表 2~表 5)。

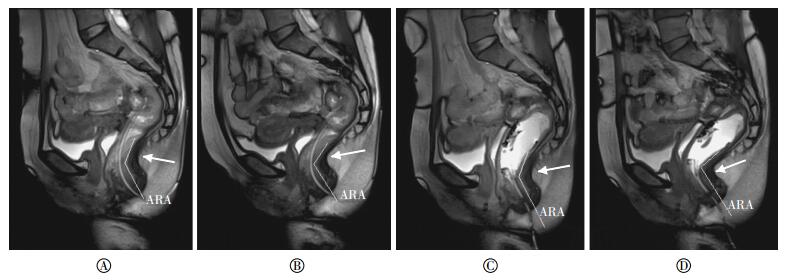
图 1 盆底痉挛患者真实稳态进动快速成像序列正中矢状位力排相图像 患者女性, 73岁, 排便困难40年, 需药物辅助排便。图中,A:未注入球囊前静息相,肛直角为130º(白色箭头所示)B:未注入球囊前力排相袁肛直角为120º(白色箭头所示); C:注入球囊后静息相, 肛直角为125º(白色箭头所示); D:注入球囊后力排相, 袁肛直角为107º(白色箭头所示);ARA; 肛直角。
Figure 1. Mid-sagittal true fast imaging with steady-state precession MRI of patient with spastic pelvic floor syndrome while straining
注入球囊前 注入球囊后 合计 X2值 P值 肛直角 肛直角 增大 减小或不变 肛直角增大 6 5 11 0.603 0.219 肛直角减小或不变 1 41 42 合计 7 46 53 表 1 注入球囊前,后肛直角变化(例)
Table 1. Anorectal angle before and after dynamic MRI with rectum injection

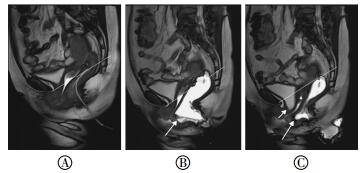
图 2 盆底痉挛合并多盆腔脏器脱垂患者真实稳态进动快速成像序列正中矢状位力排相图像患者女性,55岁,排便困难15个月,伴阴部神经痛。图中,A:未注入球囊前力排相,各个脏器均位于耻尾线以上;B:注入球囊后力排相,直肠前壁膨出(白色箭头所示),子宫颈及膀胱颈位于耻尾线上方;C:注入球囊后力排相,直肠内球囊排出后,子宫颈脱垂(白色箭头所示),膀胱颈脱垂(白色箭头所示)。
Figure 2. Mid-sagittal true fast imaging with steady-state precession MRI of patient with spastic pelvic floor syndrome associated with multiple pelvic compartment abnormalities while straining

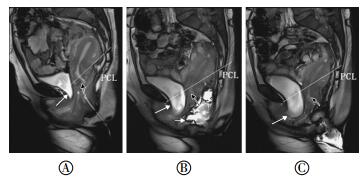
图 3 盆底痉挛合并多盆腔脏器脱垂患者真实稳态进动快速成像序列正中矢状位力排相图像患者女性,43岁,排便困难6个月,便后坠胀感。图中,A:未注入球囊前力排相,子宫颈轻度脱垂(黑色箭头所示),膀胱轻度脱垂(白色箭头所示);B:注入球囊后力排相,直肠前壁膨出(白色短箭头所示),子宫颈脱垂(黑色箭头所示),位于耻尾线下方约2.1 cm,膀胱颈脱垂(白色长箭头所示),位于耻尾线下方约3.1 cm;C:注入球囊后力排相,直肠内球囊排出后,子宫颈脱垂(黑色箭头所示),位于耻尾线下方约3.8 cm,膀胱颈脱垂(白色箭头所示),位于耻尾线下方约3.6 cm。
Figure 3. Mid-sagittal true fast imaging with steady-state precession MRI of patient with spastic pelvic floor syndrome associated with multiple pelvic compartment abnormalities while straining
注入后 未注入前 Z值 P值 阴性 轻度 中度 阴性 41 0 0 -2.714 0.007 轻度 9 1 0 中重度 0 2 0 表 2 注入球囊前、后膀胱脱垂情况及配对秩和检验(例)
Table 2. Wilcoxon rank-sum test for cystocele before and after dynamic MRI with rectum injection
注入后 未注入前 Z值 P值 阴性 轻度 中度 阴性 35 0 0 -3.947 0.000 轻度 13 0 0 中度 4 1 0 表 3 注入球囊前、后子宫或阴道穹窿脱垂情况及配对秩和检验(例)
Table 3. Wilcoxon rank-sum test for vaginal or cervical prolapse before and after dynamic MRI with rectum injection
注入后 未注入前 Z值 P值 阴性 轻度 中度 阴性 35 0 0 -3.947 0.000 轻度 13 0 0 中度 4 1 0 表 4 注入球囊前、后直肠前膨出程度及配对秩和检验(例)
Table 4. Wilcoxon rank-sum test for rectocele before and after dynamic MRI with rectum injection
注入后 未注入前 Z值 P值 阴性 阳性 阴性 46 0 -2.646 0.008 阳性 7 0 表 5 注入球囊前、后会阴体下降情况及配对秩和检验(例)
Table 5. Wilcoxon rank-sum test for descending perineum before and after dynamic MRI with rectum injection
-
SPFS又称不协调性排便[2],引起排便困难的主要原因为耻骨直肠肌或肛门内外括约肌反向收缩或不完全放松[15-19],病因尚不明确。SPFS真正的发病率难以评估,不同检查方法(肛门测压、球囊排出实验及盆底肌电图)的假阳性率和假阴性率均较高[20]。盆底肌电图结果在正常人与便秘患者中均可见[21],肛门测压法诊断的SPFS患者中约80%存在正常的放松功能[20]。盆底动态MRI技术能评价SPFS患者耻骨直肠肌或肛门内外括约肌形态学、功能性改变,及其合并的多盆腔脏器脱垂。SPFS患者耻骨直肠肌厚度明显较正常人厚,且患者力排时耻骨直肠肌异常收缩变粗,是SPFS的特异解剖及功能特征,也表明耻骨直肠肌肥厚或耻骨直肠肌异常收缩致肌肉肥厚与患者排便困难显著相关[22]。盆底动态MRI同时可观察患者动态排便过程,测量排便时间。文献研究显示,与正常对照组比较,约83%不协调性排便患者的力排时间延长,大于30 s[23]。
文献报道多盆腔器官联合病变的发生率约为95%[3],部分盆底功能紊乱患者局部盆腔器官修补后,约73.3%继发邻近器官的脱垂性病变[24]。本研究显示约45.3%(24/53)SPFS患者除耻骨直肠肌或肛门内外括约肌痉挛性病变外,还合并多盆腔器官脱垂。与盆底松弛患者相比,盆底痉挛患者较少并发多盆腔器官脱垂。Reiner等[25]研究发现,18例盆底痉挛患者中,约7%合并轻度膀胱脱垂,无患者合并子宫或阴道穹窿脱垂,33%合并轻度直肠脱垂,39%合并中度直肠脱垂,6%合并重度直肠脱垂,28%合并轻度直肠前膨出,6%合并中度直肠前膨出。本研究结果显示,53例盆底痉挛患者中,约34.0%(18/53)合并直肠前膨出,22.6%(12/53)合并膀胱脱垂,13.2%(7/53)合并子宫脱垂,13.2%(7/53)合并会阴体下降,考虑为长期用力排便导致的盆底肌肉、韧带及会阴体神经损伤,肛提肌(髂尾肌、耻尾肌)、韧带及提肌板松弛、薄弱。盆底受损可能是始发因素,盆底受损继发的多盆腔器官脱垂常相伴发生。临床治疗过程中,对于非单纯耻骨直肠肌痉挛的患者,应考虑多盆腔器官脱垂对于出口梗阻型便秘的影响。因此需要根据影像学检查获取全面准确的临床诊断,从而选择最佳治疗方法,避免二次修复术。
本研究中盆底动态MRI检查技术评价直肠内模拟粪便注入前、后肛直角的功能差异无统计学意义,提示未注入直肠内模拟粪便的动态MRI可诊断盆底痉挛。但对于多脏器脱垂的盆底痉挛患者,未注入直肠内模拟粪便的盆底动态MRI力排相常常发生漏诊。本研究显示分别有18.0%(9/50)膀胱脱垂、6.1%(3/49)子宫或阴道穹窿脱垂、32.7%(17/52)直肠前膨出及14.6%(7/48)会阴体下降诊断为阴性。且未注入直肠内模拟粪便的力排相对于盆腔脏器脱垂的分度小于注入直肠内模拟粪便的力排相。模拟烘便注入后,嘱患者用力将球囊排出,Valsalva动作程度加强,因此注入直肠内模拟粪便的力排相更接近患者日常生理排便过程中盆腔脏器的脱垂程度。未注入直肠内模拟粪便的动态MRI检查技术对于前、中、后多盆腔器官脱垂的影像诊断有一定的缺陷,存在假阴性。国内一些未注入直肠内模拟粪便的动态MRI检查对于SPFS患者的影像学诊断是不全面的,将对临床术前评估及术后效果评价造成一定的影响。
为了模拟正常排便过程,更准确地评价盆底功能性病变,大部分研究者建议直肠内注入造影剂模拟粪便。不同文献中对造影剂类型、剂量的选择多样,直肠内造影剂偏向于选择超声耦合剂,剂量约为120~150 ml[26-28]。其他研究者也建议使用混有小剂量钆螯合剂的土豆泥作为灌肠剂[29-31]。但要患者在仰卧位直接排出耦合剂在心理上仍较难接受,因此笔者进行了改进,自行设计高顺应性球囊,将球囊插入直肠后再将耦合剂注入球囊内模拟粪便,同样达到了造影目的。患者排出球囊在心理上较易接受,并且节省了检查后的整理时间。自行设计的高顺应球囊可以更好地反映盆底运动,并具有很好的稳定性及可重复性[4]。
本研究的局限性在于没有手术病理证实或金标准。多盆腔器官脱垂外科治疗为多科室联合性手术,临床途径确诊较难实现。其传统的检查方法为联合应用的排粪造影,可作为金标准,但因其风险较大,目前临床也很少应用。
通过观察直肠内模拟粪便注入后的动态MRI力排相,可以清晰显示盆底痉挛患者的耻骨直肠肌、肛管内外括约肌和肛提肌各部的协调运动功能,并可对伴发的膀胱脱垂、子宫颈或阴道脱垂、会阴体下降及直肠前膨出等多盆腔器官脱垂进行标准化分度,为术前正确诊断盆腔痉挛患者合并的多部位缺陷及术后正确评价治疗效果提供了客观依据。
直肠内注入模拟粪便的动态MRI对女性盆底痉挛综合征的诊断价值
Value of dynamic MRI with rectum injection in the diagnosis of female spastic pelvic floor syndrome
-
摘要:
目的 利用动态MRI研究直肠内模拟粪便注入前、后女性盆底痉挛综合征(SPFS)患者的肛直肠形态、功能性病变, 并对多盆腔器官脱垂进行评价, 明确注入球囊后的动态MRI在SPFS患者中的诊断优势。 方法 对53例临床诊断为SPFS的女性患者行动态MRI检查, 使用自行设计高顺应性球囊模拟大便, 测量患者直肠内球囊注入前、后力排相盆底的相关数据。 结果 盆底动态MRI结果显示, 53例女性SPFS患者中, 伴发多盆腔器官脱垂者24例。直肠内造影剂注入前、后力排相的肛直角变化, 差异无统计学意义(χ2=0.603, P > 0.05);相比直肠内模拟粪便注入后的盆底动态MRI, 未注入的力排相分别有18.0%(9/50)膀胱脱垂、6.1%(3/49)子宫或阴道穹窿脱垂、32.7%(17/52)直肠前膨出及14.6%(7/48)会阴体下降诊断为阴性。直肠内模拟粪便注入前、后力排相观察多盆腔器官脱垂变化, 差异均有明显统计学意义。 结论 直肠内注入模拟粪便的盆底动态MRI为女性SPFS患者提供了更全面的诊断, 为术前正确诊断盆腔多部位缺陷及术后正确评价治疗效果提供了客观依据。 Abstract:Objective Dynamic MRI with rectum injectionis employed to assess female spastic pelvic floor syndrome of anorectal morphology and function in relation to various pelvic compartment abnormalitiesin female outlet obstruction constipation. Methods Dynamic MRI was performed in 53 female patients(14-78 years of age, with a mean age of 52.7±15.8 years)with clinical diagnosis of spastic pelvic floor syndrome.The homemade highly conformable sacculus was inserted into the rectum to simulate stool. The relevant measurements were then obtained during straining before and after rectum injection. Results Among the 53 female patients with spastic pelvic floor syndrome, 24 patients(45.3%) have multifocal disorders involving more than one compartment.The difference in the anorectal angles before and after rectum injection was not significant(χ2=0.603, P > 0.05). Differences in the cystocele, vaginal or cervical prolapse, rectocele, and descending perineum before and after rectum injection were significant. Conclusion Using dynamic MRI with rectum injection allows for the accurate evaluation of the anorectal morphology and function related to various pelvic compartment abnormalitiesin female spastic pelvic floor syndrome; thus, this method is proved valuable in the diagnosis and treatment of female spastic pelvic floor syndrome. -
Key words:
- Pelvic floor /
- Magnetic resonance imaging /
- Spastic pelvic floor syndrome
-
图 1 盆底痉挛患者真实稳态进动快速成像序列正中矢状位力排相图像 患者女性, 73岁, 排便困难40年, 需药物辅助排便。图中,A:未注入球囊前静息相,肛直角为130º(白色箭头所示)B:未注入球囊前力排相袁肛直角为120º(白色箭头所示); C:注入球囊后静息相, 肛直角为125º(白色箭头所示); D:注入球囊后力排相, 袁肛直角为107º(白色箭头所示);ARA; 肛直角。
Figure 1. Mid-sagittal true fast imaging with steady-state precession MRI of patient with spastic pelvic floor syndrome while straining
图 2 盆底痉挛合并多盆腔脏器脱垂患者真实稳态进动快速成像序列正中矢状位力排相图像患者女性,55岁,排便困难15个月,伴阴部神经痛。图中,A:未注入球囊前力排相,各个脏器均位于耻尾线以上;B:注入球囊后力排相,直肠前壁膨出(白色箭头所示),子宫颈及膀胱颈位于耻尾线上方;C:注入球囊后力排相,直肠内球囊排出后,子宫颈脱垂(白色箭头所示),膀胱颈脱垂(白色箭头所示)。
Figure 2. Mid-sagittal true fast imaging with steady-state precession MRI of patient with spastic pelvic floor syndrome associated with multiple pelvic compartment abnormalities while straining
图 3 盆底痉挛合并多盆腔脏器脱垂患者真实稳态进动快速成像序列正中矢状位力排相图像患者女性,43岁,排便困难6个月,便后坠胀感。图中,A:未注入球囊前力排相,子宫颈轻度脱垂(黑色箭头所示),膀胱轻度脱垂(白色箭头所示);B:注入球囊后力排相,直肠前壁膨出(白色短箭头所示),子宫颈脱垂(黑色箭头所示),位于耻尾线下方约2.1 cm,膀胱颈脱垂(白色长箭头所示),位于耻尾线下方约3.1 cm;C:注入球囊后力排相,直肠内球囊排出后,子宫颈脱垂(黑色箭头所示),位于耻尾线下方约3.8 cm,膀胱颈脱垂(白色箭头所示),位于耻尾线下方约3.6 cm。
Figure 3. Mid-sagittal true fast imaging with steady-state precession MRI of patient with spastic pelvic floor syndrome associated with multiple pelvic compartment abnormalities while straining
表 1 注入球囊前,后肛直角变化(例)
Table 1. Anorectal angle before and after dynamic MRI with rectum injection
注入球囊前 注入球囊后 合计 X2值 P值 肛直角 肛直角 增大 减小或不变 肛直角增大 6 5 11 0.603 0.219 肛直角减小或不变 1 41 42 合计 7 46 53  下载: 导出CSV
下载: 导出CSV
表 2 注入球囊前、后膀胱脱垂情况及配对秩和检验(例)
Table 2. Wilcoxon rank-sum test for cystocele before and after dynamic MRI with rectum injection
注入后 未注入前 Z值 P值 阴性 轻度 中度 阴性 41 0 0 -2.714 0.007 轻度 9 1 0 中重度 0 2 0
下载: 导出CSV
表 3 注入球囊前、后子宫或阴道穹窿脱垂情况及配对秩和检验(例)
Table 3. Wilcoxon rank-sum test for vaginal or cervical prolapse before and after dynamic MRI with rectum injection
注入后 未注入前 Z值 P值 阴性 轻度 中度 阴性 35 0 0 -3.947 0.000 轻度 13 0 0 中度 4 1 0
下载: 导出CSV
表 4 注入球囊前、后直肠前膨出程度及配对秩和检验(例)
Table 4. Wilcoxon rank-sum test for rectocele before and after dynamic MRI with rectum injection
注入后 未注入前 Z值 P值 阴性 轻度 中度 阴性 35 0 0 -3.947 0.000 轻度 13 0 0 中度 4 1 0
下载: 导出CSV
表 5 注入球囊前、后会阴体下降情况及配对秩和检验(例)
Table 5. Wilcoxon rank-sum test for descending perineum before and after dynamic MRI with rectum injection
注入后 未注入前 Z值 P值 阴性 阳性 阴性 46 0 -2.646 0.008 阳性 7 0
下载: 导出CSV
-
[1] Times ML, Reickert CA.Functional anorectal disorders[J].Clin Colon Rectal Surg, 2005, 18(2):109-115. doi: 10.1055/s-2005-870892 [2] Drossman DA.The functional gastrointestinal disorders and the Rome Ⅲ process[J].Gastroenterology, 2006, 130(5):1377-1390.DOI:10.1053/j.gastro.2006.03.008. [3] Maglinte DD, Kelvin FM, Fitzgerald K, et al.Association of compartment defects in pelvic floor dysfunction[J].AJR Am J Roentgenol, 1999, 172(2):439-444.DOI:10.2214/ajr.172.2.9930799. [4] Yang A, Mostwin JL, Rosenshein NB, et al.Pelvic floor descent in women:dynamic evaluation with fast MR imaging and cinematic display[J].Radiology, 1991, 179(1):25-33.DOI:10.1148/radiology.179.1.2006286. [5] 彭朋, 蒋涛, 杨新庆, 等.盆底动态MRI对盆底功能异常的诊断价值[J].临床放射学杂志, 2009, 28(5):711-715.
Peng P, Jiang T, Yang XQ, et al.The diagnostic value of dynamic MRI in pelvic floor disfunction[J].J Clin Radiol, 2009, 28(5):711-715.[6] Goh V, Halligan S, Kaplan G, et al.Dynamic MR imaging of the pelvic floor in asymptomatic subjects[J].AJR Am J Roentgenol, 2000, 174(3):661-666.DOI:10.2214/ajr.174.3.1740661. [7] Fielding JR.Practical MR imaging of female pelvic floor weakness[J].Radiographics, 2002, 22(2):295-304.DOI:http://dx.doi.org/10.1148/radiographics.22.2.g02mr25295. [8] Boyadzhyan L, Raman SS, Raz S.Role of static and dynamic MR imaging in surgical pelvic floor dysfunction[J].Radiographics, 2008, 28(4):949-967.DOI:10.1148/rg.284075139. [9] Colaiacomo MC, Masselli G, Polettini E, et al.Dynamic MR imaging of the pelvic floor: a pictorial review[J/OL].Radiographics, 2009, 29(3): e35[2016-01-29].http://pubs.rsna.org/doi/pdf/10.1148/rg.e35.DOI: 10.1148/rg.e35. [10] 王毅, 龚水根, 张伟国.盆底MRI研究的现状[J].中华放射学杂志, 2003, 37(11):1049-1051.DOI:10.3760/j.issn:1005-1201.2003.11.018.
Wang Y, Gong SG, Zhang WG.The current research of pelvic MRI[J].Chin J Radiol, 2003, 37(11):1049-1051. doi: 10.3760/j.issn:1005-1201.2003.11.018.WangY,[11] Reiner CS, Weishaupt D.Dynamic pelvic floor imaging:MRI techniques and imaging parameters[J].Abdom Imaging, 2013, 38(5):903-911.DOI:10.1007/s00261-012-9857-7. [12] Maron DJ, Wexner SD.Disorders of the anorectum and pelvic floor[J].Gastroenterol Clin North Am, 2013, 42(4):XⅢ-XIV.DOI:10.1016/j.gtc.2013.10.001. [13] Faucheron JL, Barot S, Collomb D, et al.Dynamic cystocolpoproc-tography is superior to functional pelvic MRI in the diagnosis of posterior pelvic floor disorders:results of a prospective study[J].Colorectal Dis, 2014, 16(7):O240-O247.DOI:10.1111/codi.12586. [14] Kuijpers HC, Bleijenberg G.The spastic pelvic floor syndrome.A cause of constipation[J].Dis Colon Rectum, 1985, 28(9):669-672. doi: 10.1007/BF02553449 [15] Preston DM, Lennard-Jones JE.Anismus in chronic constipation[J].Dig Dis Sci, 1985, 30(5):413-418. doi: 10.1007/BF01318172 [16] Karasick S, Karasick D, Karasick SR.Functional disorders of the anus and rectum:findings on defecography[J].AJR Am J Roentgenol, 1993, 160(4):777-782.DOI:10.2214/ajr.160.4.8456664. [17] 郭亮亮, 郭东强.直肠黏膜脱垂患者排粪造影的X线表现分级研究[J].国际放射医学核医学杂志, 2014, 38(6):381-383.DOI:10.3760/cma.j.issn.1673-4114.2014.06.008.
LL, Guo DQ.Defecography in patients with prolapse of rectal mucosa lesions:degrees of imaging findings[J].Int J Radiat Med Nucl Med, 2014, 38(6):381-383. doi: 10.3760/cma.j.issn.1673-4114.2014.06.008.[18] Whitehead WE, Wald A, Diamant NE, et al.Functional disorders of the anus and rectum[J].Gut, 1999, 45(Suppl 2):SⅡ55-Ⅱ59.DOI:10.1136/gut.45.2008.ii55. [19] García del Salto L, de Miguel Criado J, Aguilera del Hoyo LF, et al.MR imaging-based assessment of the female pelvic floor[J].Radiographics, 2014, 34(5):1417-1439.DOI:10.1148/rg.345140137. [20] Jorge JM, Wexner SD, Ger GC, et al.Cinedefecography and electromyography in the diagnosis of nonrelaxing puborectalis syndrome[J].Dis Colon Rectum, 1993, 36(7):668-676. doi: 10.1007/BF02238594 [21] Jones PN, Lubowski DZ, Swash M, et al.Is paradoxical contraction of puborectalis muscle of functional importance?[J].Dis Colon Rectum, 1987, 30(9):667-670. doi: 10.1007/BF02561685 [22] 黄继兰, 蒋涛, 李敏.盆底动态磁共振成像诊断不协调性排便[J].中国医学影像技术, 2014, 30(4):556-559.
Huang JL, Jiang T, Li M.Pelvic dynamic MRI in diagnosis of dyssynergic defecation[J].Chin J Med Imaging Technol, 2014, 30(4):556-559.[23] Bolog N, Weishaupt D.Dynamic MR imaging of outlet obstruction[J].Rom J Gastroenterol, 2005, 14(3):293-302. [24] Siegmann KC, Reisenauer C, Speck S, et al.Dynamic magnetic resonance imaging for assessment of minimally invasive pelvic floor reconstruction with polypropylene implant[J].Eur J Radiol, 2011, 80(2):182-187. [25] Reiner CS, Tutuian R, Solopova AE, et al.MR defecography in patients with dyssynergic defecation:spectrum of imaging findings and diagnostic value[J].Br J Radiol, 2011, 84(998):136-144.DOI:10.1259/bjr/28989463. [26] Lienemann A, Anthuber C, Baron A, et al.Dynamic MR colpocys-torectography assessing pelvic-floor descent[J].Eur Radiol, 1997, 7(8):1309-1317.DOI:10.1007/s003300050294. [27] Fletcher JG, Busse RF, Riederer SJ, et al.Magnetic resonance imaging of anatomic and dynamic defects of the pelvic floor in defecatory disorders[J].Am J Gastroenterol, 2003, 98(2):399-411.DOI:10.1111/j.1572-0241.2003.07235.x. [28] Bertschinger KM, Hetzer FH, Roos JE, et al.Dynamic MR imaging of the pelvic floor performed with patient sitting in an open-magnet unit versus with patient supine in a closed-magnet unit[J].Radiology, 2002, 223(2):501-508.DOI:http://dx.doi.org/10.1148/radiol.2232010665. [29] Dvorkin LS, Hetzer F, Scott SM, et al.Open-magnet MR defaecography compared with evacuation proctography in the diagnosis and management of patients with rectal intussusception[J].Colorectal Dis, 2004, 6(1):45-53. doi: 10.1111/j.1463-1318.2004.00577.x [30] Roos JE, Weishaupt D, Wildermuth S, et al.Experience of 4 years with open MR defecography:pictorial review of anorectal anatomy and disease[J].Radiographics, 2002, 22(4):817-832.DOI:10.1148/radiographics.22.4.g02jl02817. [31] Lamb GM, De Jode MG, Gould SW, et al.Upright dynamic MR defaecating proctography in an open configuration MR system[J].Br J Radiol, 2000, 73(866):152-155.DOI:10.1259/bjr.73.866.10884727. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 3172
- HTML全文浏览量: 1709
- PDF下载量: 3