


-
核医学检查是目前临床最常用的诊断肺栓塞的无创检查手段之一。传统的肺通气/灌注(ventilation-perfusion,V/Q)平面显像对肺栓塞的检出率为50%~80%[1],且“不能确定”的结果较常见[2]。尤其是在部分患者因呼吸困难、通气功能差或通气检查所需时间太长等原因而无法配合完成通气显像时,或在通气显像质量不能满足诊断需求等情况时,其对肺栓塞的检出率明显下降。为了提高肺栓塞的检出率,肺灌注断层显像与低剂量平扫CT相结合(以下简称肺Q SPECT/CT)成了一种新的探索方式。本研究试图通过对69例临床可疑肺栓塞患者的肺V/Q平面显像与肺Q SPECT/CT结果进行比较,对肺Q SPECT/CT是否能提高肺栓塞的检出率做出判定。
-
收集2013年11月至2014年8月前来山西医科大学第一医院就诊的69例临床疑诊肺栓塞患者的完整病例资料,其中,男性33例、女性36例,年龄16~82岁,平均(59.6±14.2)岁。所有患者均无明显诱因出现胸痛、气紧、晕厥等临床症状,D-二聚体检查阳性和(或)临床WELLS评分 > 2,且同时行肺V/Q平面显像和肺Q SPECT/CT显像。所有患者均于显像前签署了知情同意书。
本研究纳入合并其他心肺疾患的病例,如肺炎、肺实变、肺不张、胸腔积液、慢性阻塞性肺疾病(chronic obstructive pulmonary disease,COPD)、大动脉炎等。疑诊患者中5例合并COPD,3例肺炎,1例肺实变,3例胸腔积液,2例大动脉炎,1例卵巢过度刺激综合征,1例动脉导管未闭。
临床对肺栓塞的诊断主要通过对临床症状、体征、D-二聚体等生化检查和双下肢彩超、心脏彩超、CT肺动脉造影及肺V/Q平面显像等影像学检查结果以及最后的随访进行综合判断后得出。
-
所有疑似肺栓塞患者均同时行肺V/Q平面显像和肺Q SPECT/CT。
SPECT/CT采用SIEMENS Symbia T16双探头+16排CT,配低能高分辨率准直器。通气设备用内蒙古英华融泰高科技发展有限公司生产的一次性使用肺通气导入器——99Tcm-DTPA气溶胶通气装置。
-
嘱患者吸氧,氧气流量为2~4 L/min,吸入时间为5~10 min。之后将1.11×106 GBq 99Tcm-DTPA(北京原子高科股份有限公司)注入雾化器,再注入5 ml空气,经雾化吸入装置雾化后,嘱患者尽可能吸入,之后间断用个人剂量检测仪在患者背部及前胸部(即肺体表投影范围内)探测,当探测剂量达到30 μSv/h时,可行肺通气显像。嘱患者仰卧于检查床上,双臂抱头,使探头尽量贴近胸部,取前、后、右前斜、右后斜、左前斜、左后斜、左侧、右侧位8个体位进行肺通气平面显像。采集时需将双肺同时包括在探头视野内,选用低能高分辨率准直器,采集矩阵512×512,每个体位采集计数为1×105。
肺通气平面显像完成后,即刻行肺灌注平面显像。
-
患者仰卧于检查床上,双臂抱头,使探头尽量贴近胸部。经双下肢足背静脉注射99Tcm标记的大颗粒聚合人血清白蛋白(2.96~3.70)×105 GBq,完成下肢静脉显像后,取前、后、右前斜、右后斜、左前斜、左后斜、左侧、右侧位8个体位进行肺灌注平面显像。采集时需将双肺同时包括在探头视野内,选用低能高分辨率准直器,采集矩阵512×512,每个体位采集计数为1×105。
-
肺灌注平面显像完成后行SPECT/CT,患者体位同肺灌注平面显像。探头旋转360°,每6°采集一帧,每帧采集5 s,共采集60帧,采集矩阵128×128。采集过程中嘱患者平稳呼吸,以减少呼吸运动对肺显像的干扰。断层采集之后同一床位进行低剂量CT扫描,以30 mm/s床速进行。
原始图像经处理后得到肺V/Q平面显像图像和肺横断位、冠状位、矢状位肺Q SPECT/CT断层融合图像。
-
由2~3位富有经验的高年资医师来阅片。肺V/Q平面显像扫描阅片时,记录所有肺灌注及通气显像时出现缺损的面积及肺段,如果灌注图像出现一个或者多个灌注缺损,相应部位通气图像正常,则“不匹配”;肺V/Q平面显像参照肺栓塞诊断前瞻性调查诊断(PIOPED)标准判定患者患肺栓塞的可能性,最后将正常及低度可能判定为阴性,中度及高度可能判定为阳性[3]。肺Q SPECT/CT扫描阅片时,记录肺Q SPECT/CT时出现缺损的面积及肺段,用CT排除由于炎症、胸腔积液等引起的缺损。肺Q SPECT/CT参照重新修订的肺栓塞诊断前瞻性调查(PIOPED II)诊断标准[3]判定患者患肺栓塞的可能性,最后同肺V/Q平面显像一致,将正常及低度可能判定为阴性,中度及高度可能判定为阳性。肺V/Q平面显像先独立阅片,确定一个诊断结果;再将肺Q SPECT/CT独立阅片,得出一个新的结果。
-
数据资料经录入、一致性检验和逻辑纠错后,应用SPSS 17.0软件进行统计学分析。做肺V/Q平面显像和肺Q SPECT/CT两种检查方法与最终临床确诊结果的Kappa一致度分析(K值评价)。以临床最终诊断为依据,采用配对χ2检验对两种方法的检出率进行比较。P < 0.05表示差异有统计学意义。
-
69例患者中,有43例被诊断为肺栓塞,占62.32%(43/69);26例排除肺栓塞。两种方法对肺栓塞诊断的阳性数、阴性数见表 1。
显像方法 临床最终确诊结果 总计 阳性 阴性 肺V/Q平面显像 阳性 34 5 39 阴性 9 21 30 总计 43 26 69 肺Q SPECT/CT 阳性 40 9 49 阴性 3 17 20 总计 43 26 69 注:表中,肺V/Q平面显像:肺通气/灌注平面显像;肺Q SPECT/CT:肺灌注SPECT/CT。 表 1 两种显像方法与临床最终确诊结果(例)
Table 1. Two imaging methods and the final clinical diagnosis results
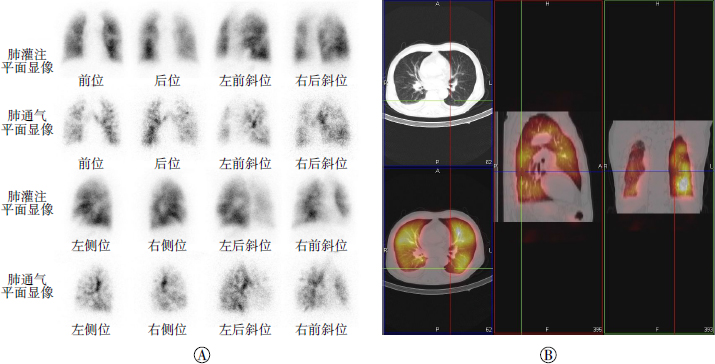
其中两种方法共同得出假阴性数3例;肺V/Q平面显像得出假阴性而肺Q SPECT/CT得出真阳性6例(图 1)。

图 1 肺栓塞患者肺通气/灌注平面显像、肺灌注SPECT/CT显像图
Figure 1. Pictures of pulmonary ventilation-perfusion planar imaging, pulmonary perfusion SPECT combining with low-dose CT of pulmonary embolism patients
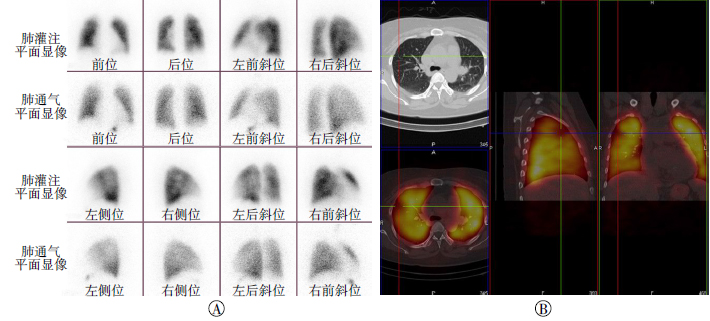
肺Q SPECT/CT对肺栓塞诊断的灵敏度(93.02%)、准确率(82.61%)、阴性预测值(85.00%)及与临床最终确诊结果的Kappa值(0.612)均较肺V/Q平面显像(79.07%、79.71%、70.00%、0.581)高。肺Q SPECT/CT对伴有COPD的肺栓塞患者的诊断特异度(65.38%)较传统的肺V/Q平面显像(80.77%)低(图 2)。

图 2 慢性阻塞性肺疾病患者肺通气/灌注平面显像和肺灌注SPECT/CT图
Figure 2. Pictures of pulmonary ventilation-perfusion planar imaging and pulmonary perfusion SPECT combining with low-dose CT of chronic obstructive pulmonary disease patients
排除COPD病例后,肺Q SPECT/CT对肺栓塞诊断的特异度(80.95%)较肺V/Q平面显像(76.19%)高。
两种方法在包含COPD病例及排除COPD的影响后,各自详细的诊断效能结果见表 2和表 3。两种显像方法对肺栓塞患者的诊断结果见表 4。
显像方法 灵敏度 特异度 准确率 阳性预测值 阴性预测值 肺V/Q平面显像 79.07 80.77 79.71 87.18 70.00 肺Q SPECT/CT 93.02 65.38 82.61 81.63 85.00 注:表中,COPD:慢性阻塞性肺疾病;肺V/Q平面显像:肺通气/灌注平面显像;肺Q SPECT/CT:肺灌注SPECT/CT。 表 2 肺栓塞患者合并COPD时两种不同显像方法的诊断效能指标(%)
Table 2. Diagnostic performance of the two different imaging methods in pulmonary embolism patients with chronic obstructive pulmonary disease(%)
显像方法 灵敏度 特异度 准确率 阳性预测值 阴性预测值 肺V/Q平面显像 79.07 76.19 78.12 87.18 64.00 肺Q SPECT/CT 93.02 80.95 89.06 90.91 85.00 注:表中,COPD:慢性阻塞性肺疾病;肺V/Q平面显像:肺通气/灌注平面显像;肺Q SPECT/CT:肺灌注SPECT/CT。 表 3 肺栓塞患者排除了合并COPD后两种不同显像方法的诊断效能(%)
Table 3. Diagnostic performance of the two different imaging methods in pulmonary embolism patients without chronic obstructive pulmonary disease(%)
肺V/Q平面显像 肺Q SPECT/CT 总计 阳性 阴性 阳性 39 0 39 阴性 10 20 30 总计 49 20 69 注:表中,肺V/Q平面显像:肺通气/灌注平面显像;肺Q SPECT/CT:肺灌注SPECT/CT。 表 4 两种不同显像方法对肺栓塞患者的诊断结果(例)
Table 4. Pulmonary embolism patients diagnostic results by two different imaging methods
两种方法检出肺栓塞的一致性为85.00%(34/40),用配对χ2检验对两种方法的检出率进行对比发现,二者对肺栓塞的检出率差异有统计学意义(χ2=8.10,P < 0.005)。
-
传统的肺V/Q平面显像具有诊断辐射剂量低、无创、对小血管敏感、可同时显示下肢深静脉是否通畅等优势,自开创以来,已经使用了40多年。但是,肺V/Q平面显像观察的是组织的重叠影像,检测的分辨率低,定位准确性差,不确定诊断率高[4]。
肺灌注显像是利用99Tcm标记的大颗粒聚合人血清白蛋白静脉注入后一过性地嵌顿在肺毛细血管内,放射性分布与血流灌注成正比这一原理检测栓塞肺段。若栓子是位于肺的主干及大的分支的附壁血栓,且并未影响99Tcm标记的大颗粒聚合人血清白蛋白的通过,那么在肺灌注显像上就表现为阴性。本研究中两种方法共同得出的3例假阴性患者就是因为上述原因所致。
肺灌注平面显像具有的优势肺Q SPECT均有。已经证实,与肺灌注平面显像相比,肺Q SPECT提高了肺栓塞的检出率[1]。这是因为肺Q SPECT显像可以避免由于结构重叠造成的周围射线散射对深部病灶和小病灶的掩盖,从而更好地显示亚肺段病变而提高灵敏度。本研究的肺V/Q平面显像中,6例假阴性患者均是由于病灶范围较小被掩盖所致。
肺通气显像能够检测气道是否通畅,可对双肺的通气功能进行评估。它可以对肺炎、肺不张等影响血流灌注的非特异性疾病做出鉴别,提高肺灌注诊断的特异性。与肺灌注平面显像相同,肺通气平面显像同样具有分辨率低、定位准确率差的缺点。同时,肺通气显像需要专门的通气装置,该通气装置价格相对昂贵,且吸入99Tcm-DTPA耗时长,通气功能严重受损或病重的患者很难配合完成,或图像质量很难达到诊断要求。因此,肺Q SPECT/CT成了一种新的探索方式。
肺Q SPECT/CT中,用平扫CT代替了肺通气显像和(或)胸片。肺Q SPECT是一种功能性成像,它观察的是生理性的结果——灌注缺损。任何影响肺血流的因素,如肿瘤压迫、肺动脉炎症、血管痉挛、COPD、充血性心力衰竭等,均可造成肺动脉灌注减低,在肺灌注图上表现为灌注稀疏或缺损,从而出现假阳性[5]。CT平扫通过增加对潜在肺栓塞患者心影、大血管、肺纹理、肺实质及胸腔积液等的变化情况的可视性[6],很好地弥补了上述问题。而且,平扫CT与肺通气显像一样,能提高肺灌注显像诊断肺栓塞的特异度。同时,CT平扫填补了阅片时对胸片的需求。
本研究发现,肺Q SPECT/CT对肺栓塞诊断的灵敏度、准确率、阴性预测值及与临床最终确诊结果的Kappa值均较肺V/Q平面显像高,与孟庆乐等[7]得到的结果稍有不同,这可能与研究的人群以及最终的临床算法有关。但得出的最终结果是相同的。
本研究结果得出肺Q SPECT/CT对肺栓塞的检出率较肺V/Q平面显像高,但是,肺Q SPECT/CT对肺栓塞诊断的特异度(65.38%)较肺V/Q平面显像(80.77%)低,主要是因为疑诊患者中有5例伴有COPD。肺通气显像对COPD、哮喘等气道疾病更灵敏。在COPD早期,CT或胸片显示完全正常。对于这部分患者,只行肺Q SPECT/CT,而未行肺通气显像,可能会出现假阳性,导致其特异度降低。如果将这6例COPD患者排除,则肺Q SPECT/CT对肺栓塞诊断的特异度上升至80.95%,而肺V/Q平面显像的特异度则降至76.19%。也就是说,在不伴有COPD的患者中,肺Q SPECT/CT对肺栓塞诊断的特异度较肺V/Q平面显像高。
肺Q SPECT/CT采集时间大约为20 min,其中CT扫描只需要不到1 min,且其操作方便,在不改变患者体位的情况下,一次扫描即可同时获得肺Q SPECT图像、CT图像及二者的融合图像,避免了肺通气显像的麻烦,而且平扫CT图像较胸片更清晰。而肺V/Q平面显像采集大约需要45 min,患者很可能会因呼吸困难、胸部不适等不能配合做完检查。
另外,肺通气显像患者接受的辐射剂量大约为0.777 mSv[8],平扫CT辐射剂量小,用平扫CT取代肺通气显像,辐射剂量仅增加了1~2 mSv[8],不需要对比剂,且能够避免通气显像剂对患者口腔、鼻腔、胃及检查空间的污染,减低患者、亲属及医护人员所受的辐射。肺Q SPECT/CT可对肾功能不良以及对碘对比剂过敏的可疑肺栓塞患者提供一个相对安全的诊断模式[9]。
综上所述,肺Q SPECT/CT明显提高了不伴有COPD的患者肺栓塞的诊断价值,用肺Q SPECT/CT取代肺V/Q平面显像值得商榷。
肺通气/灌注平面显像与肺灌注SPECT/CT对肺栓塞诊断价值的对比性研究
Comparative study of pulmonary ventilation/perfusion planar imaging and pulmonary perfusion SPECT combined with low-dose CT in the diagnosis of pulmonary embolism
-
摘要:
目的 探讨传统的肺通气/灌注(V/Q)平面显像、肺灌注断层显像与低剂量平扫CT相结合(肺Q SPECT/CT)对肺栓塞的诊断价值。 方法 收集69例临床可疑肺栓塞患者,在对其行肺V/Q平面显像的同时,进行了肺Q SPECT/CT显像。以临床最终确诊结果为金标准,对两种方法的诊断结果进行对比分析。 结果 69例临床可疑肺栓塞患者,最终确诊43例,排除26例。肺Q SPECT/CT对肺栓塞诊断的灵敏度、准确率、阴性预测值及与临床最终确诊结果的Kappa值均较肺V/Q平面显像高;肺Q SPECT/CT对合并有慢性阻塞性肺疾病(COPD)的病例诊断的特异度较肺V/Q平面显像低。排除COPD病例的影响后,肺Q SPECT/CT的特异度明显提高,且高于肺V/Q平面显像的特异度。两种方法检出肺栓塞的一致性为85%(34/40),且两种方法检出率之间的差异有统计学意义(χ2=8.10,P < 0.05)。 结论 肺Q SPECT/CT明显提高了对不伴有COPD的肺栓塞患者的诊断价值,用肺Q SPECT/CT取代肺V/Q平面显像值得商榷。 Abstract:Objective To study the value of traditional pulmonary ventilation-perfusion(V/Q)planar imaging and pulmonary perfusion SPECT combining with low-dose CT(Q SPECT/CT) in the diagnosis of pulmonary embolism. Methods Sixty nine patients with suspected pulmonary embolism were collected. Pulmonary V/Q planar imaging was performed in all the patients, meanwhile, pulmonary Q SPECT/CT was taken. Taking the final clinical diagnosis results as the gold standards and then compared and analyzed the diagnosis results of the two methods. Results Among the 69 suspected pulmonary embolism patients, 43 cases were confirmed, 26 excluded. The sensitivity, accuracy, negative predictive value and the Kappa value of the final clinical diagnosis result of pulmonary Q SPECT/CT in the diagnosis of pulmonary embolism were all higher than those of V/Q planar imaging. While, the diagnostic specificity in those patients with chronic obstructive pulmonary disease(COPD) operated by pulmonary Q SPECT/CT was lower than that of V/Q planar imaging. After adjusting the impact of COPD patients, the specificity of pulmonary Q SPECT/CT improved obviously, and was higher than that of V/Q planar imaging. The consistency of pulmonary embolism detection rate by the two methods was 85%(34/40)and the difference of the detection rate between the two methods was significant(χ2=8.10, P < 0.05). Conclusion Pulmonary Q SPECT/CT obviously improved the diagnostic value of pulmonary embolism without COPD, so it should be deliberated whether it takes the place of the V/Q planar imaging. -
Key words:
- Pulmonary embolism /
- Pulmonary disease /
- chronic obstructive /
- Radionulide imaging /
- Tomography /
- emission-computed /
- single-photon /
- Tomography /
- X-ray computed
-
图 1 肺栓塞患者肺通气/灌注平面显像、肺灌注SPECT/CT显像图
Figure 1. Pictures of pulmonary ventilation-perfusion planar imaging, pulmonary perfusion SPECT combining with low-dose CT of pulmonary embolism patients
图 2 慢性阻塞性肺疾病患者肺通气/灌注平面显像和肺灌注SPECT/CT图
Figure 2. Pictures of pulmonary ventilation-perfusion planar imaging and pulmonary perfusion SPECT combining with low-dose CT of chronic obstructive pulmonary disease patients
表 1 两种显像方法与临床最终确诊结果(例)
Table 1. Two imaging methods and the final clinical diagnosis results
显像方法 临床最终确诊结果 总计 阳性 阴性 肺V/Q平面显像 阳性 34 5 39 阴性 9 21 30 总计 43 26 69 肺Q SPECT/CT 阳性 40 9 49 阴性 3 17 20 总计 43 26 69 注:表中,肺V/Q平面显像:肺通气/灌注平面显像;肺Q SPECT/CT:肺灌注SPECT/CT。  下载: 导出CSV
下载: 导出CSV
表 2 肺栓塞患者合并COPD时两种不同显像方法的诊断效能指标(%)
Table 2. Diagnostic performance of the two different imaging methods in pulmonary embolism patients with chronic obstructive pulmonary disease(%)
显像方法 灵敏度 特异度 准确率 阳性预测值 阴性预测值 肺V/Q平面显像 79.07 80.77 79.71 87.18 70.00 肺Q SPECT/CT 93.02 65.38 82.61 81.63 85.00 注:表中,COPD:慢性阻塞性肺疾病;肺V/Q平面显像:肺通气/灌注平面显像;肺Q SPECT/CT:肺灌注SPECT/CT。
下载: 导出CSV
表 3 肺栓塞患者排除了合并COPD后两种不同显像方法的诊断效能(%)
Table 3. Diagnostic performance of the two different imaging methods in pulmonary embolism patients without chronic obstructive pulmonary disease(%)
显像方法 灵敏度 特异度 准确率 阳性预测值 阴性预测值 肺V/Q平面显像 79.07 76.19 78.12 87.18 64.00 肺Q SPECT/CT 93.02 80.95 89.06 90.91 85.00 注:表中,COPD:慢性阻塞性肺疾病;肺V/Q平面显像:肺通气/灌注平面显像;肺Q SPECT/CT:肺灌注SPECT/CT。
下载: 导出CSV
表 4 两种不同显像方法对肺栓塞患者的诊断结果(例)
Table 4. Pulmonary embolism patients diagnostic results by two different imaging methods
肺V/Q平面显像 肺Q SPECT/CT 总计 阳性 阴性 阳性 39 0 39 阴性 10 20 30 总计 49 20 69 注:表中,肺V/Q平面显像:肺通气/灌注平面显像;肺Q SPECT/CT:肺灌注SPECT/CT。
下载: 导出CSV
-
[1] 王铁, 杨媛华, 张镭, 等.肺灌注断层显像与平面显像在肺栓塞诊断中的比较[J].首都医科大学学报, 2008, 29(1):3-7. doi: 10.3969/j.issn.1006-7795.2008.01.002
[2] PIOPED Investigators. Value of the ventilation/perfusion scan in acute pulmonary embolism. Results of the prospective investigation of pulmonary embolism diagnosis(PIOPED)[J]. JAMA, 1990, 263(20):2753-2759. [3] 苏福, 范群, 陈国强.肺灌注显像结合肺64排螺旋CT平扫对急性肺栓塞的诊断价值[J].福建医药杂志, 2013, 35(4):116-118. doi: 10.3969/j.issn.1002-2600.2013.04.052
[4] Zöphel K, Bacher-Stier C, Pinkert J, et al. Ventilation/perfusion lung scintigraphy:what is still needed A review considering technetium-99m-labeled macro-aggregates of albumin[J]. Ann Nucl Med, 2009, 23(1):1-16. [5] 苏剑, 程勇, 李芳, 等. 64层CT血管成像与肺通气灌注显像诊断肺栓塞的对比研究[J].医学影像学杂志, 2011, 21(1):37-39.
[6] 明莫瑜.胸部CT平扫在肺栓塞诊断中的临床价值[J].临床合理用药杂志, 2012, 5(14):28-29. doi: 10.3969/j.issn.1674-3296.2012.14.020
[7] 孟庆乐, 姚薇萱, 王峰, 等.肺栓塞诊断中SPECT/CT融合显像技术与肺通气/灌注平面显像方法的比较[J].南京医科大学学报:自然科学版, 2010(8):1206-1208.
[8] No authors listed. Radiation dose to patients from radiopharmaceuticals(addendum 2 to ICRP publication 53)[J]. Ann ICRP, 1998, 28(3):1-126. doi: 10.1016/S0146-6453(99)00006-8 [9] Gutte H, Mortensen J, Jensen CV, et al. Detection of pulmonary embolism with combined ventilation-perfusion SPECT and low-dose CT:head-to-head comparison with multidetector CT angiography[J]. J Nucl Med, 2009, 50(12):1987-1992. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 2766
- HTML全文浏览量: 1585
- PDF下载量: 16