


-
分化型甲状腺癌(differentiated thyroid cancer,DTC)是最常见的内分泌肿瘤,占所有恶性肿瘤的1%,一般预后良好[1]。但是多达20%的患者出现局部或者远处复发[2]。TSH刺激状态下,131I全身显像和甲状腺球蛋白(Thyroglobulin,Tg)水平是监测疾病复发的灵敏指标[3]。但是当甲状腺癌细胞失分化后失去摄131I能力,将导致131I全身显像的假阴性结果。而作为一种高效的检查方法,18F-FDG PET/CT显像能探测患者肿瘤糖代谢增加的区域,可应用于甲状腺癌转移或者复发的检测[4],特别是对甲状腺术后复发组织进行精准的定位[5]。本研究的目的是评估18F-FDG PET/CT在131I全身显像阴性但是血清Tg水平升高的患者中的价值。
-
对我院2012年1月至2013年8月收治的32例DTC患者资料进行回顾性研究,其中女性21例、男性11例。行PET/CT检查时的平均年龄为46.9±18.5岁(16~75岁);其中25例患者为甲状腺乳头状癌、7例为滤泡状癌。所有患者均接受全面的tumor node metastasis(TNM)分期评估(表 1),随访时间为(22.2±10.8)个月。根据Tg水平将患者分为两组:H组(>10 ng/ml)11例和L组(2~10 ng/ml)21例。
患者术前TNM分期(n) 例数 T1 9 T2 8 T3 11 T4 4 N0 9 N1a 8 N1b 15 M0 25 M1 7 表 1 患者术前tumor node metastasis分期
Table 1. Preoperative tumor node metastasis staging
本研究中的DTC患者入选标准:①病理确诊为DTC,已行甲状腺全切术及大剂量131I去除治疗后,确保甲状腺组织完全清除;②复查血清TSH≥30 mU/L,Tg>2 ng/ml,且血清Tg抗体(thyroglobulin antibodies,TgAb)阴性;③复查131I全身显像阴性;④均行18F-FDG PET/CT显像;⑤所有患者均于检查前签署了知情同意书。
-
一位有5年以上工作经验的医师对所有DTC患者行常规的颈部超声检查。研究甲状腺血管床和颈部区域的局部肿瘤的复发和区域淋巴结肿大。记录所有患者术后甲状腺血管床及颈部淋巴结的特点。
-
本研究所用131I来自北京原子高科股份有限公司。131I显像均采用西门子Symbia T16 SPECT/CT仪,配备高能准直器,采用体表跟踪技术采集图像。患者碘扫描条件完全相同:能峰364 keV,能窗20%,矩阵256×1024,扫描速度10 cm/min。诊断性131I全身显像剂量是74 MBq,口服后48 h显像。在患者血清甲状腺激素水平低于正常、TSH≥30 mU/L的情况下,甲状腺摄131I率小于1%,诊断剂量131I甲状腺显像无甲状腺床及转移灶显像。
-
所有患者血清TSH均≥30 mU/L,在申请放射性131I显像的当天先行血液采样测量血清Tg水平。采用罗氏cobas E601电化学发光仪器,筛查血清Tg评估病情,以血清Tg水平>2 ng/ml为异常。
-
所有的患者均行18F-FDG PET/CT显像(PHILIPS GEMINI TF 128-PET/CT System,该设备配置128层螺旋CT)。所有检查者至少禁食6 h,注射185~370 MBq的18F-FDG(3.7~7.4 MBq/kg),注射前血糖要求<11.1 mmol/L。注射18F-FDG后40~60 min行PET和CT的图像采集。
两名核医学科医师结合患者的临床资料和病史进行研究评价,如有分歧,通过讨论达成一致。
-
根据Shammas等[6]随访PET/CT结果和最初血清Tg水平的相关性、最后的病理检查、其他影像学检查及随访中的Tg水平,对PET/CT检查结果进行评价,具体标准如下:PET/CT显像阳性时,如病理检查结果或其他检查方法阳性或者随访中Tg持续升高,则判定为真阳性;如病理检查结果或其他检查方法证实阴性或者随访中排除转移,则判定为假阳性。PET/CT显像阴性时,如其他检查方法阴性且随访12个月没有明显的转移出现,则判定为真阴性;如PET/CT显像当时其他检查方法阳性或者Tg持续升高,则判定为假阴性。
-
分别根据血清Tg水平低于或者高于10 mg/ml的分组,对所有患者18F-FDG PET/CT显像的灵敏度、特异性、阳性和阴性预测值和准确率进行计算。
-
15例颈部局部复发或者颈部淋巴结转移的患者中,超声检测只发现了5例(33.3%)。
-
32名患者的131I全身显像均为阴性。
-
32名患者Tg水平均>2 ng/ml。18F-FDG PET/CT阳性患者Tg水平(Tg中位数为32.6 ng/ml)显著高于18F-FDG PET/CT阴性患者(Tg中位数为19.3 ng/ml)。
-
在32例患者中,18F-FDG PET/CT显像阳性者20例(63.3%)、阴性12例(36.7%)。在20例阳性患者中,真阳性18例,经术后病理证实的12例;假阳性2例,病理检查结果均为淋巴结炎症。18例真阳性患者中,15例出现了局部复发和(或)颈部淋巴结转移;6例出现远处转移,其中4例合并局部复发或远处转移(表 2、表 3)。8例经颈部彩超或病理穿刺证实为假阴性患者的具体情况见表 4。
PET/CT显像结果(n) Tg水平(n) 超声结果(n) L组 H组 阳性 20△ 4 16 5 阴性 12※ 7 5 27 注:表中,Tg:甲状腺球蛋白;H组:Tg水平>10 ng/ml的分化型甲状腺癌患者;L组:Tg水平为2~10 ng/ml的分化型甲状腺癌患者;△:20例PET/CT显像阳性患者中,真阳性18例,假阳性2例;※:12例PET/CT显像阴性患者中,真阴性4例,假阴性8例。 表 2 分化型甲状腺癌患者的18F-FDG PET/CT显像结果与甲状腺球蛋白水平汇总
Table 2. Summary of thyroglobulin levels and results of 18F-FDG PET/CT imaging in differentiated thyroid cancer patients
患者序号 PET/CT显像结果阳性 穿刺 病理结果 手术 局部复发 颈部淋巴结转移 远处转移 1 - + - 是 + 是 2 + - + 否 - 否 3 - + - 是 + 是 4 - + - 是 - 否 5 - - + 否 - 否 6 - + - 是 + 是 7 + - + 否 - 否 8 - + - 是 + 是 9 - + + 否 - 否 10 + + - 是 + 是 11 + - - 是 + 是 12 - + - 是 - 否 13 + + - 是 + 是 14 + - - 是 + 是 15 - + - 是 + 是 16 - + - 是 + 是 17 + - - 是 + 是 18 - - - 否 - 否 19 - - + 否 - 否 20 - + + 是 + 是 阳性合计(n) 7 12 6 14 12 12 表 3 分化型甲状腺癌患者18F-FDG PET/CT显像阳性结果、病理及手术情况
Table 3. Results of different imaging modalities, pathology and surgery management in differentiated thyroid cancer patients with positive 18F-FDG PET/CT
患者序号 颈部彩超 穿刺 病理结果 手术 局部复发 颈部淋巴结转移 远处转移 1 + - - 是 + 是 2 + - - 是 + 是 3 + - - 是 + 是 4 + - - 是 + 是 5 + - - 是 + 是 6 - + - 是 + 是 7 + - - 是 + 是 8 - + - 是 + 是 表 4 18F-FDGPET/CT显像假阴性的分化型甲状腺癌患者的检查手段及最终结果
Table 4. Results of different imaging modalities and impact on clinical management in differentiated thyroid cancer patients with negative 18F-FDG PET/CT
-
32例患者中的18例因为18F-FDG PET/CT结果导致了治疗方式的改变。其中,12例局部复发患者均行了一期切除手术和淋巴结清扫手术;18F-FDG PET/CT指导了手术策略的选择;6名患者因18F-FDG PET/CT发现手术无法切除的转移(图 1、图 2)而改变了最初的治疗方案。
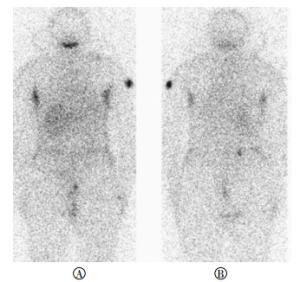
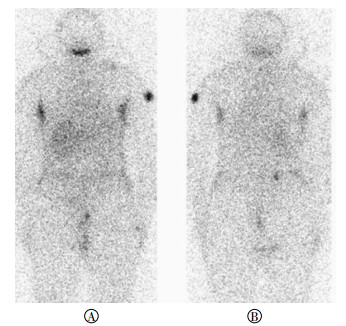
图 1 分化型甲状腺癌患者131I全身显像图 患者女性,42岁,甲癌术后5年,因甲状腺球蛋白水平高,先后进行了4次131I治疗。图中,A:131I全身显像前位像;B:后位像。131I全身显像结果示131I全身显像阴性(注:患者左肩经SPECT/CT断层融合显像证实为体表污染)。
Figure 1. 131I whole body scan findings of differentiated thyroid cancer patient
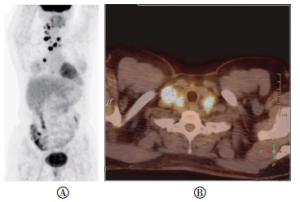
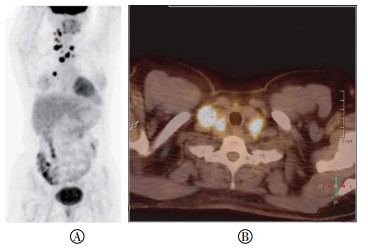
图 2 分化型甲状腺癌患者18F-FDG PET/CT显像图 患者女性,42岁,甲癌术后5年,因甲状腺球蛋白水平高,先后进行了4次131I治疗。图中,A:全身最大密度投影图;B:PET/CT融合图横断面。18F-FDG PET/CT显像结果提示颈部、纵隔、肺等部位有代谢增高(注:右颈部淋巴结穿刺,病理证实为甲状腺癌转移灶)。
Figure 2. 18F-FDG PET/CT findings of differentiated thyroid cancer patient with distant metastatic recurrence
-
18F-FDG PET/CT显像总的灵敏度和特异度分别为69.2%和66.7%。18F-FDG PET/CT显像在L组中的灵敏度为33.3%;在H组中其灵敏度为80.0%;事实上,在H组,当Tg水平 > 10 ng/ml时,不存在假阳性,其特异度和总阳性预测值均为100%;而在L组,当Tg水平≤10 ng/ml时,其特异度和总阳性预测值则分别为50.0%、60.0%(表 5)。
组别 例数
(n)阳性数
(n)阴性数
(n)真阳性数
(n)假阳性数
(n)真阴性数
(n)假阴性数
(n)灵敏度
(%)特异性
(%)诊断一致率
(%)阳性预测值
(%)阴性预测值
(%)H组 21 16 5 16 0 1 4 80.0 100 80.9 100 20 L组 11 4 7 2 2 3 4 33.3 60.0 45.5 50.0 42.9 总指标 32 20 12 18 2 4 8 69.2 66.7 68.8 90.0 33.3 注:表中,H组:Tg水平>10 ng/ml的分化型甲状腺癌患者;L组:Tg水平为2~10 ng/ml的分化型甲状腺癌患者。 表 5 分化型甲状腺癌患者18F-FDG PET/CT的结果和甲状腺球蛋白水平相比较
Table 5. The comparation of 18F-FDG PET/CT findings and serum thyroglobulin levels of the differentiated thyroid cancer patients
-
DTC术后,131I治疗后出现复发,但131I全身显像阴性时,手术治疗可能是目前唯一的方法,所以必须对全身131I显像阴性的患者进行精确地定位。本研究结果表明,18F-FDG PET/CT对临床DTC患者,特别是在探测和精准定位局部复发及远处转移上是一种潜在的有用的方法。本研究还发现,疑诊甲状腺复发或转移的患者,当其131I全身显像阴性时,进行18F-FDG PET/CT检查的整体的灵敏度、特异度及准确率分别为69.2%、66.7%及68.8%。以前报道的18F-FDG PET/CT的特异度更是高达82.4%[6]。本研究整体的特异度(66.7%)较低,主要因为研究对象少,只有4个真阴性结果和2个假阳性病例。DTC生长缓慢,只有更长时间的随访才能显示,无论依靠任何检查,只要被诊断为假阴性的患者若持续无症状,则被判定为真阴性。一般情况下,18F-FDG PET/CT假阳性结果有几个来源,包括在棕色脂肪瘤、肌肉、唾液腺、扁桃体和声带等上的非特异性摄取[7]。其他类型的癌症如前所示,18F-FDG PET/CT提供的代谢和解剖信息可以区分生理性或者病理性摄取[8]。
本研究中18F-FDG PET/CT检测DTC的总灵敏度为69.2%,这和以前报道的18F-FDG PET/CT探查甲状腺癌的复发数据相近,但整体检出率较低[6, 9],这可能与本研究中纳入患者血清Tg水平较低及肿瘤对机体的危害程度低有关。在检测甲状腺癌方面,18F-FDG PET/CT显像的灵敏度主要依赖于代谢活性,与集聚放射性131I的能力呈反比[10]。因此,18F-FDG PET/CT对于Tg水平升高且131I全身显像阴性的DTC患者来说特别有用[6, 10]。在本研究中,当Tg水平≤10 ng/ml时,18F-FDG PET/CT的灵敏度为33.3%,Tg水平 > 10 ng/ml时,18F-FDG PET/CT的灵敏度为80.0%。这些研究结果与之前的研究相符,18F-FDG PET/CT对Tg水平升高患者的检测灵敏度偏高[6, 11-12]。18F-FDG PET/CT检测DTC相当有效,尤其是在患者血清Tg水平 > 10 ng/ml且131I全身显像呈阴性的时候。但是,在本研究中,H组Tg水平 > 10 ng/ml时,18F-FDG PET/CT检测的特异度为100%,归因于此组中没有假阳性患者。
在本研究中,18例阳性患者中,18F-FDG PET/CT发现了其中的15例(83.3%)。超声检查只发现了15例中的5例(33.3%)有局部复发,而超声一直被认为是检测甲状腺癌患者颈部淋巴结转移的敏感工具[13]。本研究结果显示,18F-FDG PET/CT显像因具有较高的检出率可以在相当大的人群中指导外科,因此更具优势,其劣势为显像成本比超声检查高。其他检查也可以用来探测头颈部的复发,但因甲状腺术后结构发生了重建,因此在手术部位行MRI和CT检查时,其灵敏度和特异度较低[2, 14]。
本研究中的18例患者(56.2%)经过18F-FDG PET/CT显像后改变了患者的治疗方法,指导了其中12例(37.5%)进行外科手术治疗。在这些患者中,18F-FDG PET/CT显像提供了代谢和解剖等重要的诊断信息并对复发性病灶进行了精准定位。
该研究的局限性在于阴性和假阳性患者的分类依据是随访的Tg水平的高低。甲状腺切除后和放射性131I去除治疗后,血清Tg水平上升或者持续>10 ng/ml,可考虑甲状腺癌复发,可经验性给予131I治疗[15]。一般情况下,患者血清中没有探测到Tg水平(<1 ng/ml)均被认为治愈[16]。本研究中的32例DTC患者血清TgAb阴性,以此排除了其对Tg的影响。但是临床还有很多DTC患者伴随有TgAb阳性。有研究表明,18F-FDG PET/CT对TgAb阳性、全身显像阴性的DTC患者也有很高的灵敏度[17-18],但是此研究还需要扩大病例数,需要进一步深入研究。
综上所述,当怀疑甲状腺癌复发且131I全身显像阴性时,颈部超声检查探测局部复发的灵敏度太低。18F-FDG PET/CT是形态和功能图像的最佳结合,可以作为常规诊断工具,对明确有此类复发或转移的患者有重要的诊断价值。
18F-FDG PET/CT显像在Tg阳性131I全身显像阴性的分化型甲状腺癌患者中的应用价值
The application value of 18F-FDG PET/CT in patients with differentiated thyroid cancer of high thyroglobulin level and negative 131I whole body scan
-
摘要:
目的 评判18F-FDG PET/CT作为一个常规的检查工具对临床诊断怀疑为分化型甲状腺癌(DTC)复发、伴有甲状腺球蛋白(Tg)升高且131I全身显像阴性患者的价值。 方法 对甲状腺全切后经放射性131I去除治疗后的32例Tg升高伴全身131I显像阴性的DTC患者行18F-FDG PET/CT显像。按照Tg水平将患者分2组:H组21例(>10 ng/ml)和L组11例(2~10 ng/ml)。分别采用超声、病理学检查和临床随访对结果进行验证,评估18F-FDG PET/CT在DTC中的诊断价值。 结果 32例患者中,20例18F-FDG PET/CT显像阳性,其中18例真阳性,2例假阳性。在18例真阳性患者中,15例是局部复发,6例有远处转移,3例患者同时有局部侵犯伴远处转移。12例18F-FDG PET/CT显像阴性,其中真阴性4例,假阴性8例,总体灵敏度、特异度和准确率分别为69.2%、66.7%和68.8%。,H组的18F-FDG PET/CT显像灵敏度(80%)、特异度(100%)和准确率(80.9%)跟L组(33.3%、60.0%和45.5%)比较均显著增加。32例患者中的18例(56.2%)的临床处理策略发生了改变,12例(37.5%)进行了指导性根治手术。 结论 18F-FDG PET/CT可以探测和准确定位DTC中Tg升高且131I全身显像阴性的区域复发和远处转移,因此可推荐为常规的诊断工具。 -
关键词:
- 氟脱氧葡萄糖F18 /
- 正电子发射断层显像术 /
- 体层摄影术, X线计算机 /
- 甲状腺肿瘤 /
- 甲状腺球蛋白 /
- 血清白蛋白, 放射性碘标记
Abstract:Objective To estimate the valuate of 18F-FDG PET/CT as a routine examination for the patients with suspected differentiated thyroid carcinoma(DTC) recurrence, accompanied by the increase of thyroglobulin(Tg) and negative 131I whole body scan. Method 32 patients who suffered from DTC receiving post-operative 131I therapy, with increase of Tg and negative 131I whole body scan, were performed 18F-FDG PET/CT, and follow-up continued. Patients were divided into two groups according to the level of Tg:H group(Tg > 10 ng/ml)and L group(Tg < 10 ng/ml). Histopathological examination, ultrasound examination and clinical follow-up were used to verify the result, and assess the clinical value of PET/CT. Result PET/CT imaging results indicated that among 32 patients, there were 20 positive(18 true-positive and 2 false-positive) and 12 negative(4 true-negative and 8 false-negative). Among 18 patients with true positive, 15 cases with local disease, 6 cases with distant metastasis, and 3 patients with both local invasion and distant metastasis. The overall sensitivity, specificity and accuracy were 69.2%, 66.7% and 68.8%, respectively. Compared with the L group, H group developed higher sensitivity(80% versus 33.3%), specificity(100% versus 60%) and accuracy(80.9% versus 45.5%). In 32 patients, 18 cases(56.2%) changed the strategies of clinical treatment, and 12 cases(37.5%) were received the radical operation under guidance. Conclusion 18F-FDG PET/CT can detect and locate accurately for the regional metastasis and recurrence of patients with DTC, accompanied by the increase of serum Tg and negative 131I whole body scan. Therefore, it can be recommended as a routine diagnostic tool. -
图 1 分化型甲状腺癌患者131I全身显像图 患者女性,42岁,甲癌术后5年,因甲状腺球蛋白水平高,先后进行了4次131I治疗。图中,A:131I全身显像前位像;B:后位像。131I全身显像结果示131I全身显像阴性(注:患者左肩经SPECT/CT断层融合显像证实为体表污染)。
Figure 1. 131I whole body scan findings of differentiated thyroid cancer patient
图 2 分化型甲状腺癌患者18F-FDG PET/CT显像图 患者女性,42岁,甲癌术后5年,因甲状腺球蛋白水平高,先后进行了4次131I治疗。图中,A:全身最大密度投影图;B:PET/CT融合图横断面。18F-FDG PET/CT显像结果提示颈部、纵隔、肺等部位有代谢增高(注:右颈部淋巴结穿刺,病理证实为甲状腺癌转移灶)。
Figure 2. 18F-FDG PET/CT findings of differentiated thyroid cancer patient with distant metastatic recurrence
表 1 患者术前tumor node metastasis分期
Table 1. Preoperative tumor node metastasis staging
患者术前TNM分期(n) 例数 T1 9 T2 8 T3 11 T4 4 N0 9 N1a 8 N1b 15 M0 25 M1 7  下载: 导出CSV
下载: 导出CSV
表 2 分化型甲状腺癌患者的18F-FDG PET/CT显像结果与甲状腺球蛋白水平汇总
Table 2. Summary of thyroglobulin levels and results of 18F-FDG PET/CT imaging in differentiated thyroid cancer patients
PET/CT显像结果(n) Tg水平(n) 超声结果(n) L组 H组 阳性 20△ 4 16 5 阴性 12※ 7 5 27 注:表中,Tg:甲状腺球蛋白;H组:Tg水平>10 ng/ml的分化型甲状腺癌患者;L组:Tg水平为2~10 ng/ml的分化型甲状腺癌患者;△:20例PET/CT显像阳性患者中,真阳性18例,假阳性2例;※:12例PET/CT显像阴性患者中,真阴性4例,假阴性8例。
下载: 导出CSV
表 3 分化型甲状腺癌患者18F-FDG PET/CT显像阳性结果、病理及手术情况
Table 3. Results of different imaging modalities, pathology and surgery management in differentiated thyroid cancer patients with positive 18F-FDG PET/CT
患者序号 PET/CT显像结果阳性 穿刺 病理结果 手术 局部复发 颈部淋巴结转移 远处转移 1 - + - 是 + 是 2 + - + 否 - 否 3 - + - 是 + 是 4 - + - 是 - 否 5 - - + 否 - 否 6 - + - 是 + 是 7 + - + 否 - 否 8 - + - 是 + 是 9 - + + 否 - 否 10 + + - 是 + 是 11 + - - 是 + 是 12 - + - 是 - 否 13 + + - 是 + 是 14 + - - 是 + 是 15 - + - 是 + 是 16 - + - 是 + 是 17 + - - 是 + 是 18 - - - 否 - 否 19 - - + 否 - 否 20 - + + 是 + 是 阳性合计(n) 7 12 6 14 12 12
下载: 导出CSV
表 4 18F-FDGPET/CT显像假阴性的分化型甲状腺癌患者的检查手段及最终结果
Table 4. Results of different imaging modalities and impact on clinical management in differentiated thyroid cancer patients with negative 18F-FDG PET/CT
患者序号 颈部彩超 穿刺 病理结果 手术 局部复发 颈部淋巴结转移 远处转移 1 + - - 是 + 是 2 + - - 是 + 是 3 + - - 是 + 是 4 + - - 是 + 是 5 + - - 是 + 是 6 - + - 是 + 是 7 + - - 是 + 是 8 - + - 是 + 是
下载: 导出CSV
表 5 分化型甲状腺癌患者18F-FDG PET/CT的结果和甲状腺球蛋白水平相比较
Table 5. The comparation of 18F-FDG PET/CT findings and serum thyroglobulin levels of the differentiated thyroid cancer patients
组别 例数
(n)阳性数
(n)阴性数
(n)真阳性数
(n)假阳性数
(n)真阴性数
(n)假阴性数
(n)灵敏度
(%)特异性
(%)诊断一致率
(%)阳性预测值
(%)阴性预测值
(%)H组 21 16 5 16 0 1 4 80.0 100 80.9 100 20 L组 11 4 7 2 2 3 4 33.3 60.0 45.5 50.0 42.9 总指标 32 20 12 18 2 4 8 69.2 66.7 68.8 90.0 33.3 注:表中,H组:Tg水平>10 ng/ml的分化型甲状腺癌患者;L组:Tg水平为2~10 ng/ml的分化型甲状腺癌患者。
下载: 导出CSV
-
[1] Schlumberger MJ, Torlantano M. Papillary and follicular thyroid carcinoma[J]. Best Pract Res Clin Endocrinol Metab, 2000, 14(4):601-613. doi: 10.1053/beem.2000.0105 [2] Makeieff M, Burcia V, Raingeard I, et al. Positron emission tomography-computed tomography evaluation for recurrent differentiated thyroid carcinoma[J]. Eur Ann Otorhinolaryngol Head Neck Dis, 2012, 129(5):251-256. doi: 10.1016/j.anorl.2012.01.003 [3] Sherman SI. Thyroid carcinoma[J]. Lancet, 2003, 361(9356):501-511. doi: 10.1016/S0140-6736(03)12488-9 [4] Stokkel MP, Duchateau CS, Dragoiescu C. The value of FDG-PET in the follow-up of differentiated thyroid cancer:a review of the literature[J]. Q J Nucl Med Mol Imaging, 2006, 50(1):78-87. [5] Lee JW, Lee SM, Lee DH, et al. Clinical utility of 18F-FDG PET/CT concurrent with 131I therapy in intermediate-to-high-risk patients with differentiated thyroid cancer:dual-center experience with 286 patients[J]. J Nucl Med, 2013, 54(8):1230-1236. doi: 10.2967/jnumed.112.117119 [6] Shammas A, Degirmenci B, Mountz JM, et al. 18F-FDG PET/CT in patients with suspected recurrent or metastatic well-differentiated thyroid cancer[J]. J Nucl Med, 2007, 48(2):221-226. [7] Von Schulthess GK, Hany TF. Imaging and PET-PET/CT imaging[J]. J Radiol, 2008, 89(3 Pt 2):438-448. [8] Townsend DW. Dual-modality imaging:combining anatomy and function[J]. J Nucl Med, 2008, 49(6):938-955. doi: 10.2967/jnumed.108.051276 [9] Bannas P, Derlin T, Groth M, et al. Can 18F-FDG-PET/CT be generally recommended in patients with differentiated thyroid carcinoma and elevated thyroglobulin levels but negative 131I whole body scan?[J]. Ann Nucl Med, 2012, 26(1):77-85. [10] Bertagna F, Bosio G, Biasiotto G, et al. 18F FDG-PET/CT evaluation of patients with differentiated thyroid cancer with negative 131I total body scan and high thyroglobulin level[J]. Clin Nucl Med, 2009, 34(11):756-761. doi: 10.1097/RLU.0b013e3181b7d95c [11] Ko MS, Lee JH, Shong YK, et al. Normal and abnormal sonographic findings at the thyroidectomy sites in postoperative patients with thyroid malignancy[J]. AJR Am J Roentgenol, 2010, 194(6):1596-1609. doi: 10.2214/AJR.09.2513 [12] Vural GU, Akkas BE, Ercakmak N, et al. Prognostic significance of FDG PET/CT on the follow-up of patients of differentiated thyroid carcinoma with negative 131I whole-body scan and elevated thyroglobulin levels:correlation with clinical and histopathologic characteristics and long-term follow-up data[J]. Clin Nucl Med, 2012, 37(10):953-959. doi: 10.1097/RLU.0b013e31825b2057 [13] Torlontano M, Attard M, Crocetti U, et al. Follow-up of low risk patients with papillary thyroid cancer:role of neck ultrasonography in detecting lymph node metastases[J]. J Clin Endocrinol Metab, 2004, 89(7):3402-3407. doi: 10.1210/jc.2003-031521 [14] Rosário PW, De Faria S, Bicalho L, et al. Ultrasonographic differentiation between metastatic and benign lymph nodes in patients with papillary thyroid carcinoma[J]. J Ultrasound Med, 2005, 24(10):1385-1389. doi: 10.7863/jum.2005.24.10.1385 [15] 滕卫平, 刘永峰, 高明, 等.甲状腺结节和分化型甲状腺癌诊治指南[J].中国肿瘤临床, 2012, 33(17):1249-1272.
[16] David A, Blotta A, Rossi R, et al. Clinical value of different responses of serum thyroglobulin to recombinant human thyrotropin in the follow-up of patients with differentiated thyroid carcinoma[J]. Thyroid, 2005, 15(2):158-164. doi: 10.1089/thy.2005.15.158 [17] Ozkan E, Aras G, Kucuk NO. Correlation of 18F-FDG PET/CT findings with histopathological results in differentiated thyroid cancer patients who have increased thyroglobulin or antithyroglobulin antibody levels and negative 131I whole-body scan results[J]. Clin Nucl Med, 2013, 38(5):326-331. doi: 10.1097/RLU.0b013e318286827b [18] Ozkan E, Soydal C, Araz M, et al. The additive clinical value of 18F-FDG PET/CT in defining the recurrence of disease in patients with differentiated thyroid cancer who have isolated increased antithyroglobulin antibody levels[J]. Clin Nucl Med, 2012, 37(8):755-758. doi: 10.1097/RLU.0b013e31825ae77b -

 点击查看大图
点击查看大图
计量
- 文章访问数: 2512
- HTML全文浏览量: 1286
- PDF下载量: 3