




-
冠心病是由于冠状动脉粥样硬化引起冠状动脉循环的改变,导致冠状血流和心肌需求之间不平衡而出现心肌损害,其病理生理基础是心肌微循环状态失衡和冠状动脉血流量调节障碍[1]。心肌灌注成像(myocardial perfusion imaging,MPI)是评价心肌微循环和判断心血管疾病预后及不良事件的重要无创性检查方法[2]。冠状动脉解剖学情况和心肌灌注微循环情况相结合,对于指导缺血性心脏病患者的治疗至关重要。目前评价冠状动脉解剖学情况的主要方法是传统的冠状动脉造影(coronary angiography,CAG)或冠状动脉CT血管造影(coronary CT angiography,CCTA),评价心肌微循环灌注的主要方法为核素心肌灌注成像、磁共振心肌灌注成像等[3-4]。这些检查方法有一定的缺陷,并且都不能同时得到能够用于诊断的冠状动脉和心肌灌注图像。因此寻找一种“一站式”且能够准确得到冠状动脉管腔图像和心肌灌注图像的方法有重要的临床意义。CT灌注成像不仅可以准确地评价冠状动脉及心腔的解剖学信息,同时又能获得心肌灌注和心功能的功能学信息[5-7]。然而,传统的动态CT心肌灌注需要分次进行冠状动脉和心肌动态灌注扫描,有效射线剂量高。双源CT(dual source computed tomography)双能量(dual-energy)扫描可一次性获得冠状动脉和双能量MPI图像,“一站式”完成冠状动脉的形态学和心肌血供信息[8-11]。第二代双源CT在第一代双源CT的基础上,扩大了扫描视野,通过设置能量滤过器,纯化了能谱[12]。本研究通过建立猪急性心肌梗死模型,以组织病理学和传统CAG结果为金标准,评价第二代双源CT双能量“一站式”CCTA结合MPI检测急性心肌梗死的准确率。
-
7只健康家猪(泰州泰和生物科技有限公司,中国江苏),25~34 kg,雌雄不限。所有检查在普通麻醉及连续心电监护下进行。给予氯胺酮(福建古田药业有限公司,中国福建)6 mg/kg、咪达唑仑(江苏恩华药业集团有限公司,中国江苏)0.2 mg/kg和长托宁(成都力思制药股份有限公司)1 mg肌肉注射镇静后,建立静脉通道,静脉注射丙泊酚(西安力邦制药有限公司,中国西安)3.5 mg/kg,然后静脉持续泵注丙泊酚6~8 mg/(kg·h),保持麻醉状态,并监测其生命体征。术中以艾司洛尔(齐鲁制药有限公司,中国山东)控制心率,即刻控制剂量为1 mg/kg,在30 s内静脉注射,继之以0.15 mg/(kg·min)静脉泵注,最大维持量为0.3 mg/(kg·min)。若心率下降至70 bpm以下,立即停止输注艾司洛尔,静脉注射阿托品提升心率。这一参数用来进行整个心脏介入、CT检查。
常规消毒铺巾,使用外科切开包分离右侧股动脉,直视穿刺股动脉置入6-French动脉鞘管。静脉注入肝素10000 IU,以后每隔1 h追加注射肝素1000 IU。经动脉鞘置入CAG导管分别行左、右CAG,之后将5-French引导导管(美敦力中国有限公司)置于左冠状动脉开口,将雅培宝马导丝置于前降支第一、二对角支之间,在导丝指引下置入3-French球囊(2.0 mm×20 mm,美敦力中国有限公司)至前降支第二对角支远端,以2个标准大气压打开球囊预适应3~4次,阻断前向血流1 min、2 min、5 min,每次间隔60 s,然后将微导管置于球囊扩张处,将自制的明胶海绵栓子(1.5 mm×1.5 mm)推注到前降支中段第一、二对角支之间。术中予连续心电监护以及动脉内压力监测。术后限制猪活动,从第二天开始进食,肌肉注射庆大霉素2万单位预防感染。所有实验猪分别在造模前20 min、心肌梗死后即刻、心肌梗死后24 h进行CAG检查。
-
所有实验猪分别在造模前20 min、心肌梗死后即刻、心肌梗死后24 h采用第二代双源CT系统(SOMATOM Definition Flash,德国西门子医疗)回顾性心电门控双能量扫描模式进行心脏增强扫描。扫描范围从气管分叉下2 cm到膈部进行扫描,从头向足方向。团注方法采用团注追踪技术,非离子造影剂碘海醇(欧乃派克350,350 mg/ml,GE医疗,美国)1.5 ml/kg,用双筒高压注射器以4.0 ml/s的速率静脉注射,主动脉根部为感兴趣区(阈值100 Hu),峰值时间后延迟4 s开始扫描,之后以同样的速率注入生理盐水40 ml。扫描参数:准直2×64×0.6 mm,层厚:z-飞焦点方法采集2×128×0.6 mm,转速280 ms,管球电压A/B:100/140 Sn kV,管球电流A/B:84~100/76~88 mAs,螺距0.28 pitch,探测器宽度350 mm。
扫描完成后,图像重建系统自动获取3组图像:①140 Sn kV空间分辨率优化图像;②100 kV最佳强化优化图像;③融合70% 140 Sn kV数据和30% 100 kV的平均加权图像(M_0.3)。图像重建:①CCTA图像重建,将100 kV /140 Sn kV融合图像采用回顾性心电门控自动最佳成像,时间窗以0.75 mm层厚进行重建图像,重建间隔0.4 mm,采用软组织卷积核(B26f)。扫描后图像经最大密度投影、曲面重建、容积再现和心血管优化分析软件等处理,筛选最佳CT图像用于血管评价。②心肌灌注重建评价,将100 kV /140 Sn kV 2组数据调入心脏灌注血容量软件(VE44版本,西门子医疗),层厚1.5 mm,重建间隔0.5 mm,采用软组织卷积核(D30f),处理得到颜色编码的碘图,即心肌内碘灌注分布图(分别以横断面、心室短轴面、长轴面及四腔心面显示)。
-
左心室心肌分段根据美国心脏病协会关于心肌的17节段模型,即左心室壁在长轴位上分为3个层面(基底段、中间段、心尖段);在短轴位上,3个层面再被分为16个节段,加上1个心尖部,共17节段(前壁基底段、前间隔基底段、下间隔基底段、下壁基底段、下侧壁基底段、前侧壁基底段、前壁中间段、前间隔中间段、下间隔中间段、下壁中间段、下侧壁中间段、前侧壁中间段、前壁心尖段、室间隔心尖段、下壁心尖段、侧壁心尖段、心尖)[13](图 1)。分别由有3年和2年的独立阅读双能量CT经验的医师,在不知道病理结果的情况下对双能量CT心肌灌注碘图作出评价,碘图采用4级评分法,即0分正常、1分稀疏、2分明显稀疏、3分缺损[14]。2分以上为灌注异常。测量低灌注区域与正常灌注区域的含碘值(mg/ml)。
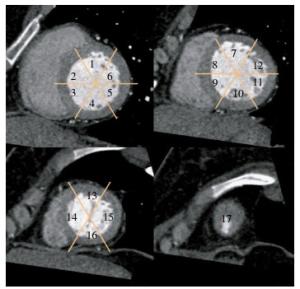
图 1 正常心肌节段划分左室短轴位图 图中,1:前壁基底段;2:前间隔基底段;3:下间隔基底段;4:下壁基底段;5:下侧壁基底段;6:前侧壁基底段;7:前壁中间段;8:前间隔中间段;9:下间隔中间段;10;下壁中间段;11:下侧壁中间段;12:前侧壁中间段;13:前壁心尖段;14:室间隔心尖段;15:下壁心尖段;16:侧壁心尖段;17:心尖。
Figure 1. Left ventricular stort axis view of normal myocardial segments
冠状动脉评价根据美国心脏病协会推荐的16分段法:右冠状动脉包括1~4段,左主干和左前降支包括5~10段,回旋支包括11~15段,中间支为16段,闭塞血管以远段不记入分析[15]。冠状动脉图像分为4级,相应评为1~4分:1级为血管显示良好,边界清晰,无伪影或血管中断;2级为血管边界模糊,有轻度伪影;3级为血管有中度伪影,尚能满足诊断要求;4级为血管显示不清,有严重伪影,不能作出诊断[16]。
有效辐射剂量:通过CT自动计算得到剂量长度乘积(dose length product,DLP),单位有效剂量(effective dose,ED)=k×DLP(k为转换系数,胸部k=0.014 mSv·mGy-1·cm-1),k值参照欧盟委员会关于CT的质量标准指南[17]。
-
CT检查结束后,立即给模型猪静脉注射空气50 ml致死,迅速取出心脏,清水洗净放在-20℃的冰箱里冰冻1 h。沿短轴切面将左心室连续切片,尽可能与双能量CT体层方向一致,层厚3 mm,平展浸于1%氯化三苯基四氮唑溶液中,37℃恒温下染色1 h,拍摄染色后各层面图像,然后以10%福尔马林固定。分别于梗死中央区、周围区及正常心肌部位取材做病理检查,苏木精-伊红染色法(hematoxylin-eosin staining,HE),染色后在光镜下观察。
-
采用SPSS 19软件进行统计学分析,计量资料采用x±s。以病理结果为参考标准,计算双能量CT心肌灌注碘图诊断心肌灌注缺损节段的敏感度、特异度、阳性预测值和阴性预测值。不同观察者间的一致性检验采用Cohen′s kappa分析(kappa > 0.81为一致性极好;kappa=0.61~0.80为一致性良好;kappa=0.41~0.60为一致性中等;kappa=0.21~0.40为一致性一般;kappa < 0.20为一致性差)。
-
共有7只猪进行心肌梗死建模,平均体质量(29±3.8)kg(25~34 kg)。其中有2只于介入过程中死亡;2只在闭塞前降支过程中发生室速,给予利多卡因静脉推注后转复,即有5只成功建成模型(其中1只闭塞右冠状动脉远段、2只闭塞前降支中段+回旋支近段、2只闭塞前降支中段)。
-
基于碘图节段分析,双能量CT心肌灌注共评价85个心肌节段,检测出45个血池缺损节段,40个正常心肌节段。以病理结果为金标准,43个节段证实为梗死区域,2个节段为假阳性,3个节段为假阴性。1号猪13节段为假阳性,14节段、16节段为假阴性;3号猪6节段为假阳性;5号猪2节段为假阴性。基于血管分布区域分析,共评价15个血管分布区域,其中9个区域检测出血池缺损区域、6个区域为正常心肌区域。以病理结果为金标准,2个区域证实为假阳性,1个区域为假阴性。双能量CT和组织病理学检出心肌梗死缺血节段部位和数量详见表 1,建模后24 h CT扫描得到的双能量心肌灌图像,检测心肌梗死的灵敏度、特异度、阳性预测值、阴性预测值(表 2),典型模型见图 1。
检查方法 心肌节段 合计 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 双能量CT碘图 2 2 1 2 2 0 4 4 4 1 4 0 4 4 4 3 4 45 组织病理学 2 2 1 2 2 2 4 4 4 1 4 0 2 4 4 4 4 46 表 1 双能量CT碘图和组织病理学检出心肌梗死缺血节段部位和数量(段)
Table 1. Segmental region and number of myocardial infarction detected by dual-energy CT and histopathology
准确率 基于节段评价
(n=85)基于区域评价
(n=15)真阳性 40 8 假阳性 2 1 真阴性 40 6 假阴性 3 0 灵敏度(95%可信区间) 93%(81%~98%) 100%(63%~100%) 特异度(95%可信区间) 95%(83%~99%) 86%(42%~97%) 阳性预测值(95%可信区间) 95%(83%~99%) 89%(52%~98%) 阴性预测值(95%可信区间) 93%(81%~98%) 100%(54%~100%) 表 2 双能量冠状动脉CT成像结合心肌灌注碘图检测心肌梗死的准确率
Table 2. Accuracy assessment for dual-energy CT Iodine map detection of myocardialinfarction
-
氯化三苯基四氮唑染色正常心肌为红色,缺血心肌为白色。共检测到46个梗死节段,39个正常心肌节段。取心肌梗死中央区、周边区及正常心肌区组织进行HE染色,梗死中央区及周边区均可见广泛的细胞核溶解甚至消失。HE染色梗死区在低倍镜下可见坏死心肌灶和正常心肌灶穿插排列;在高倍镜下可见心肌细胞浆凝聚,嗜酸性变,横纹消失,细胞核外移,心肌细胞间隙水肿,部分坏死较严重的可见细胞核消失,细胞整体呈现嗜碱性颗粒状,证明成功建成急性心肌梗死模型。

图 2 建模前后冠状动脉造影和冠状动脉CT血管造影图 图中,A:造模前冠状动脉CT血管造影;B:双能量CT心肌灌注显示心肌灌注均匀,未见明显低灌注区域;C:前降支中远段、回旋支远段栓塞后的冠状动脉造影图;D:栓塞后的冠状动脉CT血管造影容积再现图。
Figure 2. Invasive angiography and coronary CT angiography before and after animal models
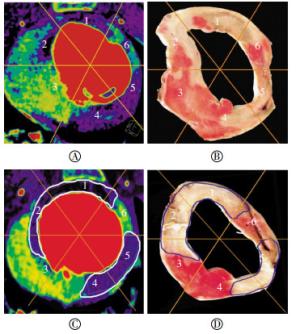
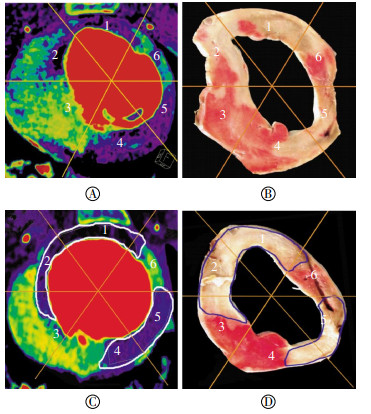
图 3 双能量CT心肌灌注碘图和心肌TTC染色标本的对照 图中,A、C为双能量碘图;B、D为TTC染色标本;显示双能量碘图心肌低灌注节段与病理染色低灌注节段相吻合。TTC:氯化三苯基四氮唑。
Figure 3. The comparison of dual-energy iodine imaging and the triphenyltetrazolium chloride pathology
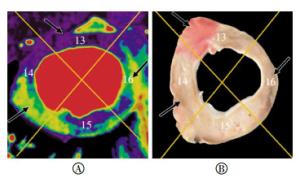
图 4 双能量碘图和TTC染色标本的对照 图中,A:双能量碘图,13节段(绿色箭头)为低灌注区域;B:TTC染色标本,TTC染色标本显示为部分正常染色,提示双能量心肌灌注为假阳性。14节段、16节段(黑色箭头)显示为假阴性。TTC:氯化三苯基四氮唑。
Figure 4. The comparison of dual-energy iodine imaging and the triphenyltetrazolium chloride pathology
-
5只猪控制心率后平均心率为(102±18)bpm(80~128 bpm),共显示56个冠状动脉节段。2只猪心率用艾司洛尔后仍超过100 bpm(分别为110、128 bpm),扫描后CCTA图像评分差,血管不可评价,其余3只猪的心率均控制在100 bpm以内,冠状动脉均可评价。心率≤100 bpm模型猪的冠状动脉节段图像质量均达到诊断要求,平均评分为1.1±0.4,心率 > 100 bpm的冠状动脉节段图像质量评分为3~4级,平均评分为3.9±0.3,不能用于诊断。
-
单次双能量CT扫描平均DLP为(219.4±60.9)mGy·cm(172~321 mGy·cm);单次双能量CT扫描平均有效射线剂量为(3.07±0.85)mSv(2.21~4.49 mSv)。
-
自2004年Hoffmann等[18]首次报道了多排螺旋CT动态心肌灌注检测急性心肌梗死猪模型的可行性以来,CT心肌灌注研究一直是临床研究的热点。双源CT双能量心肌灌注通过碘含量进行定量计算,可用来检测心肌缺血和心肌梗死。第一代双源CT双能量心肌灌注显示心肌缺血/梗死的灵敏度为72%~93%,特异度为72%~94%[6, 9-11, 19-21]。与第一代双源CT相比,第二代双源CT单个球管的转速由165 ms/圈提高至140 ms/圈[12],扩大了扫描视野,时间分辨率提高至75 ms,因而可提供更准确的碘浓度测量以及更好的冠状动脉图像质量[22]。Koonce等[22]采用体模验证了第一代和第二代双源CT双能量扫描的准确率,结果表明第二代双源CT系统双能量心肌灌注显示出更稳定的碘浓度,可提供不同体重指数患者碘浓度的精确测量。
本动物实验研究结果显示,以病理学结果为金标准,第二代双能量CT心肌灌注显示心肌梗死的敏感度为93%,特异度为95%,高于第一代双能量CT显示的准确率,与Weininger等[19]的临床研究结果接近,显示出第二代双源CT双能量心肌灌注碘图检测心肌梗死的较高准确率。本实验结果显示有2个节段为假阳性,3个节段为假阴性,其中假阳性分布于6、13节段,假阴性分布于14、16节段。假阳性的原因分析:双能量首过心肌灌注心室内的碘对比剂产生线束硬化伪影,这种线束硬化并不能被重建过程中的软组织线束硬化完全校正,影响最大的部位为四腔心层面左室下壁、前壁以及间隔壁和侧壁。进一步行心肌延迟扫描观察延迟强化可能降低单纯依靠首过心肌灌注所致的假阳性。
关于双能量心肌灌注冠状动脉的图像质量,研究显示第一代双能量CT所有的冠状动脉图像质量不能用于诊断[11, 20, 23]。本研究显示,心率≤100 bpm模型猪的冠状动脉节段图像质量均达到诊断要求,心率 > 100 bpm的冠状动脉节段图像质量差,不能用于诊断,表明第二代双源CT双能量单次增强扫描在较低心率下可获得用于诊断的图像质量,明显优于文献报道[20, 23]的第一代双源CT的成功率,这与第二代双源CT单球管时间分辨率提高有关。
在射线剂量评价方面,Ruzsics等[21]报道的双能量CT单次扫描心肌灌注的有效射线剂量为(14±5)mSv;Kerl等[10]的动物实验为(5.4±0.8)mSv。本研究的单次双能量扫描平均有效射线剂量(3.07±0.85)mSv,明显低于第一代双源CT的报道,表明第二代双能量CT扫描模式明显降低了辐射剂量,分析原因是与第二代双源CT的转速和时间分辨率的提高有关。
本研究结果显示,第二代双源CT双能量心肌灌注可“一站式”获得心肌灌注和CCTA的图像,进一步提高了心脏CT检测心肌梗死的准确率,有效射线剂量低,碘对比剂产生线束硬化伪影是造成碘图假阳性的一个重要因素。本研究不足之处:①样本量小,所得数据平均值有可能因样本量较小而造成偏倚;②样本中仅有一只右冠状动脉建模,2只回旋支建模,不容易设盲,分析者容易产生主观判断;③不能够显示诊断不同血管区域的敏感度和特异度等指标;④未进一步行延迟心肌灌注扫描。今后应进一步研究以弥补上述不足。
第二代双源CT冠状动脉成像结合双能量心肌灌注评价猪急性心肌梗死的实验研究
Evaluation of combined coronary CT angiography and dual-energy myocardial perfusion imaging for detection of acute myocardial infarction via second-generation dual-source CT: an experimental study in a porcine phantom model
-
摘要:
目的 通过建立猪急性心肌梗死模型,以组织病理学和冠状动脉造影(CAG)结果为金标准,评价第二代双源CT双能量“一站式”冠状动脉CT血管造影(CCTA)结合心肌灌注成像(MPI)检测急性心肌梗死的准确率。 方法 7只健康小型猪,采用导管介入冠状动脉明胶海绵栓塞方法制作急性心肌梗死模型,分别在造模前20 min、心肌梗死后即刻、心肌梗死后24 h行CAG及双能量模式CCTA和MPI。采用心肌17节段法评价心肌碘图灌注缺损。双盲法由2名放射科医师对图像进行评价,以病理和CAG结果为金标准,计算双能量CCTA结合心肌灌注碘图诊断心肌灌注缺损节段的灵敏度和特异度。 结果 5只小型猪成功建成急性心肌梗死模型。双能量碘图显示45个梗死节段和40个非梗死节段。以病理和CAG结果为金标准,基于节段分析得出灵敏度、特异度、阳性预测值、阴性预测值分别为93%、95%、95%、93%;基于血管分布区域分析,双能量CT心肌灌注检测心肌梗死的灵敏度、特异度、阳性预测值、阴性预测值分别为100%、86%、89%、100%。单次双能量扫描平均有效射线剂量为(3.07±0.85)mSv(2.21~4.49 mSv)。 结论 以病理和CAG结果为金标准,第二代双源CT双能量“一站式”CCTA结合心肌灌注碘图检测急性心肌梗死准确率较高,CCTA的图像质量好。 -
关键词:
- 心肌梗死 /
- 体层摄影术, X线计算机 /
- 心肌灌注 /
- 第二代双源CT
Abstract:Objective To evaluate the diagnostic accuracy of dual-energy "one-step"combined CT coronary angiography(CCTA) and myocardial perfusion imaging(MPI) for the detection of acute myocardial infarction via second-generation dual-source CT compared with histopathological and conventional coronary angiography(CAG) findings in a porcine phantom. Methods Seven minipigs underwent transcatheter embolization of the coronary arteries by using gelatin sponge to produce acute myocardial infarction. CAG, dual-energy CCTA, and MPI were performed 20 min before, immediately after, and 24 h following the modeling procedure, respectively. A color-coded iodine map was used to evaluate the myocardial perfusion defects on the 17-segment model. In consensus, two radiologists interpreted all iodine map imaging results from MPI and CCTA. Considering CAG and pathological staining as gold standards, the sensibility and specificity of the CCTA and iodine maps from MPI were evaluated using dual-energy CT. Results Models of acute myocardial infarction were successfully made in five minipigs. Following coronary embolization, dual-energy CT iodine maps showed 45 infarcted segments and 40 non-infarcted segments. Per-segment analysis indicated the sensitivity, specificity, positive predictive value and negative predictive value as 93%, 95%, 95% and 93%, respectively. The corresponding values obtained by per-territory analysis were 100%, 86%, 89% and 100%, with CAG and histopathological findings as reference standards. The effective radiation dose of each dual-energy scan was 3.07±0.85 mSv(2.21-4.49 mSv). Conclusions Dual-energy"one-step"combined CCTA and MPI iodine maps for the detection of acute myocardial infarction via second-generation dual-source CT showed enhanced diagnostic accuracy with CAG and histopathology as gold standards. -
图 1 正常心肌节段划分左室短轴位图 图中,1:前壁基底段;2:前间隔基底段;3:下间隔基底段;4:下壁基底段;5:下侧壁基底段;6:前侧壁基底段;7:前壁中间段;8:前间隔中间段;9:下间隔中间段;10;下壁中间段;11:下侧壁中间段;12:前侧壁中间段;13:前壁心尖段;14:室间隔心尖段;15:下壁心尖段;16:侧壁心尖段;17:心尖。
Figure 1. Left ventricular stort axis view of normal myocardial segments
图 2 建模前后冠状动脉造影和冠状动脉CT血管造影图 图中,A:造模前冠状动脉CT血管造影;B:双能量CT心肌灌注显示心肌灌注均匀,未见明显低灌注区域;C:前降支中远段、回旋支远段栓塞后的冠状动脉造影图;D:栓塞后的冠状动脉CT血管造影容积再现图。
Figure 2. Invasive angiography and coronary CT angiography before and after animal models
图 3 双能量CT心肌灌注碘图和心肌TTC染色标本的对照 图中,A、C为双能量碘图;B、D为TTC染色标本;显示双能量碘图心肌低灌注节段与病理染色低灌注节段相吻合。TTC:氯化三苯基四氮唑。
Figure 3. The comparison of dual-energy iodine imaging and the triphenyltetrazolium chloride pathology
图 4 双能量碘图和TTC染色标本的对照 图中,A:双能量碘图,13节段(绿色箭头)为低灌注区域;B:TTC染色标本,TTC染色标本显示为部分正常染色,提示双能量心肌灌注为假阳性。14节段、16节段(黑色箭头)显示为假阴性。TTC:氯化三苯基四氮唑。
Figure 4. The comparison of dual-energy iodine imaging and the triphenyltetrazolium chloride pathology
表 1 双能量CT碘图和组织病理学检出心肌梗死缺血节段部位和数量(段)
Table 1. Segmental region and number of myocardial infarction detected by dual-energy CT and histopathology
检查方法 心肌节段 合计 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 双能量CT碘图 2 2 1 2 2 0 4 4 4 1 4 0 4 4 4 3 4 45 组织病理学 2 2 1 2 2 2 4 4 4 1 4 0 2 4 4 4 4 46  下载: 导出CSV
下载: 导出CSV
表 2 双能量冠状动脉CT成像结合心肌灌注碘图检测心肌梗死的准确率
Table 2. Accuracy assessment for dual-energy CT Iodine map detection of myocardialinfarction
准确率 基于节段评价
(n=85)基于区域评价
(n=15)真阳性 40 8 假阳性 2 1 真阴性 40 6 假阴性 3 0 灵敏度(95%可信区间) 93%(81%~98%) 100%(63%~100%) 特异度(95%可信区间) 95%(83%~99%) 86%(42%~97%) 阳性预测值(95%可信区间) 95%(83%~99%) 89%(52%~98%) 阴性预测值(95%可信区间) 93%(81%~98%) 100%(54%~100%)
下载: 导出CSV
-
[1] Osto E, Fallo F, Pelizzo MR, et al. Coronary microvascular dysfunction induced by primary hyperparathyroidism is restored after parathyroidectomy[J]. Circulation, 2012, 126(9):1031-1039. doi: 10.1161/CIRCULATIONAHA.111.081307 [2] Metz LD, Beattie M, Hom R, et al. The prognostic value of normal exercise myocardial perfusion imaging and exercise echocardiography:a meta-analysis[J]. J Am Coll Cardiol, 2007, 49(2):227-237. doi: 10.1016/j.jacc.2006.08.048 [3] Hartlage G, Janik M, Anadiotis A, et al. Prognostic value of adenosine stress cardiovascular magnetic resonance and dobutamine stress echocardiography in patients with low-risk chest pain[J]. Int J Cardiovasc Imaging, 2012, 28(4):803-812. doi: 10.1007/s10554-011-9885-3 [4] Schwitter J, Nanz D, Kneifel S, et al. Assessment of myocardial perfusion in coronary artery disease by magnetic resonance:a comparison with positron emission tomography and coronary angiography[J]. Circulation, 2001, 103(18):2230-2235. doi: 10.1161/01.CIR.103.18.2230 [5] Feuchtner G, Goetti R, Plass A, et al. Adenosine stress high-pitch 128-slice dual-source myocardial computed tomography perfusion for imaging of reversible myocardial ischemia:comparison with magnetic resonance imaging[J]. Circ Cardiovasc Imaging, 2011, 4(5):540-549. doi: 10.1161/CIRCIMAGING.110.961250 [6] Ruzsics B, Schwarz F, Schoepf UJ, et al. Comparison of dual-energy computed tomography of the heart with single photon emission computed tomography for assessment of coronary artery stenosis and of the myocardial blood supply[J]. Am J Cardiol, 2009, 104(3):318-326. [7] Feuchtner GM, Plank F, Pena C, et al. Evaluation of myocardial CT perfusion in patients presenting with acute chest pain to the emergency department:comparison with SPECT-myocardial perfusion imaging[J]. Heart, 2012, 98(20):1510-1517. doi: 10.1136/heartjnl-2012-302531 [8] Ko SM, Choi JW, Song MG, et al. Myocardial perfusion imaging using adenosine-induced stress dual-energy computed tomography of the heart:comparison with cardiac magnetic resonance imaging and conventional coronary angiography[J]. Eur Radiol, 2011, 21(1):26-35. [9] Wang R, Yu W, Wang Y, et al. Incremental value of dual-energy CT to coronary CT angiography for the detection of significant coronary stenosis:comparison with quantitative coronary angiography and single photon emission computed tomography[J]. Int J Cardiovasc Imaging, 2011, 27(5):647-656. doi: 10.1007/s10554-011-9881-7 [10] Kerl JM, Deseive S, Tandi C, et al. Dual energy CT for the assessment of reperfused chronic infarction-a feasibility study in a porcine model[J]. Acta Radiol, 2011, 52(8):834-839. doi: 10.1258/ar.2011.100315 [11] Peng J, Zhang LJ, Schoepf UJ, et al. Acute myocardial infarct detection with dual energy CT:correlation with single photon emission computed tomography myocardial scintigraphy in a canine model[J]. Acta Radiol, 2013, 54(3):259-266. doi: 10.1258/ar.2012.120104 [12] Kang DK, Schoepf UJ, Bastarrika G, et al. Dual-energy computed tomography for integrative imaging of coronary artery disease:principles and clinical applications[J]. Semin Ultrasound CT MR, 2010, 31(4):276-291. doi: 10.1053/j.sult.2010.05.004 [13] Cerqueira MD, Weissman NJ, Dilsizian V, et al. Standardized myocardial segmentation and nomenclature for tomographic imaging of the heart. A statement for healthcare professionals from the Cardiac Imaging Committee of the Council on Clinical Cardiology of the American Heart Association[J]. Circulation, 2002, 105(4):539-542. doi: 10.1161/hc0402.102975 [14] 彭晋, 张龙江, 周长圣, 等.单次对比增强双源CT双能量心脏成像的初步应用研究[J].国际医学放射学杂志, 2009, 32(4):313-316. doi: 10.3784/j.issn.1674-1897.2009.04.10401
[15] Austen WG, Edwards JE, Frye RL, et al. A reporting system on patients evaluated for coronary artery disease. Report of the Ad Hoc Committee for Grading of Coronary Artery Disease, Council on Cardiovascular Surgery, American Heart Association[J]. Circulation, 1975, 51(4 Suppl):S5-40. [16] Ghadri JR, Küest SM, Goetti R, et al. Image quality and radiation dose comparison of prospectively triggered low-dose CCTA:128-slice dual-source high-pitch spiral versus 64-slice single-source sequential acquisition[J]. Int J Cardiovasc Imaging, 2012, 28(5):1217-1225. doi: 10.1007/s10554-011-9921-3 [17] American Association of Physicists in Medicine(AAPM). The measurement, reporting and management of radiation dose in CT: report of AAPM Task Group 23 of the Diagnostic Imaging Council CT Committee[R]. AAPM One Physics Ellipse College Park, MD 20740-3846, report No. 96, 2008: 1-28. [18] Hoffmann U, Millea R, Enzweiler C, et al. Acute myocardial infarction:contrast-enhanced multi-detector row CT in a porcine model[J]. Radiology, 2004, 231(3):697-701. doi: 10.1148/radiol.2313030132 [19] Weininger M, Schoepf UJ, Ramachandra A, et al. Adenosine-stress dynamic real-time myocardial perfusion CT and adenosine-stress first-pass dual-energy myocardial perfusion CT for the assessment of acute chest pain:initial results[J]. Eur J Radiol, 2012, 81:3703-3710. doi: 10.1016/j.ejrad.2010.11.022 [20] Zhang LJ, Peng J, Wu SY, et al. Dual source dual-energy computed tomography of acute myocardial infarction:correlation with histopathologic findings in a canine model[J]. Invest Radiol, 2010, 45(6):290-297. doi: 10.1097/RLI.0b013e3181dfda60 [21] Ruzsics B, Lee H, Zwerner PL, et al. Dual-energy CT of the heart for diagnosing coronary artery stenosis and myocardial ischemia-initial experience[J]. Eur Radiol, 2008, 18(11):2414-2424. doi: 10.1007/s00330-008-1022-x [22] Koonce JD, Vliegenthart R, Schoepf UJ, et al. Accuracy of dual-energy computed tomography for the measurement of iodine concentration using cardiac CT protocols:validation in a phantom model[J]. Eur Radiol, 2014, 24(2):512-518 [23] 彭晋, 张龙江, 朱飞鹏, 等.双源CT心肌灌注碘成像与核素心肌灌注显像诊断犬急性心肌梗死的研究[J].中华放射学杂志, 2011, 45(2):128-132.
-

 点击查看大图
点击查看大图

计量
- 文章访问数: 2720
- HTML全文浏览量: 1588
- PDF下载量: 3