


-
甲状腺结节是颈部最常见的肿块性疾病之一,女性、老年人、碘缺乏地区及接受头颈部放射性治疗的群体患病率更高[1]。欧美国家普通人群中的甲状腺结节超声检出率为20%~70%[2-3],国内为18.6%,其中5%~15%为甲状腺癌[1, 4],且有增高趋势[5]。在甲状腺结节的诊断和治疗过程中,常因无法明确肿物的性质而使治疗处于两难境地。甲状腺癌起病隐匿且生物学特征多变,影像学、细胞学及临床特征与良性病变存在较多交叉,使现有的术前甲状腺结节良恶性的评价方法存在一定的误诊率。目前术前判断甲状腺结节的良恶性主要依靠甲状腺超声检查和细针穿刺细胞学(fine-needle aspiration cytology,FNAC)检查。其中常规超声(二维及多普勒超声)作为一种非侵入性检查方法,因其无创、简便易行、费用低廉等优点已被临床广泛应用,成为甲状腺结节性疾病的首选筛查方法。近年来,诸多文献显示甲状腺相关实验室检查指标,如血清甲状腺球蛋白(thyroglobulin,Tg)、抗甲状腺球蛋白抗体(antithyroglobulin antibody,TgAb)和TSH水平与甲状腺癌关系密切。本研究旨在分析分化型甲状腺癌和良性结节性甲状腺疾病中Tg、TgAb及TSH水平的分布规律及差异,并结合常规超声特征探讨其对甲状腺结节良、恶性病变的潜在预测价值。
-
回顾性分析山西医科大学第二医院普外科2012年9月至2014年9月间收治手术的甲状腺结节患者125例,同时排除小于18岁、有甲状腺手术史、甲状腺功能亢进或甲状腺功能减退及慢性淋巴细胞性甲状腺炎患者。其中女性101例、男性24例,年龄24~77岁,平均年龄49±11岁。甲状腺癌58例,其中乳头状癌54例、滤泡状癌1例、髓样癌1例、未分化癌1例、非霍奇金淋巴瘤1例,因未分化甲状腺癌(包括髓样癌和未分化癌)和非霍奇金淋巴瘤为非分化型甲状腺癌,未被包含在本研究数据中,在最终纳入分析的55例分化型甲状腺癌患者中,男性9例、女性46例;良性结节67例(男性15例、女性52例),其中结节性甲状腺肿40例、腺瘤27例。查阅因甲状腺结节而手术的患者的病历资料,调查内容包括:患者的姓名、年龄、性别、主诉、药物使用史、头颈部照射史、血清甲状腺指标检查结果、甲状腺超声检查结果、术后病理诊断结果及病理学类型等。
-
对所有患者进行血清甲状腺指标检测,包括血清游离甲状腺素(free thyroxine,FT4)、血清游离三碘甲状原氨酸(free three iodothyronine,FT3)、TSH、Tg和TgAb等。FT4、FT3、TSH及Tg为定量结果,采用化学发光法测定,测定仪器Access 2型全自动化学发光分析仪和配套测定试剂均由美国贝克曼公司生产。TgAb为定性结果,采用放射免疫分析法测定,试剂由天津协和医药公司生产。
术前一周内对所有患者均采用促凝试管抽取空腹静脉血3 ml,于当日按3500转/min标准低温离心10 min后取血清测试。测定各项甲状腺指标,试剂界定的正常参考值范围如下:FT3:3.8~6.0 pmol/L,FT4:7.9~14.4 pmol/L,TSH:0.34~5.0 mIU/L,Tg < 35 ng/ml,TgAb < 30%。各项指标均严格按照操作规程进行操作和测定。
-
采用PHILIPS公司的iu22型彩色多普勒超声诊断仪,探头频率7.5~10 MHz。受检者仰卧于检查床上,头部后仰以充分暴露颈前区,超声检查甲状腺左叶、右叶、峡部以及双侧颈部淋巴结。结果内容包括双叶甲状腺大小、位置,结节大小、数目,结节内部性质,如实性、囊性、囊实性、钙化等,结节内部及周边甲状腺组织血流情况等。
-
取手术切除后的甲状腺组织标本,经脱水、透明、石蜡包埋及切片处理后行苏木素染色,于光学显微镜下观察,根据WHO细胞病理学诊断标准诊断。本研究中所有患者术前均未行甲状腺FNAC检查。
-
用SPSS 22.0软件进行数据分析,由于血清Tg、TgAb及TSH水平不服从正态分布,经对数转换后仍为非正态资料,故各组计量资料用中位数±四分位数间距表示;良性组和恶性组间Tg、TSH的比较采用Wilcoxon秩和检验;采用多元Logistic回归分析法分析甲状腺癌与各变量(包括性别、年龄、Tg、TgAb、TSH、钙化、回声、结节性质、结节血流等)的相关性;良性组和恶性组Tg、TgAb阳性率的比较采用χ2检验;检验均为双侧,P < 0.05表示差异有统计学意义。
-
纳入分析的122例患者中,术前血清Tg阳性者55例(45.1%),阳性患者中24例合并甲状腺癌(19.67%);血清TSH升高者12例(9.8%),其中9例为甲状腺癌患者(7.4%)。甲状腺良恶性结节患者术前血清Tg和TSH水平测定结果见表 1。采用Wilcoxon秩和检验比较良性组和恶性组的Tg水平差异无统计学意义(Z=-1.292,P > 0.05),两组TSH水平的差异有统计学意义(Z=-2.107,P < 0.05)。
组别 例数 血清Tg(ng/ml) 血清TSH(mIU/L) 中位数 四分位数间距 中位数 四分位数间距 良性组 67 23.37 112.14 1.75 1.22 恶性组 55 24.09 64.59 2.32 2.28 表 1 甲状腺良恶性结节患者术前血清Tg和TSH水平测定结果
Table 1. Preoperative serum thyroglobulin and TSH level determination results in patients with benign and malignant thyroid nodules
-
甲状腺良恶性结节患者的术前血清Tg和TgAb的分布情况见表 2。采用χ2检验比较,得出甲状腺结节良性组与恶性组Tg的阳性率差异无统计学意义(χ2=0.085,P > 0.05);两组间TgAb的阳性率差异有统计学意义(χ2=4.545,P < 0.05);良性组和恶性组Tg联合TgAb[即Tg和(或TgAb)]的阳性率差异有统计学意义(χ2=3.975,P < 0.05)。良性甲状腺结节和甲状腺癌中Tg和TgAb同时增高的例数分别为3例和2例。
组别 例数 血清Tg 血清TgAb Tg联合TgAb 阳性 阴性 阳性 阴性 阳性 阴性 良性组 67 31 36 9 58 37 30 恶性组 55 24 31 18 37 40 15 表中,Tg:甲状腺球蛋白;TgAb:抗甲状腺球蛋白抗体;Tg联合TgAb阳性组为Tg阳性和(或)TgAb阳性,阴性组为Tg和TgAb均为阴性。 表 2 甲状腺良恶性结节患者的术前血清Tg和TgAb的阳性例数
Table 2. Positive cases of preoperative serum thyroglobulin and antithyroglobulin antibody in patients with benign and malignant thyroid nodules
-
对Tg、TgAb及TSH等血清指标与甲状腺癌的相关风险分别进行Logistic回归分析,结果示血清Tg抗体阳性、血清TSH升高是甲状腺癌的危险因素(表 3、图 1)。血清Tg水平与甲状腺癌的相关性不显著,考虑到TgAb对Tg的影响,将二者联合起来统计分析,得出Tg和TgAb阴性与甲状腺癌的风险呈负相关(表 3)。

图 1 不同 TSH 水平的甲状腺癌和甲状腺良性结节比例
Figure 1. The proportion of cases with thyroid cancer and benign thy-roid nodules in different TSH levels
变量 x2 P值 95%CI Tg 升高 - - 1 不高 0.065 0.799 1.097(0.537耀2.243) TgAb 阳性 - - 1 阴性 6.190 0.013▲ 0.319(0.130耀0.785) Tg联合TgAb 阳性 - - 1 阴性 4.130 0.042▲ 0.447(0.206耀0.972) TSH(mIU/L) >5.00 - - 1 < 0.34 0.494 0.482 0.333(0.016耀7.140) 0.34~2.49 5.447 0.020▲ 0.194(0.049耀0.769) 2.50~5.00 0.582 0.446 0.542(0.112耀2.619) 注:表中,Tg:甲状腺球蛋白;TgAb:抗甲状腺球蛋白抗体;95%CI:95%可信区间。▲表示差异具有统计学意义;“-”表示其以下的P值是与其所在行变量比较得出。 表 3 Tg、TgAb及TSH与甲状腺癌相关性的Logistic回归分析
Table 3. Logistic regression analysis of correlation between thyroid cancer and thyroglobulin, antithyroglobulin anti- body and TSH
-
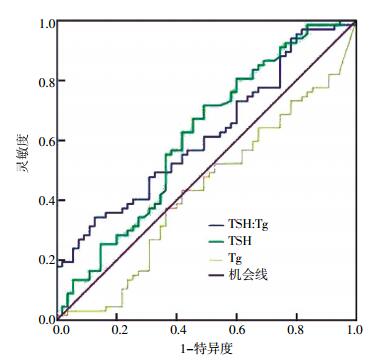
TSH的ROC显示曲线下面积(area under the curve,AUC)为0.611[95%可信区间(95%CI):0.509~0.713],P < 0.05。约登指数最大时,TSH取最佳临界值2.31 mIU/L,灵敏度和特异度分别为71.6%和50.9%;TSH : Tg的ROC显示AUC为0.617(95%CI:0.518~0.716),P < 0.05,最佳临界TSH : Tg值为0.11 IU/mg,灵敏度和特异度分别为61.2%和50.9%;Tg的ROC显示AUC < 0.5,故单独Tg因素对甲状腺癌的预测价值不太理想(图 2)。
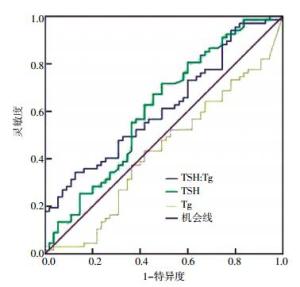
图 2 不同TSH水平的甲状腺癌和甲状腺良性结节比例
Figure 2. The proportion of cases with thyroid cancer and benign thy-roid nodules in different TSH levels
-
纳入分析的122例患者中,低回声型62例(50.8%),其中甲状腺癌44例(36.1%);等回声或高回声型60例(49.2%),其中甲状腺癌10例(8.2%);伴钙化者47例(38.5%),其中甲状腺癌37例(30.3%);囊性结节者6例,均为良性;实性结节者47例(38.5%),其中31例(25.4%)为甲状腺癌;囊实性69例(56.6%),其中24例(19.7%)为甲状腺癌;结节内部及周边无或仅见少量血流者60例(49.2%),其中29例(23.8%)为甲状腺癌;结节内部无或少量血流而周边可见丰富血流信号者28例(23.0%),其中4例(3.1%)为甲状腺癌;结节内部及周边均可见丰富血流信号者34例(27.9%),其中22例(18.0%)为甲状腺癌。
变量 x2 P值 95%CI 是否伴钙化 是 - - 1 否 30.264 0.085(0.036耀0.205) < 0.001▲ 0.085(0.036-0.205) 结节性质 囊实性 - - 1 实性 10.489 0.001▲ 3.633(1.664耀7.930) 结节血流 内有 - - 1 内周无 2.315 0.128 0.510(0.214耀1.214) 内无周有 13.675 < 0.001▲ 0.091(0.026耀0.324) 结节是否 是 - - 1 低回声 否 30.070 < 0.001▲ 0.092(0.039耀0.216) 注:表中,结节血流内有表示结节内部有丰富血流信号而结节周边有或无血流,内周无表示结节内部及周边均无明显血流信号,内无周有为结节内部无,周边有丰富血流信号;▲表示差异具有统计学意义;“-”表示其以下的χ2与P值是与其所在行变量比较得出。 表 4 甲状腺超声检查征象相关危险因素的Logistic回归分析
Table 4. Logistic regression analysis of related risk factors of thyroid cancer in ultrasound
-
甲状腺癌是最常见的颈部恶性肿瘤,近年来因FNAC检查技术的广泛应用,术前甲状腺癌的诊断率已明显提高。但由于其生物学的异质性、恶性程度不等、病理进展缓慢等因素,其发病隐匿,在一定程度上与良性结节较难区分。目前,FNAC检查技术是术前确诊甲状腺结节良恶性的重要技术和手段,确诊率可达80%,但仍有20%的可疑和漏诊率[6],且国内很多地区尚未能将该技术作为临床常规技术方法来广泛开展。早期发现甲状腺癌可避免中、高危甲状腺癌出现转移性病灶,但要尽量避免对微小甲状腺癌的过度诊断、过度治疗给患者带来的经济和心理方面的负担和压力。如何能在二者间寻找到一个平衡点已成为临床医师所面临的一道重要难题,尤其是良恶性甲状腺结节的鉴别诊断更为重要。再增加哪些甲状腺指标可有助于甲状腺结节的良恶性鉴别诊断?这为更多甲状腺指标,如Tg、TgAb、TSH等在甲状腺结节良恶性鉴别方面的应用提供了一定的探索空间。
Tg是甲状腺滤泡上皮分泌的糖蛋白,一般被认为是分化型甲状腺癌的肿瘤标志物[5],常用来进行术后血清Tg含量的监测,以判断疾病预后和评价治疗效果[7]。而在大量调查潜在临床因素预测术前甲状腺恶性结节的研究中显示,高血清Tg水平是预测甲状腺结节为恶性的重要临床特征[8],Tg水平是可在不确定性质的甲状腺结节细胞学诊断中区分甲状腺良性结节与分化型甲状腺癌的有用标记物[9]。近期,Rinaldi等[10]的一项大样本多中心研究显示,Tg升高是甲状腺癌的危险因素,多年持续存在的高Tg水平,尤其是进行性连续增高可能是甲状腺结节转化为恶性的重要指征。本研究中Tg与甲状腺癌的相关度未达到上述水平,可见一次性Tg检查对甲状腺癌的预测价值并不理想,可能与以下因素有关:①检测时间不同,Rinaldi等研究的是甲状腺组织未转变为甲状腺癌时的多年连续血清Tg水平,且对照组为正常群体。而本研究的研究对象为高度怀疑恶性的甲状腺结节患者,对照组为甲状腺良性结节患者,所测血清Tg均为其术前一周内的水平。通常良性甲状腺结节在逐渐转化为甲状腺癌时,随着甲状腺癌组织的快速生长,极易导致甲状腺组织细胞坏死,Tg透过甲状腺滤泡膜释放入血。因Tg在正常人体内的生物半衰期为8 d左右,若术前一段时间甲状腺癌的发展缓慢,甲状腺滤泡的持续性破坏已经停止,血清Tg经肝脏生理性灭活后其水平可逐渐降低至正常。②TgAb的影响,TgAb的滴度高低将直接影响血清Tg水平,当TgAb存在并异常增高时,可能导致血清Tg检测结果为阴性。③种群差异,甲状腺滤泡癌患者的血清Tg水平要高于甲状腺乳头状癌,而本研究中甲状腺滤泡癌占比仅为1.8%(1/55)。
本研究发现,甲状腺癌和甲状腺良性结节患者的Tg异常升高率、TgAb阳性率分别为43.6%(24/55)、46.3%(31/67)和32.7%(18/55)、13.4%(9/67),提示TgAb与甲状腺癌有一定的相关性。由于Tg和TgAb相互影响,可将两者联合起来比较良性组与恶性组的差异,甲状腺癌组的Tg升高和(或)TgAb阳性所占比例高达72.7%,与良性组有较大差异。Logistic回归分析再次证实Tg和(或)TgAb升高是甲状腺癌的危险因素。
多项研究发现,甲状腺癌患者的血清TSH水平均高于甲状腺良性结节患者[11-12],与本研究结果一致。图 1可见随着TSH水平的增高,甲状腺癌所占比例明显增大,但将该项指标用于甲状腺结节良恶性病变的鉴别诊断还有一定难度。图 2示TSH取最佳临界值2.31 mIU/L时,预测甲状腺癌的灵敏度和特异度分别为71.6%和50.9%;当TSH与Tg比值为0.11 IU/mg时约登指数最高,灵敏度和特异度分别为61.2%和50.9%,该临界值与王丽娜等[13]学者的研究结果(24.22 IU/g)不尽相同,可能是由于选择的研究群体不同所致,本研究中纳入的病例为高度怀疑甲状腺癌的甲状腺肿物,故TSH水平应较高,致使分析出的TSH : Tg界值也较高。本研究证实,超声检查发现甲状腺结节内出现的钙化灶、高血流信号或无血流以及低回声信号等特征与分化型甲状腺癌密切相关,但在结节无钙化、等高回声的情况下可适当参考血清Tg、TgAb及TSH : Tg等指标,在纳入本研究的55例甲状腺癌患者中,有7例并未见钙化及低回声等甲状腺癌的征象,而其中6例伴有血清Tg或TgAb升高,5例TSH : Tg > 0.11 IU/mg。上述结果表明,血清Tg升高和(或)TgAb阳性、TSH : Tg值>0.11 IU/mg时,将预示分化型甲状腺癌的发生几率明显增大,术前检测血清Tg、TgAb及TSH的意义不容忽视,可作为甲状腺超声检查的补充诊断手段。
Tg、TgAb及TSH在分化型甲状腺癌术前的预测分析
The prediction of risk of differentiated thyroid carcinoma with preoperative serum thyroid stimulating hormone, thyroglobulin and antithyroglobulin antibody
-
摘要:
目的 探讨患者术前血清促甲状腺激素、甲状腺球蛋白(Tg)、抗甲状腺球蛋白抗体(TgAb)浓度在预测甲状腺癌中的价值。 方法 对122例接受手术治疗的甲状腺结节患者进行术前研究,以术后病理结果作为甲状腺结节性质的诊断金标准进行对照,其中分化型甲状腺癌55例,良性结节67例。采用化学发光法测定Tg和TSH;放射免疫分析法测定TgAb;采用彩色多普勒超声诊断仪检查甲状腺组织和颈部淋巴结。 结果 甲状腺癌组的术前血清Tg水平(24.09±64.59)ng/ml和甲状腺良性结节组(23.37±112.14)ng/ml间的差异无统计学意义(Z=-1.092,P > 0.05);甲状腺癌组的TSH水平(2.32±2.28)mIU/L高于甲状腺良性结节组(1.75±1.22)mIU/L,(Z=-2.107,P < 0.05);甲状腺癌组Tg联合TgAb的阳性率(72.7%)高于甲状腺良性结节组(55.2%)(χ2=3.975,P < 0.05)。各指标预测甲状腺癌的受试者工作特征曲线示,TSH值的曲线下面积(AUC)为0.611[95%可信区间(95%CI):0.509~0.713],P < 0.05,最佳临界值2.31 mIU/L,灵敏度和特异度分别为71.6%和50.9%;TSH : Tg值的AUC为0.617(95%CI:0.518~0.716),P < 0.05,最佳临界TSH : Tg值为0.11 IU/mg,灵敏度和特异度分别为61.2%和50.9%;Tg曲线AUC < 0.5。 结论 术前血清Tg的异常升高不是甲状腺癌的独立预测因素,但其结合TgAb阳性、TSH:Tg值>0.11 IU/mg可作为甲状腺癌的危险预测因素,可能是甲状腺超声检查的一种有效补充诊断手段。 Abstract:Objective To explore the values of preoperative serum thyroid stimulating hormone, thyroglobulin and antithyroglobulin antibody in predicting the risk of differentiated thyroid carcinoma. Methods 122 patients with thyroid nodules who got operations were studied, among which 55 patients with differentiated thyroid carcinoma(54 papillary and 1 follicular), 67 cases with benign thyroid nodules(40 nodular goiter and 27 adenoma). Serum thyroid-stimulating hormone(TSH) and thyroglobulin(Tg)were measured by chemiluminescence method, and antithyroglobulin antibody(TgAb) by radioimmunoassay. Thyroid tissues and cervical lymph nodes were checked using color doppler ultrasonic diagnostic instrument and the postoperative pathological results was regard as the gold standard of diagnosing thyroid cancer. Results Preoperative serum Tg levels in thyroid cancer group(24.09±64.59)ng/ml and benign thyroid nodules group(23.37±112.14) ng/ml had no statistical differences(Z=1.092, P > 0.05). TSH levels in thyroid carcinoma group(2.32±2.28) mIU/L were higher than that in benign thyroid nodules group(1.75±1.22) mIU/L(Z=2.107, P < 0.05). The positive rate of Tg combined with TgAb in thyroid cancer group(72.7%) was higher than that in benign thyroid nodules group(55.2%)(χ2= 3.975, P < 0.05). Receiver operating characteristic(ROC) curves showing sensitivity as a function of specificity were calculated for TSH, Tg levels and TSH : Tg values to evaluate the potential accuracy of the three index as predicting differentiated thyroid carcinoma. The area under the curve(AUC) of TSH was 0.611[95% confidence interval(95% CI):0.509~0.713], P < 0.05. The optimum threshold in ROC curves of TSH was 2.31 mIU/L. The sensitivity and specificity of TSH were 71.6% and 50.9% respectively. The AUC of TSH : Tg values was 0.617(95% CI:0.518~0.716), P < 0.05. The best critical value of TSH : Tg was 0.11 IU/mg. The sensitivity and specificity of TSH : Tg were 61.2% and 50.9% respectively. The AUC of Tg was less than 0.5. Conclusion Serum thyroglobulin elevated abnormally is not an independent predicting factor of differentiated thyroid cancer. The elevated Tg levels and/or positive TgAb and TSH : Tg > 0.11 IU/mg can be used as effective supplementary means of ultrasound examination in predicting differentiated thyroid carcinoma. -
图 1 不同 TSH 水平的甲状腺癌和甲状腺良性结节比例
Figure 1. The proportion of cases with thyroid cancer and benign thy-roid nodules in different TSH levels
图 2 不同TSH水平的甲状腺癌和甲状腺良性结节比例
Figure 2. The proportion of cases with thyroid cancer and benign thy-roid nodules in different TSH levels
表 1 甲状腺良恶性结节患者术前血清Tg和TSH水平测定结果
Table 1. Preoperative serum thyroglobulin and TSH level determination results in patients with benign and malignant thyroid nodules
组别 例数 血清Tg(ng/ml) 血清TSH(mIU/L) 中位数 四分位数间距 中位数 四分位数间距 良性组 67 23.37 112.14 1.75 1.22 恶性组 55 24.09 64.59 2.32 2.28  下载: 导出CSV
下载: 导出CSV
表 2 甲状腺良恶性结节患者的术前血清Tg和TgAb的阳性例数
Table 2. Positive cases of preoperative serum thyroglobulin and antithyroglobulin antibody in patients with benign and malignant thyroid nodules
组别 例数 血清Tg 血清TgAb Tg联合TgAb 阳性 阴性 阳性 阴性 阳性 阴性 良性组 67 31 36 9 58 37 30 恶性组 55 24 31 18 37 40 15 表中,Tg:甲状腺球蛋白;TgAb:抗甲状腺球蛋白抗体;Tg联合TgAb阳性组为Tg阳性和(或)TgAb阳性,阴性组为Tg和TgAb均为阴性。
下载: 导出CSV
表 3 Tg、TgAb及TSH与甲状腺癌相关性的Logistic回归分析
Table 3. Logistic regression analysis of correlation between thyroid cancer and thyroglobulin, antithyroglobulin anti- body and TSH
变量 x2 P值 95%CI Tg 升高 - - 1 不高 0.065 0.799 1.097(0.537耀2.243) TgAb 阳性 - - 1 阴性 6.190 0.013▲ 0.319(0.130耀0.785) Tg联合TgAb 阳性 - - 1 阴性 4.130 0.042▲ 0.447(0.206耀0.972) TSH(mIU/L) >5.00 - - 1 < 0.34 0.494 0.482 0.333(0.016耀7.140) 0.34~2.49 5.447 0.020▲ 0.194(0.049耀0.769) 2.50~5.00 0.582 0.446 0.542(0.112耀2.619) 注:表中,Tg:甲状腺球蛋白;TgAb:抗甲状腺球蛋白抗体;95%CI:95%可信区间。▲表示差异具有统计学意义;“-”表示其以下的P值是与其所在行变量比较得出。
下载: 导出CSV
表 4 甲状腺超声检查征象相关危险因素的Logistic回归分析
Table 4. Logistic regression analysis of related risk factors of thyroid cancer in ultrasound
变量 x2 P值 95%CI 是否伴钙化 是 - - 1 否 30.264 0.085(0.036耀0.205) < 0.001▲ 0.085(0.036-0.205) 结节性质 囊实性 - - 1 实性 10.489 0.001▲ 3.633(1.664耀7.930) 结节血流 内有 - - 1 内周无 2.315 0.128 0.510(0.214耀1.214) 内无周有 13.675 < 0.001▲ 0.091(0.026耀0.324) 结节是否 是 - - 1 低回声 否 30.070 < 0.001▲ 0.092(0.039耀0.216) 注:表中,结节血流内有表示结节内部有丰富血流信号而结节周边有或无血流,内周无表示结节内部及周边均无明显血流信号,内无周有为结节内部无,周边有丰富血流信号;▲表示差异具有统计学意义;“-”表示其以下的χ2与P值是与其所在行变量比较得出。
下载: 导出CSV
-
[1] Cooper DS, Doberly GM, Haugen BR, et al. Revised American thy-roid association management guidelines for patients with thyroid cancer:the American thyroid associationATA guidelines taskforce on thyroid nodules and differentiated thyroid cancer[J]. Thyroid, 2009, 1911:1167-1214. [2] Gharib H, Papini E, Paschke R, et al. American association of clinical endocrinologists, associazione medici endocrinologi, and European thyroid association medical guidelines for clinical practice for the diagnosis and management of thyroid nodules:executive summary of recommendations[J]. Endocr Pract, 2010, 163:468-475. [3] Hegedüs L. Thyroid ultrasound[J]. Endocrinol Metab Clin North Am, 2001, 302:339-360, viii-ix. [4] Schlumberger MJ, Torlantano M. Papillary and follicular thyroid carcinoma[J]. Best Pract Res Clin Endocrinol Metab, 2000, 144:601-613. [5] Jung KW, Park S, Kong HJ, et al. Cancer statistics in Korea:incidence, mortality and survival in 2006-2007[J]. J Korean Med Sci, 2010, 258:1113-1121. [6] Crowther A, Giles K, Archer L. Thyroid FNAC inadequacy rates[J]. Clin Radiol, 2014, 69 Suppl 1:S12. [7] Nascimento C, Borget I, Troalen F, et al. Ultrasensitive serum thyroglobulin measurement is useful for the follow-up of patients treated with total thyroidectomy without radioactive Iodine ablation[J]. Eur J Endocrinol, 2013, 1695:689-693. [8] Hrafnkelsson J, Tulinius H, Kjeld M, et al. Serum thyroglobulin as a risk factor for thyroid carcinoma[J]. Acta OncolMadr, 2000, 398:973-977. [9] Lee EK, Chung KW, Min HS, et al. Preoperative serum thyroglobulin as a useful predictive marker to differentiate follicular thyroid cancer from benign nodules in indeterminate nodules[J]. J Korean Med Sci, 2012, 279:1014-1018. [10] Rinaldi S, Plummer M, Biessy C, et al. Thyroid-stimulating hormone, thyroglobulin, and thyroid hormones and risk of differentiated thyroid carcinoma: the EPIC study[J/OL]. J Natl Cancer Inst, 2014, 1066: dju097[2014-11-30].http://jnci. oxfordjournals. org/content/106/6/dju097. full. pdf+html. [11] Haymart MR, Glinberg SL, Liu J, et al. Higher serum TSH in thyroid cancer patients occurs Independent of age and correlates with extrathyroidal extension[J]. Clin EndocrinolOxf, 2009, 713:434-439. [12] 官青, 张凌, 魏文俊, 等.术前血清TSH与TGAB对于分化型甲状腺癌的预测价值[C]//2011国际暨全国第十一届头颈肿瘤学术大会论文汇编.杭州: 中国抗癌协会头颈肿瘤专业委员会, 2011: 361-362.
[13] 王丽娜, 杨中元, 李浩, 等.术前血清促甲状腺素与甲状腺球蛋白的比值是甲状腺结节的有效诊断方法[C]//2014第六届全国甲状腺肿瘤学术大会论文集.天津: 中国抗癌协会甲状腺癌专业委员会, 2014: 320-320.
-

 点击查看大图
点击查看大图

计量
- 文章访问数: 2868
- HTML全文浏览量: 1658
- PDF下载量: 3