


 下载:
下载:
-
排粪造影于1953年由Wallden等[1]首次报道,近年来随着人们对肛肠疾病的关注,其逐渐成为国内外学者研究的热点。直肠黏膜脱垂作为一种常见疾病,也是导致出口梗阻型便秘的重要原因之一。国外学者根据直肠黏膜脱垂的范围和是否累及肠壁,将直肠黏膜脱垂分为黏膜脱垂、肠套叠和脱肛[2]。黏膜脱垂是指直肠黏膜脱入肛管,但是肠壁不受累;肠套叠类似小肠套叠,是指黏膜脱垂累及肠壁,形成了类似小肠套叠的影像;脱肛是指直肠黏膜脱出肛门外。就直肠黏膜脱垂而言,Shorvon等[3]将其分为7级;国内卢任华[4]将其分为3级,分别为直肠前壁黏膜脱垂、直肠内套叠和直肠外脱垂,何宪国等[5]的分级与其相似。然而,张胜本等[6]研究认为,排粪造影不能准确区分直肠套叠是否累及全层肠壁,可能影响直肠黏膜脱垂的分级。国内外学者均有将CT及MRI技术引入排粪造影的报道,虽然CT与MRI能够很好的显示直肠周围组织,但是不能动态观察,而且需患者良好的配合。由于检查价格昂贵,且患者也不便真正行排便动作而未能得以推广应用,使得传统X线排粪造影仍然是一种经济、有效的检查。为了给临床诊断和治疗提供更为准确的X线影像学指导,本研究收集整理了本院2012年6月至2014年3月共38例诊断为直肠黏膜脱垂病例的X线影像资料,依据直肠黏膜脱垂的解剖部位以及临床治疗方法的差异,对直肠黏膜脱垂进行细化分级,现报道如下。
-
收集整理本院2012年6月至2014年3月的38例诊断为直肠黏膜脱垂病例的X线影像资料,其中男性患者13例,女性患者25例,患者年龄28~76岁,平均年龄45岁。女性患者中有19例为生育后女性,其中,16例经阴道分娩,13例为多胎妊娠。38例患者多因排便困难或排便不适就诊于本院普外科门诊,其中24例患者需经常使用开塞露等促进排便的润滑药物才能顺利排便。
-
Ikenberry等[7]认为,使用不掺入淀粉的低黏度造影剂也能达到排粪造影诊断的要求,我们将400 g硫酸钡Ⅱ型干混悬剂溶解于400 ml温水中,制成排粪造影用造影剂,水温控制在30~37 ℃,避免温度过高或过低刺激患者排便。
-
患者于检查前一天口服泻药(20%甘露醇500 ml兑等体积温水冲服)清洁肠道,次日行钡灌肠,透视下观察,直至患者乙状结肠充盈造影剂,灌肠结束后嘱患者侧坐于自制木质便桶上,调整胃肠机的摄影条件以便获得较佳的观测结果,调整患者的坐姿,尽最大可能使患者双侧股骨重叠,参照Mahieu等[8-9]的方法于透视下嘱患者静坐、提肛、强忍、力排,并适时点片,在大便排泄干净后加摄黏膜像片。
-
Faccioli等[10]和Yang等[11]通过排粪造影X线影像将直肠黏膜脱垂分为3级,第1级是直肠黏膜脱入远端直肠,力排时X线影像表现为远端直肠壁内的类圆形充盈缺损;第2级是直肠黏膜脱入肛管,在力排时X线影像表现为肛管内的类圆形充盈缺损;第3级是直肠黏膜脱出肛管,在患者力排时可见到直肠黏膜脱出肛门。
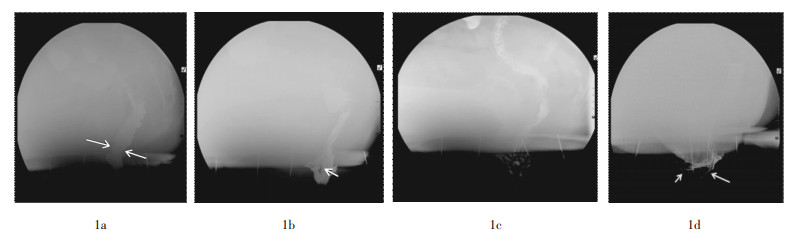
除上述第1、3级外,本研究将第2级细分为2a与2b两个亚级,当力排时X线影像表现为与小肠套叠类似的“W”征时,可确定肠套叠存在。如图 1所示,2a级是直肠黏膜脱入肛管,X线排粪造影表现为肛管内的类圆形充盈缺损,但无明确“W”征;2b级是影像上出现明确“W”征,即伴肠套叠存在。国内学者也将“W”征称为漏斗形杵臼征象或者倒伞征[12]。

图 1 直肠黏膜脱垂患者的排粪造影X线影像图图中,1a为1级黏膜脱垂,充盈像直肠远端可见局限性的小充盈缺损(箭头);1b为2a级黏膜脱垂,黏膜像观察到较明显的充盈缺损(箭头);1c为2b级黏膜脱垂,即伴有肠套叠,黏膜像可较清楚地观察到“W”征(曲线);1d为3级黏膜脱垂,黏膜像可见直肠黏膜脱出肛门(箭头)。
Figure 1. Defecography images of patients diagnosed rectal prolapse
-
① 直肠前突,是指直肠前壁向前方呈囊袋样突出,按照何宪国等[5]方法目测进行诊断,没有测量具体数值;②盆底下降,由于盆底肌肉韧带等支持结构的松弛,患者力排时直肠肛管下降幅度过大,按照卢任华等[4]方法测量直肠肛管连接部距耻尾线(耻骨联合上缘与尾骨尖的连线)的距离,该距离大于3 cm时诊断为盆底下降;③乙状结肠疝,是指乙状结肠在排便时下降至盆腔,压迫直肠导致排便困难,按照何宪国等[5]方法目测进行诊断。
-
Choi等[13]认为不同医师对X线排粪造影直肠黏膜脱垂的诊断存在差异。因此,本研究采用了3名不同级别医师(初级、中级及高级职称各1名)共同阅片的方法,最终采用经集体讨论取得一致的意见作为诊断结果。
-
本研究38例病例,其中诊断为1级直肠黏膜脱垂患者8例;2级27例(其中2a级15例,2b级12例);3级3例。除了单发直肠黏膜脱垂病例,直肠黏膜脱垂合并直肠前突患者为18例,合并盆底下降患者为4例,合并乙状结肠疝患者为1例,同时合并直肠前突及盆底下降患者为2例。
-
排粪造影是一种经济、有效的检查直肠和盆底功能的动态实时检查方法,已得到了国内外学者的广泛认可[2]。直肠黏膜脱垂是一种常见的排粪造影X线征象,但国内外学者采用的诊断方法不尽相同,对其临床意义的理解也有争议。目前主要集中于脱垂黏膜形成肠套叠的级别划归问题。Shorvon等[3]根据直肠脱垂时折叠肠管的厚度是否超过3 mm,是否累及整个直肠壁(后壁或环周),以及脱垂的直肠黏膜所到达的部位(远端直肠、肛管及肛门外),将直肠黏膜脱垂分为7级,分级较为详细,但未明确肠套叠所属分级。Baek等[14]将直肠远端与肛管上端呈“漏斗状”表现诊断为直肠套叠,但未考虑单纯黏膜脱垂的情况。Savoye-Collet等[15]采用的标准为直肠全周脱入远端直肠、肛管或者肛门外,亦未考虑黏膜脱垂是否累及肠壁。Maglinte等[2]将直肠黏膜脱垂分为直肠-直肠黏膜脱垂、直肠-肛管黏膜脱垂和直肠黏膜脱垂肛门外3种,认为侧位片上出现反“3”字征可确定肠套叠存在,据笔者观察“W”征比反“3”征更形象、更准确,因而本文称其为“W”征,但其分级划归仍不明确。卢任华[4]将直肠黏膜脱垂分为直肠前壁黏膜脱垂、直肠内套叠和直肠外脱垂,而未考虑到直肠黏膜脱垂累及直肠后壁的情况。此外,从临床治疗的角度来看,张胜本等[6]认为直肠黏膜脱垂、肠套叠和直肠外脱垂的治疗方法不同。
综合分析,笔者认为有必要将直肠黏膜脱垂的程度进行细化分级。在认同Faccioli等[10]和Yang等[11]第1、3级的分级情况下,本研究依据直肠黏膜脱垂的解剖部位以及临床治疗方法的差异,主要将第2级细分为2a和2b级(具体分级标准见本文1.3所述)。因此,本研究明确了直肠黏膜脱垂X线排粪造影影像中肠套叠的征象判断和分级归属问题,可能有助于临床治疗方案的设计。
综上所述,X线排粪造影是一种评价患者直肠功能的经济、有效手段。而直肠黏膜脱垂作为一种较为常见的疾病,目前仍缺乏统一的影像学诊断标准,其诊断方式和结果的临床意义均存在争议,不利于其临床治疗效能的提升。而本研究分级方法的临床意义也有待于进一步的大样本临床检验。
直肠黏膜脱垂患者排粪造影的X线表现分级研究
Defecography in patients with prolapse of rectal mucosa lesions: degrees of imaging findings
-
摘要:
目的 探讨X线排粪造影在诊断直肠黏膜脱垂病变中的影像学分级方法。 方法 对38例通过X线排粪造影诊断为直肠黏膜脱垂的病例进行影像表现分析,并参考国内外学者的文献进行细化分级。 结果 按照笔者研究的分级方法,38例直肠黏膜脱垂病例X线排粪造影诊断为1级的8例;2级27例,其中2a级15例,2b级12例;3级3例。部分患者同时合并直肠前突等其他征象。 结论 直肠黏膜脱垂病变X线排粪造影的细化分级,可能有助于临床治疗方案的设计。 Abstract:Objective To investigate the classification method of imaging using X-ray defecography in the diagnosis of the prolapse of rectal mucusa. Methods 38 patients(25 females, 13 males; mean age 45 years)who were diagnosed as rectal prolapse by conventional defecography were collected and analyzed. Imagining findings were divided into different degrees according to the domestic and international scholar articles. Results The rectocele imaging findings were divided into three degrees according to the clinical classification. First degree were diagnosed in 8 cases, second degree in 27 cases(2a degree 15 cases, 2b degree 12 cases), third degree in 3 cases. Some patients were complicated with rectocele and other signs. Conclusion Detailed classification of prolapse of rectal mucosa lesions by X-ray defecography may contribute to the designs of clinical treatment. -
Key words:
- Defecography /
- Prolapse of rectal mucosa /
- X-ray
-
[1] Wallden L. Roentgen examination of the deep rectogenital pouch[J]. Acta Radiol, 1953, 39(2): 105-116. [2] Maglinte DD, Bartram CI, Hale DA, et al. Functional imaging of the pelvic floor[J]. Radiology, 2011, 258(1): 23-39. [3] Shorvon PJ, McHugh S, Diamant NE, et al. Defecography in normal volunteers: results and implications[J]. Gut, 1989, 30(12): 1737-1749. doi: 10.1136/gut.30.12.1737 [4] 卢任华.排粪造影在肛肠外科的应用[J].中国实用外科杂志, 2012, 22(12): 708-709.
[5] 何宪国, 樊新云, 刘向东.排粪造影在出口梗阻型便秘中的X线测量与诊断[J].中国临床医学影像杂志, 2011, 22(3): 181-183. doi: 10.3969/j.issn.1008-1062.2011.03.010
[6] 张胜本, 张连阳, 龚水根, 等.直肠内脱垂盆底形态研究及临床意义[J].中华放射学杂志, 1996, 30(4): 253-256. doi: 10.3760/j.issn:1005-1201.1996.04.010
[7] Ikenberry S, Lappas JC, Hana MP, et al. Defecography in healthy subjects: comparison of three contrast media[J]. Radiology, 1996, 201(1): 233-238. doi: 10.1148/radiology.201.1.8816549 [8] Mahieu PH, Pringot J, Bodart P. Defecography: Ⅰ. Description of a new procedure and results in normal patients[J]. Gastrointest Radiol, 1984, 9(3): 247-251. [9] Mahieu PH, Pringot J, Bodart P. Defecography: Ⅱ. Contribution to the diagnosis of defecation disorders[J]. Gastrointest Radiol, 1984, 9(3): 253-261. [10] Faccioli N, Comai A, Paride Mainardi, et al. Defecography: a practical approach[J]. Diagn Interv Radiol, 2010, 16(3): 209-216. [11] Yang XM, Partanen K, Farin P, et al. Defecography[J]. Acta Radiol, 1995, 36(5): 460-468. doi: 10.3109/02841859509173409 [12] 吴有泉, 白宝忠, 李东冰.直肠内脱垂套叠的排粪造影诊断[J].中国医学影像技术, 1997, 13(1): 77-78.
[13] Choi JS, Wexner SD, Nam YS, et al. Intraobserver and interobserver measurements of the anorectal angle and perineal descent in defecography[J]. Dis Colon Rectum, 2000, 43(8): 1121-1126. doi: 10.1007/BF02236560 [14] Baek HN, Hwang YH, Jung YH. Clinical Significance of Perineal Descent in Pelvic Outlet Obstruction Diagnosed by using Defeco-graphy[J]. J Korean Soc Coloproctol, 2010, 26(6): 395-401. [15] Savoye-Collet C, Savoye G, Koning E, et al. Defecography in sym-ptomatic older women living at home[J]. Age Ageing, 2003, 32(3): 347-350. doi: 10.1093/ageing/32.3.347 -

 点击查看大图
点击查看大图
图(1)
计量
- 文章访问数: 3999
- HTML全文浏览量: 3221
- PDF下载量: 5