


 下载:
下载:
-
外科手术已成为药物难治性癫痫的有效治疗手段,将致痫灶切除是最有效的控制和治愈癫痫的方法,而术前精确定位致痫灶则是手术成功的关键[1-3],癫痫手术术式的选择也与癫痫灶定位密切相关。致痫灶的定位是一项复杂的工作,应采用综合性诊断程序[4]。虽然目前癫痫定位的检查方法众多,但定位诊断的一致性却较低。因此,探寻经济、吻合率高的检查方法的组合,提高术前定位致病灶的准确率,是目前亟待解决的问题,也是国内外研究的热点。本研究拟探索癫痫发作期SPECT脑血流灌注显像和视频脑电图(video-electroencephalography,VEEG)在癫痫灶定位中的一致性,阐明二者联合定位是否可为癫痫外科治疗提供手术依据。
-
选取于2009年1月至2012年12月在我院神经内科门诊、临床初次确诊且VEEG监测异常的癫痫患者45例,其中男性29例、女性16例,年龄14~53岁。其中单纯部分性发作4例,部分性发作继发全面性强直-阵挛发作9例,复杂部分性发作18例,全面性强直-阵挛发作14例。发作类型依据1981年国际抗癫痫联盟分类和命名委员会修改方案诊断标准分类[5]。
-
所有患者检查前均剥夺睡眠24 h,在VEEG描记仪(美国CARDWELL公司生产的32导长程视频脑电图描记仪)监测下等待注射显像剂锝-双半胱乙酯(Technetium-99m ethyl cysteinate dimmer,99Tcm-ECD)的时机。对于久等(一般为1 h)未见临床发作或VEEG未出现典型癫痫波的患者,经患者及家属知情同意,给予口服可乐定[6-7]以诱发癫痫。所用可乐定由常州制药厂有限公司生产,75 μg/片,剂量根据体重划分:体重<60 kg者服用150 μg、60~80 kg者服用225 μg、体重>80 kg者服用300 μg。然后建立静脉通道,进行VEEG采集及录像,将标记好的99Tcm-ECD放置于铅罐内备用。99TcmO4-由北京原子高科股份有限公司提供,ECD由江苏原子医学研究所江原制药厂提供(取本品1瓶,临用前在无菌操作条件下,根据高锝酸钠注射液的放射性浓度,取2~5 ml注入瓶内,充分震荡,使冻干粉溶解,静置15 min,即得到99Tcm-ECD注射液)。当患者出现临床发作和(或)脑电图出现典型癫痫波时,30 s内通过预先建立的静脉通道注入99Tcm-ECD,并用生理盐水冲洗管道,确保药物全部注入。注射完毕后,患者平卧休息,30 min后进行脑血流灌注断层显像。所有患者或家属均于检查前签署了知情同意书。
-
在无噪声、较暗的室内行SPECT时,受检者眼、耳均封闭。显像仪器为Siemens E-CAM型SPECT仪,配平行孔低能高分辨率准直器。矩阵128×128,步进6°,旋转360°,采集60帧,每帧25 s,截止频率为0.35~0.40。原始图像经计算机处理重建为横断面(以眦耳线为轴线)、冠状面和矢状面图像。
-
视觉阅片法:由2位有经验的医师共同读片。以横断面为基础,参照冠状面与矢状面,以2个以上的断面出现肉眼可辨的放射性异常区为阳性病灶。半定量分析法:采用镜像比值法(Ra),Ra=正常区计数/病灶区计数,发作间期Ra≥1.1视为异常,发作期Ra≤0.9视为异常[7]。
-
用SPSS 19.0软件对部分性发作和全面性-强直阵挛发作患者发作期SPECT和VEEG定位的一致性进行卡方检验,P<0.05表示差异有统计学意义。
-
在VEEG监测出现典型癫痫波的45例癫痫患者中,6例为剥夺睡眠诱发(均为亚临床发作),其余39例同时给予口服可乐定以诱发(其中临床发作3例,亚临床发作36例)。
VEEG表现为局灶性异常放电者占所有患者的68.9%(31/45),各导联同步对称性异常放电者占31.1%(14/45)。发作期SPECT定位阳性率为93.3%(42/45),均表现为高血流灌注灶,其中40例(95.2%)表现为单叶局限性高灌注,2例(4.8%)表现为多个病灶高灌注,剩余3例正常。
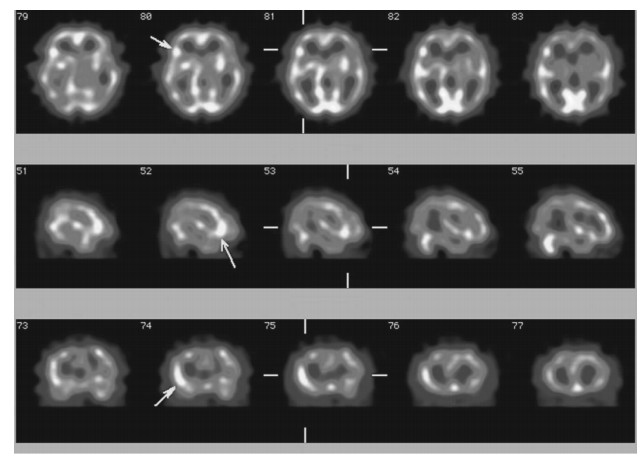
比较二者定位结果发现,对于部分性发作患者(图 1)而言,VEEG与发作期SPECT的定位关系有3种:①完全不在同一脑叶者占9.7%(3/31);②致痫灶位置对称性相反者占6.4%(2/31);③定位完全相同者占83.9%(26/31)。全面性-强直阵挛发作患者(14例)VEEG均表现为各导联异常放电,而SPECT脑血流灌注显像表现为孤立高血流灌注灶,其中6例同时伴有病灶同侧或对侧基底节区核团高灌注。故对于全面性-强直阵挛发作患者,VEEG与SPECT定位无一致性。

图 1 复杂部分性发作癫痫患者脑血流灌注显像。患者男性,19岁,发作类型为复杂部分性发作,2次/年,口服可乐定1 h后视频脑电图表现为右侧额叶高幅的棘慢综合波爆发,此图像为出现上述异常波8 s时注入显像剂所获脑血流灌注显像,箭头所示为右侧额叶血流灌注增高。Ra=0.75<0.9。此患者MRI检查为阴性。
Figure 1. Ictal brain SPECT of patients with complex partial epilepsy
部分性发作和全面性-强直阵挛发作患者VEEG和SPECT定位一致性之间的差异有统计学意义(χ2=24.478,P<0.05)。
-
近年来尽管药物治疗癫痫有了很大的进展,但仍有20%~30%的药物难治性癫痫需要手术治疗[8-9]。癫痫手术成功的关键是术前对癫痫灶的精确定位[1-3]。但因药物难治性癫痫的病因及发病机制极其复杂,目前尚无法仅凭一种检查方法即对致痫灶做出准确定位。癫痫定位检查方法众多,故探寻经济、吻合率高的检查方法的组合以清晰准确定位致痫灶,并尽量减少侵入性的检查是目前亟待解决的难题。
癫痫本质上是一种异常的电活动,所以,尽管目前各种反映脑功能的影像学检查方法不断兴起,癫痫的定性诊断与定位诊断依然主要依靠脑电图。VEEG是捕获癫痫样放电的最佳方法,它不仅可记录到患者发作时的临床表现,而且可记录到典型的癫痫发作的起始区,对定位致痫灶意义重大[10],且可协助癫痫分型诊断。在VEEG监测中,为了提高诊断的阳性率,临床常用的诱发方法为剥夺睡眠,但其阳性率较低(33.9%)[11]。因癫痫发作具有不可预测性,故本研究对于久等(一般为1 h)未见VEEG异常的患者同时给予口服可乐定以诱发癫痫,既提高了VEEG诊断的阳性率,也为获得发作期SPECT脑血流灌注显像提供了注射显像剂的时机,避免了延迟注入显像剂的弊端。
在VEEG监测中出现典型癫痫波的45例癫痫患者中,68.9%(31/45)表现为局灶性异常放电,均为部分性发作患者;31.1%(14/45)表现为各导联异常放电,均为全面性-强直阵挛发作患者。VEEG可协助癫痫患者分类诊断,9例最初划分为全面性强直-阵挛发作的患者VEEG均表现为局灶性异常放电,进一步询问病史亦支持发作类型为部分性发作继发全面性强直-阵挛发作。故部分性发作继发全面性强直-阵挛发作与全面性强直-阵挛发作患者要根据临床表现和脑电图检查仔细区分,充分发挥脑电图在癫痫分型中的重要性作用,以便准确指导治疗。
SPECT是广泛用于临床的功能影像技术。癫痫发作时由于脑血流量的增加和代谢的增强,会在癫痫灶处出现放射性核素的聚集,而发作间期则出现脑血流量的减少和代谢的减弱,使得癫痫灶处的放射性核素的分布明显减少。发作间期SPECT脑显像因容易实施,已作为常规显像方法在临床开展,但其灵敏度和特异度均低于发作期显像,其只能作为基线辅助诊断发作期病灶以排除泛化病灶[12]。发作期SPECT的术前评估价值已普遍得到临床证实,尤其是对MRI检查阴性的患者[1, 13-16]。目前国内外学者一致认为,获得真正发作期SPECT脑显像的方法是在癫痫患者出现临床发作和(或)脑电图出现典型癫痫波时的30 s内注入显像剂[17-20],为了准确把握注入显像剂的时机,本研究根据情况在剥夺睡眠的基础上给予了可乐定药物诱发,从而有目的性地把握注射显像剂的时机,避免了常规获得发作期SPECT显像而长时间等待耗时、费力的不足。本研究发作期SPECT定位阳性率为93.3%(42/45),均表现为高血流灌注灶,其中40例(95.2%)表现为单叶局限性高灌注,2例(4.8%)表现为多个病灶高灌注,且均为部分性发作患者。14例全面性-强直阵挛发作患者SPECT脑血流灌注显像表现为孤立高血流灌注灶,其中6例同时伴有病灶同侧或对侧基底节区核团高灌注。通常认为基底节区高灌注不是致痫灶,而是致痫灶泛化的结果。
比较二者定位结果发现:部分性发作患者VEEG与SPECT的定位关系有3种情况:①完全不在同一脑叶者占9.7%(3/31);②病灶位置对称性相反者占6.4%(2/31);③定位完全相同者占83.9%(26/31)。对其中1例病灶位置对称性相反的患者(VEEG提示右侧额叶癫痫波,发作期SPECT图像示左侧额叶高灌注灶)次日行发作间期SPECT检查拟进一步确定癫痫灶,但因发作间期SPECT检查为阴性,故无法判断VEEG和发作期SPECT所示癫痫灶哪个更为可靠,因条件受限,未进一步评估。因此,对部分性发作二者定位不一致的患者应行进一步评估,而不能盲目地倾向于哪种检查。而二者定位一致的病灶则应该为癫痫灶,国外也有二者定位指导手术治疗取得理想疗效的报道[21]。全面性-强直阵挛发作患者VEEG均表现为各导联对称性异常放电,这与Hamandi等[22]报道的“泛发性棘波活动(generalized spike wave)是全身性癫痫脑电图的标志”一致。发作期SPECT脑血流灌注显像表现为孤立高血流灌注灶,故对于全面性-强直阵挛发作患者VEEG与发作期SPECT定位无一致性,需借助于其他检查进一步评估。对于无创检查无法确定癫痫灶的患者,有创检查是必须的[23]。
本研究证实部分性发作患者发作期SPECT与VEEG定位有较高的吻合率(83.9%),认为二者定位一致性的病灶即为癫痫灶,可指导手术治疗[21]。但SPECT毕竟属于功能学检查,空间分辨率较低,对于有条件的医院,若能将发作期SPECT/CT与VEEG联合则会达到更加精确定位的目的,这也是本研究的不足之一;再者,由于本研究对象均为初诊的癫痫患者,不符合癫痫手术指征,故对于定位一致的患者未能通过手术证实该定位模式的优越性。但有一点是肯定的,癫痫灶定位的一致性是实施手术的前提,这也是本研究的最终目的和要解决的关键问题。
总之,本研究联合发作期SPECT与VEEG两种相对经济的检查组合,提示对于部分性发作患者,二者联合可对83.9%的患者达到一致性定位的目的,但其远期疗效有待于进一步研究证实,而对于全面性-强直阵挛发作患者二者定位无一致性,需进一步评估。
发作期SPECT脑血流灌注显像和VEEG在癫痫灶定位诊断中的一致性
The consistency of ictal SPECT and VEEG studies in localizing the epileptic focus
-
摘要:
目的 探讨癫痫发作期SPECT脑血流灌注显像和视频脑电图(VEEG)在致痫灶定位中的一致性。 方法 选择VEEG监测异常的癫痫患者45例,当患者出现临床发作和(或)脑电图出现典型癫痫波时30 s内注入锝-双半胱乙酯(99Tcm-ECD),30 min后行脑血流灌注断层显像。比较癫痫发作期SPECT脑血流灌注显像和VEEG在癫痫定位诊断中的一致性,对部分性发作和全面性-强直阵挛发作患者发作期SPECT和VEEG定位的一致性进行卡方检验。 结果 45例癫痫患者中,发作期SPECT定位阳性率为93.3%(42/45),均表现为高血流灌注灶,其中40例(95.2%)表现为单叶局限性高灌注,2例(4.8%)表现为多个病灶高灌注。VEEG监测结果为:31例患者VEEG表现为局灶性异常放电,明确定位达68.9%(31/45),各导联同步对称性异常放电不能定位者占所有患者的31.1%(14/45)。比较二者定位结果发现,对于部分性发作的患者,发作期SPECT和VEEG定位的一致性为83.9%(26/31);对于全面性-强直阵挛发作的患者,VEEG表现为各导联同步对称性异常放电,而发作期SPECT则显示为孤立高血流灌注灶,故二者定位无一致性。部分性发作和全面性-强直阵挛发作患者发作期SPECT和VEEG定位的一致性差异有统计学意义(χ2=24.478,P<0.05)。 结论 发作期SPECT脑血流灌注显像和VEEG在癫痫灶定位诊断中的一致性与癫痫发作类型相关。对于部分性发作的癫痫患者二者联合定位可指导手术治疗;而对于全面性-强直阵挛发作患者,发作期SPECT脑血流灌注显像和VEEG联合定位无一致性,需借助于其他检查方法方可明确定位。 -
关键词:
- 癫痫 /
- 体层摄影术,发射型计算机,单光子 /
- 视频脑电图
Abstract:Objective To localize the epileptic focus by means of ictal SPECT and video-electroencephalography(VEEG) patterns to decide whether the combination of them are capable of localizing epileptic focus correctly. Methods The present study was performed in 45 epileptic patients, who showed spike waves during VEEG monitoring when deprived of sleep to provoke seizures, even oral application of clonidine was given when deprivation of sleep was failed in limited time. Technetium-99m ethyl cysteinate dimer(99Tcm-ECD)was injected within 30 s when a clinical sign and/or an typical VEEG discharge was recognized, then brain SPECT was performed after 30 min. In the end, compared the results of ictal SPECT and VEEG in localization. χ2 test was performed by using software SPSS l 9.0. Results Ictal brain SPECT localized in 93.3%(42/45)patients, of whom 95.2%(40/42)patients had single hyperperfusion, and 4.8%(2/42)had multiple hyperperfusion. VEEG showed partial seizures in 68.9%(31/45) patients, and 31.1%(14/45)patients showed generalized spike waves. The relationship of ictal SPECT and VEEG in localizing epileptic focus was turned out as following:Firstly, the consistency of ictal SPECT and VEEG is 83.9%(26/31)in partial seizure, as for generalized tonic-clonic seizure, VEEG showed generalized spike waves, and ictal brain SPECT declared single hyperperfusion, therefore, the localization of them was different. The consistency of partial seizure was significantly higher than that of generalized tonic-clonic seizure(χ2=24.478, P < 0.05). Conclusions The consistency of ictal SPECT and VEEG in localization has something to do with epilepsy categories. The study indicates that it is possible to obtain localization in patients with partial seizures using a combination of ictal SPECT and VEEG patterns, as for generalized tonic-clonic seizure, the combination of them is not enough and it's imperative to use other techniques. -
[1] la Fougère C, Rominger A, Fèrster S, et al. PET and SPECT in epilepsy: a critical review[J]. Epilepsy Behav, 2009, 15(1): 50-55. doi: 10.1016/j.yebeh.2009.02.025 [2] Navarro V, Clemenceau S, Habert MO, et al. Epilepsy surgery: when thinking about? Who are the good candidates?[J]. Presse Med, 2011, 40(3): 293-300. doi: 10.1016/j.lpm.2011.01.004 [3] Olsson I, Danielsson S, Hedstrèm A, et al. Epilepsy surgery in children with accompanying impairments[J]. Eur J Paediatr Neurol, 2013, 17(6): 645-650. doi: 10.1016/j.ejpn.2013.06.004 [4] Foldvary-Schaefer N, Unnwongse K. Localizing and lateralizing features of auras and seizures[J]. Epilepsy Behav, 2011, 20(2): 160-166. doi: 10.1016/j.yebeh.2010.08.034 [5] 王维治, 罗祖明.神经病学. 5版.北京:人民卫生出版社, 2005: 227-229.
[6] Kettenmann B, Feichtinger M, Tilz C, et al. Comparison of clonidine to sleep deprivation in the potential to induce spike or sharp-wave activity[J]. Clin Neurophysiol, 2005, 116(4): 905-912. doi: 10.1016/j.clinph.2004.11.006 [7] 王晓慧, 陈雪红, 王正江, 等.可乐定联合剥夺睡眠诱发癫(癎)发作的SPECT脑血流灌注显像研究[J].中华核医学杂志, 2010, 30(6): 375-377.
[8] Lee SK, Lee SY, Yun CH, et al. Ictal SPECT in neocortical epilepsies: clinical usefulness and factors affecting the pattern of hyperperfusion[J]. Neuroradiology, 2006, 48(9): 678-684. doi: 10.1007/s00234-006-0106-z [9] Placantonakis DG, Schwartz TH. Localization in Epilepsy[J]. Neurol Clin, 2009, 27(4): 1015-1030. doi: 10.1016/j.ncl.2009.08.004 [10] 吴立文, 林华.我国癫痫外科术前评估的现状和存在的问题[J].中华医学杂志, 2006, 86(47): 3313-3314. doi: 10.3760/j:issn:0376-2491.2006.47.001
[11] 葛彤, 杨玉芳.药物诱发试验对癫痫患者脑电图的影响[J].山东医药, 2007, 47(29): 81-82.
[12] Sturm JW, Newton MR, Chinvarun Y, et al. Ictal SPECT and interictal PET in the localization of occipital lobe epilepsy[J]. Epilepsia, 2000, 41(4): 463-466. doi: 10.1111/j.1528-1157.2000.tb00190.x [13] Koepp MJ, Woermann FG. Imaging structure and function in refractory focal epilepsy[J]. Lancet Neurol, 2005, 4(1): 42-53. doi: 10.1016/S1474-4422(04)00965-2 [14] Van Paesschen W. Ictal SPECT[J]. Epilepsia, 2004, 45 Suppl 4: S35-40. [15] Yeni SN, Kabasakal L, Yalçinkaya C, et al. Ictal and interictal SPECT findings in childhood absence epilepsy[J]. Seizure, 2000, 9(4): 265-269. [16] Jayalakshmi S, Sudhakar P, Panigrahi M. Role of single photon emission computed tomography in epilepsy[J/OL]. Int J Mol Imaging, 2011, 2011: 803920[2014-01-22]. http://www.hindawi.com/journals/ijmi/2011/803920. [17] 郭勇, 杨自更, 周颖, 等.癫痫患者发作期脑血流灌注显像规范化采集的初步探讨[J].西北国防医学杂志, 2008, 29(3): 189-191.
[18] Calcagni ML, Giordano A, Bruno I, et al. Ictal brain SPET during seizures pharmacologically provoked with pentylenetetrazol: a new diagnostic procedure in drug-resistant epileptic patients[J]. Eur J Nucl Med Mol Imaging, 2002, 29(10): 1298-1306. doi: 10.1007/s00259-002-0879-1 [19] Pastor J, Dominguez-Gadea L, Sola RG, et al. First true initial ictal SPECT in partial epilepsy verified by electroencephalography[J]. Neuropsychiatr Dis Treat, 2008, 4(1): 305-309. [20] Haginoya K, Uematsu M, Munakata M, et al. The usefulness of subtraction ictal SPECT and ictal near-infrared spectroscopic topography in patients with West syndrome[J]. Brain Dev, 2013, 35(10): 887-893. doi: 10.1016/j.braindev.2013.08.011 [21] Thomas R, Bhatia M, Bal CS, et al. Correlation of ictal EEG and SPECT studies in patients of intractable epilepsy with normal MRI[J]. Neurol India, 2002, 50(4): 440-443. [22] Hamandi K, Salek-Haddadi A, Laufs H, et al. EEG-fMRI of idiopathic and secondarily generalized epilepsies[J]. NeuroImage, 2006, 31(4): 1700-1710. doi: 10.1016/j.neuroimage.2006.02.016 [23] Siegel AM. Presurgical evaluation and surgical treatment of medically refractory epilepsy[J]. Neurosurg Rev, 2004, 27(1): 1-21. doi: 10.1007/s10143-003-0305-6 -

 点击查看大图
点击查看大图
图(1)
计量
- 文章访问数: 2504
- HTML全文浏览量: 1216
- PDF下载量: 3