


 下载:
下载:


-
膀胱肿瘤是泌尿系统最常见的肿瘤,多数为移行上皮细胞癌,占我国泌尿生殖系统肿瘤发病率的第一位[1-3]。其检查方法包括尿常规、尿脱落细胞学检查、尿肿瘤标志物检查、盆腔B超、膀胱镜、静脉尿路造影、盆腔CT和(或)盆腔MRI检查。本研究应用64排螺旋CT(64-multi detector spiral CT,64-MSCT)对48例小膀胱肿瘤(直径≤1.5 cm)进行膀胱轴位平扫、动脉期、静脉期、延迟期增强扫描及图像多平面重建后处理,对照临床、影像、手术及病理资料进行回顾性分析、总结,评价64-MSCT在小膀胱肿瘤诊断中的应用价值及临床意义。
-
选取威海市文登中心医院影像科于2006年7月至2012年12月诊断的48例小膀胱肿瘤(直径≤1.5 cm)患者,其中,男性36例、女性12例,年龄23~78岁,平均年龄(48.3±12.2)岁。48例患者中,45例出现血尿,38例为无痛性血尿,26例伴有膀胱刺激症状,仅3例无血尿,但尿急、尿频、尿痛明显。
-
去除患者扫描区多余衣物、饰物和一切影响扫描效果的外来物,注意询问患者近期内有无做钡餐检查,如有需确认排空后方可进行检查。患者于检查前饮温开水500~1000 ml后0.5~1 h,有尿意感时,嘱患者憋尿,继行膀胱CT轴位平扫及增强扫描。
所有患者或家属均于检查前签署了知情同意书。
-
采用荷兰Philips公司生产的Brilliancs型64-MSCT仪,常规轴位平扫参数为:层厚5.0 mm,层间隔5.0 mm,螺距0.891,电压120 kV,电流300 mAs。增强扫描采用双筒注射器,静脉注射60~80 ml非离子造影剂及20~40 ml生理盐水,以3.0 ml/s速度注射,分别于造影剂注入开始后20~25 s(动脉期)、55~65 s(静脉期)和3 min(延迟期)行3次扫描。扫描范围为:髂脊水平至耻骨联合下缘;扫描基线为:平扫由耻骨联合下缘往上扫描,增强扫描由髂脊水平向下扫描。扫描完毕后图像进行1 mm层厚、1 mm间隔重建,在Philips 64-MSCT工作站中将所得数据进行多平面重建后处理,从各种角度观察膀胱癌的部位、形态、大小及其与周围组织结构的关系。
-
本研究48例小膀胱肿瘤中,64-MSCT膀胱轴位平扫检出45例,检出率为93.75%,未检出3例,漏检率为6.25%,漏检病变为扁平状或直径<0.5 cm的小病灶;64-MSCT膀胱轴位平扫及动脉期、静脉期、延迟期增强扫描检出48例,检出率为100%。通过对64-MSCT膀胱轴位及多平面重建图像的观察发现,48例小膀胱肿瘤中,发生在膀胱左侧壁8例、膀胱右侧壁5例、膀胱前壁4例、膀胱三角27例、膀胱憩室内4例。膀胱原位癌2例,0.5 cm≤瘤体直径≤1.5 cm 43例,瘤体直径≤0.5 cm 3例。手术及病理结果发现,膀胱原位癌2例、移行上皮癌38例、腺癌6例、乳头状瘤2例。小膀胱肿瘤的64-MSCT典型影像学表现为:平扫病灶膀胱壁呈不规则增厚或突出膀胱壁类圆形(图 1)、菜花样(图 2)小结节状软组织密度影,平扫CT值为28~35 HU;增强扫描病灶强化幅度明显高于正常膀胱壁,呈均匀性、持续性强化,动脉期CT值为40~46 HU,静脉期为49~66 HU,延迟期为57~62 HU。4例膀胱憩室内小肿瘤表现为突出于憩室壁类圆形小结节状软组织密度影,强化方式基本同前(图 3)。64-MSCT对小膀胱肿瘤诊断及鉴别诊断原位癌2例,1例影像学诊断与手术病理相符(图 4),1例多灶性膀胱原位癌,误诊为膀胱炎,误诊率为50.00%;6例窄基底的带蒂病灶(图 5)均诊断为乳头状瘤,病理诊断结果为膀胱乳头状瘤2例,移行上皮癌4例,误诊4例,误诊率为66.67%;综上,48例小膀胱肿瘤中,43例影像学诊断符合手术病理诊断,诊断准确率为89.59%(43/48),误诊率为10.41%(5/48)。

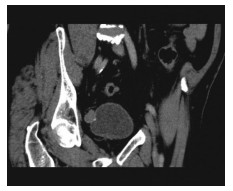
图 1 膀胱CT轴位动脉期显像图。患者男性,46岁。图中示突出膀胱左侧壁膀胱壁类圆形软组织密度影,CT增强扫描病灶强化幅度明显高于正常膀胱壁,表现为均匀、持续性强化,CT诊断为膀胱癌,病理诊断为膀胱移行上皮癌。
Figure 1. Arterial phase CT image of bladder axial scan

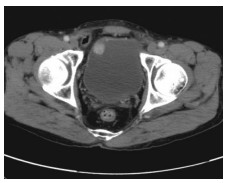
图 2 膀胱CT轴位静脉期显像图。患者女性,52岁。图中示膀胱三角菜花样小结节状软组织密度影,CT增强扫描病灶强化幅度明显高于正常膀胱壁,表现为均匀、持续性强化,CT诊断为膀胱癌,病理诊断为膀胱移行上皮癌。
Figure 2. Venous phase CT image of bladder axial scan

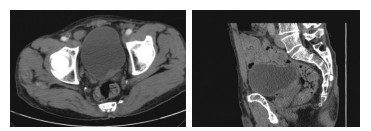
图 3 膀胱CT多平面重建显像图。患者男性,62岁,肉眼无痛性血尿。CT增强扫描膀胱憩室内瘤体表现为均匀、持续性强化。CT诊断为膀胱憩室癌。病理诊断为移行细胞乳头状癌(Ⅱ级),病灶侵及膀胱肌层。
Figure 3. CT multi-planar reconstruction of bladder

图 4 膀胱CT轴位动脉期和多平面重建显像图。患者女性,56岁,血尿7 d,CT表现为膀胱三角壁局限性不规则增厚、毛糙,病变壁厚度为2.5 mm,增强扫描病变强化幅度明显强于正常的膀胱壁,表现为均匀、持续性强化,CT诊断为膀胱原位癌,手术及病理结果为膀胱原位癌。
Figure 4. Arterial phase CT image and multi-planar reconstruction of bladder

图 5 膀胱CT轴位静脉期显像图。患者女性,24岁,无血尿,膀胱刺激症状明显。CT增强扫描窄基底带蒂瘤体表现为均匀、持续性强化,CT误诊为乳头状瘤,病理诊断为膀胱移行上皮癌。
Figure 5. Venous phase CT image of bladder axial scan
-
膀胱肿瘤是泌尿系统最常见的肿瘤,90%为移行上皮肿瘤,其余是鳞状上皮癌和腺癌或其他肿瘤。男性、女性患病率之比约为(2.3~2.7):1。该病可发生于任何年龄,20岁以前的发病率较低,40岁以后逐渐上升,60~70岁发病率达到高峰。该病的临床症状多为无痛性血尿,有时为肉眼无痛性血尿;其次为尿频、尿急、尿痛等膀胱刺激症状,也可有腰部、耻骨上或会阴等处疼痛症状[1-3]。及早发现和诊断病变一直是影像学研究的重点和难点[4]。MSCT的逐渐应用基本已能满足对小病灶检出的要求,明显提高了小病灶的检出率及诊断准确率,已被影像学界所共识[4-5]。
-
美国癌症联合委员会将膀胱癌分为5期[6]。不同分期的膀胱肿瘤,疾病的严重程度和预后转归各不相同。肿瘤分期是膀胱癌最重要的预后因子。
膀胱原位癌:这些“扁平”的肿瘤局限于膀胱的黏膜内,有时膀胱镜下难于发现[3, 7-9],通过膀胱MSCT检查可以检出,原位癌的特征性表现为膀胱壁呈局限性不规则增厚(厚度>2.5 mm)、边缘毛糙;增强扫描病灶强化幅度明显高于正常的膀胱壁,表现为均匀、持续性强化。本研究中1例膀胱壁弥漫性不规则增厚,增强扫描病变表现为多处斑点状、均匀、持续性强化,手术前诊断为膀胱炎,手术及病理结果为膀胱原位癌。
Ta期:占浅表性膀胱癌的70%,肿瘤呈乳头状,像漂动的水草,局限于膀胱的黏膜内,通常是低级别,很少进展为恶性程度高的肿瘤[10-12]。其特征性表现为CT平扫病灶呈突出膀胱壁类圆形或菜花样小结节状软组织密度影;增强扫描病灶呈均匀、持续性强化。本研究30例Ta期患者中,24例小膀胱癌手术前影像诊断与手术及病理结果相符。6例窄基底的带蒂病灶,手术前4例误诊为乳头状瘤,病理诊断为膀胱移行上皮癌;2例乳头状瘤手术前影像诊断与手术及病理结果相符。窄基底带蒂病灶常为乳头状瘤的影像学表现形式,乳头状瘤具有恶化可能,在诊断乳头状瘤的同时,不能排除膀胱癌的诊断。
T1期:肿瘤呈乳头状或结节状,肿瘤穿透基底膜到达黏膜下层,黏膜下层内有淋巴管和毛细血管,因此T1期较Ta期肿瘤更具侵袭性,进展的风险约为30%[3, 7, 11]。本研究11例T1期患者中,手术前影像诊断均为膀胱癌,手术及病理结果与之相符。其特征性表现为CT平扫病变呈突出膀胱壁类圆形或菜花样小结节状软组织密度影,窄基底带蒂病灶非常少见,增强扫描病变表现为均匀、持续性强化。
T2期:肿瘤侵犯膀胱肌层,一般是高级别的,对此期肿瘤尽管能采用局部治疗手段如手术根治,但进一步侵袭发展为转移性疾病的风险仍然存在[3, 7, 10, 14, 17]。本研究5例T2期患者中,手术前影像诊断均为膀胱癌,手术及病理结果与之相符。其特征性表现为CT平扫病灶呈突出膀胱壁类圆形或菜花样小结节状软组织密度影,增强扫描病变表现为均匀、持续性强化,受侵膀胱壁强化幅度高于正常膀胱壁。本研究中1例膀胱憩室内小癌灶属于T2期。
T3期:此期肿瘤通常具有分级高、结节状、侵袭性高的特点,而且有些T3期肿瘤常扩散至膀胱外,治愈难度很大。
T4期:此期肿瘤是高级别、高侵袭性的肿瘤,已侵犯周围邻近器官,有些已扩散至远处器官。
本研究由于未涉及T3、T4期膀胱癌,而且对于T3及T4期膀胱癌的CT表现已有多篇文献报道[8, 10, 13, 15-17],此处不再赘述。
-
膀胱乳头状瘤是一种良性的肿瘤,全名应该为低度恶性潜能的乳头状尿路上皮肿瘤,长期临床观察后发现,此类肿瘤的生物学行为不能归为恶性,其性质介于良、恶性之间,所以世界卫生组织给予其“低度恶性潜能肿瘤”的名称。膀胱乳头状瘤根部可有蒂,与正常的膀胱壁相连向腔内生长,形成指状或乳头状突起,也可呈菜花状或绒毛状。镜下每一乳头由具有血管的分支状结缔组织间质构成其轴心,其表面覆盖的增生上皮因起源部位不同而异,可为鳞状、柱状或移行上皮。此类肿瘤的特征性表现为CT平扫病灶呈窄基底,蒂与正常膀胱壁相连向腔内突起呈菜花状、绒毛状或乳头状肿物,增强扫描病灶为均匀、持续性强化,类似于小膀胱癌的强化表现[18-19]。
总之,对于小膀胱肿瘤的诊断,需要密切结合临床表现,血尿是膀胱癌最常见也是最早出现的症状,患者一般表现为时有时无的、肉眼或镜下可以看见的不伴随疼痛症状的血尿。尤其是40岁以上的成年人,要提高警惕,考虑存在泌尿系肿瘤的可能性。早期膀胱癌多处于良好分化或中等分化状态,治疗效果较好[18]。B超是检查膀胱疾病的常用方法,当腹腔内气体干扰及膀胱充盈不足时,检查效果不佳;当膀胱内充满血液及尿道狭窄时,膀胱镜检查效果不满意。MSCT膀胱轴位平扫加增强扫描基本能满足检出、诊断小膀胱肿瘤的要求,应用多平面重建后处理技术,有利于小膀胱肿瘤的定位。MSCT可以对膀胱癌作出分期判断,了解肿瘤是否浸润膀胱壁及浸润膀胱壁的范围、深度,为临床治疗膀胱癌提供了非常有价值的诊断信息,是一种无创地诊断小膀胱肿瘤的较理想方法。
64排螺旋CT在小膀胱肿瘤诊断中的应用价值
Application value of 64 multi-detector helical CT for diagnosis of small bladder tumor
-
摘要:
目的 评价64排螺旋CT(64-MSCT)在小膀胱肿瘤诊断中的应用价值。 方法 采用64-MSCT对48例小膀胱肿瘤(直径≤1.5 cm)患者进行膀胱轴位平扫、动脉期、静脉期、延迟期增强扫描及图像多平面重建后处理,回顾性分析所获得的CT影像学资料。 结果 48例小膀胱肿瘤中,64-MSCT膀胱轴位平扫检出45例,检出率为93.75%,未检出3例,漏检率为6.25%,漏检病灶均<0.5 cm;64-MSCT膀胱轴位平扫及动脉期、静脉期、延迟期增强扫描检出48例,检出率为100%。应用多平面重建后处理方法检查,有利于小膀胱肿瘤的定位,48例小膀胱肿瘤中,发生在膀胱壁44例、发生在膀胱憩室内4例。经手术及病理证实,48例小膀胱肿瘤中,膀胱原位癌2例、腺癌6例、移行上皮癌38例、乳头状瘤2例。小膀胱肿瘤的64-MSCT平扫表现为乳头状或菜花样小结节状软组织密度影,增强扫描表现为均匀、持续性强化。6例窄基底的带蒂病灶,64-MSCT均诊断为乳头状瘤,而病理诊断结果为乳头状瘤2例,移行上皮癌4例,64-MSCT误诊率为66.67%,表明64-MSCT对窄基底带蒂病灶的鉴别诊断存在一定难度。64-MSCT对诊断小膀胱肿瘤总的准确率为89.59%,误诊率为10.41%。 结论 64-MSCT基本能满足检出、诊断小膀胱肿瘤的要求,是一种无创伤地诊断小膀胱肿瘤较理想的方法。 -
关键词:
- 膀胱肿瘤 /
- 体层摄影术,螺旋计算机 /
- 图像处理,计算机辅助
Abstract:Objective To evaluate the application value of 64-multi detector spiral CT (64-MSCT)in the diagnosis of small bladder tumor. Methods Forty-eight patients with small bladder tumor(≤1.5 cm) were re-checked by bladder axial scans of 64-MSCT, arterial phase, venous phase, delayed phase enhancement scanning and multi planar reconstruction(MPR) reprocessing. CT imaging data were analyzed retrospectively. Results Among the 48 cases of small bladder tumor, 45 cases were detected through bladder axial scans of 64-MSCT, with the positive rate of 93.75%, and 3 cases were not detected, with the miss rate of 6.25%. While 48 cases were detected through bladder axial scans of 64-MSCT, arterial phase, venous phase and delayed enhancement scanning, the positive rate was 100%. The application of MPR reprocessing is favorable to the location of small bladder tumor. Among the 48 cases of small bladder tumor, 44 cases occurred on walls of urinary bladders, and 4 cases in vesical diverticulum. All the cases were confirmed by surgery and pathology. Among the 48 cases of small bladder tumour, 2 cases were demonstrated as carcinoma in situ, 6 cases as adenocarcinoma, 38 cases as transitional cell carcinoma, and 2 cases as papillary epithelioma. The signal intensities of small nodular soft tissues with the papillary or cauliflower-like structures were shown by axial scans of 64-MSCT, and uniform and constant reinforcement were appeared in delayed enhancement scanning. Six cases of narrow base pedunculated lesions were diagnosed as papillary epithelioma by 64-MSCT, while 2 cases were confirmed as papillary epithelioma, and 4 cases as transitional cell carcinoma by pathology. Four cases were misdiagnosed by 64-MSCT, with the misdiagnosis rate of 66.67%. There is some difficulty in differential diagnosis of 64-MSCT on narrow base pedunculated lesions. The accuracy rate of diagnosis of small bladder tumor by 64-MSCT was 89.59%, and the rate of misdiagnosis was 10.41%. Conclusion 64-MSCT can meet the needs of detection and diagnosis of small bladder tumor, and may be an ideal method for the non-invasive diagnosis of small bladder tumor. -
图 1 膀胱CT轴位动脉期显像图。患者男性,46岁。图中示突出膀胱左侧壁膀胱壁类圆形软组织密度影,CT增强扫描病灶强化幅度明显高于正常膀胱壁,表现为均匀、持续性强化,CT诊断为膀胱癌,病理诊断为膀胱移行上皮癌。
Figure 1. Arterial phase CT image of bladder axial scan
图 2 膀胱CT轴位静脉期显像图。患者女性,52岁。图中示膀胱三角菜花样小结节状软组织密度影,CT增强扫描病灶强化幅度明显高于正常膀胱壁,表现为均匀、持续性强化,CT诊断为膀胱癌,病理诊断为膀胱移行上皮癌。
Figure 2. Venous phase CT image of bladder axial scan
图 3 膀胱CT多平面重建显像图。患者男性,62岁,肉眼无痛性血尿。CT增强扫描膀胱憩室内瘤体表现为均匀、持续性强化。CT诊断为膀胱憩室癌。病理诊断为移行细胞乳头状癌(Ⅱ级),病灶侵及膀胱肌层。
Figure 3. CT multi-planar reconstruction of bladder
图 4 膀胱CT轴位动脉期和多平面重建显像图。患者女性,56岁,血尿7 d,CT表现为膀胱三角壁局限性不规则增厚、毛糙,病变壁厚度为2.5 mm,增强扫描病变强化幅度明显强于正常的膀胱壁,表现为均匀、持续性强化,CT诊断为膀胱原位癌,手术及病理结果为膀胱原位癌。
Figure 4. Arterial phase CT image and multi-planar reconstruction of bladder
-
[1] 郭应禄.泌尿、男生殖系肿瘤[M].北京:人民卫生出版社, 2000: 25-39.
[2] 解云川, 张凌.膀胱平滑肌瘤的CT诊断[J].实用放射学杂志, 1999, 15(7): 444-445.
[3] 蒿崑, 韩广秀, 王玉芹, 等.低浓度造影剂膀胱造影对诊断膀胱小肿瘤的价值[J].实用放射学杂志, 2004, 20(3): 257-259. doi: 10.3969/j.issn.1002-1671.2004.03.020
[4] 蒿崑, 赵斌. CT、MRI肝脏局灶性小病灶的影像学研究进展[J].中国实用医刊, 2013, 40(21): 86-88. doi: 10.3760/cma.j.issn.1674-4756.2013.21.038
[5] 李松柏, 徐克.多层螺旋CT临床诊断实践图谱[M].北京:人民军医出版社, 2004: 7-11.
[6] 沈益君, 朱一平, 叶定伟, 等.窄波成像电子膀胱软镜在膀胱肿瘤诊断中的应用价值[J].中华泌尿外科杂志, 2010, 31(6): 383-385. doi: 10.3760/cma.j.issn.1000-6702.2010.06.008
[7] Greene FL, Page DL, Fleming ID, et al. AJCC肿瘤分期手册[M].戈伟, 吴耀贵, 译.北京: 中国医药科技出版社, 2009: 8941-8952.
[8] 周康荣.腹部CT[M].上海:上海医科大学出版社, 1993: 206-209.
[9] 王秀忠, 啜振华, 刘荣欣, 等. CT仿真膀胱镜的临床应用研究[J].中华放射学杂志, 2001, 35(3): 221-223. doi: 10.3760/j.issn:1005-1201.2001.03.018
[10] 沈益君, 叶定伟.浸润性膀胱癌保留膀胱的综合治疗进展[J].中国癌症杂志, 2007, 17(3): 265-268. doi: 10.3969/j.issn.1007-3639.2007.03.019
[11] 沈益君, 叶定伟, 姚旭东, 等.再次经尿道电切术治疗非肌层浸润性膀胱癌[J].中华外科杂志, 2009, 47(10): 725-727. doi: 10.3760/cma.j.issn.0529-5815.2009.10.004
[12] 蒋国梁, 叶定伟, 李进.常见恶性肿瘤的多学科综合诊断和治疗[M].上海:复旦大学出版社, 2011: 387-391.
[13] 叶定伟, 戴波, 方银忠, 等.吉西他滨联合顺铂方案治疗晚期尿路上皮移行细胞癌18例报告[J].中华泌尿外科杂志, 2005, 26(5): 331-333. doi: 10.3760/j:issn:1000-6702.2005.05.014
[14] 叶定伟.膀胱肿瘤家庭防治手册[M].上海:上海第二军医大学出版社, 2009: 69-71.
[15] 沈益君, 叶定伟, 陈羽, 等.膀胱癌根治术中的盆腔淋巴结清扫[J].中华泌尿外科杂志, 2009, 30(2): 114-116. doi: 10.3760/cma.j.issn.1000-6702.2009.02.016
[16] 杨玲, 李连弟, 陈育德, 等.中国2000年及2005年恶性肿瘤发病死亡的估计与预测[J].中国卫生统计, 2005, 22(4): 218-221, 231. doi: 10.3969/j.issn.1002-3674.2005.04.008
[17] 陈燕萍, 冯文兰.膀胱癌的CT诊断及分期[J].中华放射学杂志, 1996, 30(4): 225. doi: 10.3760/j.issn:1005-1201.1996.04.002
[18] 姚德惠.膀胱肿瘤的CT鉴别诊断[J]. CT理论与应用研究, 1999, 8(1): 29-31.
[19] 吴春芳, 王小林, 乌有弘, 等.膀胱肿块的CT诊断探讨[J].实用放射学杂志, 2003, 19(8): 760-763. doi: 10.3969/j.issn.1002-1671.2003.08.027
-

 点击查看大图
点击查看大图
计量
- 文章访问数: 2715
- HTML全文浏览量: 1449
- PDF下载量: 3