


 下载:
下载:
-
在分化型甲状腺癌女性患者131I治疗后5~7 d的全身扫描图像中,常见盆腔子宫水平131I明显浓聚,由于解剖位置关系和131I经由膀胱排出的原因,易误认为是膀胱显影,而本研究发现盆腔子宫水平131I明显浓聚以子宫原因所致的浓聚较多见,并往往伴随子宫病变。本文通过回顾性分析病例资料,结合SPECT/CT断层定位、超声、病史和其他临床资料,了解盆腔浓聚的确切部位和原因,并就盆腔浓聚131I的常见情况及可能的机制进行讨论。
-
选取我院核医学科2007年12月至2013年8月收治的行131I治疗的女性分化型甲状腺癌患者168例,其中,满足纳入标准的盆腔浓聚者46例,均为住院患者,平均年龄(44±9)岁(31~67岁),其中有26例行SPECT/CT定位检查和图像融合处理,其余20例至少2次治疗后全身显像(posttreatment whole body scan,Rx-WBS)图像在盆腔同一部位有相同或相似的浓聚。
纳入标准:①所有患者均经甲状腺全切或次全切后,行131I清甲或清灶治疗,图像资料完整; ②每例患者的Rx-WBS图像至少1次满足盆腔明显浓聚,且若仅有1次显像,必行SPECT/CT定位检查; 若2次及以上显像时,几次显像出现明显浓聚处必在盆腔同一部位,且浓聚特征相对一致; 当疑似子宫浓聚131I且具体原因不明时,行盆腔B超和(或)CT检查。
-
所有患者在131I治疗前均行甲状腺癌手术,服131I前停服左旋甲状腺素钠3~4周以上,低碘饮食两周,测甲状腺功能、甲状腺球蛋白(thyroglobulin,Tg)、Tg抗体水平并行相关影像学检查。纳入分析的46例患者服131I的剂量为2220~9250 MBq,平均(5106 ±1443)MBq。服131I后住院约5~7 d,于服131I后第3天起,给予左旋甲状腺素钠替代、抑制治疗。服131I后5~7 d常规行Rx-WBS,对可疑处行SPECT/CT检查,显像仪器是美国GE公司Infinia VCTM Hawkeye双探头带有符合线路的SPECT/CT仪。治疗前,所有患者或家属均签署了知情同意书。
对于子宫明显浓聚者,均行盆腔B超检查,部分患者行CT检查进一步明确浓聚原因。
-
对经SPECT/CT定位检查的患者,服131I后5~7 d行Rx-WBS,由2名医师用肉眼判断盆腔处是否明显浓聚,判断标准为:①与周围比较有显著浓聚,估计浓聚程度在2倍以上; ②较肝脏处的放射性明显增高或相当,估计浓聚比值≥1;③排除污染。对肉眼判断明显浓聚者再根据SPECT/CT定位和图像融合处理显像,确定具体浓聚部位; 结合对应部位的B超、CT等影像学资料、病史及临床其他相关检查结果进行综合判断。
对未经SPECT/CT定位检查的患者,根据Rx-WBS的图像特点(盆腔131I明显浓聚,数次131I治疗后的Rx-WBS图像浓聚灶相对固定、特征一致),再结合随访及B超、CT等影像学资料进行综合判断。
对盆腔子宫水平浓聚者均行半定量分析:勾画子宫水平浓聚灶的圆形ROI,ROI为软件所允许画出的最小面积,并复制于周边及约肝脏最浓处,分别记录各自前位、后位放射性计数,再根据平方平均数算出每个图像的子宫、周围、肝脏的放射性计数,计算疑似子宫浓聚灶与周围、疑似子宫浓聚灶与肝脏放射性计数的平方平均数比值。
-
对满足纳入条件的46例患者及盆腔未浓聚的23例患者进行随访,采取完善相关病史资料的形式,如是否有妇科疾病,做检查时宫腔是否有节育环,服131I距最近一次月经的时间和经期。对照几次Rx-WBS图像,比较盆腔处同一部位显像的变化及可能原因。
-
在168例分化型甲状腺癌女性患者中,共纳入研究对象46例(46处浓聚灶),半定量分析结果发现,疑似子宫浓聚灶与周围放射性计数的平方平均数比值为5.36±3.27,疑似子宫浓聚灶与肝脏放射性计数的平方平均数比值为2.86±3.26。其中,6例盆腔浓聚分别有两种可能原因,2例浓聚原因目前仍在随访中。在50个导致盆腔131I浓聚的原因中,与子宫相关的浓聚因素41个,与子宫外相关的浓聚因素9个,包括直肠3个(图 1)、膀胱5个、卵巢巧克力囊肿1个。

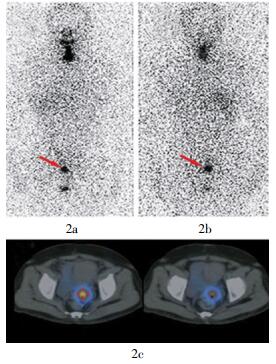
图 1 直肠原因导致的盆腔131I浓聚 图中,1a:治疗后全身显像前位像;1b:治疗后全身显像后位像;1c:SPECT/CT断层融合图像,浓聚定位于直肠,为附壁粪便。
Figure 1. Pelvic 131I uptake caused by rectum
在与子宫有关的41个浓聚因素中,经B超、CT及随访结果证实,子宫肌瘤18个,其他包括节育器9个、子宫内膜增厚2个、宫腔积液3个、月经期7个、子宫内膜腺肌症1个(图 2)、孕囊1个。而在18个子宫肌瘤因素所致的盆腔浓聚患者中,1例同时存在节育器和子宫肌瘤,经SPECT/CT定位检查,浓聚灶仅位于子宫肌瘤处,节育器处未见浓聚。

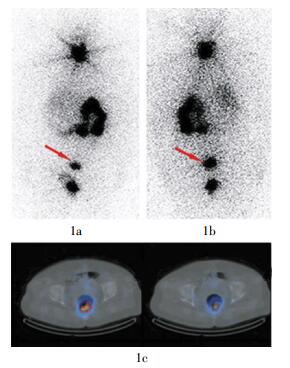
图 2 子宫内膜腺肌症导致的盆腔131I浓聚 图中,2a:治疗后全身显像前位像;2b:治疗后全身显像后位像;2c:SPECT/CT断层融合图像,浓聚定位于子宫,随访证实为子宫内膜腺肌症。
Figure 2. Pelvic 131I uptake caused by uterine adenomyosis
在随访的46例患者中,2例目前为止浓聚原因不明。其中1例曾做过子宫肌瘤手术,随访当时B超正常,131I浓聚是否与手术瘢痕有关还有待证实; 另1例随访及检查结果正常,需继续随访。在另外随访的23例盆腔未浓聚者中,2例患有子宫肌瘤,其余21例无明确子宫病变的证据。
-
造成盆腔131I浓聚的原因很多,正确判断浓聚部位对临床有很大的指导意义。比如,若浓聚在膀胱,应提示患者多喝水,多无需进一步处理; 若浓聚在直肠,应及时给以缓泻剂等促排便药物,以减少局部照射反应; 若浓聚在子宫,应在排除生理性摄取后,建议患者进一步检查以明确可能的妇科疾病。以下为常见浓聚原因的鉴别诊断及可能机制。
-
分化型甲状腺癌组织转移到子宫的概率很低,曾有一篇文献报道了660例分化型甲状腺癌患者,最终仅1例证实为子宫转移[1],因此当浓聚灶定位到子宫时,首先应考虑非转移性因素,包括子宫颈慢性炎症病变,如宫颈糜烂、宫颈息肉、纳氏囊肿; 子宫体病变,如子宫内膜增生症、子宫内膜异位症、子宫肌瘤; 一些引起子宫内膜变化的因素及体液集聚等原因。
本组研究对象中,由子宫原因导致的131I浓聚最多(41/50)。因不同病因、不同子宫位置等因素使不同患者的Rx-WBS图像无明确规律,但同一患者的多次Rx-WBS图像往往变化不大。在Rx-WBS图像中,若盆腔出现浓聚影,行SPECT/CT定位到子宫时,应建议患者行B超、CT等相关检查,以及时发现可能的妇科疾病。
本研究中子宫肌瘤的患者较多(18/46),曾有一篇个例报道提到子宫肌瘤浓聚131I,而其具体机制却不详[2]。也有学者因行肾动态显像时子宫肌瘤显像而得出肌瘤的毛细血管渗透性异常,显像剂泄漏到组织而使子宫肌瘤显影的结论[3]。
子宫内膜腺肌症可能与子宫肌瘤的浓聚原理类似,但尚未查到相关报道。
子宫内膜增厚、服131I时患者处于月经期也会出现131I摄取,推测可能与子宫内膜变化引起血运变化相关。
宫内节育器浓聚131I可能与节育器长期刺激引起宫腔慢性炎症反应有关。虽然子宫相关的炎性病变浓聚131I的报道很少,但其他部位的炎性病灶浓聚131I的报道很多[4-9],比如慢性胆囊炎、自体骨移植处、肺曲霉菌感染、支气管扩张等,只是炎症发生的部位不同,而浓聚机制可能相同。目前认为炎症病变浓聚131I的机制为:局部释放类毒素等炎症介质使血管舒张,血流增加,管腔通透性增加,使131I渗出血管外而聚集在炎症部位,同时,感染过程中增加的血流也携带着增加了131I的浓聚。因此,并非所有宫腔节育器处都会出现131I浓聚,只在发生炎症反应时才出现,本组就有1例患者宫内节育器处未摄取131I。
子宫颈处出现的浓聚灶可因宫颈慢性炎症相关病变所致,如宫颈糜烂、宫颈息肉,或者为月经残留积血,曾有关于阴道积血浓聚131I的报道[10]。
至于月经期子宫[11]、孕囊[12]、宫腔积液浓聚131I的具体机制则不详,可能与含131I的体液被动性聚集有关。
文献报道的涉及子宫附件摄取131I的因素包括卵巢甲状腺囊肿、卵巢囊腺瘤等[12-13],本研究中仅有1例患者的131I浓聚是由子宫外病变——巧克力囊肿所致。
-
由于在平面图像中膀胱与子宫重叠,且90%以上的131I经膀胱排泄,因此在Rx-WBS图像中,若盆腔出现明显浓聚,常被误认为是膀胱显像。而本研究中患者在服131I后5~7 d的Rx-WBS图像中,盆腔明显浓聚者46例(50个浓聚因素),其中与膀胱相关的浓聚因素只占10%(5/50)。分析5例膀胱显像患者的图像后发现,浓聚多为卵圆形,往往前位比后位略浓,且常为某一次而非数次Rx-WBS都出现膀胱浓聚。当膀胱浓聚明显时,常伴较多的残留甲状腺和(或)转移灶。
-
有关直肠浓聚131I的情况,曾有1例直肠肠壁畸胎瘤的报道[14]。本研究经SPECT/CT定位发现,3例浓聚在直肠,其直肠肠壁未见明确的肿块影,仅有少量粪便附着。其Rx-WBS图像表现为后位比前位更明显,常伴结肠显影。直肠浓聚的患者中往往有便秘现象,这与甲状腺癌患者此时处于甲状腺功能减低状态、胃肠道功能降低有关。对于此类患者要及时给予缓泻剂及润便药物,防止局部照射引起不必要的并发症。
-
通过对比研究患者数次Rx-WBS图像后发现,首次清甲治疗后Rx-WBS图像中盆腔处多不会出现131I浓聚,这可能与残留甲状腺组织较多,其他部位131I浓聚减少有关。当浓聚原因为膀胱、直肠时,同一患者数次Rx-WBS图像的变化较大,而为子宫原因时则相对稳定。
总之,当盆腔出现明显131I浓聚时,SPECT/CT定位很重要。在明确具体部位后,应结合病史资料,根据情况提示患者进行相关检查,以及时发现可能的生殖系统疾病。
虽然盆腔明显或异常131I浓聚对甲状腺癌患者的整体治疗方案影响不大,但它能指导临床采取合理的措施,减少不必要的辐射损伤以及提示潜在的妇科疾病,同时还可纠正长期以来误认为盆腔明显浓聚影为膀胱的认识。另外,本研究证实了131I可浓聚在与甲状腺癌无关的病变组织中,比如炎症组织、囊肿、积液等。这就要求临床医师在诊断时一定要结合甲状腺功能、Tg、Tg抗体水平及相关影像学检查进行综合判断。
甲状腺癌131I治疗后全身扫描盆腔浓聚131I的临床分析
Analysis of pelvic 131I uptake after 131I whole body scan in patients with thyroid cancer
-
摘要:
目的 了解分化型甲状腺癌患者131I治疗后全身显像(Rx-WBS)盆腔131I明显浓聚情况及可能机制。 方法 ① 回顾性收集168例分化型甲状腺癌女性患者的资料(均有Rx-WBS图像)。②分析Rx-WBS图像特点,根据一定的纳入标准,最终纳入分析46例患者,并进行随访。 结果 盆腔131I明显浓聚的46例(46处浓聚)患者中,6例同时存在2个可能的浓聚原因,2例目前浓聚原因不明。在50个导致盆腔131I浓聚的原因中,与子宫相关41个,与子宫外相关9个,分别为直肠3个、膀胱5个、卵巢巧克力囊肿1个。在41个与子宫相关的浓聚因素中,结合SPECT/CT定位、B超、CT及随访结果发现,子宫肌瘤18个、节育器9个、子宫内膜增厚2个、宫腔积液3个、月经期7个、子宫内膜腺肌症1个、孕囊1个。 结论 ① 当女性甲状腺癌患者的Rx-WBS图像在盆腔子宫水平出现131I明显浓聚时,多与子宫相关,膀胱因素相对少见;当浓聚定位到子宫时,排除生理性摄取,多提示相关的妇科疾病,以子宫肌瘤多见。②膀胱、直肠所致的盆腔子宫水平131I明显浓聚有其自身特点,相对易区分。③SPECT/CT对定位子宫浓聚131I具有重要意义。 Abstract:Objective To analyze and explore the possible mechanism for pelvic 131I uptake after 131I post treatment whole body scan(RX-WBS)in patients with differentiated thyroid cancer. Methods ① Data were retrospectively reviewed from 168 female patients with differentiated thyroid cancer(everyone has a RX-WBS). ②46 patients were accepted by analyzing the characteristics of Rx-WBS and combing with some inclusion criteria, and then followed up. Results Among the 46 patients(46 positions accumulated 131I)with significant pelvic 131I uptake, 6 patients had two reasons leading to pelvic 131I uptake, and 2 patients had no specific reason. Among the 50 reasons for pelvic 131I uptake, 41 reasons related with uterus, 3 reasons related to rectum, 5 related to bladder and 1 related to ovarian chocolate cyst. Among the 41 reasons related to uterus, by combining the examinations of SPECT/CT, ultrasound, CT and the follow-up results, 18 were uterine leiomyomas, 9 were intrauterine devices, 2 were endometrial thickening, 3 were uterine cavity effusion, 7 were menstrual periods, 1 were uterine adenomyosis, 1 were gestational sac. Conclusions ① In the Rx-WBS of female, the significant pelvic 131I uptake is generally caused by uterus, but not bladder. And it usually means gynecological disease, especially uterine leiomyomas when excluding physiological factors. ②It is generally easy to differentiate bladder from rectum because they have different characteristic features of the pelvic 131I uptake. ③SPECT/CT plays a very important role in locating 131I uptake in uterus. -
Key words:
- Thyroid neoplasms /
- Iodine radioisotopes /
- Whole body imaging /
- Pelvic uptake
-
图 1 直肠原因导致的盆腔131I浓聚 图中,1a:治疗后全身显像前位像;1b:治疗后全身显像后位像;1c:SPECT/CT断层融合图像,浓聚定位于直肠,为附壁粪便。
Figure 1. Pelvic 131I uptake caused by rectum
-
[1] Benbassat CA, Mechlis-Frish S, Hirsch D. Clinicopathological characteristics and long-term outcome in patients with distant metastases from differentiated thyroid cancer[J]. World J Surg, 2006, 30(6):1088-1095. doi: 10.1007/s00268-005-0472-4 [2] Hirata K, Shiga T, Kubota KC, et al. Radioiodine therapy for thyroid cancer depicted uterine leiomyoma[J]. Clin Nucl Med, 2009, 34(1):180-181. [3] Elgazzar AH, Mahmoud AR, Abdel-dayem HM. Technetium-99m DTPA uptake in uterine leiomyoma[J]. Clin Nucl Med, 1988, 13(1):29-31. [4] 罗琼, 罗全勇, 陆汉魁, 等.甲状腺癌131I治疗后扫描胆囊显影1例[J].中国医学影像技术, 2005, 21(10):1551. doi: 10.3321/j.issn:1003-3289.2005.10.060
[5] Yang J, Codreanu I, Servaes S, et al. Elevated iodine uptake at autogenous bone graft harvest sites[J]. Clin Nucl Med, 2012, 37(9):901-903. doi: 10.1097/RLU.0b013e31825b25a7 [6] Ahn BC, Lee SW, Lee J, et al. Pulmonary aspergilloma mimicking metastasis from papillary thyroid cancer[J]. Thyroid, 2011, 21(5):555-558. doi: 10.1089/thy.2010.0448 [7] Triggiani V, Moschetta M, Giagulli VA, et al. Diffuse 131I lung uptake in bronchiectasis:a potential pitfall in the follow-up of differentiated thyroid carcinoma[J]. Thyroid, 2012, 22(12):1287-1290. doi: 10.1089/thy.2011.0439 [8] Gargya A, Chua E. Focal bronchiectasis causing abnormal pulmonary radioiodine uptake in a patient with well-differentiated papillary thyroid carcinoma[J/OL]. Case Rep Endocrinol, 2012, 2012[2013-09-22]. http://www.hindawi.com/crim/endocrinology/2012/452758. [9] Picolos MK, Habra M, Safdar A, et al. Inactive pulmonary tuberculosis mimicking metastasis from papillary thyroid carcinoma in diagnostic radioiodine whole-body scintigraphy[J]. Thyroid, 2005, 15(9):1105-1106. doi: 10.1089/thy.2005.15.1105 [10] Matthern M, Staab E. I-131 localization in hematocolpos:a differential diagnosis consideration for pelvic I-131 uptake[J]. Clin Nucl Med, 2007, 32(8):659-660. doi: 10.1097/RLU.0b013e3180a1ad35 [11] Rachinsky I, Driedger A. Iodine-131 uptake in a menstruating uterus:value of SPECT/CT in distinguishing benign and metastatic iodine-positive lesions[J]. Thyroid, 2007, 17(9):901-902. doi: 10.1089/thy.2007.0084 [12] Leitha T, Staudenherz A. Frequency of diagnostic dilemmas in 131I whole body scanning[J]. Nuklearmedizin, 2003, 42(2):55-62. [13] Song HJ, Xue YL, Xu YH, et al. Abnormal 131I uptake in a benign serous ovarian cystadenoma mimicking bladder physiological uptake[J]. Clin Nucl Med, 2012, 37(3):e59-60. [14] Lakshmanan M, Reynolds JC, De Vecchio S, et al. Pelvic radioiodine uptake in a rectal wall teratoma after thyroidectomy for papillary carcinoma[J]. J Nucl Med, 1992, 33(10):1848-1850. -

 点击查看大图
点击查看大图
图(2)
计量
- 文章访问数: 2092
- HTML全文浏览量: 1512
- PDF下载量: 2