


-
异位肾是一种相对少见的泌尿系统先天疾患, 其以单侧或双侧肾脏位置改变为特征。因异位肾的形态、位置以及与正常位置肾脏的关系不同, 其功能状态也有较大差异。CT血管造影术与CT尿路造影可分别显示肾血管的起源、走行和集合系统状态, 有助于了解异位肾的病情, 为合理制定治疗方案提供依据。上述检查主要应用于异位肾的定位、形态大小的估测, 无法正确评估其功能状况, 而肾动态显像可弥补这一不足, 但在肾动态显像处理图像并计算肾小球滤过率(glomerular filtration rate, GFR)时, 因肾影清晰, 通常采用后位像进行处理, 而无法采用前位像处理。异位肾、移植肾因肾脏靠近腹壁, 肾影较为清晰, 采用前位像处理图像并获取GFR应更为准确。但目前并未见到有关盆腔异位肾前、后位像处理所获GFR差异的分析报道。
-
回顾性分析2007年10月至2013年10月由我院核医学科收集的20例经B超、CT等影像学手段确诊的盆腔异位肾患者, 其中男性12例、女性8例, 年龄2.5~68岁, 平均(28.6±17.6)岁, 多数患者由体检发现, 少数因就诊其他疾病而无意间发现。所有患者分别采用美国ADAC公司双探头SPECT仪和美国GE公司InfiniaVC SPECT仪进行前、后位肾动态显像, 两种仪器各检查10例。因ADAC公司SPECT仪损坏, 无法按要求进行前、后位像对照处理分析, 故从研究中剔除, 其余10例患者[其中男性3例、女性7例, 年龄5~68岁, 平均(26.3±18.3)岁]肾动态显像时分别行前位异位肾单独处理和后位双肾处理, 所得前、后位双肾总GFR分别与双血浆法GFR结果进行比较分析。20例患者中, 有3例失访; 另有3例因输尿管上端梗阻, 有严重肾盂积液, 从而行梗阻处手术治疗, 术后复查尿常规、血肌酐和尿素氮水平均正常; 其余14例均无不适症状, 尿常规、血肌酐和尿素氮水平均正常, 未行任何治疗。
-
采用美国GE公司生产的Infiniavc Hawkeye SPECT仪, 显像剂为99Tcm-DTPA, 99Tcm和DTPA分别由原子高科股份有限公司和北京师宏药物研究中心提供, 放射化学纯度 > 95%, 剂量为111~185 MBq, 采用床旁"弹丸"注射, 前后位双探头采集, 采集矩阵为64×64, 配平行孔准直器。采集前记录患者的身高和体重, 嘱患者空腹按8~10 ml/kg的标准饮水, 若发现肾积水者, 采用利尿肾动态显像。患者饮水20 min后排空膀胱。将含有显像剂的满针注射器置于探头上方30 cm处, 采集10 s。患者取仰卧位, 采集视野包含双肾和膀胱, 共采集20 min(第1分钟为灌注相, 第2~20分钟为功能相)。采集结束后, 将空针注射器置于探头上30 cm处测定10 s。注射显像剂后, 要求患者240 min内禁饮食和暂停输液, 分别于120 min和240 min时在注射显像剂的对侧肘静脉处抽血4~5 ml, 用于计算双血浆法GFR。平均净注射剂量为144.3 MBq。
-
采用前位像处理异位肾, 后位像处理双肾, 通过Gates法计算肾脏GFR。处理时按要求输入患者身高、体重、年龄和注射99Tcm-DTPA前后注射器的放射性活度等数据, 并在计算机显示器上准确勾画出肾脏及本底的感兴趣区, 经计算机处理自动计算出GFR。勾画异位肾感兴趣区时, 应尽量避开膀胱(如有部分肾脏与膀胱重叠, 要将这部分去除), 以免放射性计数异常偏高, 影响相应肾脏GFR结果。双血浆法[1]是一种计算GFR相对准确的方法, 以此作为参照, 将前位异位肾和后位正常肾的GFR总和以及后位双肾GFR与双血浆法GFR进行对比, 以此来判断前、后位像处理异位肾时GFR的相对准确性。前位仅处理异位肾, 与后位异位肾GFR具有可比性, 可将后位正常肾与前位异位肾GFR相加, 获得前位总肾GFR及后位总肾GFR与双血浆法GFR的对比。
-
使用SPSS17.0软件, 采用配对t检验法和双变量相关分析检验法, P < 0.05表示差异有统计学意义。
-
10例行前、后位采集的异位肾患者, 分别行前位异位肾处理和后位双肾处理, 所获得盆腔异位肾的GFR结果见表 1。其中, 10例患者前位像和后位像处理所获异位肾GFR的均数分别为(27.48±12.24)和(10.71±4.74) ml/(min·1.73 m2), 前者比后者高出46%, 二者间差异有统计学意义(t=5.481, P < 0.01)。
患者编号 GFR前位 GFR后位 1 10.90 4.74 2 24.44 4.24 3 41.31 15.57 4 11.24 6.20 5 40.60 16.33 6 26.38 10.82 7 35.97 9.11 8 28.15 9.45 9 41.39 16.51 10 14.41 14.11 注:表中,GFR:肾小球滤过率;GFR前位:前位像处理所获的盆腔异位肾GFR;GFR后位:后位像处理所获的盆腔异位肾GFR。其中,第6、10号患者在处理前位像时因部分异位肾与膀胱重叠,在勾画肾脏感兴趣区时,将重叠部分去除,异位肾GFR被低估。 表 1 盆腔异位肾肾动态显像前、后位像两种处理方法得到的GFR结果比较[ml/(min·1.73 m2)]
Table 1. Comparing of measured GFR of ectopic pelvic kidney between anterior and posterior imaging processing in renal dynamic imaging[ml/(min·1.73 m2)]
-
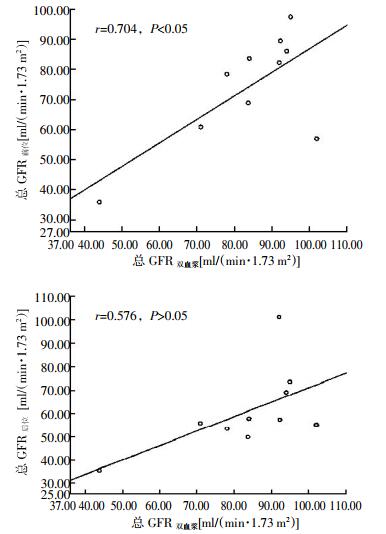
10例异位肾患者行前、后位像处理所获双肾总GFR与双血浆法GFR结果比较及相关性分析结果见表 2、图 1。其中, 10例患者总GFR前位(前位像处理所获异位肾GRF+后位像处理所获正常肾脏GFR)、总GFR后位(后位像处理所获双肾GRF总和)及总GFR双血浆(双血浆法所获双肾GRF总和)的均数分别为(73.98±18.41)、(60.90±14.47)和(83.59±16.63) ml/(min·1.73 m2), 总GFR前位与总GFR双血浆间差异无统计学意义(t=-2.238, P > 0.05), 总GFR前位与总GFR后位间差异有统计学意义(t=2.638, P < 0.05), 总GFR双血浆与总GFR后位间差异也有统计学意义(t=4.629, P < 0.01)。
患者编号 总GFR前位 总GFR后位 总GFR双血浆 1 82.24 101.24 92.00 2 89.45 57.37 92.30 3 83.61 57.83 84.00 4 60.84 55.80 71.00 5 97.40 73.53 95.00 6 57.00 55.14 102.00 7 86.03 69.05 94.00 8 68.84 49.92 83.70 9 78.41 53.54 78.00 10 35.93 35.62 43.90 注:表中,GFR:肾小球滤过率;总GFR前位:前位像处理所获的异位肾GFR+后位像处理所获的正常肾脏GFR;总GFR后位:后位像处理所获的双肾GFR总和;总GFR双血浆:双血浆法所获双肾GFR总和。 表 2 盆腔异位肾肾动态显像前、后位像两种处理方法所获总GFR与双血浆法所获总GFR结果的比较[ml/(min·1.73 m2)]
Table 2. Comparing of measured total GFR of two kidneys among anterior and posterior imaging processing in renal dynamic imaging and in two-sample method[ml/(min·1.73 m2)]

图 1 10例盆腔异位肾患者肾动态显像前、后位像处理所获总GFR与双血浆法所获总GFR的相关性比较图中,GFR:肾小球滤过率;总GFR前位:前位像处理所获的异位肾GFR+后位像处理所获的正常肾脏GFR;总GFR后位:后位像处理所获的双肾GFR总和;总GFR双血浆:双血浆法所获双肾GFR总和。
Figure 1. All correlation analysis of GFRs from anterior and posterior imaging processing in renal dynamic imaging and in two-sample method in 10 patients with ectopic pelvic kidney
从表 2得知, 前位像处理所获GFR更接近于双血浆法GFR结果, 即前位像GFR更接近于真实的盆腔异位肾功能。第6、10号患者经前、后位像两种处理方法所获GFR结果接近, 这与盆腔异位肾部分同膀胱影重叠有关, 在处理过程中, 重叠部分被剔除。因此, 其前、后位像处理所获的GFR小于双血浆法GFR。
将总GFR前位和总GFR后位与总GFR双血浆分别进行pearson分析和spearman分析, 结果发现总GFR前位(r=0.704, P < 0.05)较总GFR后位(r=0.576, P > 0.05)与总GFR双血浆具有更好的相关性(图 1)。
-
异位肾相对少见, 且多位于盆腔内, 是因胚胎发育异常所导致, 多伴有发育不全、外型小、呈分叶或形成双肾盂双输尿管畸形, 也常见肾脏旋转不良和尿路梗阻, 并发肾积水[2]、尿路感染[3]、结石[4]等。异位肾的诊断多依赖于常规的影像学检查, 如超声[5]、CT等[6-7], 磁共振泌尿系水成像技术的三维立体成像也具有很好的实用性和优越性[8]。
异位肾的治疗取决于肾脏病变的程度、临床症状及相关并发症等, 当异位肾功能极差或功能已丧失, 而对侧肾功能正常时, 行异位肾切除可缓解症状或防止相关并发症的发生[9]。有文献报道, 异位肾因其位置的改变, 可能较正常肾更易发生病变, 如发生癌变, 故建议切除异位肾[10-12]。还有文献报道, 在对侧肾功能正常的情况下, 还可以将异位肾作为移植肾的供体, 这样将增加移植肾的供给来源[13]。因此, 对异位肾和对侧正常肾功能的评价, 尤其对各自分肾功能的评价就显得较为重要, 该结果将直接影响对异位肾采取的处置方法。常规影像学检查对异位肾可进行筛查诊断, 并能较准确地了解其形态、大小、输尿管的走形、合并积水的程度等解剖学信息, 却无法准确评估其功能。而核素肾动态显像在异位肾的评价中具有很好的优势, 尤其是在对双肾的分肾功能的评价中。此外, 双血浆法与24 h肌酐清除率测定法对双肾(即总肾)功能的评价也具有很好的优势, 且双血浆法和24 h肌酐清除率测定法已成为测定GFR的经典方法。以上3种方法在肾功能评估中的准确性具有很好的相关性[14]。肾动态显像测定GFR具有无创、操作简便、可同时获得双肾及分肾功能的优势, 被广泛应用于临床; 虽然此法通过Gates法测定分肾功能具有很大的优势, 但其不足之处在于受到的影响因素较多。在保证其他影响因素基本不变的前提下, 肾脏的位置与距离前后体表的远近(即肾脏深度)便成为重要的影响因素, 对盆腔异位肾GFR的测定尤为重要[15]。有研究显示, 99Tcm在腹盆部软组织中的衰减系数约为0.153 cm-1, 肾脏深度每变化1 cm, GFR的测定值就会变化14%;而两侧肾脏深度差的变化, 也会使分肾GFR发生改变[16]。因此, 盆腔异位肾的具体位置决定了其肾脏深度, 也就决定了其GFR的估测值。大量影像学资料显示, 盆腔异位肾更接近于腹前壁。在肾动态显像中, 前位像较后位像可见更为清晰的盆腔异位肾影, 便于勾画异位肾的感兴趣区, 能获得更为精确的异位肾图像和相应的肾功能测定结果。在应用Gates法测算GFR时, 理论上来说前位像所获GFR应大于后位像GFR。本研究结果显示, 前位像所获GFR要远大于后位像GFR, 也更接近于真实的双血浆法GFR, 在评判盆腔异位肾功能时, 采用前位像处理图像测定GFR更为合理、真实和可靠。但因盆腔异位肾多数位于膀胱上方, 时常会与充盈的膀胱影重叠, 在测算GFR时会受到一定的影响。本研究中第6、10例患者即是该种情况, 在剔除重叠影后, 所测异位肾的GFR与后位像GFR相差不大, 而与双血浆法GFR的差值明显增大, 在评估盆腔异位肾时应适当引起关注。因此, 对于依靠盆腔异位肾功能状况来决定如何处置异位肾时, 在处理图像计算GFR的过程中, 建议使用前位肾动态图像来进行测定, 能够更真实地反映其功能状态。因本研究病例数较少, 无法涵盖异位肾的各种情况, 今后还需继续收集病例, 进一步完善研究。
盆腔异位肾肾动态显像前后位像GFR测定值的差异比较
Comparing the difference of measured GFR of ectopic pelvic kidney between anterior and posterior imaging processing in renal dynamic imaging
-
摘要:
目的 比较分析盆腔异位肾肾动态显像前、后位像肾小球滤过率(GFR)测定值的差异。 方法 回顾性分析10例盆腔异位肾患者的肾动态显像GFR测定结果, 分别进行前位异位单肾处理和后位双肾处理, 将后位像处理所获正常肾脏GFR与前位像处理所获异位肾GFR相加, 获得总肾GFR, 并与后位像处理所获双肾GFR和双血浆法GFR测定结果进行比较和相关性分析, 并进行了相应随访。采用配对t检验法和双变量相关分析检验法对数据进行统计学分析。 结果 10例盆腔异位肾患者前位像处理所获异位肾GFR[(27.48±12.24)ml/(min·1.73 m2)]较后位像处理所获异位肾GFR[(10.71±4.74)ml/(min·1.73 m2)]高出46%, 二者间差异有统计学意义(t=5.481, P < 0.01)。前位像处理所获总GFR与双血浆法GFR差异无统计学意义(t=-2.238, P>0.05), 二者的相关性较好(r=0.704, P < 0.05);后位像处理所获总GFR与双血浆法GFR差异有统计学意义(t=4.629, P < 0.01), 二者的相关性较差(r=0.576, P>0.05)。 结论 在肾动态显像中, 前位像处理所获GFR较后位像更能真实地反映盆腔异位肾的功能状况。 Abstract:Objective To compare and analyze the difference of measured glomerular filtration rate(GFR)of ectopic pelvic kidney between anterior and posterior imaging processing in renal dynamic imaging. Methods Methods There were 10 patients collected retrospectively, with ectopic kidneys in pelvic cavity confirmed by ultrasound, CT, renal dynamic imaging and other imaging modalities. All images of ectopic kidneys in renal dynamic imaging were processed by anterior and posterior methods respectively. The ectopic kidney was only processed in anterior imaging, ectopic kidney and contralateral normal kidney were processed in posterior imaging. Total GFR equalled the sum of GFR of normal kidney in posterior imaging and GFR of ectopic kidney in anterior imaging, was compared with total GFR of two kidneys in posterior imaging and GFR in two-sample method. Allcorrelation analysis were completed between GFRs from three methods and all patients were followed up. Statistically paired t-test and bivariate correlation analysis test were used. Results The mean GFR of ectopic kidney in anterior imaging equal to(27.48±12.24) ml/(min·1.73 m2). It was more than GFR[(10.71±4.74) ml/(min·1.73 m2)] in posterior imaging above 46%(t=5.481, P < 0.01). There was no significant difference(t=-2.238, P>0.05), but better correlation(r=0.704, P < 0.05)between total GFR in anterior imaging and GFR in two-sample method. There was significant difference(t=4.629, P < 0.01)and worse correlation(r=0.576, P>0.05)between total GFR in posterior imaging and GFR in two-sample method. Conclusions Comparing with GFR in posterior imaging, GFR in anterior imaging can more truly reflect function condition of ectopic pelvic kidney in renal dynamic imaging. -
Key words:
- Glomerular filtration rate /
- Ectopic kidney /
- Renal dynamic imaging
-
图 1 10例盆腔异位肾患者肾动态显像前、后位像处理所获总GFR与双血浆法所获总GFR的相关性比较图中,GFR:肾小球滤过率;总GFR前位:前位像处理所获的异位肾GFR+后位像处理所获的正常肾脏GFR;总GFR后位:后位像处理所获的双肾GFR总和;总GFR双血浆:双血浆法所获双肾GFR总和。
Figure 1. All correlation analysis of GFRs from anterior and posterior imaging processing in renal dynamic imaging and in two-sample method in 10 patients with ectopic pelvic kidney
表 1 盆腔异位肾肾动态显像前、后位像两种处理方法得到的GFR结果比较[ml/(min·1.73 m2)]
Table 1. Comparing of measured GFR of ectopic pelvic kidney between anterior and posterior imaging processing in renal dynamic imaging[ml/(min·1.73 m2)]
患者编号 GFR前位 GFR后位 1 10.90 4.74 2 24.44 4.24 3 41.31 15.57 4 11.24 6.20 5 40.60 16.33 6 26.38 10.82 7 35.97 9.11 8 28.15 9.45 9 41.39 16.51 10 14.41 14.11 注:表中,GFR:肾小球滤过率;GFR前位:前位像处理所获的盆腔异位肾GFR;GFR后位:后位像处理所获的盆腔异位肾GFR。其中,第6、10号患者在处理前位像时因部分异位肾与膀胱重叠,在勾画肾脏感兴趣区时,将重叠部分去除,异位肾GFR被低估。  下载: 导出CSV
下载: 导出CSV
表 2 盆腔异位肾肾动态显像前、后位像两种处理方法所获总GFR与双血浆法所获总GFR结果的比较[ml/(min·1.73 m2)]
Table 2. Comparing of measured total GFR of two kidneys among anterior and posterior imaging processing in renal dynamic imaging and in two-sample method[ml/(min·1.73 m2)]
患者编号 总GFR前位 总GFR后位 总GFR双血浆 1 82.24 101.24 92.00 2 89.45 57.37 92.30 3 83.61 57.83 84.00 4 60.84 55.80 71.00 5 97.40 73.53 95.00 6 57.00 55.14 102.00 7 86.03 69.05 94.00 8 68.84 49.92 83.70 9 78.41 53.54 78.00 10 35.93 35.62 43.90 注:表中,GFR:肾小球滤过率;总GFR前位:前位像处理所获的异位肾GFR+后位像处理所获的正常肾脏GFR;总GFR后位:后位像处理所获的双肾GFR总和;总GFR双血浆:双血浆法所获双肾GFR总和。
下载: 导出CSV
-
[1] Hephzibah J, Shanthly N, Oommen R. Comparison of glomerular filtration rate measured by plasma sample technique, Cockroft Gault method and Gates′method in voluntary kidney donors and renal transplant recipients[J]. Indian J Nucl Med, 2013, 28(3):144-151. doi: 10.4103/0972-3919.119544 [2] Hsieh MY, Ku MS, Tsao TF, et al. Rare case of atrophic ectopic kidney with giant hydronephrosis in a 7-year-old girl[J]. Urology, 2013, 81(3):655-658. doi: 10.1016/j.urology.2012.11.036 [3] Lu CC, Tain YL, Yeung KW, et al. Ectopic pelvic kidney with urinary tract infection presenting as lower abdominal pain in a child[J]. Pediatr Neonatol, 2011, 52(2):117-120. [4] Taslim BB, Abdulwasiu BA, Olusegun S, et al. Crossed renal ectopia coexisting with nephrolithiasis in a young Nigerian man[J]. Arab J Nephrol Transplant, 2012, 5(2):107-110. [5] Markov D, Atanassova D, Pavlova E, et al. Empty renal fossa-a prenatal diagnostic dilemma[J]. Akush Ginekol(Sofiia), 2010, 49(5):13-19. [6] Kim TH, Lee HH, Lee SH, et al. Three-dimensional CT is useful for diagnosing an ectopic kidney[J]. J Obstet Gynaecol, 2010, 30(8):877-878. doi: 10.3109/01443615.2010.516376 [7] Bolen MA, Tandon NS, Roselli EE. Pseudocoarction of the aorta and crossed fused ectopic kidney assessed by multidetector computed tomography[J]. J Cardiovasc Comput Tomogr, 2010, 4(6):405-406. doi: 10.1016/j.jcct.2010.09.003 [8] Muthusami P, Ramesh A. Appearances of the circumcaval ureter on excretory urography and MR urography:A single-center case series[J]. Indian J Radiol Imaging, 2013, 23(1):81-85. doi: 10.4103/0971-3026.113621 [9] Negre T, Haddad M, Garaix F, et al. Laparoscopic nephrectomy of a cross-fused ectopic kidney in a child with hypertension[J]. J Pediatr Urol, 2010, 6(5):522-524. doi: 10.1016/j.jpurol.2010.03.006 [10] Soni HC, Jadav VJ, Sumariya B, et al. Primary malignancy in crossed fused ectopic kidney[J]. Abdom Imaging, 2012, 37(4):659-663. doi: 10.1007/s00261-011-9824-8 [11] Baldie KG, Al-Qassab UA, Ritenour CW, et al. Pelvic nephroureterectomy for renal cell carcinoma in an ectopic kidney[J/OL]. Case Rep Oncol Med, 2012, 2012[2013-11-25]. http://www.hindawi.com/crim/oncological.medicine/2012/350916. [12] Yadav R, Kataria K, Balasundaram P, et al. Mucinous cystadenocarcinoma arising in an ectopic kidney simulating a retroperitoneal dermoid cyst:a rare tumour presenting as a diagnostic dilemma[J]. Malays J Pathol, 2013, 35(1):95-98. [13] He B, Mitchell A. Laparoscopic donor nephrectomy for ectopic kidney[J]. Transplant Proc, 2012, 44(10):3051-3054. doi: 10.1016/j.transproceed.2012.05.078 [14] 解朋, 吴炜杰, 黄建敏, 等.测定慢性肾小球肾炎患者肾小球滤过率的三种方法比较[J].中华肾脏病杂志, 2010, 26(10):766-769. doi: 10.3760/cma.j.issn.1001-7097.2010.10.009
[15] 麻广宇, 邵明哲, 陈云爽, 等.肾脏深度对SPECT测定肾小球滤过率的影响[J].中国医学影像技术, 2013, 29(5):161-165.
[16] Gates GF. Computation of glomerular filtration rate with Tc-99m DTPA:an in-house computer program[J]. J Nucl Med, 1984, 25(5):613-618. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 1906
- HTML全文浏览量: 1229
- PDF下载量: 5