


-
呼吸门控PET/CT(respiratory-gated PET/CT,RG PET/CT)有效改善了PET/CT检查中呼吸运动造成的干扰,在临床上发挥出越来越重要的应用价值[1-2]。然而,采用常规剂量管电流进行RG PET/CT将产生相当大的辐射剂量,因此造成其临床应用受限。辐射防护的最优化一直是医学影像学研究的热点问题[3~5]。目前,国内关于RG PET/CT的文献仅有几篇[6-7],国外也仅有几篇涉及到RG CT的辐射剂量的研究[8~10],采用的管电流范围为50~150 mA,均将呼吸周期分为10个时相,产生的辐射剂量较大。常规胸部CT扫描管电流一般为250~350 mA,而常规PET/CT一般采用较低剂量管电流(120 mA),本研究选用30 mA管电流行RG PET/CT,对比其与120 mA的PET及CT图像质量,试图建立一个图像质量适于临床(结节诊断分期、放疗生物靶区勾画等)且辐射剂量相对较低的理想扫描条件。
-
收集2010年5月至2012年8月在我院核医学科行PET/CT检查发现肺结节有18F-FDG摄取且肺结节分布在一个PET床位内的受检者26例,其中,男性13例、女性13例,平均年龄(63.6±9.7)岁。受检者均行RG PET/CT,并签署知情同意书。
-
Discovery VCT型PET/CT仪由美国GE公司生产,RG数据的采集由美国Varian公司开发的实时监控系统完成。图像后处理工作在美国GE公司AW4.4工作站上进行。患者检查前禁食、禁水6 h以上,检查当日空腹血糖浓度控制在适当范围。
常规显像(1个床位):注射18F-FDG后静息40~65 min,显像前排空膀胱。CT扫描条件为:120 kV,120 mA,层厚3.75 mm,螺距0.984:1,旋转时间0.8 s,扫描范围1个床位。PET采集2 min/床位。
RG PET/CT:紧接常规显像进行,检查前对患者行自由呼吸训练。连接好呼吸实时监控系统。先行衰减校正CT扫描:管电流120 mA,其余条件同非门控显像,再行6个时相的PET采集,采集时间6 min,即1 min/时相。PET采集完成后行低剂量四维CT电影模式扫描:管电压120 kV,管电流30 mA,旋转时间0.5 s,螺距0.984:1,上下扫描范围略大于PET采集范围,层厚2.5 mm,电影持续时间为呼吸周期+1 s,间隔时间为0.3 s。
模拟实验:①对水模分别行120 mA及30 mA管电流CT扫描,其余条件同四维CT,各扫描10幅图像,测量均匀性及噪声,评估图像质量;②应用呼吸模拟机模拟不同的呼吸周期,探讨呼吸周期长短与辐射剂量间的关系,寻找低剂量扫描的理想呼吸模式;③常规胸部CT及肺部肿瘤放疗定位常采用250~350 mA管电流,因此我们选取3名志愿者行1个床位的常规PET/CT显像,分别采用250、300、350 mA的管电流(其余扫描条件同上),对比其与30 mA RG PET/CT产生的辐射剂量的关系。
-
辐射剂量数据均取自扫描程序结束后计算机自动输出的剂量报告。剂量参数包括CT容积剂量指数、剂量长度乘积(dose-length product,DLP)、有效吸收剂量。胸部有效剂量变换系数取0.017。
-
CT图像质量评估:(1)水模成像的均匀性及噪声评价:在模拟实验得到的2组各10幅图像上各选择5个面积为100 mm2的圆形ROI,分别位于图像的中心和上、下、左、右距边缘20 mm处,测量CT值和标准差,计算均匀性及噪声:均匀性=CTc-CTp(CTc为中心测量区的平均CT值,CTp为边缘4个测量区的平均CT值),噪声即上述测量区CT值的标准差平均值。根据国家计量检定规定,均匀性绝对值≤5 HU为可接受范围[11]。(2)受检者图像的视觉评价:由2名高年资放射科医师对26例共33个结节所在肺段支气管血管束、结节特性(形态、周边特性)、结节大小进行观测。评价标准为:①支气管血管束:段级或段级以下支气管、三级或三级以下肺血管清晰显示,且边缘锐利为优;段级或段级以下支气管、三级或三级以下肺血管可以显示,但边缘略毛糙为较好;段级或段级以下支气管、三级或三级以下肺血管不可显示为差。②肺结节特性:分可观和不可观,结节形态主要包括大体形状(球形、类圆形、不规则形)、分叶征、棘状突起,周边特性则包括细毛刺征、结节周边磨玻璃密度、卫星灶、胸膜凹陷征等;③结节大小:选择结节显示的最大横轴面,手动勾画测其横截面积,取3次测量的平均值。
PET图像质量评估:由于RG PET/CT将呼吸时相分为6份,1个床位PET采集6 min,即1 min/时相,因此会造成PET图像信息量的减低。通过查阅文献,可用SUV信噪比这一参数来评价其与常规PET图像(2 min/床位)的差异。在肺结节上选取面积为100 mm2的圆形ROI,测量SUV平均值及标准差,并计算信噪比:信噪比= SUV平均值/SUV标准差[12]。
-
应用SPSS 17.0软件进行统计学分析,数据采用x±s表示,差值满足正态分布及方差齐性的数据用配对t检验,否则用配对秩和检验。P < 0.05表示差异有统计学意义。
-
受检者行1个床位的低剂量(30 mA)RG PET/CT的有效吸收剂量为4.88~7.69 mSv,常规剂量(120 mA)PET/CT的有效吸收剂量为1.68 mSv,3名志愿者行常规剂量(250~350 mA)PET/CT的有效吸收剂量为5.60~7.85 mSv(表 1)。低剂量RG PET/CT与常规剂量(250~350 mA)PET/CT产生的剂量接近,说明采用低管电流行RG PET/CT可以使辐射剂量得到有效控制。
CT剂量类型
(1个PET床位)例数 有效吸收剂量
(mSv)剂量长度乘积
(mGy·cm)30 mA低剂量RG PET/CT 26 5.68±0.83 333.95±48.58 250~350 mA常规剂量PET/CT 3 6.73±1.13 395.64±65.94 120 mA常规剂量PET/CT 26 1.68±0.73 99.03±43.15 表 1 低剂量RG PET/CT与常规剂量PET/CT的辐射剂量结果(x±s)
-
水模图像的均匀性及噪声分析结果见表 2。30 mA低剂量CT图像的均匀性 < 5 HU,在可接受范围,但噪声较120 mA常规剂量CT更高,二者间差异有统计学意义(t=2.736,P < 0.05)。
CT剂量类型 例数 均匀性(HU) 噪声(HU) 30 mA低剂量CT 10 0.34±0.21 21.65±0.83 120 mA常规剂量CT 10 0.29±0.17 8.38±1.46 表 2 低剂量CT与常规剂量CT图像质量比较(x±s)
-
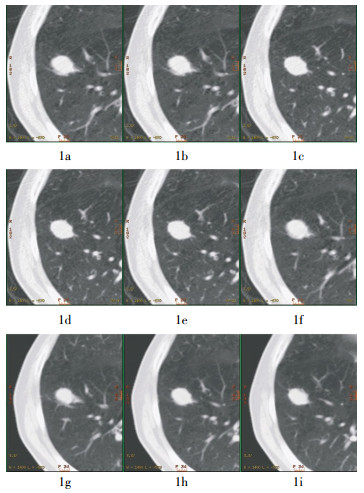
26例患者共33个结节所在肺段的支气管血管束显示常规剂量(120 mA)时全部为优或较好,低剂量(30 mA)时85%显示为较好或优,仅有3枚结节因患者呼吸明显不均而显示较差,二者间差异无统计学意义(Z=-1.615,P > 0.05);而结节特性观察及大小测量结果显示二者间差异亦无统计学意义(Z=-1.315,P > 0.05),且在第3~5个呼吸时相肺结节的边界更锐利,分叶征、细毛刺征等征象更容易观察(图 1)。

图 1 患者男性,56岁,无明显不适主诉,体检胸部X线片发现右肺结节。PET/CT发现右下肺前基底段18F-FDG摄取增高结节。图中,1a~1f为同一层面肺结节的6个呼吸时相的30 mA CT图像,其中,1c~1e示第3~5个时相的肺结节大小、形态及周边细短毛刺显示清晰;1g~1i为连续3个层面的120 mA常规剂量CT图像。
-
RG PET/CT的6 min/床位即1 min/时相所得的PET图像SUV信噪比为4.00±0.35,常规2 min/床位的PET图像SUV信躁比为3.98±0.55,二者间的信噪比差异无统计学意义(Z=-1.109,P > 0.05)。
-
由表 3可以看出,呼吸周期和扫描持续时间越长,受检者所接受的CT容积剂量指数及DLP越大,即有效吸收剂量越大。因此,嘱咐受检者尽量缩短呼吸周期是减少辐射剂量的有效办法。
呼吸周期(s) 电影持续时间(s) CT容积剂量指数(mGy) 剂量长度乘积(mGy·cm) 0.5 1.5 3.94 63.03 1.0 2.0 5.25 84.04 1.5 2.5 6.57 105.05 2.0 3.0 7.88 126.06 2.5 3.5 9.19 147.07 3.0 4.0 10.50 168.07 3.5 4.5 11.82 189.08 4.0 5.0 13.13 210.09 4.5 5.5 14.44 231.10 5.0 6.0 15.76 252.11 5.5 6.5 17.07 273.12 6.0 7.0 18.38 294.13 6.5 7.5 19.70 315.14 7.0 8.0 21.01 336.15 7.5 8.5 22.32 357.16 8.0 9.0 23.64 378.17 表 3 呼吸周期与辐射剂量关系的模拟结果
-
由于RG PET/CT能有效校正运动伪影,其测量的SUV相应增高,从而提高了病变的检出率及争议病变的诊断准确率,因此在临床及基础研究中的应用越来越广泛,已从早期较广泛的肺部肿瘤诊断[1]、放疗靶区勾画研究[13]扩展到腹部胰腺癌[14]、肝转移灶[15]等的研究中,且最新发现已用于建立动物模型的基础研究[16]。
本研究为了避免受检者短时间内受到大量照射,仅对其行30 mA的RG PET/CT,不足之处在于未能对比低剂量与常规剂量(120 mA或更高剂量管电流)、6个呼吸时相与更多呼吸时相(> 6个)的RG PET/CT数据。而本研究的重点在于探讨30 mA、6个呼吸时相RG PET/CT采集的可行性。
-
在适当范围内降低管电流对CT图像质量的影响在可接受范围内。国内学者报道的最低管电流为20~35 mA(或mAs)[17-18],殷瑞根等[19]还针对肺尖部这一特殊部位提出30~50 mA的低剂量管电流;而国外较早的相关报道为50 mAs[20],近年则低至10~20 mAs[8, 21~24]。Christe等[24]对比了5~300 mAs的不同管电流对肺结节的检出率,结果发现10 mAs及以上的低剂量管电流的图像检出率无明显差异。Li等[8]对10 mAs CT图像进行四维惩罚加权最小二乘算法重建,得到了噪声抑制较好、分辨率较高的PET/CT图像。Das等[23]也在10 mAs基础上对比肉眼与计算机辅助检测算法对肺结节检出率的差异,结果发现借助计算机辅助检测算法能更好地显示肺结节。诸如计算机辅助检测算法及四维惩罚加权最小二乘算法重建技术等都为RG PET/CT进一步降低辐射剂量提供了技术基础。
基于以上研究,本研究选择30 mA作为实验性低剂量管电流,研究结果证明30 mA采集的图像质量基本满意,又能大幅降低对患者的辐射剂量。
-
基于非均匀有理B样条曲线的心脏-躯干体模是集成了人体解剖数据并能够模拟心脏和呼吸运动的动态数字体模,Zhu等[25]研究了不同门控方案对基于非均匀有理B样条曲线的心脏-躯干数字体模的蒙特卡罗仿真图像的呼吸伪影校正效果,结果表明:当时相数小于6个时,起始时相位于呼气和吸气末时的图像比其他位置的图像更模糊;当时相数在8个以上时,可消除起始时相位置对图像的影响,伪影也校正得更彻底。而呼吸时相数目越多,相同采集时间内单个相位获得的信息越少,图像质量则相应变差。故本研究选择6个呼吸时相,在有效校正呼吸伪影的同时,又不必特意增加单个床位的采集时间。
呼吸周期模拟实验证实辐射剂量与呼吸周期呈正相关。呼吸周期和扫描时间越短,受检者所接受的辐射剂量越低。但在临床实际中一味要求受检者缩短呼吸周期,反而常会引发呼吸不均,依旧会影响RG的采集甚至采集失败。一般来说,正常人呼吸周期多为3~5 s(12~20次/min),如此模拟的有效吸收剂量为2.86~4.28 mSv,仍低于本研究中的实际采集吸收剂量。因此,嘱咐受检者尽量避免大幅度喘气、尽可能平静均匀地呼吸即为相对理想的呼吸方式。
此外,四维CT扫描的范围应略大于PET范围,技术人员应尽量缩短Z轴的扫描范围,这对减低受检者的辐射剂量亦有意义。
-
根据国家计量检定规定,低剂量RG PET/CT的CT图像均匀性良好(< 5 HU),但噪声水平较大,除了管电流较低这个主要原因外,2.5 mm的较小层厚也是重要原因之一[26]。然而,2位高年资放射科医师对于肺结节特性的观测在低剂量CT中并未受到明显影响,相反,由于克服了呼吸伪影,在某些时相上(如第3~5个时相)的观测反而更优。因此,低剂量CT不仅足以满足放疗靶区勾画的需要,也能基本满足肺结节的诊断需求。
-
国内一项研究报道常规胸部CT扫描辐射剂量约为(6.9±0.1)mSv[120 kV,(382.8±26.0)mA] [27],本研究中250~350 mA常规PET/CT扫描患者的有效吸收剂量为5.60~7.85 mSv。而低剂量RG PET/CT的有效吸收剂量为4.88~7.69 mSv,与上述常规诊断的辐射剂量近似,说明采用低管电流可以使辐射剂量得到有效地控制。国外有研究指出,RG PET/CT显像的辐射剂量是常规CT的15~16倍[9]。Pan等[10]的研究发现,在50~150 mA管电流、5 s的电影持续时间、0.5 s的球管旋转时间、20 cm的扫描范围、10个时相的胸部RG PET/CT的采集条件下,辐照剂量为23~70 mGy,有效剂量相当于7.82~23.8 mSv,辐射剂量相对较高。而Li等[8]则发现,在120 kV、90 mA、2.5 mm层厚、25 cm扫描范围、0.45 s的扫描间隔时间、0.8 s的持续时间下,辐照剂量为80.2 mGy,有效剂量相当于34 mSv,受检者的受照剂量更高。
此外,关于30 mA低剂量RG PET/CT在放疗生物靶区定位中的应用,考虑到放疗患者在定位前多数已行近期诊断剂量的胸部CT,因此没有必要采用诊断剂量的管电流对其进行PET/CT靶区定位,而低剂量管电流既可满足定位需求又不致无谓地加大患者的受照剂量。
基于30 mA管电流低剂量呼吸门控PET/CT扫描条件的建立讨论
Low-dose respiratory-gated PET/CT: based on 30 mA tube current
-
摘要:
目的 通过改善呼吸门控PET/CT(RG PET/CT)的扫描参数(如管电流、呼吸时相数目、呼吸周期等),拟建立一个低辐射剂量且图像质量适于临床的扫描条件。 方法 对26例有18F-FDG摄取的肺结节患者行1个床位的低剂量RG PET/CT(30 mA,1min/时相),评估其辐射剂量,并对比其与常规PET/CT(120 mA,2 min/床位)的图像质量(如均匀性、噪声、视觉评价)的差别。此外,通过模拟不同呼吸周期探讨其与辐射剂量间的关系。 结果 1个PET床位的低剂量RG PET/CT的有效吸收剂量可降至4.88~7.69 mSv[平均(5.68±0.83)mSv],且其PET图像信噪比与常规剂量时相比无明显差异,低剂量CT图像的均匀性在可接受范围(< 5 HU),噪声较高,视觉评价肺结节特性在某些时相优于常规剂量CT。受检者的呼吸周期与辐射剂量呈正相关。 结论 基于30 mA管电流、6个呼吸时相、1 min/时相、平静呼吸下的RG PET/CT的图像质量能满足肺结节特性观测及肿瘤放疗生物靶区勾画等临床应用,且辐射剂量大幅减低。 -
关键词:
- 辐射剂量 /
- 正电子发射断层显像术 /
- 体层摄影术,X线计算机 /
- 呼吸门控
Abstract:Objective To establish a low-dose but image-comparable respiratory-gated PET/CT(RG PET/CT) protocol based on 30 mA tube current plus other improved scanning parameters, such as the tube current, the number of respiratory phase and length of breathing cycle. Methods Twenty-six patients with 18F-FDG-intaking lung nodules underwent one-bed standard-dose PET/CT(120 mA, 2 min/bed)and low-dose RG PET/CT(30 mA, 6 respiratory phases, 1min/phase). The radiation dose and image quality were analyzed subsequently with signal to noise ratio(SNR)for PET and the homogeneity, noise level for CT in the water phantom respectively. Otherwise the CT images were both visual evaluated by two experienced doctors. In addition, different respiratory cycle was simulated to observe its relation with radiation dose. Results The effective dose of low-dose RG PET/CT was 4.88~7.69 mSv[mean(5.68±0.83) mSv]. The PET SNR showed no significance between groups. The homogeneity of 30 mA is good(< 5 HU), although noise level was high, the visual character like lobulation, speculation of lung nodule was superior in some respiratory phases. The radiation dose was positively correlated with respiratory cycle. Conclusions The performance of low-dose RG PET/CT was comparable to those of standard-dose PET/CT based on a protocol with 30 mA tube current, 6 respiratory phases and breathing state of eupnoea. It produced a much lower radiation exposure and the image quality was enough for clinical use such as delineation of tumor active target, characterization and staging of lung nodules, etc. -
图 1 患者男性,56岁,无明显不适主诉,体检胸部X线片发现右肺结节。PET/CT发现右下肺前基底段18F-FDG摄取增高结节。图中,1a~1f为同一层面肺结节的6个呼吸时相的30 mA CT图像,其中,1c~1e示第3~5个时相的肺结节大小、形态及周边细短毛刺显示清晰;1g~1i为连续3个层面的120 mA常规剂量CT图像。
表 1 低剂量RG PET/CT与常规剂量PET/CT的辐射剂量结果(x±s)
CT剂量类型
(1个PET床位)例数 有效吸收剂量
(mSv)剂量长度乘积
(mGy·cm)30 mA低剂量RG PET/CT 26 5.68±0.83 333.95±48.58 250~350 mA常规剂量PET/CT 3 6.73±1.13 395.64±65.94 120 mA常规剂量PET/CT 26 1.68±0.73 99.03±43.15  下载: 导出CSV
下载: 导出CSV
表 2 低剂量CT与常规剂量CT图像质量比较(x±s)
CT剂量类型 例数 均匀性(HU) 噪声(HU) 30 mA低剂量CT 10 0.34±0.21 21.65±0.83 120 mA常规剂量CT 10 0.29±0.17 8.38±1.46
下载: 导出CSV
表 3 呼吸周期与辐射剂量关系的模拟结果
呼吸周期(s) 电影持续时间(s) CT容积剂量指数(mGy) 剂量长度乘积(mGy·cm) 0.5 1.5 3.94 63.03 1.0 2.0 5.25 84.04 1.5 2.5 6.57 105.05 2.0 3.0 7.88 126.06 2.5 3.5 9.19 147.07 3.0 4.0 10.50 168.07 3.5 4.5 11.82 189.08 4.0 5.0 13.13 210.09 4.5 5.5 14.44 231.10 5.0 6.0 15.76 252.11 5.5 6.5 17.07 273.12 6.0 7.0 18.38 294.13 6.5 7.5 19.70 315.14 7.0 8.0 21.01 336.15 7.5 8.5 22.32 357.16 8.0 9.0 23.64 378.17
下载: 导出CSV
-
[1] Guerra L, De Ponti E, Elisei F, et al. Respiratory gated PET/CT in a European multicentre retrospective study: added diagnostic value in detection and characterization of lung lesions. Eur J Nucl Med Mol Imaging, 2012, 39(9):1381-1390. doi: 10.1007/s00259-012-2148-2 [2] van Elmpt W, Hamill J, Jones J, et al. Optimal gating compared to 3D and 4D PET reconstruction for characterization of lung tumours. Eur J Nucl Med Mol Imaging, 2011, 38(5):843-855. doi: 10.1007/s00259-010-1716-6 [3] Prokop M. Radiation dose in computed tomography. Risks and challenges. Radiology, 2008, 48(3):229-242. [4] Cohen MD. Pediatric CT radiation dose: how low can you go?. AJR Am J Roentgenol, 2009, 192(5):1292-1303. doi: 10.2214/AJR.08.2174 [5] McCollough CH, Primak AN, Braun N, et al. Strategies for reducing radiation dose in CT. Radiol Clin North Am, 2009, 47(1):27-40. doi: 10.1016/j.rcl.2008.10.006 [6] 武志芳, 李思进, 刘建忠, 等.呼吸门控PET/CT对肺部结节SUV的影响.中华核医学与分子影像杂志, 2012, 32(2):111-114. doi: 10.3760/cma.j.issn.2095-2848.2012.02.007
[7] 樊卫, 张伟光, 杨小春. PET/CT呼吸门控技术及其应用介绍.中华核医学杂志, 2007, 27(2):126-128. doi: 10.3760/cma.j.issn.2095-2848.2007.02.028
[8] Li T, Schreibmann E, Thorndyke B, et al. Radiation dose reduction in four-dimensional computed tomography. Med Phys, 2005, 32(12):3650-3660. doi: 10.1118/1.2122567 [9] Hara R, Itami J, Kondo T, et al. Stereotactic single high dose irradiation of lung tumors under respiratory gating. Radiother Oncol, 2002, 63(2):159-163. [10] Pan T, Mawlawi O, Nehmeh SA, et al. Attenuation correction of PET images with respiration-averaged CT images in PET/CT. J Nucl Med, 2005, 40:1481-1487. [11] 北京市计量科学研究所, 首都医科大学医学仪器质量控制技术研究中心. JJG 961-2001医用诊断计算机断层摄影装置(CT)X射线辐射源检定规程.北京: 中国计量出版社, 2001.
[12] Chang G, Chang T, Pan T, et al. Implementation of an automated respiratory amplitude gating technique for PET/CT:clinical evaluation. J Nucl Med, 2010, 51(1):16-24. [13] Lamb JM, Robinson C, Bradley J, et al. Generating lung tumor internal target volumes from 4D-PET maximum intensity projections. Med Phys, 2011, 38(10):5732-5737. doi: 10.1118/1.3633896 [14] Kasuya T, Tateishi U, Suzuki K, et al. Role of respiratory-gated PET/CT for pancreatic tumors: a preliminary result. Eur J Radiol, 2013, 82(1):69-74. doi: 10.1016/j.ejrad.2012.05.037 [15] Suenaga Y, Kitajima K, Aoki H, et al. Respiratory-gated 18F-FDG PET/CT for the diagnosis of liver metastasis. Eur J Radiol, 2013, 82(10):1696-1701. doi: 10.1016/j.ejrad.2013.05.019 [16] Wu A, Zheng H, Kraenzle J, et al. Ferret thoracic anatomy by 2-deoxy-2-(18F)fluoro-D-glucose(18F-FDG) positron emission tomography/computed tomography(18F-FDG PET/CT) imaging. ILAR J, 2012, 53(1):9-21. doi: 10.1093/ilar.53.1.9 [17] 黎喜, 谢增海, 罗慧.低剂量(30 mA)胸部螺旋CT扫描的效果观察.广东医学院学报, 2006, 24(1):39-40. doi: 10.3969/j.issn.1005-4057.2006.01.021
[18] 孔秋雁, 陈廷港, 许崇永, 等.多排螺旋CT低剂量扫描在小儿胸部的应用.实用放射学杂志, 2007, 23(6):792-794. doi: 10.3969/j.issn.1002-1671.2007.06.023
[19] 殷瑞根, 王冬青, 赵亮, 等.多层螺旋CT肺部低剂量扫描的参数优化.实用放射学杂志, 2004, 20(8):694-697. doi: 10.3969/j.issn.1002-1671.2004.08.008
[20] Karabulut N, Törü M, Gelebek V, et al. Comparison of low-dose and standard-dose helical CT in the evaluation of pulmonary nodules. Eur Radiol, 2002, 12(11):2764-2769. doi: 10.1007/s00330-002-1368-4 [21] Zhu X, Yu J, Huang Z. Low-dose chest CT: optimizing radiation protection for patients. AJR Am J Roentgenol, 2004, 183(3):809-816. doi: 10.2214/ajr.183.3.1830809 [22] Wormanns D, Ludwig K, Beyer F, et al. Detection of pulmonary nodules at multirow-detector CT: effectiveness of double reading to improve sensitivity at standard-dose and low-dose chest CT. Eur Radiol, 2005, 15(1):14-22. [23] Das M, Mühlenbruch G, Heinen S, et al. Performance evaluation of a computer-aided detection algorithm for solid pulmonary nodules in low-dose and standard-dose MDCT chest examinations and its influence on radiologists. Br J Radiol, 2008, 81(971):841-847. doi: 10.1259/bjr/50635688 [24] Christe A, Torrente JC, Lin M, et al. CT Screening and follow-up of lung nodules: effects of tube current-time setting and nodule size and density on detectability and of tube current-time setting on apparent size. AJR Am J Roentgenol, 2011, 197(3):623-630. doi: 10.2214/AJR.10.5288 [25] Zhu Zhiyu, Tsui BMW, Segars WP. A Simulation Study of the Effect of Gating Scheme on respiratory Motion Blurring in FDG lung PET. IEEE Transactions on Nuclear Science, 2003, 13(3):1554-1558. [26] 黄明刚, 郭佑民, 郑桂芳, 等.早期肺癌低剂量CT检测的技术优化与应用.实用放射学杂志, 2011, 27(8):1263-1268. doi: 10.3969/j.issn.1002-1671.2011.08.039
[27] 刘彬, 白玫. 64层螺旋CT检查中患者受照剂量的研究.中华放射学杂志, 2008, 42(10):1050-1052. doi: 10.3321/j.issn:1005-1201.2008.10.010
-

 点击查看大图
点击查看大图
图(1)表(3)
计量
- 文章访问数: 2761
- HTML全文浏览量: 1255
- PDF下载量: 3