


-
乳腺癌是女性最常见的恶性肿瘤之一,雌激素受体(estrogen receptor,ER)是乳腺癌发生和发展最为重要的生物标志物,也是乳腺癌预后的相关因素。ER能够与乳腺癌细胞表面受体结合从而监测乳腺癌组织中相关受体的分布和浓度,在肿瘤的诊断、分期、疗效判断和观察中具有重要意义。功能分子影像学方法和其他诊断技术相比具有高灵敏度、高特异度的特点,在乳腺癌诊疗中的应用日益增多,但常规显像剂18F-FDG作为葡萄糖的衍生物,仅能反映肿瘤细胞的糖代谢,无法判断ER的表达情况。16α-[18F]氟-17β-雌二醇(16α-[18F]fluoro-17β-estradiol,18F-FES)作为ER的特异性显像剂,可在活体内反映ER的表达情况,从而指导临床选择个性化的治疗方案[1-2]。本研究采用18F-FES和18F-FDG PET/CT联合显像对乳腺癌进行特异性诊断。
-
收集2010年12月至2012年9月经我院临床最终病理证实的乳腺癌术前患者19例和乳腺癌术后转移患者7例,共26例,年龄24~83岁,中位年龄51岁。其中,浸润性导管癌19例、导管原位癌2例、细胞型黏液癌2例、恶性上皮性肿瘤3例。所有病理标本均行免疫组化测定肿瘤细胞的ER阳性百分数及染色强度。所有患者均行全身18F-FDG、18F-FES PET/CT双显像剂显像;7例患者经超声引导下乳腺病灶或腋窝淋巴结穿刺活检病理证实,其余患者经手术病理症实。
-
Discovery LS16型PET/CT仪由美国GE公司生产;18F由美国GE公司MINItrace加速器生产,显像剂18F-FDG、18F-FES由我科合成(采用美国GE公司Microlab全自动合成系统),放射化学纯度均 > 95%。新型PET/CT显像剂18F-FES经我院伦理委员会验证并批准使用,患者检查前均签署了知情同意书。
-
患者行18F-FDG PET/CT检查前空腹6 h以上,平静休息10~15 min,测定血糖浓度在正常范围内,18F-FDG按照4.44 MBq/kg经肘静脉注射,安静休息50~60 min后开始采集图像,患者仰卧于检查床上,先行16层螺旋CT扫描,CT扫描参数为:管电压120 kV,管电流100~130 mA,扫描层厚5 mm,进床速度27 mm/0.8 s,PET采用二维扫描,采集6~8个床位,4 min/床位,图像重建采用有序子集最大期望值迭代法。CT数据采用512×512矩阵,4.25 mm层厚标准算法无间隔重建,通过Xeleris工作站进行图像融合,分别得到横断面、矢状面及冠状面的CT、PET图像和PET/CT融合断层图像。18F-FES PET/CT检查前患者无需禁食,按18F-FDG相同注射剂量经肘静脉注射,其他条件同18F-FDG PET/CT。所有患者均在一周内完成18F-FDG、18F-FES PET/CT显像。
-
以病灶放射性分布较邻近组织结构高且呈结节状、团块状放射性异常浓聚者判断为阳性,由我科3位医师独立阅片。
-
选择病灶放射性浓聚程度最高的层面,勾画感兴趣区,自动测量最大标准化摄取值(maximum standardized uptake value,SUVmax),18F-FDG SUVmax大于2.5判断为阳性,18F-FES SUVmax大于1.0判断为阳性[3]。
-
采用SPSS 14.0软件进行统计学分析,SUVmax采用x±s表示,组间比较采用t检验。P < 0.05为差异有统计学意义。
-
在19例乳腺癌术前患者中,ER阳性者9例,共10个病灶,18F-FES SUVmax与病灶的ER表达水平及病灶大小均密切相关(图 1),如其中1个ER低表达[15%(+)]的较大病灶(2.0 cm×3.0 cm),18F-FES SUVmax为1.1,18F-FDG SUVmax为3.7;1个ER高表达[90%(+++)]的小病灶(1.0 cm×1.1 cm),18F-FES SUVmax为1.7,18F-FDG SUVmax为2.5。10个病灶的放射性分布情况、病灶大小及ER表达水平见表 1。

图 1 患者79岁,左乳外下象限浸润性导管癌,ER[90%(+++)]。图中,1a、1b:18F-FES显像的PET/CT融合图像和最大密度投影图像;1c、1d:18F-FDG显像的PET/CT融合图像和最大密度投影图像;示病灶(十字交叉处)大小约3.0 cm×3.0 cm,18F-FDG、18F-FES显像均呈放射性异常浓聚,18F-FES SUVmax为5.6,18F-FDG SUVmax为15.0;其中,ER:雌激素受体,18F-FES:16α-[18F]氟-17β-雌二醇,SUVmax:最大标准化摄取值。
病灶ER表达水平 15%
(+)75%
(++)80%
(+++)80%
(+++)80%
(++)80%
(++)80%
(++)80%
(++)90%
(+++)90%
(+++)18F-FES SUVmax 1.1 2.8 1.1 3.3 2.6 4.4 3.1 8.8 1.7 5.6 18F-FDG SUVmax 3.7 5.9 5.1 10.5 7.0 3.5 3.7 12.3 2.5 15.0 病灶大小(cm2) 2.0×3.0 2.9×7.0 1.0×1.0 2.5×3.0 1.6×2.2 1.5×2.6 5.0×5.0 2.6×2.8 1.0×1.1 3.0×3.0 注:表中,ER:雌激素受体;18F-FES:16α-[18F]氟-17β-雌二醇;SUVmax:最大标准化摄取值。 表 1 ER阳性原发灶ER表达水平、病灶大小与18F-FES及18F-FDG显像SUVmax的关系
19例乳腺癌术前患者中,ER阳性表达病灶的18F-FES显像的放射性分布显著高于ER阴性表达病灶(t=3.782,P < 0.01)和健侧乳腺腺体(t=5.678,P < 0.01),而ER阳性表达病灶和阴性表达病灶的18F-FDG显像均表现为明显的放射性异常浓聚,两者间SUVmax差异无统计学意义(t=0.483,P > 0.05)(表 2)。
个数 18F-FES
显像SUVmax18F-FDG
显像SUVmax乳腺癌原发灶 ER阳性病灶 10 3.45±2.34 6.90±4.28 ER阴性病灶 11 0.74±0.12 8.02±5.27 健侧乳腺腺体 19 0.64±0.15 1.56±0.61 注:表中,健侧乳腺腺体对应个数为患者例数;ER:雌激素受体;18F-FES:16α-[18F]氟-17β-雌二醇;SUVmax:最大标准化摄取值。 表 2 乳腺癌原发灶与健侧乳腺腺体18F-FES SUVmax、18F-FDG SUVmax的对比
-
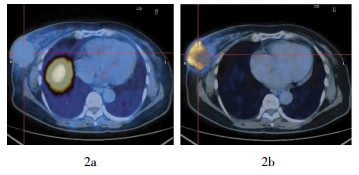
在19例乳腺癌术前患者中,ER阴性者10例,共11个病灶,18F-FES SUVmax为0.3~1.2,18F-FDG SUVmax为2.6~17.8,病灶最大约6.0 cm×7.1 cm,最小约0.9 cm×1.1 cm。ER阴性病灶18F-FES显像的放射性分布与健侧乳腺腺体相近(图 2),两者间SUVmax差异无统计学意义(t=0.872,P > 0.05)。其中1例18F-FES显像假阳性患者的CT表现为右侧乳腺巨大软组织密度肿块影,大小约6.0 cm×7.1 cm,18F-FES有轻度放射性摄取,SUVmax为1.2,18F-FDG有明显放射性异常浓聚,SUVmax为8.6,考虑为乳腺癌雌二醇受体低表达,病理诊断为浸润性导管癌,ER阴性。

图 2 患者69岁,右乳腺浸润性导管癌伴右侧腋窝、右锁骨上多发淋巴结转移,ER阴性,右乳外下象限病灶(十字交叉处)大小约5.3 cm×5.4 cm。图中,2a:18F-FES PET/CT显像放射性分布未见增高,SUVmax为0.7;2b:18F-FDG PET/CT显像示放射性异常浓聚,SUVmax为5.6;其中,ER:雌激素受体;18F-FES:16α-[18F]氟-17β-雌二醇;SUVmax:最大标准化摄取值。
-
18F-FES PET/CT诊断乳腺癌原发灶ER阳性的准确率、灵敏度、特异度、阳性预测值、阴性预测值分别为:95.23%、100%、90.90%、90.90%和100%。
-
在7例乳腺癌术后转移患者中,乳腺癌ER阳性患者3例,18F-FES PET/CT共发现64个转移灶(内分泌治疗后患者转移灶另计),最大约2.0 cm×2.8 cm,最小约0.5 cm×0.7 cm,18F-FES SUVmax为1.8~11.5。18F-FDG PET/CT共发现47个转移灶,最大约2.0 cm×2.8 cm,最小约0.7 cm×0.7 cm,18F-FDG SUVmax为2.5~12.3。18F-FES、18F-FDG PET/CT检查均为假阴性者2例,手术病理示该2例为腋窝淋巴结转移,病灶大小约0.5 cm×0.5 cm,ER[80%(++)]。18F-FDG PET/CT检查有1例假阳性,左侧乳腺浸润性导管癌术后半年,ER[90%(+++)],18F-FDG PET/CT检查发现右侧股骨上段放射性异常浓聚灶,大小约3.0 cm×6.0 cm,考虑骨转移瘤可能,18F-FES PET/CT检查未见放射性摄取,结合乳腺癌原发灶ER高表达提示为股骨原发性病灶,手术病理证实为骨纤维异常增殖症。
在7例乳腺癌术后转移患者中,乳腺癌ER阴性患者4例,18F-FDG PET/CT共发现51个转移灶,最大约2.4 cm×4.7 cm,18F-FDG SUVmax为2.5~5.9,18F-FES PET/CT相应部位放射性摄取未见明显增高。
-
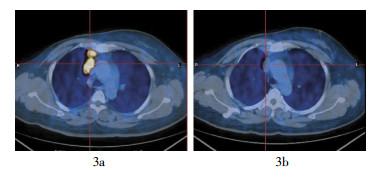
3例乳腺癌术后复查患者,ER[90%(++~+++)],18F-FES PET/CT显像发现全身多发转移,治疗前检查共发现23个转移灶,分布于锁骨上、内乳区、纵隔、下肺静脉旁淋巴结以及肺部、胸膜、骨盆等,病灶最大为1.9 cm×2.8 cm,SUVmax为2.2~11.5。口服抗雌激素(他莫昔芬)治疗1~3个月后复查,其中7个病灶消失,另外16个病灶均有不同程度变小,放射性摄取降低,SUVmax为1.1~2.9(图 3)。

图 3 患者53岁,右乳外下象限浸润性导管癌术后,前上纵隔淋巴结转移,ER[90%(+++)]。图中,3a:内分泌治疗前18F-FES PET/CT显像,病灶(十字交叉处)大小约1.7 cm×2.6 cm,SUVmax为11.5;3b:内分泌治疗后18F-FES PET/CT显像,治疗1个月后病灶明显变小,大小约1.0 cm×1.8 cm,放射性摄取降低,SUVmax为1.9;其中,ER:雌激素受体,18F-FES:16α-[18F]氟-17β-雌二醇,SUVmax:最大标准化摄取值。
-
目前,临床上主要采用免疫组化法检测ER,需有创性地获取肿瘤组织,测定状态受组织离体的局限,其反映的是所取病灶部位ER的免疫活性,并不一定能表现出该部位ER的生物学活性,更不能完全代表全身其他病灶ER的生物学活性。18F-FES是一种雌激素的类似物,能够特异性地和ER结合,18F-FES PET/CT可以无创、灵敏、准确地对原发灶和转移灶同时进行显像,反映的是病灶有功能的ER(即ER的生物学活性);同时,18F-FES PET/CT还可以对受体水平进行定量分析,为临床提供乳腺癌组织及转移灶内癌细胞的ER的分布、密度变化及活动状态等方面的信息。
本研究中乳腺癌原发灶ER阳性患者18F-FES PET/CT检查结果与病理结果基本一致;病灶放射性摄取值同ER表达水平呈正相关,与病灶大小也密切相关,病理ER表达水平相同的患者,1 cm以下的病灶SUVmax明显较低。1例局部晚期乳腺癌患者手术标本经免疫组化法检测为ER阴性,而18F-FES半定量分析为阳性,SUVmax为1.2,可能由于肿瘤的异质性、取材误差或出血、坏死,免疫组化法检测有时不能真正反映肿瘤的ER状态而致假阴性,或该病灶的某种生物学活性尚未能被现有的免疫组化技术所检测。
对乳腺癌ER阳性转移灶的诊断,18F-FES显像明显优于18F-FDG,而且18F-FES具有特异性诊断的意义。但对于小于0.5 cm的淋巴结转移灶,由于仪器分辨率的原因,18F-FES也可能造成假阴性。本研究中ER阴性患者18F-FES SUVmax显著低于ER阳性患者;而18F-FDG SUVmax与病灶ER的表达与否无关,因此对于ER阴性的原发灶及转移灶,18F-FES检测有明显的局限性,18F-FES PET/CT检查只对乳腺癌ER高表达患者具有特异性,不能完全取代18F-FDG PET/CT。
18F-FES、18F-FDG PET/CT显像可以对ER的表达水平以及病灶的代谢水平等进行评价,能更灵敏和准确地体现出治疗后的反应程度[4]。雌激素拮抗剂能特异性地与ER结合,使18F-FES与ER的结合减少。本研究中3例ER阳性患者接受口服抗雌激素治疗后行18F-FES PET/CT检查,发现病灶变少、变小,放射性摄取明显降低,提示内分泌治疗有效。有学者研究发现,ER阳性乳腺癌治疗前18F-FES摄取水平与随后6个月内分泌治疗的疗效密切相关,以治疗前18F-FES SUVmax=2.0为界,对治疗有效的预测值分别为79%和88%,而SUVmax < 1.5时内分泌治疗的效果较差[5]。故18F-FES PET/CT有助于对内分泌治疗疗效的预测,对治疗的决策具有重要意义[6-7]。本研究对3例ER高表达患者进行了他莫昔芬治疗前后的18F-FES显像,表明疗效与SUV的降低相关,但由于观察例数有限未行统计学分析。乳腺癌ER的表达情况、18F-FES SUV与内分泌治疗疗效的相关性以及疗效的其他影响因素有待于进一步的研究。
18F-FES PET/CT是一种无创的检查方法,作为一种在活体内对肿瘤ER的生物学活性的检测技术,主要应用于ER阳性的乳腺癌患者,对于子宫内膜癌等其他ER阳性患者的显像亦有报道[8],18F-FES是目前具有发展前景的显像剂,其对ER阳性乳腺癌的特异性诊断、个性化治疗方案的制定、疗效观察具有非常重要的临床意义。
18F-FES PET/CT显像在雌激素受体阳性乳腺癌诊疗中的初步应用
Application of 18F-FES PET/CT in diagnosis and endocrine therapy of patients with estrogen receptor-positive breast cancer
-
摘要:
目的 探讨16α-[18F]氟-17β-雌二醇(18F-FES)PET/CT显像在乳腺癌诊疗中的应用价值。 方法 对19例乳腺癌术前患者、7例乳腺癌术后转移患者行18F-FDG、18F-FES PET双显像剂显像,并与雌激素受体(ER)的表达情况进行对照分析。 结果 19例乳腺癌术前患者中,乳腺癌原发灶ER阳性者9例,共10个病灶,18F-FES最大标准化摄取值(SUVmax)为3.45±2.34,与病灶的ER表达水平及病灶大小均密切相关;ER阴性者10例,共11个病灶,18F-FES SUVmax为0.74±0.12,两组间差异有统计学意义(t=3.782,P < 0.01)。而ER阳性者和阴性者的18F-FDG SUVmax与病灶的ER表达水平无关。18F-FES PET/CT诊断原发灶ER阳性的灵敏度、特异度、准确率分别为100%、90.90%、95.23%。在7例术后转移患者中,原发灶ER阳性者3例,18F-FES共发现64个转移灶,而18F-FDG仅发现47个。 结论 18F-FES PET/CT在ER阳性乳腺癌的特异性诊断、个性化治疗方案制定、疗效观察中具有非常重要的临床意义。 -
关键词:
- 受体,雌激素 /
- 乳腺肿瘤 /
- 雌二醇 /
- 氟脱氧葡萄糖F18 /
- 正电子发射断层显像术 /
- 体层摄影术,X线计算机
Abstract:Objective To evaluate the role of 16α-[18F]fluoro-17β-oestradiol(18F-FES)PET/CT in the diagnosis and management of breast cancer. Methods Nineteen pre-operation cases with breast cancer and 7 post-operation cases with metastatic breast cancer underwent 18F-FES PET/CT and 18F-FDG PET/CT, and comparative analysis with the expression of estrogen receptor(ER)was performed. Results Of the primary lesions, the ER was positive in 9 patients(10 lesions), negative in 10 patients(11 lesions). The maximum standardized uptake value(SUVmax) for FES uptake was positively related to the lesion size and ER expression. The mean SUVmax for FES uptake was 3.45±2.34 in the 10 ER positive tumors, and 0.74±0.12 in the 11 ER negative tumors, which showed significant differences between the two groups(t=3.782, P < 0.01). The sensitivity, specificity and accuracy of FES PET for diagnosis ER positive patients were 100%, 90.90% and 95.23% respectively. Sixty-four 18F-FES positive metastases were found in the three ER positive metastatic patients, whereas only 47 18F-FDG positive metastases were found. Conclusion 18F-FES PET/CT will be useful for diagnosis, individualized medicine and detecting therapeutic changes in patients with ER positive breast cancer. -
图 1 患者79岁,左乳外下象限浸润性导管癌,ER[90%(+++)]。图中,1a、1b:18F-FES显像的PET/CT融合图像和最大密度投影图像;1c、1d:18F-FDG显像的PET/CT融合图像和最大密度投影图像;示病灶(十字交叉处)大小约3.0 cm×3.0 cm,18F-FDG、18F-FES显像均呈放射性异常浓聚,18F-FES SUVmax为5.6,18F-FDG SUVmax为15.0;其中,ER:雌激素受体,18F-FES:16α-[18F]氟-17β-雌二醇,SUVmax:最大标准化摄取值。
图 2 患者69岁,右乳腺浸润性导管癌伴右侧腋窝、右锁骨上多发淋巴结转移,ER阴性,右乳外下象限病灶(十字交叉处)大小约5.3 cm×5.4 cm。图中,2a:18F-FES PET/CT显像放射性分布未见增高,SUVmax为0.7;2b:18F-FDG PET/CT显像示放射性异常浓聚,SUVmax为5.6;其中,ER:雌激素受体;18F-FES:16α-[18F]氟-17β-雌二醇;SUVmax:最大标准化摄取值。
图 3 患者53岁,右乳外下象限浸润性导管癌术后,前上纵隔淋巴结转移,ER[90%(+++)]。图中,3a:内分泌治疗前18F-FES PET/CT显像,病灶(十字交叉处)大小约1.7 cm×2.6 cm,SUVmax为11.5;3b:内分泌治疗后18F-FES PET/CT显像,治疗1个月后病灶明显变小,大小约1.0 cm×1.8 cm,放射性摄取降低,SUVmax为1.9;其中,ER:雌激素受体,18F-FES:16α-[18F]氟-17β-雌二醇,SUVmax:最大标准化摄取值。
表 1 ER阳性原发灶ER表达水平、病灶大小与18F-FES及18F-FDG显像SUVmax的关系
病灶ER表达水平 15%
(+)75%
(++)80%
(+++)80%
(+++)80%
(++)80%
(++)80%
(++)80%
(++)90%
(+++)90%
(+++)18F-FES SUVmax 1.1 2.8 1.1 3.3 2.6 4.4 3.1 8.8 1.7 5.6 18F-FDG SUVmax 3.7 5.9 5.1 10.5 7.0 3.5 3.7 12.3 2.5 15.0 病灶大小(cm2) 2.0×3.0 2.9×7.0 1.0×1.0 2.5×3.0 1.6×2.2 1.5×2.6 5.0×5.0 2.6×2.8 1.0×1.1 3.0×3.0 注:表中,ER:雌激素受体;18F-FES:16α-[18F]氟-17β-雌二醇;SUVmax:最大标准化摄取值。  下载: 导出CSV
下载: 导出CSV
表 2 乳腺癌原发灶与健侧乳腺腺体18F-FES SUVmax、18F-FDG SUVmax的对比
个数 18F-FES
显像SUVmax18F-FDG
显像SUVmax乳腺癌原发灶 ER阳性病灶 10 3.45±2.34 6.90±4.28 ER阴性病灶 11 0.74±0.12 8.02±5.27 健侧乳腺腺体 19 0.64±0.15 1.56±0.61 注:表中,健侧乳腺腺体对应个数为患者例数;ER:雌激素受体;18F-FES:16α-[18F]氟-17β-雌二醇;SUVmax:最大标准化摄取值。
下载: 导出CSV
-
[1] Hospers GA, Helmond FA, de Vries EG, et al. PET imaging of steroid receptor expression in breast and prostate cancer. Curr Pharm Des, 2008, 14(28): 3020-3032. doi: 10.2174/138161208786404362 [2] Kumar P, Mercer J, Doerkson C, et al. Clinical production, stability studies and PET imaging with 16-alpha-[18F]-fluoroestradiol([18F]-FES) in ER positive breast cancer patients. J Pharm Pharm Sci, 2007, 10(2): 256s-265s. [3] Mortimer JE, Dehdashti F, Siegel BA, et al. Positron emission tomography with 2-[18F]Fluoro-2-deoxy-D-glucose and 16α-[18F]-17β-estradiol in breast cancer: correlation with estrogen receptor status and response to systemic therapy. Clin Cancer Res, 1996, 2(6): 933- 939. [4] Eubank WB, Mankoff DA. Evolving role of positron emission tomography in breast cancer imaging. Semin Nucl Med, 2005, 35(2): 84-99. doi: 10.1053/j.semnuclmed.2004.11.001 [5] Linden HM, Stekhova SA, Link JM, et al. Quantitative fluoroestradiol positron emission tomography imaging predicts response to endocrine treatment in breast cancer. J Clin Oncol, 2006, 24(18): 2793-2799. doi: 10.1200/JCO.2005.04.3810 [6] Linden HM, Kurland BF, Peterson LM, et al. Fluoroestradiol positron emission tomography reveals differences in pharmacodynamics of aromatase inhibitors, tamoxifen, and fulvestrant in patients with metastatic breast cancer. Clin Cancer Res, 2011, 17(14): 4799-4805. doi: 10.1158/1078-0432.CCR-10-3321 [7] van Kruchten M, Glaudemans AW, de Vries EF, et al. PET imaging of estrogen receptors as a diagnostic tool for breast cancer patients presenting with a clinical dilemma. J Nucl Med, 2012, 53(2): 182-190. [8] Tsujikawa T, Yoshida Y, Kudo T, et al. Functional images reflect aggressiveness of endometrial carcinoma: estrogen receptor expression combined with 18F-FDG PET. J Nucl Med, 2009, 50(10): 1598-1604. doi: 10.2967/jnumed.108.060145 -

 点击查看大图
点击查看大图

计量
- 文章访问数: 2511
- HTML全文浏览量: 1167
- PDF下载量: 3