



-
18F-FDG PET/CT分子影像学技术是肺癌临床早期诊断和分期中最重要的无创性医学影像学工具。但是,18F-FDG在人体内的生理代谢和在肿瘤组织细胞中的代谢具有明显的特殊性,且18F-FDG PET/CT显像过程受到众多因素的影响,因此,18F-FDG PET/CT图像中的SUV只能作为一个半定量诊断指标而被临床使用[1]。这明显限制了18F-FDG PET/CT定量化研究在指导肿瘤个性化治疗中的临床应用。本研究回顾性分析了影响18F-FDG PET/CT临床显像的3个因素:患者体重、血糖浓度和病灶大小,探讨其对SUV影响的程度,试图为18F-FDG PET/CT定量化分析建立模型[2-4]。
-
选取2009年至2011年在新疆维吾尔自治区人民医院行18F-FDG PET/CT显像的肺癌患者50例,其中,男性37例、女性13例。患者平均年龄为(65.1±10.3)岁,平均体重为(64.7±10.3)kg、平均身高为(166.5±7.2)cm。50例患者均无糖尿病病史,患者血糖浓度为(6.31±0.95)mmol/L。所有患者均经明确的临床病理确诊(5例为经皮穿刺活检病理确诊、18例为手术后病理确诊、27例为支气管镜活检病理确诊),按2004年版世界卫生组织恶性上皮肺肿瘤分类标准[5],其中,肺大细胞癌2例、肺小细胞癌5例、肺腺癌20例、肺鳞状细胞癌23例。50例肺癌患者中,21例患者有纵隔转移灶。所有肺癌患者均未经过放射治疗或化学药物治疗。50例肺癌患者均采用CT图像测量原发病灶的直径,平均直径为(47.54±24.48)mm,21例肺癌患者纵隔转移灶的平均直径为(22.57±9.78)mm。所有患者均于检查前签署了知情同意书。
-
18F-FDG由美国GE公司的MiniTrace和TraceLab FXFDG制备,放化纯度>99%。Discovery PET/CT仪由美国GE公司生产。
-
检查前患者禁食6 h,禁止使用镇静药物,测量血糖浓度后安静休息。按4.44 MBq/kg依次静脉注射18F-FDG,随后,患者在暗室静息状态下平卧60 min,排尿后行18F-FDG PET/CT显像,每床位扫描1.5 min,CT参数:管电压120 kV,管电流30~210 mA,层厚3.75 mm,并根据扫描部位厚度及密度进行管电流实时动态自动调节。图像均选择重建PET图像。
-
采用GE Advantage Workstation图像处理工作站处理图像。使用GE公司提供的PET容积计算机辅助诊断(volume computer-assisted reading,VCAR)对肺结节进行定量处理。采用全自动一键式获得病灶的SUV和瘦体标准化摄取值(standardized uptake value normalized to lean body mass,SUL),包括平均标准化摄取值(mean standardized uptake value,SUVmean)和平均瘦体标准化摄取值(mean standardized uptake value normalized to lean body mass,SUL mean)、最大标准化摄取值(maximum standardized uptake value, SUVmax)和最大瘦体标准化摄取值(maximum standardized uptake value normalized to lean body mass, SULmax)、SUV标准差、SUL标准差及病灶大小[6]。在肝脏右下叶(避开肝脏的血管和肝管道系统)选择直径3 cm的ROI作为肝脏参考本底的部位,分别计算肝脏参考本底ROI的SUV和SUL,其中,SUV计算公式为:SUV=每克组织的平均放射性活度(Bq/g)/{注射的放射性活度(Bq)/[体重(kg)·身高(m)2]}。
PET/CT图像肺癌原发灶和转移灶诊断参考标准按照肝脏参考本底SUV或体型校正SUV×1.5+2×标准差。为了研究血糖浓度对SUV和SUL的影响,需进一步按照患者血糖浓度对SUV和SUL进行校正,即校正后的SUV和SUL等于血糖浓度分别乘以SUV和SUL;计算所有原发灶和转移灶病灶大小与病灶SUV和SUL的相关性,并进行回归计算以便获得他们之间的相关回归公式;利用回归公式对不同大小病灶的SUV和SUL进行校正。
-
采用MinTab 1.2统计学软件对数据进行统计学分析,计量资料采用均数±标准差(x±s)表示;两组计量资料的比较使用t检验;P < 0.05为差异有统计学意义。
-
图 1和图 2为肺癌及肺癌伴纵隔肺门淋巴结转移患者的PET/CT影像学表现,均由术后病理证实。

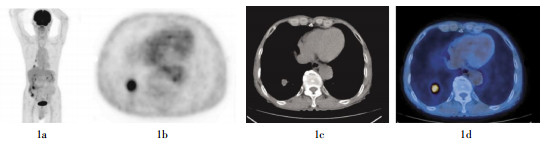
图 1 患者男性,73岁,肺癌无纵隔肺门淋巴结转移。图中1a、1b:患者体部冠状面及横断面PET图像,示右肺下叶结节样高代谢病灶,考虑肺癌;1c、1d:患者胸部横断面CT图像与PET/CT融合图像,示右肺下叶结节样高代谢病灶,CT与相应部位见分叶状软组织密度肿块影。术后病理示为低分化腺癌。

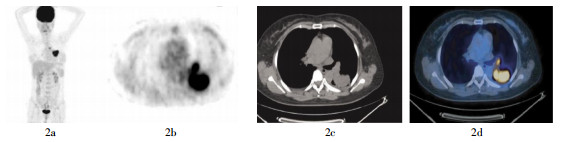
图 2 患者女性,47岁,肺癌伴纵隔肺门淋巴结转移。图中,2a、2b:患者体部冠状面及横断面PET图像,示左肺下叶处高代谢病灶,考虑肺癌,纵隔及左侧肺门结节状高代谢病灶,考虑纵隔及肺门淋巴结转移癌;2c、2d:患者胸部横断面CT图像与PET/CT融合图像,示左肺下叶背段块状高代谢病灶,CT与相应部位可见形态不规则分叶状软组织密度肿块影,考虑肺癌。纵隔及左侧肺门可见结节状高代谢病灶,CT与相应部位可见肿大淋巴结影,考虑淋巴结转移癌。术后病理检查示为中分化腺癌,伴有纵隔及肺门淋巴结腺癌转移。
-
从不同病理类型肺癌患者的原发灶和转移灶的统计结果可以看出,不同类型肺癌患者肝脏参考本底SUVmean、SULmean均小于SUVmax、SULmax(表 1)。并且,SUVmean与SULmean以及SUVmax与SULmax之间的相关系数分别为0.98,P < 0.01和0.99,P < 0.001。原发灶直径的平均值比转移灶大2倍。
病理类型 病灶大小(mm) SUVmean SUVmax SUV标准差 SULmean SULmax SUL标准差 大细胞癌 肝脏参考部位(n=2) - 2.66±0.74 2.89±0.59 0.26±0.11 2.09±0.49 2.24±0.43 0.20±0.10 原发灶(n=2) 20.50±6.36 7.10±0.23 9.41±0.99 2.02±0.07 6.3±0.83 7.41±1.09 0.97±0.10 转移灶(n=1) 23.00 9.24 10.26 - 7.50 8.91 - 小细胞癌 肝脏参考部位(n=5) - 2.84±0.42 3.13±0.48 0.14±0.04 2.17±0.13 2.39±0.18 0.11±0.03 原发灶(n=5) 44.20±13.97 10.26±5.24 12.30±6.38 1.68±0.86 7.94±4.33 9.34±4.75 1.01±0.71 转移灶(n=5) 17.20±3.49 5.19±2.29 6.38±2.91 1.31±0.99 4.20±2.07 5.01±2.43 0.92±0.65 腺癌 肝脏参考部位(n=20) - 2.54±0.52 2.84±0.64 0.21±0.10 1.91±0.40 2.14±0.39 0.18±0.10 原发灶(n=20) 40.05±19.66 8.19±3.69 9.80±3.94 1.47±0.65 6.39±2.93 7.48±3.46 1.09±0.55 转移灶(n=7) 20.71±5.31 7.18±3.35 8.13±3.35 0.86±0.38 5.51±2.98 6.19±3.18 0.69±0.24 鳞状细胞癌 肝脏参考部位(n=23) - 2.56±0.37 2.81±0.40 0.27±0.09 2.09±0.28 2.32±0.29 0.17±0.05 原发灶(n=23) 57.13±27.34 12.27±4.16 15.02±4.58 2.44±0.88 9.69±2.89 12.08±3.59 1.88±0.85 转移灶(n=8) 27.50±13.78 6.67±1.96 8.27±2.69 1.32±0.65 5.58±1.84 6.63±2.23 1.10±0.55 合计 肝脏参考部位(n=50) - 2.59±0.45 2.86±0.51 0.23±0.10 2.03±0.33 2.25±0.34 0.19±0.09 原发灶(n=50) 47.54±24.48 10.22±4.40 12.44±5.01 1.96±0.89 8.06±3.34 9.78±4.14 1.44±0.81 转移灶(n=21) 22.57±9.78 6.61±2.59 7.87±2.92 1.16±1.13 5.32±2.30 6.21±2.60 0.93±0.90 注:表中,“-”表示无此项数据;SUL为瘦体标准化摄取值;SUVmean为平均标准化摄取值;SUVmax为最大标准化摄取值;SULmean为平均瘦体标准化摄取值;SULmax为最大瘦体标准化摄取值。 表 1 50例不同病理类型肺癌患者病灶SUV和SUL结果
(x±s) -
50例不同病理类型的肺癌患者经过血糖浓度校正后SUV和SUL见表 2。患者血糖浓度与肝脏参考本底SUVmean、SUVmax、SULmean和SULmax的相关系数分别为:0.03、0.09、0.02和0.01,P均 > 0.05,由此可以看出患者的血糖浓度与肝脏参考本底SUV和SUL无相关性。患者血糖浓度与肺部原发病灶SUVmean、SUVmax、SULmean和SULmax的相关系数分别为:-0.34、-0.33、-0.33和-0.32,P均 < 0.05,这表明肺部原发病灶SUV、SUL与血糖浓度呈负相关,且血糖浓度与SUV的相关性高于SUL。50例肺癌患者中21例患者的血糖浓度与21个纵隔转移灶SUVmean、SUVmax、SULmean和SULmax的相关系数分别为:0.02、0.02、0.05和0.02,P均 < 0.01。肺癌纵隔转移灶SUV、SUL与血糖浓度无明显的相关性。
病理类型 病灶大小(mm) SUVmean SUVmax SUV标准差 SULmean SULmax SUL标准差 大细胞癌 肝脏参考部位(n=2) - 16.16±6.82 17.5±6.15 0.81±0.12 12.66±4.87 13.50±4.62 0.64±0.07 原发灶(n=2) 20.50±6.36 42.14±5.18 55.53±2.76 12.05±2.28 37.11±0.91 43.59±0.33 5.73±0.30 转移灶(n=1) 23.00 48.97 54.38 6.25 39.75 47.22 6.63 小细胞癌 肝脏参考部位(n=5) - 16.75±3.03 18.44±3.63 1.58±0.55 12.78±1.64 14.09±1.74 1.01±0.24 原发灶(n=5) 44.20±13.97 59.40±3.01 71.90±36.9 9.79±4.88 46.40±25.40 54.40±26.70 5.71±3.52 转移灶(n=5) 17.20±3.49 30.20±15.40 37.03±15.82 7.50±5.54 24.18±11.17 29.05±13.25 5.28±3.65 腺癌 肝脏参考部位(n=20) - 16.86±4.72 18.86±5.66 1.71±0.73 12.70±3.62 14.14±3.62 1.31±0.63 原发灶(n=20) 40.05±19.66 52.78±21.16 63.43±23.01 9.55±4.31 41.27±17.35 48.29±20.46 7.07±3.40 转移灶(n=7) 20.71±5.31 47.48±22.58 53.97±24.11 5.87±3.63 36.67±20.63 41.22±22.17 4.64±1.99 鳞状细胞癌 肝脏参考部位(n=23) - 15.85±3.05 17.46±3.50 1.31±0.70 12.91±2.45 14.40±2.84 1.25±0.67 原发灶(n=23) 57.13±27.34 74.87±24.73 91.78±28.05 15.10±6.15 59.22±17.12 74.03±22.22 11.50±5.43 转移灶(n=8) 27.50±13.78 39.75±11.65 49.34±16.61 7.81±4.03 33.34±11.61 39.69±14.45 6.58±3.62 合计 肝脏参考部位(n=50) - 16.36±3.84 18.12±4.50 1.48±0.71 12.80±2.92 14.23±3.07 1.18±0.62 原发灶(n=50) 47.54±24.48 63.18±25.51 77.00±29.48 12.23±5.80 49.88±19.50 60.56±24.58 8.92±4.97 转移灶(n=21) 22.57±9.78 40.49±16.71 48.19±19.14 7.02±4.07 32.62±15.01 38.02±16.87 5.62±3.04 注:表中,“-”表示无此项数据;SUL为瘦体标准化摄取值;SUVmean为平均标准化摄取值;SUVmax为最大标准化摄取值;SULmean为平均瘦体标准化摄取值;SULmax为最大瘦体标准化摄取值。 表 2 50例不同病理类型的肺癌患者经过血糖浓度校正后SUV和SUL结果
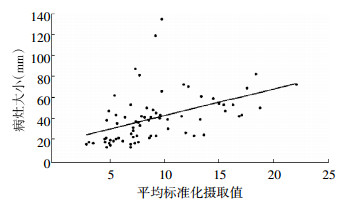
(x±s) 71个病灶(肺部原发灶50个、转移灶21个)的大小与SUVmean、SUVmax、SULmean和SULmax的相关系数分别为:0.46、0.50、0.47和0.47,P均 < 0.01。病灶大小=16.71+2.56×SUVmean、病灶大小=15.60+3.39×SULmean。图 3和图 4分别是71个病灶大小与校正后的病灶SUVmean和SULmean之间的相关关系图。

图 3 71个肺癌病灶与校正后病灶平均标准化摄取值的关系

图 4 71个肺癌病灶与校正后病灶平均瘦体标准化摄取值的关系
依据本研究PET/CT图像诊断参考标准回顾性分析对肺癌诊断的准确率。表 3是50例肺癌患者(原发灶和转移灶共71个病灶)采用PET/CT诊断标准诊断的结果(经血糖浓度校正前和校正后,以及病灶大小校正后的PET/CT图像诊断结果)。由表 3可知,SUV和SUL按照该诊断标准获得的临床诊断准确率相同。
病灶类型 血糖浓度和病灶大小校正前 单进行血糖浓度校正后 单进行病灶大小校正后 血糖浓度和病灶大小校正后 肺癌原发灶
(n=50)90.00 96.00 96.00 100 肺癌转移灶
(n=21)71.43 80.95 80.95 95.24 表 3 18F-FDG PET/CT对肺癌患者血糖浓度和病灶大小校正前、后诊断准确率的比较
(%) -
本研究是在已有研究结果的基础上,进一步探讨肺癌患者体重、血糖浓度和病灶大小对18F-FDG PET/CT肺癌临床诊断准确率的影响。本研究结果部分与已经报道结果一致[1-4, 6],同时也有一些新的发现。
(1)肝脏参考本底SUV与患者体重和血糖浓度之间无相关性。SUV和SUL之间最大的区别在于SUL更多地考虑了患者体重对18F-FDG摄取的影响。本研究结果表明,SUV和SUL之间存在很好的相关性,但是两者之间存在显著性差异。这主要是因为本研究选择的患者均未进行临床治疗,患者体重对SUV影响不明显。对于常规临床诊断SUV和SUL之间并无显著性差异。本研究表明,患者血糖浓度与肝脏参考本底SUV、SUL之间无明显的相关性。血糖浓度升高、肝脏参考本底SUV、SUL也相应升高。这与其他学者报道的结果一致[1-4]。肝脏SUV可以作为临床诊断的参考。
(2)患者原发灶和转移灶的SUV和SUL与血糖浓度之间存在相关性。研究结果表明,肺癌原发灶SUV、SUL均与血糖浓度呈负相关,这与已经报道的结果相似[2-4]。但是,纵隔转移灶SUV、SUL却与患者血糖浓度呈正相关。迄今,我们未发现有关此类研究结果的报道,所以对于该结果的解释还需要进一步详细的研究。
(3)肺癌患者18F-FDG PET/CT的SUV和SUL按照血糖浓度和病灶大小校正后明显提高了对肺癌诊断的准确率,特别是对于纵隔转移灶。血糖浓度对于病灶对18F-FDG摄取具有不同程度的影响,所以很多学者提出通过校正患者血糖浓度能够明显提高对肿瘤诊断的准确率。同时,病灶大小不同,其对18F-FDG的摄取也存在明显差异,特别是对于小于30 mm的病灶。为此,新近推出的PET/CT均采用点扩展函数(point spread function,PSF)技术来提高PET/CT中PET图像的分辨率,以便减少部分容积效应导致获得的SUV不准确[6]。本研究使用的是较早的PET/CT,并没有配置PSF图像重建技术。所以,我们采取简单的病灶大小校正方法来提高SUV和SUL的准确率。
(4)采用肝脏作为参考本底使得肺癌的临床诊断达到了个性化(个体化)诊断的目的,并明显提高了临床诊断的准确率。由于个体之间存在体重、血糖浓度、病灶大小等差异,传统采用一个SUV标准诊断肿瘤的方法已经受到很大程度的挑战,特别是一些新的重建技术,比如:PSF、全三维迭代图像重建技术等,使得不同设备之间的SUV存在巨大差异。采用个体肝脏本底作为参考,明显消除了个体差异对诊断结果的影响。本研究首次提出了18F-FDG PET/CT个体化诊断方法。
综上所述,肺癌患者18F-FDG PET/CT图像经过体重、血糖浓度和病灶大小校正后,明显提高了肺癌临床诊断的准确率。特别是采用肝脏参考本底作为检测病灶的诊断方法,使得肺癌18F-FDG PET/CT临床诊断达到了个性化诊断的目的。
肺癌患者体重、血糖浓度和病灶大小对18F-FDG PET/CT病灶SUV的影响
The effect of lung cancer patients′ weight, blood glucose concentration and lesion size of lung cancer on 18F-FDG PET/CT lesions SUV results
-
摘要:
目的 研究肺癌患者体重、血糖浓度和病灶大小对18F-FDG PET/CT病灶SUV的影响。 方法 50例无糖尿病病史的肺癌患者中,21例有纵隔转移灶。所有患者均行常规18F-FDG PET/CT,使用Advantage Workstation图像处理工作站自动提取肺癌病灶SUV以及经过体重和体型校正的SUV。采用半自动方法提取肝脏参考本底SUV。肺癌原发灶和转移灶诊断参考标准按照肝脏参考本底SUV或体型校正SUV×1.5+2×标准差。 结果 50例肺癌患者血糖浓度与肝脏参考本底SUV之间呈正相关,与肺癌原发灶SUV呈负相关,但是与转移灶SUV之间却呈正相关。按照参考诊断标准,50个肺癌原发灶和21个肺癌转移灶经过血糖浓度、病灶大小进行校正前和校正后,临床诊断的准确率分别为90.00%、71.43%和100%、95.24%。 结论 患者体重、血糖浓度和病灶大小对肺癌临床诊断准确率具有显著影响。经过血糖浓度、病灶大小校正后临床对肺癌诊断的准确率明显提高。这些结果提示,行18F-FDG PET/CT诊断肺癌时,需要高度重视患者体重、血糖浓度和病灶大小对结果的影响。 -
关键词:
- 肺肿瘤 /
- 氟脱氧葡萄糖F18 /
- 正电子发射断层显像术 /
- 体层摄影术,X线计算机 /
- 标准化摄取值
Abstract:Objective To study the effects of lung cancer patients′ weight, blood glucose concentration and lesion size of lung cancer on 18F-FDG PET/CT lesions SUV results. Methods Fifty cases of lung cancer patients without a history of diabetes mellitus were enrolled in this study. Among them, 21 patients with mediastinal metastases were detected. According to clinical routine 18F-FDG PET/CT scanning, automatic extraction of lung cancer SUV, weight and size correction SUV were obtained using the GE Advantage Workstation image processing workstation. Liver reference background SUV was obtained using semi-automatic extraction method of extraction. Lung cancer primary tumors and metastatic lesions diagnosis reference standards were accordant with the liver reference background SUV or SUV shape correction×1.5+2×standard deviation. Results Fifty cases of lung cancer in patients with blood sugar concentration and liver reference background SUV had positive correlation with lung cancer, SUV of primary lung cancer was negatively correlated with blood sugar, but it showed a positive correlation between blood sugar and lung metastases. According to the reference criteria for the diagnosis of 50 primary lung cancer cases and 21 metastatic lung cancer cases before and after the clinical diagnosis, the glucose concentration, lesion size correction accuracies were 90.00%, 71.43% and 100%, 95.24% respectively. Conclusions Patients′ body weight, blood glucose concentration and lesion size significantly affect the accuracy of clinical diagnosis of lung cancer. After correction accuracy, it remarkably improved the clinical diagnosis of lung cancer. The results suggest that when using 18F-FDG PET/CT for lung cancer diagnosis, the effects of body weight, blood glucose concentration and lesion size should be concerned. -
图 1 患者男性,73岁,肺癌无纵隔肺门淋巴结转移。图中1a、1b:患者体部冠状面及横断面PET图像,示右肺下叶结节样高代谢病灶,考虑肺癌;1c、1d:患者胸部横断面CT图像与PET/CT融合图像,示右肺下叶结节样高代谢病灶,CT与相应部位见分叶状软组织密度肿块影。术后病理示为低分化腺癌。
图 2 患者女性,47岁,肺癌伴纵隔肺门淋巴结转移。图中,2a、2b:患者体部冠状面及横断面PET图像,示左肺下叶处高代谢病灶,考虑肺癌,纵隔及左侧肺门结节状高代谢病灶,考虑纵隔及肺门淋巴结转移癌;2c、2d:患者胸部横断面CT图像与PET/CT融合图像,示左肺下叶背段块状高代谢病灶,CT与相应部位可见形态不规则分叶状软组织密度肿块影,考虑肺癌。纵隔及左侧肺门可见结节状高代谢病灶,CT与相应部位可见肿大淋巴结影,考虑淋巴结转移癌。术后病理检查示为中分化腺癌,伴有纵隔及肺门淋巴结腺癌转移。
表 1 50例不同病理类型肺癌患者病灶SUV和SUL结果
(x±s) 病理类型 病灶大小(mm) SUVmean SUVmax SUV标准差 SULmean SULmax SUL标准差 大细胞癌 肝脏参考部位(n=2) - 2.66±0.74 2.89±0.59 0.26±0.11 2.09±0.49 2.24±0.43 0.20±0.10 原发灶(n=2) 20.50±6.36 7.10±0.23 9.41±0.99 2.02±0.07 6.3±0.83 7.41±1.09 0.97±0.10 转移灶(n=1) 23.00 9.24 10.26 - 7.50 8.91 - 小细胞癌 肝脏参考部位(n=5) - 2.84±0.42 3.13±0.48 0.14±0.04 2.17±0.13 2.39±0.18 0.11±0.03 原发灶(n=5) 44.20±13.97 10.26±5.24 12.30±6.38 1.68±0.86 7.94±4.33 9.34±4.75 1.01±0.71 转移灶(n=5) 17.20±3.49 5.19±2.29 6.38±2.91 1.31±0.99 4.20±2.07 5.01±2.43 0.92±0.65 腺癌 肝脏参考部位(n=20) - 2.54±0.52 2.84±0.64 0.21±0.10 1.91±0.40 2.14±0.39 0.18±0.10 原发灶(n=20) 40.05±19.66 8.19±3.69 9.80±3.94 1.47±0.65 6.39±2.93 7.48±3.46 1.09±0.55 转移灶(n=7) 20.71±5.31 7.18±3.35 8.13±3.35 0.86±0.38 5.51±2.98 6.19±3.18 0.69±0.24 鳞状细胞癌 肝脏参考部位(n=23) - 2.56±0.37 2.81±0.40 0.27±0.09 2.09±0.28 2.32±0.29 0.17±0.05 原发灶(n=23) 57.13±27.34 12.27±4.16 15.02±4.58 2.44±0.88 9.69±2.89 12.08±3.59 1.88±0.85 转移灶(n=8) 27.50±13.78 6.67±1.96 8.27±2.69 1.32±0.65 5.58±1.84 6.63±2.23 1.10±0.55 合计 肝脏参考部位(n=50) - 2.59±0.45 2.86±0.51 0.23±0.10 2.03±0.33 2.25±0.34 0.19±0.09 原发灶(n=50) 47.54±24.48 10.22±4.40 12.44±5.01 1.96±0.89 8.06±3.34 9.78±4.14 1.44±0.81 转移灶(n=21) 22.57±9.78 6.61±2.59 7.87±2.92 1.16±1.13 5.32±2.30 6.21±2.60 0.93±0.90 注:表中,“-”表示无此项数据;SUL为瘦体标准化摄取值;SUVmean为平均标准化摄取值;SUVmax为最大标准化摄取值;SULmean为平均瘦体标准化摄取值;SULmax为最大瘦体标准化摄取值。  下载: 导出CSV
下载: 导出CSV
表 2 50例不同病理类型的肺癌患者经过血糖浓度校正后SUV和SUL结果
(x±s) 病理类型 病灶大小(mm) SUVmean SUVmax SUV标准差 SULmean SULmax SUL标准差 大细胞癌 肝脏参考部位(n=2) - 16.16±6.82 17.5±6.15 0.81±0.12 12.66±4.87 13.50±4.62 0.64±0.07 原发灶(n=2) 20.50±6.36 42.14±5.18 55.53±2.76 12.05±2.28 37.11±0.91 43.59±0.33 5.73±0.30 转移灶(n=1) 23.00 48.97 54.38 6.25 39.75 47.22 6.63 小细胞癌 肝脏参考部位(n=5) - 16.75±3.03 18.44±3.63 1.58±0.55 12.78±1.64 14.09±1.74 1.01±0.24 原发灶(n=5) 44.20±13.97 59.40±3.01 71.90±36.9 9.79±4.88 46.40±25.40 54.40±26.70 5.71±3.52 转移灶(n=5) 17.20±3.49 30.20±15.40 37.03±15.82 7.50±5.54 24.18±11.17 29.05±13.25 5.28±3.65 腺癌 肝脏参考部位(n=20) - 16.86±4.72 18.86±5.66 1.71±0.73 12.70±3.62 14.14±3.62 1.31±0.63 原发灶(n=20) 40.05±19.66 52.78±21.16 63.43±23.01 9.55±4.31 41.27±17.35 48.29±20.46 7.07±3.40 转移灶(n=7) 20.71±5.31 47.48±22.58 53.97±24.11 5.87±3.63 36.67±20.63 41.22±22.17 4.64±1.99 鳞状细胞癌 肝脏参考部位(n=23) - 15.85±3.05 17.46±3.50 1.31±0.70 12.91±2.45 14.40±2.84 1.25±0.67 原发灶(n=23) 57.13±27.34 74.87±24.73 91.78±28.05 15.10±6.15 59.22±17.12 74.03±22.22 11.50±5.43 转移灶(n=8) 27.50±13.78 39.75±11.65 49.34±16.61 7.81±4.03 33.34±11.61 39.69±14.45 6.58±3.62 合计 肝脏参考部位(n=50) - 16.36±3.84 18.12±4.50 1.48±0.71 12.80±2.92 14.23±3.07 1.18±0.62 原发灶(n=50) 47.54±24.48 63.18±25.51 77.00±29.48 12.23±5.80 49.88±19.50 60.56±24.58 8.92±4.97 转移灶(n=21) 22.57±9.78 40.49±16.71 48.19±19.14 7.02±4.07 32.62±15.01 38.02±16.87 5.62±3.04 注:表中,“-”表示无此项数据;SUL为瘦体标准化摄取值;SUVmean为平均标准化摄取值;SUVmax为最大标准化摄取值;SULmean为平均瘦体标准化摄取值;SULmax为最大瘦体标准化摄取值。
下载: 导出CSV
表 3 18F-FDG PET/CT对肺癌患者血糖浓度和病灶大小校正前、后诊断准确率的比较
(%) 病灶类型 血糖浓度和病灶大小校正前 单进行血糖浓度校正后 单进行病灶大小校正后 血糖浓度和病灶大小校正后 肺癌原发灶
(n=50)90.00 96.00 96.00 100 肺癌转移灶
(n=21)71.43 80.95 80.95 95.24
下载: 导出CSV
-
[1] Adams MC, Turkington TG, Wilson JM, et al. A systematic review of the factors affecting accuracy of SUV measurements. AJR Am J Roentgenol, 2010, 195(2): 310-320. doi: 10.2214/AJR.10.4923 [2] Kubota K, Watanabe H, Murata Y, et al. Effects of blood glucose level on FDG uptake by liver: a FDG-PET/CT study. Nucl Med Biol, 2011, 38(3): 347-351. [3] Kaneta T, Hakamatsuka T, Takanami K, et al. Evaluation of the relationship between physiological FDG uptake in the heart and age, blood glucose level, fasting period, and hospitalization. Ann Nucl Med, 2006, 20(3): 203-208. doi: 10.1007/BF03027431 [4] Hadi M, Bacharach SL, Whatley M, et al. Glucose and insulin variations in patients during the time course of a FDG-PET study and implications for the "glucose-corrected" SUV. Nucl Med Biol, 2008, 35(4): 441-445. [5] William DT, Elisabeth B, H Konrad Müller-Hermelink, et al. Patho-logy and genetics: tumors of the lung, pleura, thymus and heart. Lyon: IARC Press, 2004: 35. [6] Wahl RL, Jacene H, Kasamon Y, et al. From RECIST to PERCIST: Evolving considerations for PET response criteria in solid tumors. J Nucl Med, 2009, 50 suppl 1: S122-150. -

 点击查看大图
点击查看大图
图(4)表(3)
计量
- 文章访问数: 2361
- HTML全文浏览量: 1010
- PDF下载量: 5