


 下载:
下载:
-
18F-FDG PET/CT利用正电子核素18F标记葡萄糖代谢底物或类似物,在不影响正常机体代谢的情况下,引入体内参与细胞代谢过程,从分子水平上能够更准确地反映淋巴瘤组织与正常组织间的活性差异。PET/CT将PET和CT融为一体,可以无创、动态、定量地观察人体内病理生理过程,弥补了CT的不足,在淋巴瘤疗效评价中起着重要作用。本研究旨在探讨18F-FDG PET/CT定性、半定量分析在淋巴瘤化疗期间及化疗后评价中的临床价值。
-
本组病例为2008年1月至2012年3月在我院行躯干部PET/CT检查,且经手术或穿刺活检病理确诊为弥漫性大B细胞淋巴瘤(diffuse large B-cell lymphoma,DLBCL)的患者34例(其中,男性22例、女性12例,平均年龄50岁),首发病灶均为结内,共102处,主要分布于颈部、纵隔、胃周、肠系膜周围、腹膜后。30例行美罗华联合环磷酰胺+多柔比星+长春新碱+泼尼松(rituximab in combination with cyclophosphamide,doxorubicin,vincristine and prednisolone,R-CHOP)方案化疗,4例行CHOP方案化疗,21 d为一个化疗疗程,化疗前1周、化疗6疗程结束后1周内分别行PET/CT显像。其中12例患者在化疗前、第2疗程结束后、第4疗程结束后1周内均行PET/CT。对6疗程化疗后行PET/CT显像达到完全缓解的8例和部分缓解的10例,进行临床随访,每3个月一次,随访时间为12个月,观察1年无进展生存期(progression-free survival,PFS)。
-
18F-FDG由日本住友重机械株式会社HM-12回旋加速器生产,放化纯度≥95%。采用Siemens Discovery 16HR PET/CT扫描仪。患者检查前禁食6 h以上,所有患者治疗前后均按统一标准即3.7 MBq/kg的剂量经手背静脉注射18F-FDG,休息60 min后,在平静呼吸下行PET/CT,扫描范围从头到股骨上段的驱干部分,采用迭代法重建图像,层厚为3.75 mm,以获得PET和CT的横断、矢状、冠状断层图像及PET/CT融合图像。
-
PET/CT图像由2位经验丰富的核医学科诊断医师分别对图像进行阅片,若有不同意见,共同讨论得出结论,观察病变的位置、大小、形态,随后采用半定量分析,以纵隔血池为标准,选择所有病灶中目测代谢最高部位勾画出ROI,测出该区域的最大标准化摄取值(maximum standardized uptake value,SUVmax),CT图像测量病灶最大直径(maximum diameter,Dmax)。对同一部位均取SUVmax、Dmax 3次测量的平均值。随访中对同一患者固定同一病灶进行测量。
-
PET/CT评价中期疗效标准[1]:①完全缓解:所有病灶证据均消失,即治疗后PET阴性;CT显示淋巴结的最大横径缩小至≤1.5 cm。②部分缓解:病灶缩小,无新发病灶,即治疗后原受累部位有1个或多个PET阳性病灶,病灶数量 > 6个:6个最大病灶的最大垂直径乘积之和(sum of the product of the diameters, SPD)缩小≥50%,其他结节大小无增大;病灶数量≤6个:所有病灶的SPD缩小≥50%。③无缓解:出现新的PET阳性病灶或原病灶直径缩小 < 50%。
-
采用SPSS17.0统计学软件进行分析,两组间均数比较采用t检验,多组间均数比较采用方差分析,检验水准α=0.05,P<0.05表示差异有统计学意义。
-
34例DLBCL患者行化疗前、6疗程化疗后病灶SUVmax平均值分别为11.08±3.74和5.08±1.25;Dmax平均值分别为(5.63±2.15)cm、(2.26±1.04)cm;患者治疗前后的病灶SUVmax之间和Dmax之间的差异均具有统计学意义(t=3.58和2.96,P < 0.05);即PET与CT均可用于评价DLBCL化疗6疗程后的疗效。
-
12例DLBCL患者行化疗前、第2疗程结束后、第4疗程结束后的SUVmax平均值分别为15.67±8.02、7.87±3.21和3.25±1.22,Dmax平均值分别为(5.23±3.43)cm、(4.74±2.27)cm、(2.43±1.29)cm。12例患者在化疗前、第2疗程结束后、第4疗程结束后,SUVmax之间和Dmax之间的差异均有统计学意义(F=18.64和4.33,P均 < 0.05),且第2疗程结束后,病灶Dmax未见显著变化(t=1.05,P > 0.05)时,SUVmax值即已经显著改变(t=5.37,P < 0.05),第4疗程结束后,与化疗前相比,SUVmax之间和Dmax之间的差异均具有统计学意义(t=8.56和3.90,P均 < 0.05),即PET在治疗早期就可用来评价DLBCL的治疗反应。
-
34例患者6疗程化疗后PET/CT显像,完全缓解者8例,部分缓解者10例,无缓解者16例。对16例无缓解者临床改变了治疗方案,故未纳入本次随访研究中。对已达完全缓解或部分缓解的患者随访发现:
(1)完全缓解的8例患者中,PFS > 1年者6例,PFS < 1年者2例。8例患者6疗程化疗后的PET/CT结果示原有的病症均消失。在12个月的随访过程中发现,1例以颈部淋巴结肿大为首发症状的患者在6.2个月时出现发热,复查颈部彩超发现原病灶淋巴结明显肿大;另1例以胃周淋巴结为首发病灶的患者在9个月复查腹部CT时发现胃周、肝门区淋巴结增大,临床症状逐渐恶化。
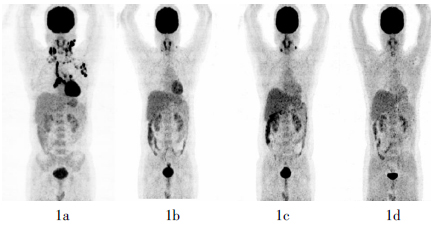
(2)部分缓解的10例患者中,PFS > 1年者2例,PFS < 1年者8例。1例采用CHOP方案化疗的患者,化疗前PET/CT示双侧颈部、双侧锁骨上窝、纵隔、左侧腋窝多发淋巴结病灶。6疗程化疗后行第2次PET/CT发现,除双侧颈部病灶淋巴结外其余病灶均消失,判断为部分缓解,临床上继续给予2疗程CHOP方案化疗后行第3次PET/CT,显像结果示双侧颈部病灶淋巴结代谢较第2次增高。临床把CHOP方案改为环磷酰胺+多柔比星+长春新碱+泼尼松+依托泊苷(CHOP+etoposide,CHOPE)方案化疗,2疗程后行第4次PET/CT,显像结果示双侧颈部病灶基本消失(图 1)。

-
治疗DLBCL的主要化疗方案是CHOP和R-CHOP方案,在化疗早期判定治疗反应可决定后续治疗决策的制定。目前,18F-FDG PET/CT是恶性肿瘤治疗疗效评价的重要方法,SUV是PET/CT中重要的半定量指标,它主要反映组织中葡萄糖的代谢程度。DLBCL病灶对18F-FDG的摄取程度与化疗前的SUV以及患者的年龄、肿瘤分期不相关,治疗后,肿瘤存活部分吸收18F-FDG,纤维瘢痕组织及肿瘤坏死部分不吸收18F-FDG。SUV受患者血糖、病灶血流量、注射的显像剂剂量、ROI的设置等多种因素的影响,在疗效评价中的意义存在较多争议。Meignan等[2]的研究发现,在DLBCL化疗早期的疗效评价中,SUV半定量法优于目测法,但Imataki等[3]认为,SUV的高低在疗效评价中无意义。本研究中以纵隔血池为本底标准测量SUV发现,SUVmax在2个疗程的化疗后即可反映疗效,而此时的Dmax尚无显著改变;在4疗程、6疗程化疗后的疗效评价中,SUVmax、Dmax均有显著改变,故在DLBCL早期(2疗程化疗后)疗效评价中,PET比CT更灵敏,但在化疗中期(4疗程化疗后)疗效评价中,PET和CT均可用。
PET/CT融合了PET和CT,不仅能显示病灶的大小、形态,更重要的是能显示病灶的活性有无及高低,在评价治疗反应上提供了更准确的信息[4-5]。有研究表明,在DLBCL患者中,近9%的患者利用18F-FDG PET/CT评价化疗疗效后改变了治疗手段和强度[6]。本研究中,6疗程化疗后PET/CT显像评价治疗反应,完全缓解者8例,部分缓解者10例。随访12个月后证实,完全缓解的患者中PFS > 1年者6例,部分缓解的患者中PFS > 1年者2例。在临床上,行R-CHOP方案化疗的DLBCL患者中,PFS为5年者占(56.4±8.3)%,PFS为1年者占84%[7]。PET/CT显像的结果对DLBCL患者的临床治疗具有指导性意义,有研究者认为,PET结果阳性者需要继续化疗;PET结果阴性者继续化疗与随访观察二者间的PFS无显著差异,故PET结果阴性患者可随访观察或随机行化疗[8]。
用18F-FDG PET/CT对DLBCL进行疗效评价,可早期、全面、客观地反映全身各部位淋巴结及脏器受累情况。PET/CT的特异度、灵敏度均高于CT[9]。但是18F-FDG PET/CT对微小淋巴结受侵或肿瘤活性低的病灶检出率低,易出现假阴性结果;另一方面,一些炎性病变、结核活动期、肉芽肿、化疗后骨髓活性增强等吸收18F-FDG出现假阳性。因此,18F-FDG PET/CT虽在影像学上是评价DLBCL疗效的首选方法,但仍不能替代组织活检的金标准。
综上所述,PET/CT对DLBCL化疗早期及化疗后进行的疗效评价有明显优势。目测法、SUVmax和Dmax半定量分析法可以评价早期治疗反应,在实时调节治疗方案、制定个体化治疗及预见性治疗方案上具有广泛的应用前景。本研究中的病例数较少,具有一定的局限性,故需更进一步的研究来确定18F-FDG PET/CT在DLBCL患者疗效评价中的意义。
18F-FDG PET/CT在弥漫性大B细胞淋巴瘤疗效评价中的临床价值
Clinical value of 18F-FDG PET/CT in evaluation of curative effect on diffuse large B cell lymphoma
-
摘要:
目的 探讨18F-FDG PET/CT在弥漫性大B细胞淋巴瘤(DLBCL)化疗早期及化疗后疗效评价中的临床价值。 方法 回顾性分析采用美罗华联合环磷酰胺+多柔比星+长春新碱+泼尼松方案或环磷酰胺+多柔比星+长春新碱+泼尼松方案化疗的34例DLBCL患者的PET/CT结果。所有患者分别在化疗前、化疗6疗程后行PET/CT,比较化疗前后病灶最大标准化摄取值(SUVmax)及病灶最大直径(Dmax);其中12例患者于化疗前、第2疗程结束后、第4疗程结束后行PET/CT,比较3组间的SUVmax与Dmax。对在化疗6疗程后行PET/CT显像已达到完全缓解的8例和部分缓解的10例患者进行临床随访,观察1年无进展生存期(PFS)。 结果 ①34例患者化疗前和6疗程化疗后,SUVmax之间和Dmax之间的差异均有统计学意义(t=3.58和2.96,P均 < 0.05)。② 12例患者在化疗前、第2疗程结束后、第4疗程结束后,SUVmax之间和Dmax之间的差异均有统计学意义(F=18.64和4.33,P均 < 0.05);第2疗程结束后与化疗前相比,病灶Dmax未见显著变化(t=1.05,P > 0.05),SUVmax显著降低(t=5.37,P < 0.05);第4疗程结束后与化疗前相比,SUVmax之间和Dmax之间的差异均具有统计学意义(t=8.56和3.90,P均 < 0.05)。③对18例患者进行的随访发现,完全缓解的8例中,PFS > 1年者6例,PFS < 1年者2例;部分缓解的10例中,PFS > 1年者2例,PFS < 1年者8例。 结论 在DLBCL化疗早期及化疗后的疗效评价上,PET比CT更灵敏,以两种显像方法相结合的PET/CT在淋巴瘤疗效评价上具有较高的临床价值。 Abstract:Objective To explore the clinical value of 18F-FDG PET/CT in evaluation of curative effect on diffuse large B-cell lymphoma(DLBCL). Methods 18F-FDG PET/CT was performed before and after 6 cycles of chemotherapy(R-CHOP or CHOP protocol) in 34 patients. By measuring maximum SUV(SUVmax) and maximum diameter(Dmax), the clinical value of PET and CT were compared in evaluation of curative effect on DLBCL after chemotherapy. Twelve patients underwent PET/CT examination for three times: before treatment, after 2 cycles of chemotherapy and after 4 cycles of chemotherapy. SUVmax and Dmax were compared among three groups. All the 8 patients who have reached complete response and 10 patients who have reached partial response after 6 cycles of chemotherapy were followed-up, and then the one-year progression-free survival (PFS) was observed. Results ①There was significant difference between SUVmax and Dmax before and after 6 cycles of chemotherapy on DLBCL patients(t=3.58 and 2.96, both P < 0.05). ② There was significant difference among before, after 2 cycles of chemotherapy, after 4 cycles of chemotherapy in SUVmax and Dmax (F= 18.64 and F=4.33, both P < 0.05). There was significant difference of SUVmax between before and after 2 cycles of chemotherapy (t=5.37, P < 0.05), and no difference of Dmax(t=1.05, P > 0.05). There was significant difference of both SUVmax and Dmax between before and 4 cycles of chemotherapy(t=8.56 and 3.90, both P < 0.05). ③Among 8 patients who have reached complete response, 6 cases were PFS > 1, 2 cases were PFS < 1. Among 10 patients who have reached partial response, 2 cases were PFS > 1, 8 cases were PFS < 1. Conclusions In evaluation curative effect on malignant DLBCL during and after treatment, PET was significantly better than CT. PET/CT as combination of PET with CT had a higher clinical value to evaluate the therapeutic effect of DLBCL. -
Key words:
- Lymphoma /
- B-cell /
- Fluorodeoxyglucose F18 /
- Positron-emission tomography /
- Tomography /
- X-ray /
- Treatment outcome /
- Standardized uptake value
-
[1] 李洪生, 吴湖炳, 王全师, 等. 18F-FDG PET-CT评价弥漫性大B细胞淋巴瘤化疗中期的治疗反应.中华核医学杂志, 2011, 31(3): 145-150. doi: 10.3760/cma.j.issn.0253-9780.2011.03.001
[2] Meignan M, Itti E, Gallamini A, et al. Interim 18F-fluorodeoxyglucose positron emission tomography in diffuse large B-cell lymphoma: qualitative or quantitative interpretation-where do we stand?. LEUK lymphoma, 2009, 50 (11): 1753-1756. doi: 10.3109/10428190903308056 [3] Imataki O, Tamai Y, Yokoe K, et al. The utility of FDG- PET for managing patients with malignant lymphoma: analysis of data from a single cancer center. Intern Med, 2009, 48(17): 1509-1513. doi: 10.2169/internalmedicine.48.1856 [4] Kasamon YL, Jones RJ, Wahl RL. Integrating PET and PET-CT into the risk-adapted therapy of lymphoma. J Nucl Med, 2007, 48 suppl1: S19-27. [5] Itti E, Juweid ME, Haioun C, et al. Improvement of early 18F-FDG PET interpretation in diffuse large B-cell lymphoma: importance of the reference background. J Nucl Med, 2010, 51(12): 1857-1862. doi: 10.2967/jnumed.110.080556 [6] 阎骅, 沈志祥.淋巴瘤循证治疗解读.肿瘤, 2008, 28 (9): 733-735. doi: 10.3781/j.issn.1000-7431.2008.09.003
[7] Petrausch U, Samaras P, Haile SR, et al. Risk-adapted FDG-PET-CT-based follow-up in patients with diffuse large B-cell lymphoma after first-line therapy. Ann Oncol, 2010, 21(8): 1694-1698. doi: 10.1093/annonc/mdq015 [8] Connors JM. Positron emission tomography in the management of Hodgkin lymphoma. Hematology Am Soc Hematol Educ Program, 2011, 116(21): 317-322. [9] 李倩, 刘建军. 18F-FDG PET-CT评价淋巴瘤疗效及预后的价值.国际放射医学核医学杂志, 2011, 35(4): 220-222. doi: 10.3760/cma.j.issn.1673-4114.2011.04.006
-

 点击查看大图
点击查看大图
图(1)
计量
- 文章访问数: 2004
- HTML全文浏览量: 825
- PDF下载量: 2