


 下载:
下载:
-
PET-CT是将PET的功能显像和CT的解剖显像有机结合在一起的现代影像设备, 是目前肺癌定性诊断及分期的主要影像学检查方法。细支气管肺泡癌(bronchial alveolar carcinoma, BAC)与其他腺癌相比具有不同的组织发生类型及形态学表现, 18FFDG PET的检查结果也与其他肺癌有所差别。本研究对BAC患者行18F-FDG PET, 并结合高分辨率CT(high resolution CT, HRCT)的影像特征进行分析, 探讨18F-FDG PET结合HRCT在BAC诊断中的临床价值。
-
2006年1月至2009年12月在福建省立医院PET-CT中心检查的具有完整临床资料的疑似BAC患者18例, 其中男性6例、女性12例, 年龄34~80岁, 平均60岁。18例患者中有17例经病理检查确诊, 其中, 10例经手术后病理证实, 5例经穿刺活检证实, 2例经脱落细胞学检查证实, 另1例经抗炎治疗后病灶消失。
-
18F-FDG由美国GE公司生产的MINItrace加速器及Tracelab自动化合成系统生产合成, 放化纯度 > 95%。显像仪器为美国GE公司生产的Discovery LS16 PET-CT仪, 应用Xeleris工作站进行图像后处理。
-
18例患者全部行PET检查, 检查前患者禁食6 h以上, 糖尿病患者需控制血糖水平在正常范围内。患者安静休息10 min后经肘前静脉注射4.44~5.55 MBq/kg(0.12~0.15 mCi/kg)的18F-FDG, 静卧休息50~60 min后扫描。扫描范围自颅顶部至双侧股骨上段, 采用三维扫描, 每个床位4 min, 重建方式为有序子集迭代法, 经计算机处理后获得横断面、冠状面及矢状面的PET图像。使用勾画ROI法测量病变的标准化摄取值(standarized uptake value, SUV)。
-
对16例患者的病灶部位行同机HRCT, 参数为330 mA, 120 kV, 层厚1.25 mm, 无间隔骨算法重建, 在WD4.2工作站进行后处理重建, 多角度显示病灶内部及周围结构细节。
-
所有患者均由两名富有经验的放射学医师及核医学医师综合分析病灶HRCT图像的部位、数目、大小、形态、分布、密度、内部结构等, 并进行病灶18F-FDGPET图像的肉眼分析及SUV半定量分析。在充分讨论的基础上, 结合临床病史确定诊断。
-
18例患者中BAC17例, 肺炎1例, BAC患者根据形态学表现及分布进行分组分析:
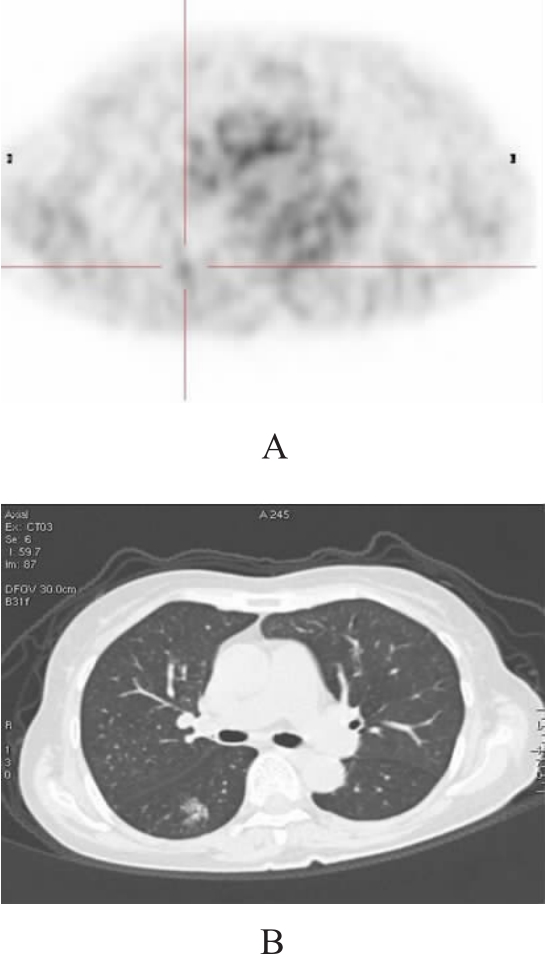
单发结节组5例(图 1), 其中1例为混合癌。病灶最大径为1.8~2.8 cm, 平均2.16 cm; SUV为1.5~3.5, 平均2.36, 其中仅2例的SUV > 2.5, 若以SUV > 2.5为BAC阳性参考界值, 则18F-FDG PET诊断的灵敏度仅为40%。4例患者同时行HRCT, 见毛玻璃征1例、毛刺征4例、分叶3例、空泡征2例、胸膜凹陷征3例、血管集束征3例。

图 1 患者男性,62岁,体检时发现右下肺一结节,后经病理证实为细支气管肺泡癌。图 1A为18F-FDG PET横断面图像,病灶SUV仅为1.2;图 1B为高分辨率CT横断面图像,可见毛玻璃征、毛刺征、分叶和空泡征。
局限性实变组6例, 病灶最大径为2.1~4.5 cm, 平均2.91 cm; SUV为0.9~2.3, 平均1.87;若以SUV > 2.5为BAC阳性参考界值, 则18F-FDG PET诊断的灵敏度为0。5例患者同时行HRCT, 见毛玻璃征5例、蜂窝征2例、胸膜凹陷征3例、“枯树枝”征2例、血管集束征1例。
混合组4例, 其中1例为混合癌。病灶呈结节状、片状、团块状高密度影弥漫分布于双肺野, SUV为4.5~10.0, 平均4.45;4例SUV均大于2.5, 若以SUV > 2.5为BAC阳性参考界值, 则18F-FDG PET诊断的灵敏度为100%。4例患者同时行HRCT, 见毛玻璃征2例、空泡征1例、胸膜凹陷征2例、“枯树枝”征3例、纵隔淋巴结转移2例。
肿块组1例, 为混合癌, 病灶大小为4.5 cm× 7.3 cm, SUV为5.6, HRCT见分叶、空洞、胸膜凹陷征及血管集束征。
多发结节组1例, 病灶最大径约1.3 cm, SUV为4.6, HRCT见毛玻璃征、分叶、细毛刺征伴纵隔淋巴结转移。
假阳性组1例, 病灶大小约2.1 cm×2.3 cm, 病灶代谢轻度增高, SUV为1.2, 结合HRCT的毛玻璃征、空泡征、条索影及相邻胸膜轻度凹陷等征象误诊为BAC, 抗炎治疗后随访观察3个月, 病灶消失。
单纯18F-FDG PET、单纯HRCT及二者联合诊断BAC的灵敏度和准确率分别为47.0%(8/17)和50.0%(9/18)、73.3%(11/15)和68.8%(11/16)、93.3%(14/15)和87.5%(14/16)。综上可见, 18F-FDG PET和HRCT联合能提高BAC诊断的灵敏度和准确率。
-
BAC在世界卫生组织分类中归于肺腺癌, 但对其组织发生、亚型分类以及究竟是腺癌的亚型还是肺癌的独立类型等均无统一认识, 根据BAC的病理学基本特征, 有4项诊断标准: 周围型病灶、非来源于中央支气管、肿瘤细胞沿肺泡间隔生长、肺外无原发性腺癌。进一步可将BAC分为非黏液型(占60%~65%)、黏液型(占20%~25%)和混合型(占12%~14%)3种。与其他种类的肺癌相比, BAC有许多不同的特点: 多为周围型肺癌, 易沿呼吸道播散转移, 血行及淋巴转移相对较少, 肿瘤生长速度缓慢, 增殖潜力远远低于高分化腺癌[1]。
PET可用半定量分析法判断病变的良恶性, 即根椐SUV来描述组织的18F-FDG摄取程度, 一般以SUV为2.5作为病变良、恶性的参考界值, 但本研究结果表明, 单纯依靠葡萄糖代谢情况来诊断BAC往往会出现假阴性的情况。Kim等[2]报道, 不论肿瘤大小, 只有接近50%的BAC病灶的SUV > 2.5。单发结节BAC组织18F-FDG摄取不高, 本组5例中有3例(60%)SUV < 2.5, 表明单发结节BAC虽属恶性肿瘤, 但恶性程度和葡萄糖代谢水平相对较低[3]; 单发结节BAC的形态学表现与一般肺癌相似, 具有恶性肿瘤征象, 但HRCT具有特殊征象: ①毛玻璃征: 表现为肺密度轻度增加, 但仍可显示血管支气管影; ②空泡征: 定义为结节内直径小于5 mm气体密度影或低密度影, 有时含气腔隙不规则呈囊状或条状。
局限性实变BAC组织对18F-FDG的摄取更低, 本组5例局限性实变BAC患者SUV均 < 2.5, 形态学表现类似肺炎, 单凭18F-FDG摄取指标进行判断易导致假阴性率较高。HRCT具有一定特征: ①毛玻璃征; ②“枯树枝”征: 表现为充气支气管管壁不规则、凹凸不平、普遍性狭窄及僵硬; ③蜂窝征: 表现为实变区密度不均匀, 呈蜂房状气腔。病理基础是肿瘤沿肺泡壁生长并分泌大量黏液而形成实变, 而细支气管被肿瘤浸润后形成活瓣性狭窄, 导致管腔及肺泡不规则扩张[4]。
本组共有6例BAC患者表现为多种形态混合并存或单一肿块、多发结节, SUV均 > 2.5, 说明18F-FDG PET诊断混合型或多结节型的BAC的假阴性率明显较低, 诊断准确率高。
BAC的影像学表现有其特征性, 当18F-FDG PET阴性时, 诊断应密切结合HRCT结果; 当18FFDG PET阳性而HRCT表现不典型时, 应以PET的表现为主并结合临床, 必要时行抗炎治疗后复查; 若18F-FDG PET及HRCT表现均不典型时, 多种显像剂的联合应用能为该病的诊断提供更多有价值的信息。总之, 对于BAC的诊断应密切结合PET中18F-FDG的代谢特点及HRCT的形态特征表现, 二者应互相印证, 不可偏重一方, 方能提高诊断的准确率。
18F-FDG PET结合高分辨率CT在细支气管肺泡癌诊断中的价值
The application of 18F-FDG PET and HRCT in the diagnosis of bronchial alveolar carcinoma
-
摘要:
目的 探讨18F-FDG PET及高分辨率CT(HRCT)在细支气管肺泡癌(BAC)诊断及鉴别诊断中的价值。 方法 回顾性分析具有完整临床资料的患者18例,其中病理检查确诊17例为BAC,1例经抗炎治疗后病灶消失。测量病灶标准化摄取值(SUV),分析病灶的影像学征象,比较单纯18F-FDG PET、HRCT及二者联合诊断的效能。 结果 ① 单发结节组5例,SUV为1.5~3.5,其中4例同时行HRCT,见毛刺征4例、分叶3例、胸膜凹陷征3例、血管集束征3例、空泡征2例、毛玻璃征1例。②局限性实变组6例,SUV为1.6~2.3,其中5例同时行HRCT,见毛玻璃征5例、胸膜凹陷征3例、空泡征2例、支气管充气征2例、血管集束征1例。③混合组4例,SUV为4.5~10.0,4例均同时行HRCT,见毛玻璃征2例、空泡征1例、胸膜凹陷征2例、支气管充气征3例。④肿块组1例,SUV为5.6,见分叶、空洞、胸膜凹陷征及血管集束征。⑤多发结节组1例,SUV为4.6,见分叶、细毛刺征。⑥假阳性组1例,病灶大小为2.1 cm×2.3 cm,SUV为1.2。 结论 单发结节组、局限性实变组的病灶对18F-FDG摄取较低,易误诊,PET代谢显像结合HRCT有利于提高BAC诊断及鉴别诊断的准确率。 -
关键词:
- 腺癌, 细支气管肺泡 /
- 氟脱氧葡萄糖F18 /
- 正电子发射断层显像术 /
- 体层摄影术, X线计算机
Abstract:Objective To investigate the features and diagnostic values of 18F-FDG PET and high resolution CT(HRCT) in patients with bronchial alveolar carcinoma(BAC). Methods Seventeen cases with pathologically confirmed BAC and 1 case confirmed inflammation were studied retrospectively.The standardized uptake value(SUV) of the lesions were detected and 18F-FDG uptake characteristics were studied.The diagnostic values of 18F-FDG PET, HRCT and 18F-FDG PET combined with HRCT were analyzed. Results ① In the group of solitary nodule(n=5), SUV of lesions were 1.5-3.5.HRCT(4/5) demonstrated spiculated(4/4), lobulated(3/4), pleural indentation(3/4), vascular convergence(3/4), vacuole sign(2/4) and ground-glass sign(1/4).②In the group of lobar consolidation(n=6), SUV of lesions were 1.6-2.3. HRCT(5/6) demonstrated ground-glass(5/5), pleural indentation(3/5), vacuole sign(2/5), air bronchogram sign (2/5) and blood vessel convergency(1/5).③In the group of mixed shadow(n=4), SUV of lesions were 4.5-10.0.Ground-glass sign, vacuole sign, pleural tag and air bronchogram sign were seen in 2, 1, 2 and 3 cases respectively.④There was 1 case in the group of mass lesion.The SUV of lesion was 5.6, and HRCT demonstrated lobulated, cavity, pleural indentation and blood vessel convergency.⑤There was 1 case in the multi-nodular group, SUV was 4.6, lobulation and spiculation sign were found.⑥SUV was 1.2 in the false positive case, with the lesion size of 2.1 cm×2.3 cm. Conclusions Low uptake of 18F-FDG in solitary nodule and lobar consolidation groups might cause false negative in the diagnosis of BAC.To improve the diagnosisaccuracy and to decrease misdiagnosis rate of BAC, combination of HRCT with 18F-FDG PET should be carried out. -
[1] Raz DJ, He B, Rosell R, et al. Current concepts in bronchioloalveolar carcinoma biology. Clin Cancer Res, 2006, 12(12): 3698-3704. doi: 10.1158/1078-0432.CCR-06-0457 [2] Kim HY, Shim YM, Lee KS, et al. Persistent pulmonary nodularground-glass opacity at thin-section CT: histopathologic comparisons. Radiology, 2007, 245(1): 267-275. doi: 10.1148/radiol.2451061682 [3] Wang T, Sun YE, Zhou NK, et al. Fluorine-18 fluorodeoxyglucose uptake in patients with primary lung cancer. Chin J Surg, 2002, 40(6): 437-440. [4] 邓宇, 曾庆思, 伍筱梅, 等. 细支气管肺泡癌影像学特征的深入性探讨. 放射学实践, 2005, 20(2): 128-131.
-

 点击查看大图
点击查看大图
图(1)
计量
- 文章访问数: 1068
- HTML全文浏览量: 433
- PDF下载量: 1