


-
肾血管性高血压占人群高血压的3%~10%, 其最主要原因为肾动脉狭窄。在我国, 随着生活水平的提高, 动脉粥样硬化性肾动脉狭窄(atherosclerotic renal arterystenosis, ARAS)的发病率越来越高, 而明确诊断、及时治疗可以大大减少并发症, 对患者预后十分重要。
多层螺旋CT血管造影(multi-slice computed tomographic angiography, MSCTA)具有无创性、图像分辨率高等特点, 加之其操作简单、安全经济, 使之成为无创性血管造影的主要方法, 其应用价值越来越受到关注。本研究对在我院行MSCTA肾动脉成像的82例患者进行回顾性分析, 并与其进行的数字减影血管造影(digital substrction angiography, DSA)结果做对照, 旨在探讨无创性MSCTA在诊断ARAS中的应用价值。
-
2007年4月至2009年2月在本院就诊的ARAS患者82例, 其中, 男性49例、女性33例, 年龄为46~77岁, 平均59岁。全部病例均进行了MSCTA与DSA检查, 两项检查的间隔时间为3~28 d。82例患者都存在不同程度的高血压, 平均血压为168/91 mmHg(1 mmHg=0.133 kPa), 大多数患者用降压药物治疗效果不佳。
-
患者禁食6~8 h, 并于扫描前30 min口服纯水500~700 ml, 以消除含碘的阳性对比剂对图像后处理质量的影响。采用美国GE公司16层螺旋CT仪, 扫描条件采用层厚1.25 mm、螺距0.625∶1、电压120 kV、电流200~300 mA, 扫描范围自膈肌至髂动脉分叉处; 对比剂使用德国先灵公司生产的非离子型对比剂欧乃派克(300 mg/ml)80~100 ml, 用高压注射器经肘静脉给药, 注射流速为5 ml/s; 应用自动触发技术触发增强扫描。
-
DSA仪采用飞利浦公司FD20数字化平板探测器血管造影机。经桡动脉行选择性肾动脉造影, 在C型臂下将猪尾巴导管置于双侧肾动脉开口以上, 以15ml/s的速度注入非离子型对比剂欧乃派克40ml, 观察肾动脉有无狭窄及双肾灌注情况。
-
对扫描所得的原始数据进行重建, 重建层厚为0.625 mm, 然后将重建数据传至美国GE公司生产的4.3三维后处理工作站, 应用三维后处理软件进行图像后处理重建, 重建方法为: ①多平面重建, ②最大密度投影法重建, ③表面阴影遮盖法重建, ④容积重建。
-
肾动脉狭窄率以最窄处管径与近端血管管径相比较, 如果狭窄段位于起始部, 则与远端正常管径相比较。狭窄率以正常肾血管直径的百分比表示, 即: 肾动脉狭窄率(%)=100×(1-狭窄血管直径/正常血管直径), MSCTA与DSA使用同一判定标准。
以肾动脉血管造影为标准, 将肾动脉管径评价分为正常、轻度狭窄(< 50%)、中度狭窄(51%~74%)、重度狭窄(75%~99%)和血管闭塞(100%)等5个等级[1-2]。
-
图像分析及诊断由两位资深影像诊断医师独立进行, 比较各种后处理技术的显示效果, 同时分析有无狭窄及狭窄程度, 并与DSA图像进行比较, 若两人意见有分歧, 则通过协商达成一致。
-
82例ARAS患者均获得满意的肾动脉MSCTA轴位扫描图像及影像后处理图像, 图像清晰地显示了肾动脉的数目、肾动脉主干及分支结构形态、动脉硬化斑块、管壁钙化、狭窄程度。82例患者用MSCTA共显示164支主肾动脉, 其中狭窄血管95支, 且均为主肾动脉狭窄, 95支狭窄血管中, 30例为双侧(共计60支), 35例为单侧(图 1)。横轴位显示狭窄血管95支, 多平面重建显示狭窄血管95支, 最大密度投影法重建显示狭窄血管90支, 表面阴影遮盖法重建显示狭窄血管89支, 容积重建显示狭窄血管91支; 而采用最大密度投影法重建+容积重建显示狭窄血管95支, 显示率高达100%。
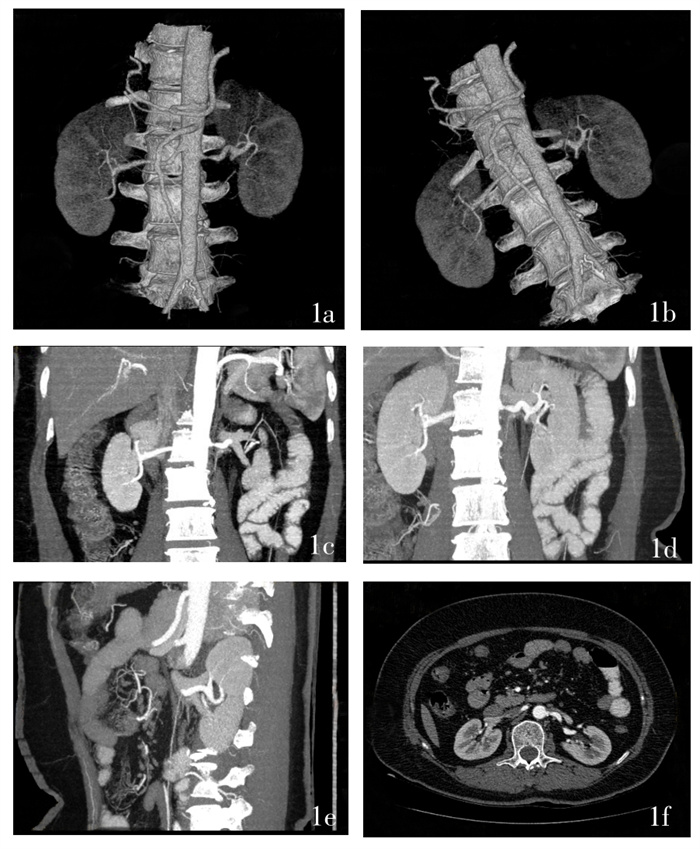
图 1 患者女性,60岁,发现高血压2年后来诊,入院时血压为180/100 mmHg。图 1a为肾动脉多层螺旋CT血管造影容积重建图像,见左侧肾动脉起始处有局限性狭窄;图 1b为肾动脉多层螺旋CT血管造影,见左侧肾动脉起始处有局限性狭窄;图 1c为肾动脉多层螺旋CT血管造影最小密度投影图像,矢状位,见左侧肾动脉起始处有局限性狭窄;图 1d为肾动脉多层螺旋CT血管造影最大密度投影图像,矢状位,见左侧肾动脉起始处有局限性狭窄;图 1e为肾动脉多层螺旋CT血管造影最大密度投影图像,冠状位,见左侧肾动脉起始处有局限性狭窄;图 1f为肾动脉多层螺旋CT血管造影横轴位原始图像,见左侧肾动脉起始处有局限性狭窄。
-
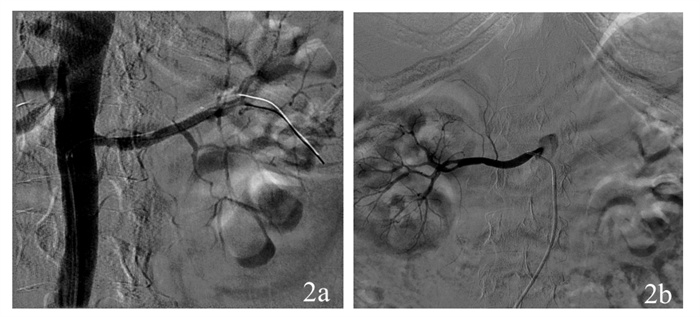
82例ARAS患者DSA显示164支主肾动脉, 发现狭窄血管85支, 全部为主肾动脉狭窄(图 2), 正常主肾动脉79支; 85支狭窄血管中, 25例为双侧(共计50支), 35例为单侧。
-
MSCTA未见ARAS的69支主肾动脉均经DSA证实, 无假阴性结果; MSCTA发现95支狭窄血管, 其中, 85支经DSA证实, 符合率为89%, 另10支用MSCTA见狭窄而DSA未见异常, 为假阳性结果, 假阳性率为6.1%。
MSCTA对24支血管的狭窄程度“过度评价”(表 1), 比例为25%, 同马炎鑫等[3]的研究结果基本一致, 笔者以为MSCTA确有过高评价血管狭窄程度的倾向。
多层螺旋CT血管造影分级 数字减影血管造影分级 总计 正常 轻度狭窄(< 50%) 中度狭窄(51% ~ 74%) 重度狭窄(75% ~ 99%) 闭塞(100%) 正常 69 0 0 0 0 69 轻度狭窄 10 27 0 0 0 37 中度狭窄 0 13 24 0 0 37 重度狭窄 0 0 9 10 0 19 闭寒 0 0 0 2 0 2 总计 79 40 33 12 0 164 表 1 多层螺旋CT血管造影与数字减影血管造影对动脉粥样硬化性肾动脉狭窄分级对比
-
无创性血管检查技术包括彩色多普勒超声、磁共振血管成像(mannetic resonance annionraphy)及MSCTA等多种成像方法。彩色多普勒超声在适当的条件下可诊断肾动脉狭窄, 但图像质量欠佳, 不能整体清晰显示肾动脉的解剖图像, 对肾动脉分支和副肾动脉的显示亦不能令人满意, 易受患者肥胖、憋气不足、肠道气体和组织等影像干扰, 而且, 即使肾动脉显示正常者也不能排除狭窄存在的可能性[4]。磁共振血管成像能很好地显示腹主动脉且不需用对比剂, 但由于肾动脉几乎以水平方向发出, 与腹主动脉几乎垂直, 因此在成像时会因层面内饱和作用而不能真实地显示肾动脉, 易产生肾动脉狭窄的假象[5]; 此外, 如果血流速度减慢或血流状态改变, 亦均可产生肾动脉狭窄的假阴性或假阳性结果[6]。DSA属创伤性检查, 只能提供管腔内情况, 不能显示管壁及相邻血管与组织结构的病理改变, 对钙斑和血栓的显示亦不如MSCTA, 而且DSA所显示的肾动脉是逆行充盈, 有时也会低估狭窄的程度[7]。
传统的单层螺旋CT由于不能将层厚、扫描速度及检查范围有效地结合在一起, 因此不能完全获得纯动脉期肾动脉及分支图像, 且图像质量明显不佳[8-9]。MSCTA通过工作站对所得图像进行三维重建, 可以清楚地显示肾动脉的正常解剖及变异, 多方位地观察血管及其周围情况, 提供血管内外的影像信息, 显示血管与邻近结构的关系, 对ARAS可以清晰地显示血管壁的钙斑, 确定其性质, 了解其狭窄程度, 从而对肾动脉狭窄做出可靠的诊断[10]。MSCTA应用于肾动脉主干狭窄患者的筛选时, 对于动脉粥样硬化患者, 如果MSCTA显示肾动脉主干正常或者轻度狭窄, 则结合临床可以考虑不再做DSA检查[11]。
MSCTA所获取的图像及各种后处理的图像中, 横轴面断层图像是诊断的基础, 它所显示的血管信息最为可靠。在后处理方法中, 最大密度投影法重建技术能多角度成像, 表达深度关系, 又能清晰显示小病灶, 可作为肾动脉狭窄测量与分级的主要依据, 其不足之处在于有时细小血管内对比剂密度不够高或受肾静脉重叠的影响而显示不清; 容积重建可以立体直观地显示肾动脉与周围组织器官的空间关系, 通过旋转不同角度观察肾动脉狭窄及支架的情况, 能够较好地显示血管壁钙化及寻找狭窄的原因, 亦能较准确地测量肾动脉管腔, 但不足之处在于其不能显示血管腔内情况[12-13]; 多平面重建是一种非常简便的重建方法, 可以在任意平面重建图像, 显示血管上下的走行关系以及上下侧的狭窄程度[14]; 表面阴影遮盖法立体感强, 可以在同一幅图像上显示肾动脉全貌, 并且可以从不同的角度观察, 但由于阈值以下的像素不能在二维图像上显示, 从而丢失大量信息, 不能准确测量血管直径, 亦不易显示小血管[15-16]。笔者体会, 在实际工作中, 对于上述多种后处理方法应该综合应用, 特别是应注意最大密度投影法重建技术和容积重建技术的结合。
MSCTA对肾动脉管径的准确测量依靠高质量的图像, 而要取得高质量图像有赖于扫描参数的合理选择和影像后处理方式的合理运用, 结合我们的经验是, MSCTA诊断ARAS应兼顾以下几个方面: ①扫描参数的合理配合: 最主要就是选择薄的层厚, 尽量选择最薄的层厚来完成肾动脉扫描, 本研究取1.25 mm层厚等相应的参数, 效果满意; ②对比剂的用量尽可能减少, 以减少肾静脉显影的干扰, 本研究用80~100 ml对比剂即完全能够满足诊断的要求; ③快速注射对比剂: 用高压注射器经肘静脉以5 ml/s的速度注入, 使腹主动脉肾动脉内对比剂浓度迅速升高; ④快速扫描: 由于肾脏血流丰富, 肾静脉显影早, 扫描时间应相应提前, 应用自动触发技术触发增强扫描, 可取得良好效果[17-18]。
多层螺旋CT血管造影术诊断动脉粥样硬化性肾动脉狭窄的价值
Evaluation of atherosclerotic renal artery stenosis by multi-slice CT angiography
-
摘要:
目的 探讨多层螺旋CT血管造影(MSCTA)诊断动脉粥样硬化性肾动脉狭窄(ARAS)的必要性和可靠性。 方法 选取82例曾做过数字减影血管造影(DSA)的ARAS患者行肾动脉MSCTA,将所获得的图像数据进行多平面重建、最大密度投影法重建、容积重建和表面阴影遮盖法重建,将结果与DSA进行对比分析。 结果 ① MSCTA发现狭窄血管95支,其中85支经DSA证实(10支为假阳性),符合率为89%,假阳性率为6.1%。②密度投影法重建+容积重建显示狭窄血管率达到100%。 结论 MSCTA是筛选ARAS的可靠方法。 -
关键词:
- 动脉粥样硬化 /
- 肾动脉梗阻 /
- 体层摄影术, 螺旋计算机 /
- 血管造影术
Abstract:Objective To study the reliability and necessity of multi-spiral computed tomography angiography(MSCTA)for non-invasive examination of patients with atherosclerotic renal artery stenosis (ARAS). Method Eighty-two ARAS patients who had taken intraarterial digital subtraction angiography were performed with MSCTA.The obtained image data were analyzed in MPR, MIP, VR and SSD with multi-spiral CT at certain condition and were compared with digital substrction angiography(DSA)images. Results ① MSCTA visualized 95 renal artery stenosis on DSA, 85 of which were detected coordinate(10 were falsepositive cases).The concordance rate of DSA and MSCTA was 89%, and the false positive rate was 6.1%.②The intensity projection reconstruction and volume reconstruction perfectly showed stenosis. Conclusion MSCTA is helpful to accurately display the renal artery variation and lesions, and is also a reliable and accurate screening modality for the evaluation of patients with ARAS. -
Key words:
- Atherosclerosis /
- Renal artery obstruction /
- Tomography, spiral computed /
- Angiography
-
图 1 患者女性,60岁,发现高血压2年后来诊,入院时血压为180/100 mmHg。图 1a为肾动脉多层螺旋CT血管造影容积重建图像,见左侧肾动脉起始处有局限性狭窄;图 1b为肾动脉多层螺旋CT血管造影,见左侧肾动脉起始处有局限性狭窄;图 1c为肾动脉多层螺旋CT血管造影最小密度投影图像,矢状位,见左侧肾动脉起始处有局限性狭窄;图 1d为肾动脉多层螺旋CT血管造影最大密度投影图像,矢状位,见左侧肾动脉起始处有局限性狭窄;图 1e为肾动脉多层螺旋CT血管造影最大密度投影图像,冠状位,见左侧肾动脉起始处有局限性狭窄;图 1f为肾动脉多层螺旋CT血管造影横轴位原始图像,见左侧肾动脉起始处有局限性狭窄。

表 1 多层螺旋CT血管造影与数字减影血管造影对动脉粥样硬化性肾动脉狭窄分级对比
多层螺旋CT血管造影分级 数字减影血管造影分级 总计 正常 轻度狭窄(< 50%) 中度狭窄(51% ~ 74%) 重度狭窄(75% ~ 99%) 闭塞(100%) 正常 69 0 0 0 0 69 轻度狭窄 10 27 0 0 0 37 中度狭窄 0 13 24 0 0 37 重度狭窄 0 0 9 10 0 19 闭寒 0 0 0 2 0 2 总计 79 40 33 12 0 164  下载: 导出CSV
下载: 导出CSV
-
[1] Schoenberg SO, Knopp MV, Londy F, et al. Morphologic and functional magnetic resonance imaging of renal artery stenosis: a multireader tricenter study. J Am Soc Nephrol, 2002, 13(1): 158-169. doi: 10.1681/ASN.V131158 [2] Hirsch AT, Haskal Z, Hertzer NR, et al. ACC/AHA guidelines for the management of patients with peripheral arterial disease(lower extremity, renal, mesenteric, and abdominal aotic): a collaborative report fromthe American Associations for Vascular Surgery/Society for Vascular Surgery, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, Society of Interventional Radiology, and the ACC/AHA Task Force on Practice Guidelines(writing committee to develop guidelines for the management of patients with peripheral arterial disease)--summary of recommendations. J Vasc Interv Radiol, 2009, 17(9): 1383-1397. [3] 马炎鑫, 徐建军, 刘影, 等. 多层螺旋CT肾动脉血管造影用于肾动脉狭窄检查112例分析. 中国误诊学杂志, 2007, 7(9): 2070. doi: 10.3969/j.issn.1009-6647.2007.09.146
[4] 张天宁, 陈涧新, 冯俊玲, 等. 彩色多普勒超声诊断肾动脉狭窄的临床价值. 浙江医学, 2008, 30(9): 1009-1010. doi: 10.3969/j.issn.1006-2785.2008.09.046
[5] Eklöf H, Ahlström H, Magnusson A, et al. A prospective comparison of duplex ultrasonography, captopril renography, MRA, and CTA in assessing renal artery stenosis. Acta Radiol, 2006, 47(8): 764-774. doi: 10.1080/02841850600849092 [6] Willmann JK, Wildermuth S, Pfammatter T, et al. Aortoiliac and renal arteries: prospective intraindividual comparison of contrastenhanced three-dimensional MR angiography and multi-detector row CT angiography. Radiology, 2003, 226(3): 798-811. doi: 10.1148/radiol.2271020014 [7] 王刚, 廖凯兵, 孙仁荣, 等. 肾动脉狭窄的临床研究进展. 放射学实践, 2008, 23(5): 567-571. doi: 10.3969/j.issn.1000-0313.2008.05.029
[8] 商秀林. 螺旋CT诊断肾动脉狭窄11例分析. 中国误诊学杂志, 2007, 7(6): 1321-1322.
[9] 蒋礼, 张玲. 肾动脉狭窄的诊治进展. 重庆医学, 2003, 32(10): 1415-1417. doi: 10.3969/j.issn.1671-8348.2003.10.066
[10] 李艳艳, 沈彦坡, 李会芝. 16层螺旋CTA在肾动脉狭窄中的应用. 中国误诊学杂志, 2008, 8(19): 4569. doi: 10.3969/j.issn.1009-6647.2008.19.023
[11] Kim TS, Chung JW, Park JH, et al. Renal artery evaluation: comparison of spiral CT angiography to intra-arterial DSA. J Vasc Interv Radiol, 1998, 9(4): 553-559. doi: 10.1016/S1051-0443(98)70320-3 [12] 王建军, 马大庆. MSCTA与DSA对动脉粥样硬化性肾动脉狭窄的临床应用. 放射学实践, 2008, 23(9): 1049-1051. doi: 10.3969/j.issn.1000-0313.2008.09.029
[13] 廖明壮, 赵海波, 腾才均, 等. 多层螺旋CT在肾动脉成像中的应用价值. 实用医学杂志, 2008, 24(9): 1603-1604. doi: 10.3969/j.issn.1006-5725.2008.09.061
[14] Schoenberg SO, Rieger J, Johannson LO, et al. Diagnosis of renal artery stenosis with magnetic resonance angiography: update 2003. Nephrol Dial Transplant, 2003, 18(5): 1252-1256. [15] 王建军, 马大庆, 高宗辉, 等. 动脉粥样硬化性肾动脉狭窄的SCTA与DSA对比研究. 中国临床医学影像杂志, 2008, 19(8): 577-580.
[16] 钱萍艳, 陈寅, 吴曼琍. 多层螺旋CT肾动脉成像的临床应用价值. 实用医技杂志, 2008, 15(27): 3679-3680.
[17] 胥洪卫, 唐志全, 张明睿, 等. 肾动脉狭窄多层螺旋CT血管成像与DSA对照研究. 医疗卫生装备, 2008, 29(10): 201-202.
[18] Wasser MN, Westenberg J, van der Hulst VP, et al. Hemodynamic significance of renal artery stenosis: digital subtraction angiography versus systolically gated three-dimensional phase-contrast MR angiography. Radiology, 1997, 202(2): 333-338. -

 点击查看大图
点击查看大图
图(2)表(1)
计量
- 文章访问数: 1949
- HTML全文浏览量: 649
- PDF下载量: 2