


-
传统的胸部特征性形态学影像对孤立性肺结节(solitry pulmonary nodule, SPN)的诊断价值有限。SPN良性结节生长很快或很慢, 而恶性结节持续生长, 研究发现, 倍增时间(doubling time, DT)即结节体积增长1倍所需的时间, 是肺癌预后的独立影响因素[1-2]。多层螺旋CT特别是64层螺旋CT的Z轴分辨率有了明显提高, 可达到各向同性; 其扫描速度及重建速度也大幅度提高, 这使得三维立体成像成为可能, 并促使了计算机辅助诊断和检测系统的快速发展[3-5]。LungCARE软件是一种肺结节分析软件, 能够自动精确地测量结节的体积, 并可计算容积DT(volumedoublingtime, DTV), 本研究通过对LungCARE软件三维体积测量技术及DTV在SPN随访中作用的研究, 评估DTV在64层螺旋CT诊断SPN中的价值。
-
选取2007年8月至2011年4月在我院行胸部CT的SPN患者46例, SPN指肺内单发的、直径≤3 cm的圆形或类圆形病灶, 未伴有肺不张、慧星灶和局部淋巴结的肿大[6]。其中, 男性21例、女性25例, 年龄38~76岁(中位年龄56岁)。
-
采用德国西门子公司SOMATOM Sensation 64 CT机行常规螺旋CT胸部扫描, 扫描参数为: 管电压120 kV, 管电流140 mAs, 准直0.6 mm, 层厚3 mm, 矩阵512×512。患者取仰卧位, 扫描范围从肺尖到膈顶。扫描后对原始数据按1.5 mm层厚进行重建, 重建后在工作站利用LungCARE软件中肺结节检测技术测量所有肺结节的容积(V), 并用电子鼠标测量其二维最大直径(D)。
-
DTV的计算公式: DTV=log2×△t/log(Vn/V1), 其中△t为初查与复查的时间间隔, Vn为复查结节容积, V1为初查结节容积。
直径DT(DTD)的计算公式: DTD=log2×△t/3 log (Dn/D1), 其中Dn为复查结节直径, D1为初查结节直径。
-
由于胸部CT初查不能确定SPN的良恶性, 故对所有患者均行抗感染治疗0.5至1个月后复查, 第一次复查时间为第一个月末(间隔约30 d), 第二次复查时间为第三个月末(间隔约90 d)。以DT在30~400 d作为恶性肺结节的诊断标准, 以容积缩小或不变及DT≤30 d或DT > 400 d作为良性结节的影像诊断标准[7-8]。同时, 以病理和临床结果作为诊断良恶性肺结节的金标准。
-
使用SPSS 13.0软件, 采用非参数统计中的配对资料McNemar检验比较两种方法的诊断价值。用Mann-Whitney U非参数检验方法评价DTV在恶性SPN不同复查时期及不同病例类型之间的差异, P < 0.05为差异有统计学意义。
-
46例SPN患者DTV为42~1082 d, 经临床和病理证实, 其中, 恶性肺结节29例, 包括18例腺癌(图 1)和11例鳞癌(术后病理证实有1例为肺泡癌, 归入腺癌, 其DTV为512 d, 术前诊断为肺结核, 经过半年抗结核治疗无效); 良性肺结节17例, 包括4例炎性假瘤(图 2)、3例肺脓肿、4例结核瘤、2例错构瘤、1例巨淋巴结增生症和1例血管瘤, 其余2例误诊为恶性(一例其第一月末DTV为42 d, 继续抗感染治疗后第三个月末DTV为382 d, 经胸腔穿刺病理证实为炎性假瘤, 另一例为结核瘤, DTV为347 d, 经胸腔穿刺病理证实)。良恶性肺结节中均存在实性结节、磨玻璃密度结节及混合密度结节。

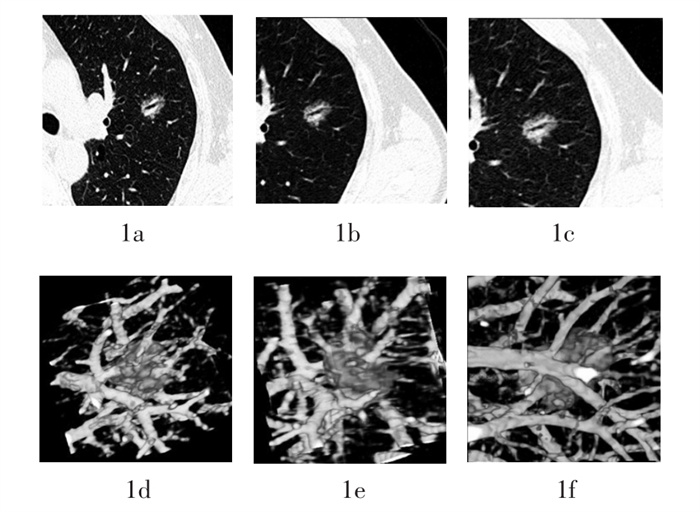
图 1 患者男性,59岁,患糖尿病住院,胸部CT左上肺非实性结节,其中可见空气支气管征,无分叶征,抗感染治疗半个月,经手术证实为高分化腺癌。图中,1a、1b、1c为肺窗测量结节直径,1d、1e、1f为LungCARE软件测量结节体积;1a、1d为初查时,直径=19.42mm,体积=2048.91 mm3;1b、1e为第一个月末复查时,直径=20.47mm,体积=2248mm3,容积倍增时间=201d;1c、1f为第三个月末复查时,直径=21.36 mm,体积=2840.95 mm3,容积倍增时间=194 d。
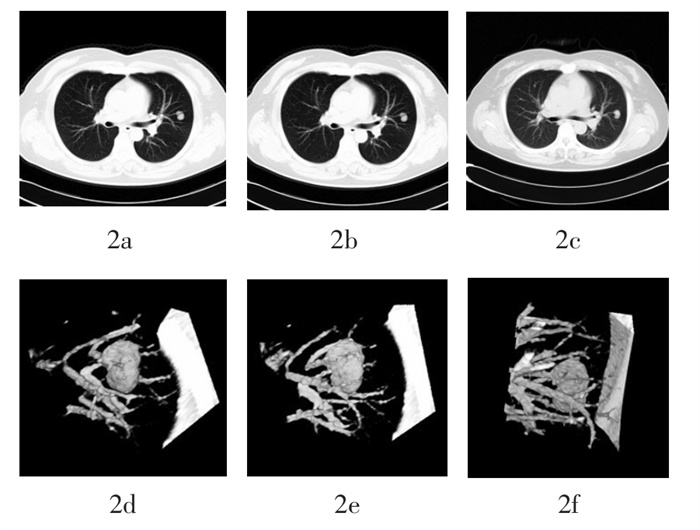
图 2 患者女性,46岁,咳嗽,左肺上叶实性结节, 抗感染治疗1个月,手术后病理证实为炎性假瘤。图中,2a、2b、2c为肺窗测量结节直径,2d、2e、2f为LungCARE软件测量结节体积;2a、2d为初查时,直径=15.40mm,体积=1658.95mm3;2b、2e为第一个月末复查时,直径=15.57mm,体积=1643.47mm3;2c、2f为第三个月末复查时,直径=14.70 mm,体积= 1656.21 mm3。
DTD法与DTV法对SPN的良恶性诊断效能的比较: 两种测量方法对恶性肺结节诊断的灵敏度、特异度、阳性预测率、阴性预测率和Youden指数见表 1。结果显示, DTV法判定SPN良恶性的效能显著优于DTD法(χ2=10.211, P < 0.05)。
灵敏度(%) 特异度(%) 阳性预测率(%) 阴性预测率(%) Youden指数 DTD法 79.31(23/29) 70.59(12/17) 82.14(23/28) 66.67(12/18) 0.50 DTV法 93.10(27/29) 94.11(16/17) 96.42(27/28) 88.89(16/18) 0.87 注:表中,DTD表示用普通平扫横断面测量直径计算所得的直径倍增时间;DTV表示用LungCARE软件测量体积计算所得的容积倍增时间。 表 1 直径倍增时间法和容积倍增时间法对良恶性孤立性肺结节诊断效能的比较
18例腺癌和11例鳞癌患者第一个月末及第三个月末的DTV比较, 差异无统计学意义(U=0.127和U=0.066, P均 > 0.05)。第一个月末及第三个月末, 18例腺癌和11例鳞癌患者的DTV比较, 差异有统计学意义(U=-3.193和U=-2.810, P均 < 0.01)(表 2)。
例数 第一个月末(d) 第三个月末(d) U值 P值 范围 中位数 范围 中位数 腺癌 18 98~312 193 89~298 167 0.127 > 0.05 鱗癌 11 67~176 121 58~189 102 0.066 > 0.05 U值 -3.193 -2.810 P值 < 0.01 < 0.01 表 2 容积倍增时间在恶性孤立性肺结节不同复查时期及不同病例类型之间的比较
-
本研究用LungCARE软件测定SPN容积计算DTV的方法, 其诊断效能明显优于测量直径计算DTD的方法, 分析原因主要是因为采用二维平面评估病变容积变化的误差比较大, 临床上用直径或最大横断面积计算DT时, 假设结节在三维上是球形物体, 但其在各个空间方向上的生长速度并不完全一致; 此外, 受心脏和呼吸运动伪影、呼吸深度变化、部分容积效应及不同观察者测量等因素的影响, 很难保证两次检查是在相同的层面比较结节的大小。因此, 短期内通过测量肿瘤的最大横径来观察肿瘤的生长时, 会因直径变化不明显、前后两次对结节直径的测量不够准确, 从而难以客观、准确地评价结节大小的细微改变。而LungCARE软件的工作原理是选择结节中心做标记, 提取包含结节信息的连续层面, 根据预先设定的阈值和连续性原则判断结节的边缘, 计算结节体积, 同时计算结节在X、Y和Z轴的直径、结节的最大径和最小径及平均密度值、密度标准差[9-10]。其实质是通过真正的三维重建测量结节体积, 因此该方法对结节体积的增长变化非常敏感, 能在相对较短的时间间隔内对结节进行随诊, 测量值客观、准确, 受操作者主观因素及不同观察者的影响较小, 适合短期内对结节随访。本研究表明, 在发现SPN后1个月对结节的体积随访就可明确测定DTV, 并与3个月后测定的DTV差异无统计学意义, 证实LungCARE软件能在相对较短的时间间隔内对结节体积的细微变化作出客观、准确的测定, 并有助于SPN良恶性的判断, 从而指导临床做出合理的处置决定, 使良性患者避免了不必要的手术, 而恶性患者可尽早手术, 以提高肺癌5年生存率。目前, 国际早期肺癌行动计划(International Early Lung Cancer Action Program)提出, 对直径大于10 mm的结节可选择抗生素保守治疗1个月后复查CT, 根据肿瘤DT的特点, 有效地筛查肺癌随访时间间隔, 有利于早期发现肺癌; 或进行进一步的影像学检查, 如增强CT、PET或活检[11]。本研究使用Lung CARE软件测定SPN容积计算DTV的诊断效能与国内刘瑛等[12]的研究结果相近。
目前, 肺癌已成为发病率和病死率最高的恶性肿瘤, 中晚期肺癌的5年生存率为15%, 如果I期肺癌患者手术及时, 5年生存率可达70%。既往的研究表明, 通过胸穿及痰细胞学检查筛查肺癌的方法并没有明显降低肺癌病死率[2]; SPN的定性诊断直接关系到治疗方法的选择与预后。对比增强检查、18F-FDG PET、经胸壁针刺活组织检查以及可视内窥镜下活组织检查等对于直径较小的SPN都显得无能为力, 尤其是结节直径越小, 上述检查越不准确。因此, 如何找到SPN适用的诊断方法是目前临床医师及影像医师的研究热点。目前, 对SPN的影像形态学特征分析仍是鉴别其良恶性的主要手段, DT是判断结节良恶性的另一个重要指标。
国外对肺癌DT的研究表明, DT是肺癌预后的独立且重要的影响因素, DT长的肺癌有较好的预后。Yankelevitz等[4]指出, 短期内通过CT三维重建测量结节体积来观察结节的生长速度, 能够区别良恶性肿瘤, 而DT是评价SPN生长性的独立性指标。目前较一致的结论为: 良、恶性结节DT存在差异, DT可作为良恶性鉴别的一个指标。另外, 不同组织学类型的肺癌, 其DT也不同, 小细胞肺癌最短, 腺癌最长; 并且早期肺癌的DT较长, 肿瘤生长缓慢, 随着肿瘤侵袭力的增加, DT缩短, 肿瘤生长迅速[13-14]。对影像学表现不典型的SPN, 需要多次行CT随诊复查, 并预测其DT来判断它是稳定静止的还是活动增长的。结节大小保持2年无变化或变小, 可诊断为良性。研究发现, 不同类型的肺癌DT差异较大, 其中鳞癌DT为90 d, 而侵袭性高和侵袭性一般的腺癌为180d以上[15-16]。但大多数恶性结节在30~400 d[2]。当然也有极少数例外, 如细支气管肺泡癌, 尤其是磨玻璃样结节表现的细支气管肺泡癌, 其平均DT为880 d。本研究结果也得出类似的结论, 但因样本量小, 具体的差别还需大样本和长期随访了解。另外, 64层螺旋CT作为一种新的检查手段, 目前于扫描条件尚未形成统一的标准, CT诊断结果与病理学诊断结果还存在一定差距, 对它的应用还缺乏足够的经验。
综上所述, 应用Lung CARE软件测量体积计算DTV的方法在64层螺旋CT诊断SPN中的效能优于测量直径计算DTD的方法。DTV可作为观察指标, 评估不同性质SPN的生长特征, 为肺结节的早期随访及定性诊断提供帮助。
容积倍增时间在64层螺旋CT诊断孤立性肺结节中的价值
The value of volume doubling time in diagnosis of solitry pulmonary nodules by 64-slice spiral CT
-
摘要:
目的 探讨容积倍增时间(DTV)在64层螺旋CT诊断孤立性肺结节(SPN)中的价值。 方法 初次胸部CT检查后,于第一个月末及第三个月末行2次以上随访的SPN患者46例,分别采用普通平扫横断面测量直径及LungCARE软件测定体积,计算所有结节的直径倍增时间(DTD)和DTV,比较两种测量方法对恶性肺结节的诊断价值;并用Mann-Whitney U非参数检验方法评价DTV在恶性SPN不同复查时期及不同病例类型之间的差异。 结果 经临床和病理证实,46例SPN患者中,恶性肺结节29例(包括18例腺癌和11例鳞癌)、良性肺结节17例。DTV法与DTD法在恶性SPN诊断中的灵敏度、特异度、阳性预测率、阴性预测率和Youden指数分别为93.10%、94.11%、96.42%、88.89%和0.87 vs.79.31%、70.59%、82.14%、66.67%和0.50,DTV法的诊断价值显著优于DTD法(χ2=10.211,P < 0.05)。腺癌与鳞癌患者第一个月末与第三个月末的DTV比较,差异无统计学意义(U=0.127和U=0.066,P均 > 0.05)。第一个月末及第三个月末,腺癌患者恶性肺结节的DTV显著大于鳞癌患者(U=-3.193和U=-2.810,P均 < 0.01)。 结论 DTV法在64层螺旋CT诊断SPN中的效能优于DTD法。DTV可作为观察指标,评估不同性质SPN的生长特征,为肺结节的早期随访及定性诊断提供帮助。 -
关键词:
- 硬币病变, 肺 /
- 体层摄影术, 螺旋计算机 /
- 图像处理, 计算机辅助 /
- 容积倍增时间
Abstract:Objective To discuss the value of volume doubling time(DTV)in diagnosis of solitry pulmonary nodules(SPN)by 64-slice spiral CT. Methods There were 46 cases which were underwent repeated follow-up CT at the first month and at the third month after the initial chest CT.We evaluated the value of DTV calculated by Lung CARE volumetry software and diameter doubling time(DTD)calculated by diameter method in the diagnosis of SPN.We compared the difference of DTV in different kinds of SPN and in different follow-up periods by Mann-Whitney U test. Results Twenty-nine malignant nodules and seventeen benign nodules were confirmed in forty-six SPN cases.The sensitivity, specificity, positive predictive value, negative predictive value and Youden index of DTV and DTD in the diagnosis of malignant nodules were 93.10%, 94.11%, 96.42%, 88.89%and 0.87 vs.79.31%, 70.59%, 82.14%, 66.67%and 0.50.The diagnostic value of DTVwas better than DTD(χ2=10.211, P < 0.05).Furthermore, there were no differences in DTVbetween different follow-up periods(U=0.127 and U=0.066, P > 0.05)but significant differences between adenocarcinomas and squamous cell carcinomas(U=-3.193 and U=-2.810, P < 0.01). Conclusions The value of DTV in diagnosis of malignant nodule was superior to DTD.The evaluation of DTV may be helpful in assessing the growth characteristic of SPN and its follow-up. -
图 1 患者男性,59岁,患糖尿病住院,胸部CT左上肺非实性结节,其中可见空气支气管征,无分叶征,抗感染治疗半个月,经手术证实为高分化腺癌。图中,1a、1b、1c为肺窗测量结节直径,1d、1e、1f为LungCARE软件测量结节体积;1a、1d为初查时,直径=19.42mm,体积=2048.91 mm3;1b、1e为第一个月末复查时,直径=20.47mm,体积=2248mm3,容积倍增时间=201d;1c、1f为第三个月末复查时,直径=21.36 mm,体积=2840.95 mm3,容积倍增时间=194 d。
图 2 患者女性,46岁,咳嗽,左肺上叶实性结节, 抗感染治疗1个月,手术后病理证实为炎性假瘤。图中,2a、2b、2c为肺窗测量结节直径,2d、2e、2f为LungCARE软件测量结节体积;2a、2d为初查时,直径=15.40mm,体积=1658.95mm3;2b、2e为第一个月末复查时,直径=15.57mm,体积=1643.47mm3;2c、2f为第三个月末复查时,直径=14.70 mm,体积= 1656.21 mm3。
表 1 直径倍增时间法和容积倍增时间法对良恶性孤立性肺结节诊断效能的比较
灵敏度(%) 特异度(%) 阳性预测率(%) 阴性预测率(%) Youden指数 DTD法 79.31(23/29) 70.59(12/17) 82.14(23/28) 66.67(12/18) 0.50 DTV法 93.10(27/29) 94.11(16/17) 96.42(27/28) 88.89(16/18) 0.87 注:表中,DTD表示用普通平扫横断面测量直径计算所得的直径倍增时间;DTV表示用LungCARE软件测量体积计算所得的容积倍增时间。  下载: 导出CSV
下载: 导出CSV
表 2 容积倍增时间在恶性孤立性肺结节不同复查时期及不同病例类型之间的比较
例数 第一个月末(d) 第三个月末(d) U值 P值 范围 中位数 范围 中位数 腺癌 18 98~312 193 89~298 167 0.127 > 0.05 鱗癌 11 67~176 121 58~189 102 0.066 > 0.05 U值 -3.193 -2.810 P值 < 0.01 < 0.01
下载: 导出CSV
-
[1] Usuda K, Saito Y, Sagawa M, et al. Tumor doubling time and prognostic assessment of patients with primary lung cancer. Cancer, 1994, 74(8): 2239-2244. doi: 10.1002/1097-0142(19941015)74:8<2239::AID-CNCR2820740806>3.0.CO;2-P [2] Steele JD, Buell P. Asymptomatic solitary pulmonary nodules. Host survival, tumor size, and growth rate. J Thorac Cardiovasc Surg, 1973, 65(1): 140-151. doi: 10.1016/S0022-5223(19)40835-0 [3] Kostis WJ, Reeves AP, Yankelevitz DF, et al. Three-dimensional segmentation and growth-rate estimation of small pulmonary nodules in helical CT images. IEEE Trans Med Imaging, 2003, 22(10): 1259-1274. doi: 10.1109/TMI.2003.817785 [4] Yankelevitz DF, Reeves AP, Kostis WJ, et al. Small pulmonary nodules: volumetrically determined growth rates based on CT evaluation. Radiology, 2000, 217(1): 251-256. doi: 10.1148/radiology.217.1.r00oc33251 [5] Gietema HA, Schaefer-Prokop CM, Mali WP, et al. Pulmonary nodules: Interscan variability of semiautomated volume measurements with multisection CT--influence of inspiration level, nodule size, and segmentation performance. Radiology, 2007, 245(3): 888-894. doi: 10.1148/radiol.2452061054 [6] Remy-Jardin M, Remy J, Giraud F, et al. Pulmonary nodules: detection with thick-section spiral CT versus conventional CT. Radiology, 1993, 187(2): 513-520. doi: 10.1148/radiology.187.2.8475300 [7] Xu DM, Gietema H, de Koning H, et al. Nodule management protocol of the NELSON randomised lung cancer screening trial. Lung Cancer, 2006, 54(2): 177-184. doi: 10.1016/j.lungcan.2006.08.006 [8] Xu DM, van der Zaag-Loonen HJ, Oudkerk M, et al. Smooth or attached solid indeterminate nodules detected at baseline CT screening in the NELSON study: cancer risk during 1 year of follow-up. Radiology, 2009, 250(1): 264-272. doi: 10.1148/radiol.2493070847 [9] 宋伟, 金征宇, 严洪珍, 等. 初步评估16层螺旋CT的Lung Care软件在肺结节研究中的辅助价值. 中华放射学杂志, 2005, 39(1): 11-16. doi: 10.3760/j.issn:1005-1201.2005.01.004
[10] 刘瑛, 吴宁. CT三维体积测量技术在孤立性肺结节诊断中的初步应用. 医学影像学杂志, 2006, 16(1): 88-90. doi: 10.3969/j.issn.1006-9011.2006.01.028
[11] Godoy MC, Naidich DP. Subsolid pulmonary nodules and the spectrum of peripheral adenocarcinomas of the lung: recommended interim guidelines for assessment and management. Radiology, 2009, 253(3): 606-622. doi: 10.1148/radiol.2533090179 [12] 刘瑛, 吴宁, 唐威. 计算机辅助诊断的三维体积测量技术在实性肺结节CT随诊中的价值. 中华放射学杂志, 2009, 43(4): 351-355. doi: 10.3760/cma.j.issn.1005-1201.2009.04.004
[13] Lillington GA. Management of solitary pulmonary nodules. Dis Mon, 1991, 37(5): 271-318. [14] Marchianò A, Calabrò E, Civelli E, et al. Pulmonary nodules: volume repeatability at multidetector CT lung cancer screening. Radiology, 2009, 251(3): 919-925. doi: 10.1148/radiol.2513081313 [15] de Hoop B, Gietema H, van Ginneken B, et al. A comparison of six software packages for evaluation of solid lung nodules using semiautomated volumetry: what is the minimum increase in size to detect growth in repeated CT examinations?. Eur Radiol, 2009, 19(4): 800-808. doi: 10.1007/s00330-008-1229-x [16] Hasegawa M, Sone S, Takashima S, et al. Growth rate of small lung cancers detected on mass CT screening. Br J Radiol, 2000, 73(876): 1252-1259. doi: 10.1259/bjr.73.876.11205667 [17] Jennings SG, Winer-Muram HT, Tann M, et al. Distribution of stage I lung cancer growth rates determined with serial volumetric CT measurements. Radiology, 2006, 241(2): 554-563. doi: 10.1148/radiol.2412051185 -

 点击查看大图
点击查看大图
图(2)表(2)
计量
- 文章访问数: 1892
- HTML全文浏览量: 705
- PDF下载量: 2