


-
在活体肾移植手术中, 亲属活体供肾为减少移植肾的紧缺起到了重要的作用。由于国内活体供肾移植起步较晚, 目前尚无对供肾的统一评估标准, 有关适合我国国情的供肾的选择与评估及安全性等问题的研究文献也相对较少[1]。本研究对161名亲属活体肾供者的临床资料进行分析, 探讨亲属活体肾供者99Tcm-二亚乙基三胺五乙酸(99Tcm-diethylenetriamine pentaacetic acid, 99Tcm-DTPA)肾动态显像肾小球滤过率(glomerular filtration rate, GFR)与年龄变化的相关性, 以期为临床活体肾移植供者的选择及安全性评估提供参考。
-
2007年10月至2009年3月, 我院共有212名拟供肾的亲属候选者, 应用99Tcm-DTPA肾动态显像的GFR及相关指标, 最终选取161名候选者作为供肾者(均无糖尿病、高血压及肝炎病毒感染等, 肝肾功能正常), 其中男性105名、女性56名, 年龄20~62岁, 平均(42.9±11.9)岁。供肾者选定后, 按其年龄的不同分为4组: 20~29岁组(52名), 30~39岁组(44名), 40~49岁组(38名)及≥50岁组(27名); 同时, 以55岁为界, > 55岁者作为老年组(24名)和年龄≤55岁者作为中青年组(137名)。所有供肾者均签署供肾知情书。
-
供肾者检查前3 d禁服利尿剂, 禁行静脉肾盂造影检查; 检查当日早晨正常饮食, 检查前30min内饮水500ml; 记录身高(cm)、体重(kg)及血压, 排空膀胱。
-
严格按照《临床技术操作规范核医学分册》[2]采用99Tcm-DTPA(由北京原子高科公司提供)肾动态显像法(Gates法)测定GFR。用SPECT仪(菲利普公司生产的双探头扫描仪)测量注射显像剂前及采集结束后注射器内的放射性计数, 时间为1min。患者取仰卧位, 探头视野包括双肾区及膀胱, 于肘静脉弹丸式注射显像剂99Tcm-DTPA 111~185MBq(≤0.5ml), 同时启动采集开关, 行连续双肾动态采集, 共21min。采集分为两个时相进行, 肾动脉灌注时相采集时2 s/帧, 连续采集60 s; 肾功能动态时相60 s/帧, 连续采集20min。探头配置低能通用型准直器, 能峰为140 keV, 窗宽20%, 矩阵128×128。
-
利用显像仪专用处理软件对原始数据进行处理, 应用感兴趣区技术分别勾画出双肾轮廓及本底, 根据注入静脉的显像剂99Tcm-DTPA的放射性计数及受检者的体重和身高, 计算机自动计算出总肾和分肾GFR。同时, 于供肾前后空腹取血用生化法(日立全自动生化仪)测定血清肌酐和血尿素氮水平。
-
统计学处理应用SPSS13.0统计学软件, 数值结果用均数±标准差x±s表示; 组间差异用ANOVA方差分析, 相关分析应用等级相关系数(Kendall’s tau-b)。P≤0.05为差异有统计学意义。
-
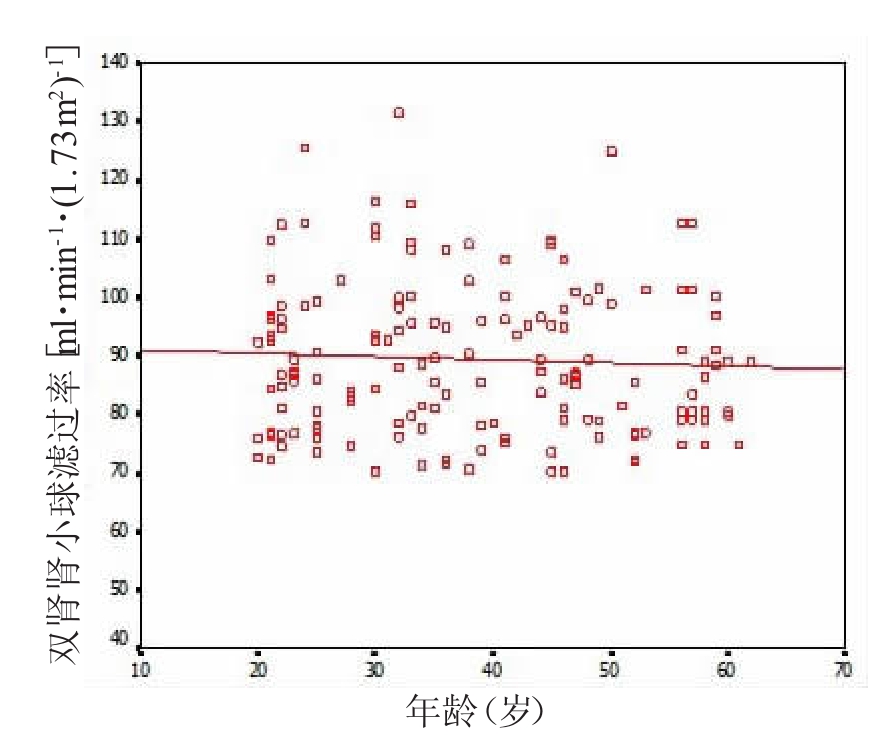
双肾GFR为(89.55±12.87)ml·min-1·(1.73m2)-1, 亲属活体肾供者不同年龄段GFR见表 1, 各组间均无显著统计学差异(F=2.09, P=0.10);以55岁为界, 老年组和中青年组GFR分别为(88.57±13.14)ml·min-1·(1.73m2)-1和(89.44±10.34)ml·min-1·(1.73 m2)-1, 两组间差异无统计学意义(F=1.31, P=0.25)。供肾者GFR与年龄相关性见图 1, 结果显示, 两者间无明显相关性(r=-0.033, P=0.69)。
年龄(岁) 例数 肾小球滤过率[ml·min1·(1.73m2)-1] 左肾 右肾 双肾 20 〜29 52 43.56±6.41 4470± 6.62 88.27± 12.29 30 〜39 44 45.15±8.42 46.70±7.28 91.85±14.51 40-49 38 44.74±6.38 44.51 ±6.71 89.25± 11.26 ≥50 27 42.82±7.50 45.42±7.09 88,24± 13.20 表 1 亲属活体肾供者不同年龄组肾小球滤过率结果比较(x±s)
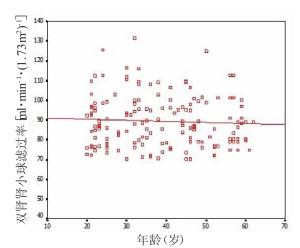
图 1 不同年龄组供肾者肾小球滤过率变化趋势图中的斜率代表肾小球滤过率与年龄变化的相关程度,斜率越大,两者相关性越好。
供肾前, 血清肌酐为(61.64±9.12)μmol/L, 血尿素氮为(4.34±1.02)mmol/L; 供肾后, 所有供者血清肌酐和血尿素氮均于短期内恢复至正常水平。随访8个月以上, 复查血常规、肝肾功能及尿常规未见异常, 未发生严重并发症。
-
临床所指的肾功能一般用GFR表示, GFR是反映肾脏滤过功能的重要指标及肾功能分期的主要依据。活体供肾移植术前对供肾功能的评估是活体肾移植最具挑战性的领域, 对保证供肾者和受肾者术后的安全至关重要[3-4]。由于国内活体肾移植的临床研究起步较晚, 对供肾的选择标准多数是借鉴国外经验, 国内临床应用经验尚需进一步积累。
-
GFR可以通过测定某种外源性或内源性滤过标志物的滤过率得到, 前者包括菊粉、同位素标记物, 后者包括血清肌酐、血尿素氮、内生肌酐清除率、胱抑素C(cystatin C), 以及在此基础上校正年龄、性别等多种因素的MDRD公式、Crokroft-Gault公式等。在GFR测定的各种方法中, 菊粉清除率被认为是测定GFR的金标准, 但其方法复杂、价格昂贵, 不适于临床常规应用; 在其他各种预测方法中, 99Tcm-DTPA肾动态显像简便易行、安全无创, 可同时观察肾脏的功能、分肾功能及解剖改变, 且有较好的精确性、准确性和可重复性, 是其他方法不可替代的, 因而在临床上应用广泛, 并得到普遍认同[5-6]。目前, 国内多数移植中心采用此方法检测供肾者术前的肾功能和分肾功能[1, 7]。
-
在正常供肾人群中, 有关GFR伴随年龄增长的变化存在争议, 文献报道的结果不一致性表现在3个方面: 一是GFR的变化与年龄呈显著负相关, 二是GFR的变化与年龄无相关性, 三是男性供肾者GFR与年龄呈显著负相关、女性供肾者GFR与年龄无相关性[8-10]。由于国内活体供肾移植起步较晚, 缺乏活体供肾者GFR大样本相关研究, 虽然现有文献报道支持青年与老年供者组GFR间差异无统计学意义[11], 但未对供体GFR与年龄相关性进行详尽系统的阐述, 因此, 供体GFR与年龄相关性需要进一步研究。
本研究严格按照《核医学诊断和治疗规范》采用99Tcm-DTPA肾动态显像法(Gates法)测定GFR, 并比较GFR与年龄相关性, 结果显示, 亲属活体供肾者GFR的变化与年龄无相关性, 中青年与老年供肾者的GFR间差异无统计学意义。所得的结果无统计学差异的原因可能是: 与一般健康人群比较, 对供肾者的健康选择标准更为严格, 几乎避免了高血压及糖尿病等因素的影响, 而高血压、糖尿病等均是加速肾小球硬化的高风险因素。供肾者的选择标准、年龄段组成的差异及检查中的质量控制等的不同, 可能是造成相关研究结果存在不一致的主要原因。
-
GFR是临床普遍认可的选择供肾者的重要参考标准, 合适的GFR是保证供肾者和受肾者安全性的重要指标, 有研究认为, GFR是影响移植肾存活率的惟一独立因素[12]。伴随老龄供肾者临床应用的逐步广泛, 老龄供肾者本身的安全性及能否提供合适、有效的GFR越来越受到关注。关于年龄对供肾者的安全性和受肾者预后的影响, 有文献报道, 供肾者高龄组与低龄组采用肌酐长期随访, 结果无统计学差异, 所有供肾者均未发生严重并发症, 两组受肾者的移植肾存活率及移植肾GFR等无统计学差异, 提示老龄供肾与低龄供肾的长期效果无统计学差异[13-14]。也就是说, 在保证供肾者合适有效的GFR前提下, 供者的年龄不是限制供体选择的独立预测因素, 此研究结果对老龄供肾者的选择有重要的指导意义。但也有极少数相关研究称, 供肾者的年龄可能会影响活体肾移植的存活率[15]。
本研究结果表明, 活体肾供者GFR与年龄变化无明显相关性, 所有活体肾移植后供肾者未发生严重并发症, 术后血清肌酐、血尿素氮均于短期内恢复正常水平, 复查肝肾功能均正常, 随访8个月以上, 复查血常规、肝肾功能及尿常规未见异常, 结果提示, 年龄≥55岁老年供肾者留存的肾代偿能力同中青年者一样, 足以维持肾功能在正常水平, 仍能满足机体代谢产物排泄的需要, 支持单纯年龄因素并不影响供肾者的选择及老年供肾者的安全性。但本组供肾者年龄最大为62岁, 年龄≥55岁的样本量相对较少, 且考虑到供肾者及受肾者安全性及检测技术的限制, 对供肾者GFR < 70ml· min-1·(1.73m2)-1者排除在外, 没有对其GFR进一步做金标准的检测及相关分析, 这是今后需进一步研究的课题, 因此在老年供肾者的选择上还应相对慎重。另需注意的是, 对肾功能的评价还要综合临床、化验及其他影像学根据, 相关系列研究尚需长期临床随访。进一步的研究应包括扩大样本量、99Tcm-DTPA肾动态显像与99Tcm-DTPA血浆清除率(双血浆法)GFR的对比分析及GFR与受肾者安全性的相关性研究。
亲属活体肾供者肾小球滤过率与年龄的相关性及其临床意义
Correlation and clinical significance between glomerular filtration rate and age in living-related kidney donors
-
摘要:
目的 探讨亲属活体肾供者肾小球滤过率(GFR)与年龄的相关性及其临床意义,为活体肾供者的选择提供客观的依据。 方法 161名亲属活体肾供者按年龄分为4组:第1组20~29岁(n=52),第2组30~39岁(n=44),第3组40~49岁(n=38),第4组≥50岁(n=27);同时以55岁为界,分为老年供肾组(> 55岁,n=24)和中青年供肾组(≤55岁,n=137)。利用99Tcm-二亚乙基三胺五乙酸肾动态显像法定量测量供肾者GFR,对比分析不同年龄组间GFR的特性。 结果 亲属活体供肾者双肾GFR为(89.55±12.87)ml·min-1·(1.73m2)-1,不同年龄组(1~4组)GFR分别为:(88.27±12.29)ml·min-1·(1.73m2)-1、(91.85±14.51)ml·min-1·(1.73m2)-1、(89.25±11.26)ml·min-1·(1.73m2)-1和(88.24±13.20)ml·min-1·(1.73m2)-1,各组间GFR差异无统计学意义(F=2.09,P= 0.10);老年供肾组与中青年供肾组GFR分别为(88.57±13.14)ml·min-1·(1.73m2)-1、(89.44±10.34)ml·min-1·(1.73m2)-1,两组间GFR差异无统计学意义(F=1.31,P=0.25)。经相关性分析,亲属供肾者GFR与年龄变化无明显相关性(r=-0.033,P=0.69)。活体肾移植后供肾者均未发生严重并发症,血清肌酐、血清尿素氮均于短期内恢复正常水平,肝肾功能均正常。 结论 亲属活体肾供者GFR与年龄变化无明显相关性,对于指导活体供体的选择有重要意义。 Abstract:Objective To quantitatively investigate the effectof age on the glomerular filtration rate (GFR)in living-related kidney donors, to analyze the clinicalvalue and the dependence ofGFR on age and toprovide an Objective basis for the selection of the living kidney donor.M ethods One hundred and sixtyone living-related kidney donorswere divided into four age groups, namely 20-29 years(n=52), 30-39 years (n=44), 40-49 years(n=38)and≥50 years(n=27).On theotherhand, the totaldonorswere divided into the groupsolder than 55 years(n=24)and younger than 55 years(n=137).To quantify GFR in all the subjects using the99Tcm-diethylenetriamine pentaacetic acid(99Tcm-DTPA)renography according to standard procedure and to evaluate the effects of age on renal function. Results The total GFR in living-related kidney donorswas calculated as(89.55±12.87)ml·min-1·(1.73m2)-1.The GFR in the first to the four age groups were(88.27±12.29)ml·min-1·(1.73m2)-1, (91.85±14.51)ml·min-1·(1.73m2)-1, (89.25±11.26)ml·min-1· (1.73m2)-1and(88.24±13.20)ml·min-1·(1.73m2)-1.The difference ofGFRwere notsignificant between the fouragegroups(F=2.09, P=0.10).The GFR in the donorsolder than 55 yearsand younger than 55 years were(88.57±13.14)ml·min-1·(1.73m2)-1and(89.44±10.34)m l·min-1·(1.73m2)-1, therewere no significant difference in GFR between the two groups(F=1.31, P=0.25).When relating GFR to age in all the livingrelated kidneydonors, there was nosignificant correlation(r=-0.033, P=0.69).No serious complications occurred after living kidney transplantation, serum creatinine values and blood urea nitrogen recovered to the normal levels in a shortperiod, hepatic and renal functionswere normal. Conclusion This study indicated that the GFR valueswere not correlated with the change of age in living-related kidney donors, and the Results were helpful for the selection of living donors. -
Key words:
- Kidney transplantation /
- Glomerular filtration rate /
- Livingdonors /
- Nuclearfamily
-
表 1 亲属活体肾供者不同年龄组肾小球滤过率结果比较(x±s)
年龄(岁) 例数 肾小球滤过率[ml·min1·(1.73m2)-1] 左肾 右肾 双肾 20 〜29 52 43.56±6.41 4470± 6.62 88.27± 12.29 30 〜39 44 45.15±8.42 46.70±7.28 91.85±14.51 40-49 38 44.74±6.38 44.51 ±6.71 89.25± 11.26 ≥50 27 42.82±7.50 45.42±7.09 88,24± 13.20  下载: 导出CSV
下载: 导出CSV
-
[1] 王强, 蔡明, 石炳毅, 等. 亲属肾移植供者77例移植前医疗评估. 中国组织工程研究与临床康复, 2010, 14(5): 874-878.
[2] 陈盛祖. 临床技术操作规范核医学分册. 北京: 人民军医出版社, 2003: 157-167.
[3] Hawley CM, Kearsley J, Campbell SB, et al. Estimated donor glomerular filtration rate is the most important donor characteristic predicting graft function in recipients of kidneys from live donors. Transpl Int, 2007, 20(1): 64-72. doi: 10.1111/j.1432-2277.2006.00400.x [4] 曾凡军, 刘斌, 蒋继贫, 等. 亲属活体肾移植101例分析. 中华器官移植杂志, 2006, 27(5): 265-267. doi: 10.3760/cma.j.issn.0254-1785.2006.05.003
[5] 姚立新, 李昨非, 刘波, 等. 99Tcm-DTPA核素肾动态显像对糖尿病肾功能的评价. 国际放射医学核医学杂志, 2009, 33(6): 343-346. doi: 10.3760/cma.j.issn.1673-4114.2009.06.007
[6] 朱阳军, 杜晓英, 李林法, 等. 肾动态显像法与双血浆法在肾移植GFR测定中的对比. 中华核医学杂志, 2007, 27(4): 243-244.
[7] 赖彦华, 孙煦勇, 聂峰, 等. 同一移植中心2年间亲属活体肾移植38例安全性评估. 中国组织工程研究与临床康复, 2010, 14(5): 883-886.
[8] Rook M, van der Heide JJ, Navis G. Significant negative association with age and both GFR and ERPF in male and female living kidney donors. Nephrol Dial Transplant, 2007, 22(1): 283. [9] Grewal GS, Blake GM. Reference data for 51Cr-EDTA measurements of the glomerular filtration rate derived from live kidney donors. Nucl Med Commun, 2005, 26(1): 61-65. [10] Berg UB. Differences in decline in GFR with age between males and females. Reference data on clearances of inulin and PAH in potential kidney donors. Nephrol Dial Transplant, 2006, 21(9): 2577-2582. [11] 方佳丽, 陈正, 潘光辉, 等. 99Tcm-DTPA肾动态显像评估活体供肾功能. 中华泌尿外科杂志, 2008, 29(1): 31-34. doi: 10.3321/j.issn:1000-6702.2008.01.007
[12] Kuo PC, Johnson LB, Schweitzer EJ, et al. Utilization of the older donor for renal transplantation. Am J Surg, 1996, 172(5): 551-555. doi: 10.1016/S0002-9610(96)00233-4 [13] Wolters HH, Schmidt-Traub H, Hölzen HJ, et al. Living donor kidney transplantation from the elderly donor. Transplant Proc, 2006, 38(3): 659-660. doi: 10.1016/j.transproceed.2006.01.057 [14] Kumar A, Verma BS, Srivastava A, et al. Long-term follow-up of elderly donors in a live related renal transplant program. J Urol, 2000, 163(6): 1654-1658. [15] Baid-Agrawal S, Frei UA. Kidney-transplant rejection and anti-MICA antibodies. N Engl J Med, 2008, 358(2): 196. -

 点击查看大图
点击查看大图
图(1)表(1)
计量
- 文章访问数: 1865
- HTML全文浏览量: 593
- PDF下载量: 4