


 下载:
下载:
-
超急性缺血性脑卒中的最有效治疗方法是溶栓治疗, 目前指导溶栓的CT不匹配模型主要是依据CT灌注参数图, CT灌注参数图可以有效地鉴别梗死核心与半暗带[1-2]。然而急性期脑卒中患者躁动或无意识运动不可避免, 特别是在CT灌注动脉期的头部运动, 会导致CT灌注参数图软件做不出参数图, 或伪影太明显而无法进行判读, 以及无法测量参数绝对值和相对值。本研究旨在分析CT灌注源图像(CT perfusion source images, CTPSI)在获得临床诊断和治疗所需要的影像信息中的价值。
-
所有患者选自2007年3月至2009年10月在本院绿色通道急诊的超急性期缺血性脑卒中(发病时间 < 9 h)患者。入选标准: 年龄18~80岁; 美国国立卫生研究院神经功能缺损评分≥4分; 没有卒中病史或发病前改良Rankin量表评分≤2分; 前循环缺血。排除标准: 颅内出血和肿瘤; 血糖浓度 < 2.7 mmol/L或 > 22.2 mmol/L; 有对比剂过敏史和肾功能不全史; 影像资料不全; 美国国立卫生研究院神经功能缺损评分≥25分。共100例患者符合入选标准, 其中男性65例, 年龄36~77岁(中位年龄57.5岁); 女性35例, 年龄50~76岁(中位年龄66.0岁), 病灶全部位于大脑中动脉分布区。所有患者均签署临床试验知情同意书和对比剂使用知情同意书, 并经本院伦理委员会批准。
-
影像方案包括基线“一站式”CT和2~7 d随访影像检查。基线“一站式”CT首先行平扫CT排除颅内出血, 随后行CT灌注成像和全脑CT血管造影, 随访影像为平扫CT。
“一站式”CT采用GE Brightspeed 16层螺旋CT仪。平扫CT覆盖全脑; 4层CT灌注成像定位于基底节水平和其上方的侧脑室体部水平, 用高压注射器经右侧肘正中静脉注入对比剂碘海醇(含I剂量: 300 mg/ml)40 ml, 流速为8 ml/s(18 G静脉留置针), 延迟4 s, 层厚1.25 mm, 重复扫描50次, 电压100 kV, 电流180 mA; 全脑CT血管造影使用同一对比剂80 ml, 注射流速5 ml/s, 延迟10 s, 扫描6 s, 层厚1.25 mm, 电压120 kV, 电流120 mA。
-
图像分析处理使用CT灌注成像后处理软件获取动脉时间-密度曲线和静脉时间-密度曲线, 本研究定义动脉期CTPSI和静脉期CTPSI分别是动脉时间-密度曲线和静脉时间-密度曲线峰值时的图像。分析层面为基底节层面和其上方的侧脑室体部层面, 应用Alberta卒中早期CT评分(Alberta stroke program early CT score, ASPECTS) 对大脑中动脉分布区缺血改变进行评估。动脉期CTPSI和静脉期CTPSI异常定义为对比剂降低的脑实质区域。由2名影像医师对动脉期CTPSI和静脉期CTPSI的ASPECTS进行盲法评定, 即评定者只知道患者症状体征位于左侧或右侧, 而不知道其他任何临床信息。至少1周后对随访影像行ASPECTS。
应用ASPECTS评价病灶范围, 延迟灌注定义为静脉期CTPSI ASPECTS-动脉期CTPSI ASPECTS≥1。2名影像医师评定是否存在延迟灌注, 结果不一致者商议后作出评定。
-
采用SPSS 11.5统计学软件。Spearman相关分析比较各个影像学形态(平扫CT图像、动脉期CTPSI、静脉期CTPSI和随访影像)之间ASPECTS的统计学相关性; Wilcoxon秩和检验比较动脉期CTPSI与静脉期CTPSI ASPECTS之间的统计学差异; 应用多元线性回归分析基线“一站式”CT各个影像学形态ASPECTS与随访影像ASPECTS之间的线性依存关系。P < 0.05为差异有统计学意义。
-
根据延迟灌注的定义, 经ASPECTS分析, 100例超急性脑缺血患者分为有延迟灌注组(42例), 无延迟灌注组(58例)。本研究有延迟灌注组中20例采用静脉溶栓治疗, 无延迟灌注组34例行静脉溶栓治疗。溶栓治疗前后患者行基线“一站式”CT及随访CT检查结果见图 1、图 2。有延迟灌注组基线平扫CT、动脉期、静脉期和随访影像的ASPECTS中位数(最小值~最大值)分别为: 8.0(6.0~10.0)、7.0(1.0~8.0)、8.0(3.0~10.0) 和7.5(0~10.0), 无延迟灌注组分别为: 8.0(1.0~10.0)、7.5(1.0~10.0)、8.5(1.0~10.0)、7.0(0~10.0)。有延迟灌注者提示存在缺血半暗带, 是溶栓治疗的重要依据, 而无延迟灌注者不存在半暗带, 提示不适合溶栓治疗。
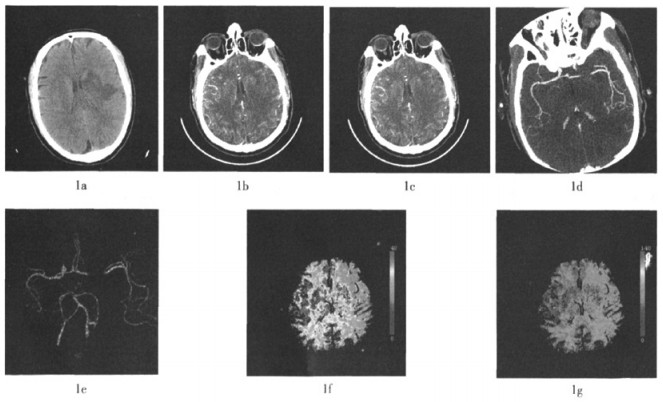
图 1 患者为男性, 52岁, 突发右侧肢体无力3 h来诊 图中,1a为平扫CT,显示左侧基底节区低密度影;1b为CTPSI动脉期图像;1c为CTPSI静脉期图像,显示左侧大脑半球呈低灌注缺血改变;1d为最大密度投影重建图像,显示左侧大脑中动脉走行中断;1e为容积重建图像,清晰显示左侧大脑中动脉局限闭塞;1f、1g为CT灌注图像,显示左侧大脑半球脑血流量明显降低,平均通过时间明显延长。
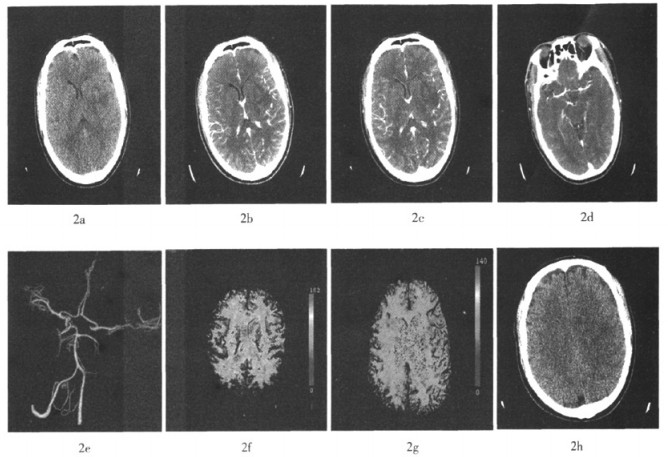
图 2 同一患者接受静脉溶栓治疗后10 d复查图像 图中,2a为平扫CT,显示左侧基底节区低密度影范围较前缩小;2b为CTPSI动脉期图像;2c为CTPSI静脉期图像,显示左右侧大脑半球灌注基本相当;2d为最大密度投影重建图像,显示左侧大脑中动脉走行较连续;2e为容积重建图像,清晰显示左侧大脑中动脉通畅;2f、2g为CT灌注图像,显示双侧大脑半球脑血流量、平均通过时间基本相当,原低灌注区消失;2h为随访平扫CT图像,显示原左侧基底节区低密度影基本消失。
在无延迟灌注组, 动脉期与静脉期CTPSI ASPECTS差异无统计学意义(Z=-1.00, P=0.459), 而在有延迟灌注组, 两者差异有统计学意义(Z=-3.08, P=0.001)。在无延迟灌注组, 基线平扫CT (r=0.879, P < 0.001)、动脉期CTPSI(r=0.902, P < 0.001)及静脉期CTPSI(r=0.945, P < 0.001)ASPECTS与随访影像ASPECTS均呈正相关; 有延迟灌注组, 只有静脉期CTPSI ASPECTS与随访影像ASPECTS呈正相关(r=0.831, P=0.004)。在无延迟灌注组, 标准化回归系数β=0.946, P < 0.001;有延迟灌注组β=0.714, P=0.003。
-
溶栓治疗无疑是超急性期缺血性脑卒中最有效的治疗手段, 目前采用的溶栓标准主要是依据梗死核心与半暗带的范围[3-4], CTPSI可以明确显示缺血低灌注脑组织。不管有无延迟灌注组, 平扫CT图像ASPECTS均高于动脉期CTPSI、静脉期CTPSI及随访影像, 一方面, 说明平扫CT图像显示超早期脑缺血病灶方面存在局限性; 另一方面, 由于CT灌注成像应用动态扫描技术以及对比剂增大了缺血脑组织和正常血供脑组织的对比度, 有利于早期发现缺血改变的脑组织[5-6], 本研究结果亦证明了CTPSI显示缺血低灌注脑组织优于平扫CT图像。
有延迟灌注组中: 动脉期CTPSI与静脉期CTPSI显示低灌注范围不一致; 静脉期CTPSI显示低密度范围小于动脉期CTPSI, 动脉期CTPSI显示低密度的区域中, 有一部分在静脉期出现延迟灌注, 这部分有延迟灌注的区域即是非梗死脑组织, 包括缺血半暗带和脑良性灌注不足。对于有延迟灌注, 即存在可挽救脑组织的患者, 需要进一步分析梗死核心的范围[7]。静脉期CTPSI显示低密度范围与最终梗死范围有较好的相关性, 其线性关系有统计学意义, 提示静脉期CTPSI可以有效地预测最终梗死范围。联合应用动脉期和静脉期CTPSI可以判断缺血半暗带和梗死核心的范围, 为溶栓治疗提供依据[8]。
无延迟灌注组中: 动脉期CTPSI与静脉期CTPSI显示的低密度范围一致, 两者的ASPECTS差异无统计学意义, 而且两者显示低密度区与随访最终梗死范围有统计学相关性, 提示动脉期CTPSI与静脉期CTPSI显示的低密度区均为梗死的脑组织, 不存在缺血半暗带, 即没有可以挽救的脑组织。对于无延迟灌注的患者, 溶栓治疗显然已无临床应用价值, 此方法只会增加溶栓后出血的危险性[9-10]。
本研究的初步结果表明, CTPSI显示无延迟灌注者不存在缺血半暗带, 提示不适合溶栓治疗; 有延迟灌注者提示存在缺血半暗带, 患者可以从溶栓中获益。在实际工作中, 作为“一站式”CT的一个重要组成部分, CTPSI并没有得到足够的重视, 或者说根本就被忽略了。尽管没有CT灌注参数图直观且容易判读, 然而没有经过处理的源图像是对脑组织血流灌注情况最真实的反映, 影像医师及神经内科医师有理由高度重视CTPSI的临床价值, 特别是在无法重建出参数图的情况下, 仍然不应放弃对患者的评价, 可以根据CTPSI判读患者是否符合溶栓标准, 并制定个体化治疗方案。
CT灌注源图像在诊断超急性期缺血性脑卒中的应用价值
Diagnostic value of perfusion source images in hyperacute stroke
-
摘要:
目的 探讨CT灌注源图像(CTPSI)在超急性期缺血性脑卒中诊断中的临床应用价值。 方法 100例急性缺血性脑卒中(发病时间 < 9 h)的患者行“一站式”CT检查,根据动脉期与静脉期CTPSI Alberta卒中早期CT评分(ASPECTS)的不同将100例患者分为2组:有延迟灌注组和无延迟灌注组。分析基线平扫CT、动脉期及静脉期CTPSI ASPECTS,并与随访影像ASPECTS进行对照。Wilcoxon秩和检验比较动脉期CTPSI与静脉期CTPSI ASPECTS之间的统计学差异;应用多元线性回归分析基线“一站式”CT各个影像学形态ASPECTS与随访影像ASPECTS之间的线性依存关系。 结果 100例患者分为有延迟灌注组42例和无延迟灌注组58例。基线平扫CT、动脉期、静脉期和随访影像的ASPECTS中位数(最小值~最大值)在有延迟灌注组分别为:8.0(6.0~10.0)、7.0(1.0~8.0)、8.0(3.0~10.0)、7.5(0~10.0);在无延迟灌注组分别为:8.0(1.0~10.0)、7.5(1.0~10.0)、8.5(1.0~10.0)、7.0(0~10.0)。在无延迟灌注组,动脉期与静脉期CTPSI ASPECTS差异无统计学意义(Z=-1.00,P=0.459),而在有延迟灌注组,两者差异有统计学意义(Z=-3.08,P= 0.001)。在无延迟灌注组,基线影像ASPECTS(平扫CT、动脉期及静脉期CTPSI)与随访影像ASPECTS均存在正相关(r值分别为0.879、0.902、0.945,P值均 < 0.01);在有延迟灌注组,静脉期CTPSI与随访影像ASPECTS的相关性最好(r=0.831, P=0.004)。多元线性回归结果显示只有静脉期CTPSI与随访影像ASPECTS之间的线性关系有统计学意义:无延迟灌注组,标准化回归系数β= 0.946,P < 0.001;有延迟灌注组,β=0.714,P=0.003。 结论 CTPSI显示无延迟灌注者不存在缺血半暗带,提示不适合溶栓治疗;有延迟灌注者提示存在缺血半暗带,是溶栓治疗的重要依据之一。 -
关键词:
- 脑血管意外 /
- 脑缺血 /
- 体层摄影术, X线计算机 /
- 灌注
Abstract:Objective To investigate the diagnostic value of CT perfusion source images(CTPSI)in acute stroke less than 9 hours. Methods "One-stop shop"CT examination were performed in 100 patients with symptoms of acute stroke in less than 9 hours.Patients were divided into two groups according to with and without delayed perfusion on CTPSI, and compared Alberta stroke program early CT score study(ASPECTS)scores on non-contrast CT, arterial phase CTPSI and venous phase CTPSI with follow-up imaging.The ASPECTS were analyzed on arterial phase CTPSI and venous phase CTPSI using Wilcoxon rank-sum test, then compared with the follow up imaging ASPECTS using multiple linear regressions. Results The median(min-max)scores of ASPECTS on NCCT, arterial phase CTPSI, venous phase CTPSI and follow-up imaging were 8.0(6.0-10.0), 7.0 (1.0-8.0), 8.0(3.0-10.0)and 7.5(0-10.0)in group with delayed perfusion, respectively, and 8.0(1.0-10.0), 7.5 (1.0-10.0), 8.5(1.0-10.0)and 7.0(0-10.0)in group without delayed perfusion respectively.ASPECTS scores measured on arterial phase CTPSI did not differ with venous phase CTPSI group without delayed per-fusion (Z=-1.00, P=0.459), while there was statistic difference in group with delayed perfusion(Z=-3.08, P=0.001).There were significant correlation of ASPECTS scores measured on mon-contrast CT, arterial phase CTPSI and venous phase CTPSI to follow-up imaging ASPECTS(r=0.879, 0.902, 0.945, P < 0.01)in group without delayed perfusion; ASPECTS measured in venous phase CTPSI showed the best correlation to follow-up imaging ASPECTS (r=0.831, P=0.004)in group with delayed perfusion.Multiple linear regression showed that the correlation in only venous phase CTPSI with follow-up imaging ASPECTS was statistically significant: in group without delayed perfusion, β=0.946, P < 0.001; in group with delayed perfusion, β=0.714, P=0.003. Conclusion Presence of delayed perfusion in CTPSI is quit important in identifying ischemic penumbra, which plays a critical role in imaging-guided thrombolytic therapy. -
Key words:
- Cerebrovascular accident /
- Brain ischemia /
- Tomography, X-ray computed /
- Perfusion
-
图 1 患者为男性, 52岁, 突发右侧肢体无力3 h来诊 图中,1a为平扫CT,显示左侧基底节区低密度影;1b为CTPSI动脉期图像;1c为CTPSI静脉期图像,显示左侧大脑半球呈低灌注缺血改变;1d为最大密度投影重建图像,显示左侧大脑中动脉走行中断;1e为容积重建图像,清晰显示左侧大脑中动脉局限闭塞;1f、1g为CT灌注图像,显示左侧大脑半球脑血流量明显降低,平均通过时间明显延长。
-
[1] Barber PA, Demchuk AM, Zhang J, et al. Validity and reliability of a quantitative computed tomography score in predicting outcome of hyperacute stroke before thrombolytic therapy. ASPECTS Study Group. Alberta Stroke Programme Early CT Score. Lancet, 2000, 355(9216): 1670-1674. [2] Wintermark M, Meuli R, Browaeys P, et al. Comparison of CT perfusion and angiography and MRI in selecting stroke patients for acute treatment. Neurology, 2007, 68(9): 694-697. doi: 10.1212/01.wnl.0000255959.30107.08 [3] Wintermark M, Flanders AE, Velthuis B, et al. Perfusion-CT assessment of infarct core and penumbr a: receiver operating characteristic curve analysis in 130 patients suspected of acute hemispheric stroke. Stroke, 2006, 37(4): 979-985. doi: 10.1161/01.STR.0000209238.61459.39 [4] Ezzeddine MA, Lev MH, McDonald CT, et al. CT angiography with whole brain perfused blood volume imaging: added clinical value in the assessment of acute stroke. Stroke, 2002, 33(4): 959-966. doi: 10.1161/hs0402.105388 [5] González RG. Imaging-guided acute ischemic stroke therapy: From"time is brain"to"physiology is brain". AJNR Am J Neuroradiol, 2006, 27(4): 728-735. [6] Murphy BD, Fox AJ, Lee DH, et al. Identification of penumbra and infarct in acute ischemic stroke using computed tomography perfusion-derived blood flow and blood volume measurements. Stroke, 2006, 37(7): 1771-1777. doi: 10.1161/01.STR.0000227243.96808.53 [7] Hill MD, Rowley HA, Adler F, et al. Selection of acute ischemic stroke patients for intra-arterial thrombolysis with prourokinase by using ASPECTS. Stroke, 2003, 34(8): 1925-1931. doi: 10.1161/01.STR.0000082483.37127.D0 [8] Pexman JH, Barber PA, Hill MD, et al. Use of the Alberta Stroke Program Early CT Score(ASPECTS)for assessing CT scans in patients with acute stroke. AJNR Am J Neuroradiol, 2001, 22(8): 1534-1542. [9] Pepper EM, Parsons MW, Bateman GA, et al. CT perfusion source images improve identification of early ischaemic change in hyperacute stroke. J Clin Neurosci, 2006, 13(2): 199-205. doi: 10.1016/j.jocn.2005.03.030 [10] Parsons MW, Pepper EM, Bateman GA, et al. Identification of the penumbra and infarct core on hyperacute noncontrast and perfusion CT. Neurology, 2007, 68(10): 730-736.
-

 点击查看大图
点击查看大图
图(2)
计量
- 文章访问数: 1767
- HTML全文浏览量: 590
- PDF下载量: 2