



-
心绞痛是心肌缺血最常见的症状之一,其发病人数在全球范围内高达1亿余人[1]。自1904年德国病理学家Marchand提出“动脉粥样硬化”这一定义以来,动脉粥样硬化和心外膜冠状动脉狭窄就一直被视为导致心绞痛的主要原因[2]。然而,近年的研究结果显示,70%的心肌缺血患者通过冠状动脉造影(coronary angiography,CAG)或冠状动脉CT血管造影并未发现明显的冠状动脉狭窄(狭窄程度≥50%)[3]。2020年欧洲非阻塞性冠状动脉缺血疾病专家共识[3]明确定义了缺血伴非阻塞性冠状动脉疾病(ischaemia and non-obstructive coronary arteries,INOCA)。INOCA的病理生理学机制复杂多样,其病因目前尚未完全明确,有研究结果表明,59%~89%的INOCA患者病因是由于冠状动脉微血管功能障碍(coronary microvascular dysfunction,CMD)引起[4- 5]。传统CAG对前小动脉和小动脉等冠状动脉微血管的评估价值有限[6],因此需要寻找一种新型的功能影像检查方法[7-9]。
SPECT心肌灌注显像(myocardial perfusion imaging, MPI)是一种被广泛认可的无创性诊断心肌缺血的功能影像手段,可以通过目测法和半定量参数反映患者心肌缺血的部位和程度。新一代碲锌镉(cadmium zinc telluride, CZT)心脏专用SPECT在性能方面得到了显著提高[10],不仅能获得传统的MPI半定量参数用于评估可逆性心肌缺血,而且还可以实现动态心肌灌注显像(dynamic myocardial perfusion imaging, D-MPI)及心肌血流量(myocardial blood flow, MBF)和心肌血流储备(myocardial flow reserve, MFR)的定量测定,提供全面的诊断信息。动物实验结果已经证实,CZT心脏专用SPECT在冠心病的诊断中具有一定的可行性和准确性[11],与PET测定的MFR的一致性也已得到临床验证[12]。
目前,CZT心脏专用SPECT提供的半定量参数在INOCA与阻塞性冠状动脉粥样硬化性心脏病(obstructive coronary artery disease, OCAD)患者预后评估中的价值已被验证[13]。而基于CZT心脏专用SPECT D-MPI定量参数(以下简称D-MPI定量参数)的预后评估价值方面的文献报道较少[14-15],尤其是关于 D-MPI定量参数与 MPI半定量参数的预后诊断效能的比较研究目前尚未见报道。本研究旨在探讨D-MPI定量参数在INOCA和OCAD患者预后评估中的诊断价值,并与MPI半定量参数进行比较。
-
回顾性分析2020年3月至2021年7月在泰达国际心血管病医院行CZT心脏专用SPECT D-MPI、具备显像前后3个月内的CAG资料并最终完成随访的100例INOCA患者[其中,男性37例、女性63例,年龄62.0(55.3,66.0)岁]和同期诊断为OCAD的203例患者[其中,男性122例、女性81例,年龄63.0(57.0,69.0)岁]。纳入标准:(1)年龄≥18岁;(2)初诊经心内科医师结合临床症状、体征及心电图等综合分析诊断为心肌缺血;(3)具备在SPECT D-MPI显像前后3个月内的CAG资料,且二者之间未进行血运重建治疗。排除标准:(1) 既往有明确的冠状动脉粥样硬化性心脏病(简称冠心病)病史,包括有陈旧性心肌梗死病史、接受过经皮冠状动脉介入治疗、冠状动脉旁路移植术治疗;(2)患有心肌病、严重的瓣膜性心脏病,或有严重的肝病、肾病和恶性肿瘤病史,预期生存期低于1年;(3)临床资料不完整;(4)存在腺苷或ATP药物负荷禁忌证。脱落标准:(1) 拒绝参与电话随访调查;(2) 调查问卷回答不完整。
患者在检查前均被告知ATP或腺苷药物负荷试验的试验过程和潜在风险,并签署了知情同意书。本研究获得泰达国际心血管病医院伦理委员会的批准(批准号:[2022]-0429-1)。
-
使用美国GE公司Discovery NM 530c 型CZT心脏专用SPECT仪,显像剂为99Tcm-MIBI(天津原子高科同位素医药有限公司)。严格要求患者显像前24 h不饮用茶、咖啡、可乐等饮品或食用任何含咖啡因与茶碱的食物,并停止服用各种心血管病药物(主要包括硝酸酯类、钙拮抗剂、β阻滞剂等)。显像方法采用一日法,先行静息显像,后行药物负荷显像,静息显像注射99Tcm-MIBI剂量为185~296 MBq,间隔1~4 h后,行ATP或腺苷药物负荷试验,药物负荷试验具体方案参见文献[16],负荷高峰时(第3 分钟末)注射静息显像3倍剂量(555~888 MBq)的显像剂。99Tcm-MIBI SPECT静息显像:预注射显像剂剂量为18.5~37.0 MBq(预定位显像用);预定位后先启动动态采集(表模式采集10 min),开启程序10 s后再经预埋静脉通道注射显像剂,注射方式采用“弹丸”式注射,在5 s内完成,动态采集结束后40~60 min行常规静息门控SPECT断层显像。99Tcm-MIBI SPECT药物负荷显像:心脏预定位后,在负荷高峰时注射99Tcm-MIBI显像剂,注射要求同静息显像,表模式连续采集10 min,间隔15~30 min后行常规药物负荷门控SPECT断层显像。常规门控采集参数:每个心动周期采集8帧图像,心率窗宽±15%,能峰140 keV,窗宽±10%,一日法静息和药物负荷显像分别采集6 min和4 min。所有患者SPECT显像前均使用美国GE公司Discovery NM 690型CT 采集衰减校正数据,CT图像采集条件:电压120 kV,电流20 mA,扫描范围为自肺尖至肝脏中下部。
将所有动态表模式数据传送至MyoflowQ工作站(北京百灵云生物医学科技有限公司),自动重分为系列动态图像:10 s×10次+20 s×5次+60 s×2次+280 s×1次;然后调用CT衰减校正数据进行完整的CT与SPECT图像的融合对位、轴位调整、衰减和散射校正;自动或手动调整心血池曲线输入函数的ROI和心肌基底部位置,生成左心室心血池、左心室心肌的动态曲线和拟合曲线,获得左心室三支血管区域的静息心肌血流量(rest myocardial blood flow, r-MBF)和负荷心肌血流量(stress myocardial blood flow, s-MBF),进而获得左心室三支血管区域的MFR,即s-MBF与r-MBF的比值,并采用静息收缩期血压与心率的乘积对r-MBF进行校正。按照美国心脏协会(AHA)17节段法[17]对左心室壁心肌进行区域划分,心肌节段放射性分布按5分法评估标准:0分为显像剂摄取正常;1分为显像剂摄取轻度减低;2分为显像剂摄取中度减低;3分为显像剂摄取重度减低;4分为显像剂摄取缺失。通过QGS+QPS软件(美国Cedars-Sinai医学中心)获得相应的半定量参数:总灌注缺损(total perfusion defect, TPD)、静息总积分(summed rest score, SRS)、负荷总积分(summed stress score, SSS)、差值总积分(summed different score, SDS)。MPI半定量参数异常定义为SSS≥4分且SDS≥2分。
-
依据患者行SPECT D-MPI检查的时间确定入组时间,电话随访在患者行SPECT D-MPI检查后每6个月进行一次,随访截止日期为2022年8月1日。生存期定义为从患者入组至主要不良心血管事件(major adverse cardiovascular events,MACE)发生或随访结束的时间。MACE定义为心源性死亡、非致死性心肌梗死、非致死性卒中、心力衰竭、非计划性的冠状动脉血运重建和心绞痛再住院。
-
应用IBM SPSS 26.0 软件、MedCalc 20.0软件及RStudio软件进行统计学分析。计数资料以频数和百分比表示,组间比较采用Pearson卡方检验。符合正态分布的计量资料以
$\bar x \pm s $ 表示,组间比较采用两独立样本t检验(方差齐);不符合正态分布的计量资料以M (Q1, Q3)表示,组间比较采用Mann-Whitney U检验。采用ROC曲线评估D-MPI定量参数与 MPI半定量参数预测INOCA和OCAD患者发生MACE的诊断效能。AUC>0.5提示具有诊断效能,AUC为0.7~0.9提示具有较高的诊断效能,数值越大提示诊断效能越高。根据Youden指数确定D-MPI定量参数和MPI半定量参数用于预测患者预后的最佳临界值。采用Delong检验和净重新分类指数(net reclassification index,NRI)对D-MPI定量参数和MPI半定量参数的诊断效能进行对比分析。P<0.05 为差异有统计学意义。 -
患者中位随访时间为16个月。100例INOCA患者中,无MACE组89例[男性29例、女性60例,年龄54.0(49.0,56.0)岁],有MACE组11例[男性8例、女性3例,年龄52.0(46.0,58.0)岁]。发生MACE的具体情况为心绞痛再住院10例(10.0%)、非致死性卒中1例(1.0%)。有MACE组男性患者比例高于无MACE组(χ2=6.768, P=0.009),但2组患者年龄的差异无统计学意义(Z=−0.011, P=0.991)。
203例OCAD患者中,无MACE组187例[男性112例、女性75例,年龄66.0 (63.0,70.0)岁],有MACE组16例[男性10例、女性6例,年龄67.0 (65.0,70.8)岁]。发生MACE的具体情况为心绞痛再住院11例(5.4%)、非计划性的冠状动脉血运重建2例(1.0%)、心力衰竭1例(0.5%)、非致死性卒中2例(1.0%)。有MACE组和无MACE组患者的性别(χ2=0.042,P=0.838)、年龄(Z=−1.249, P=0.212)的差异均无统计学意义。
-
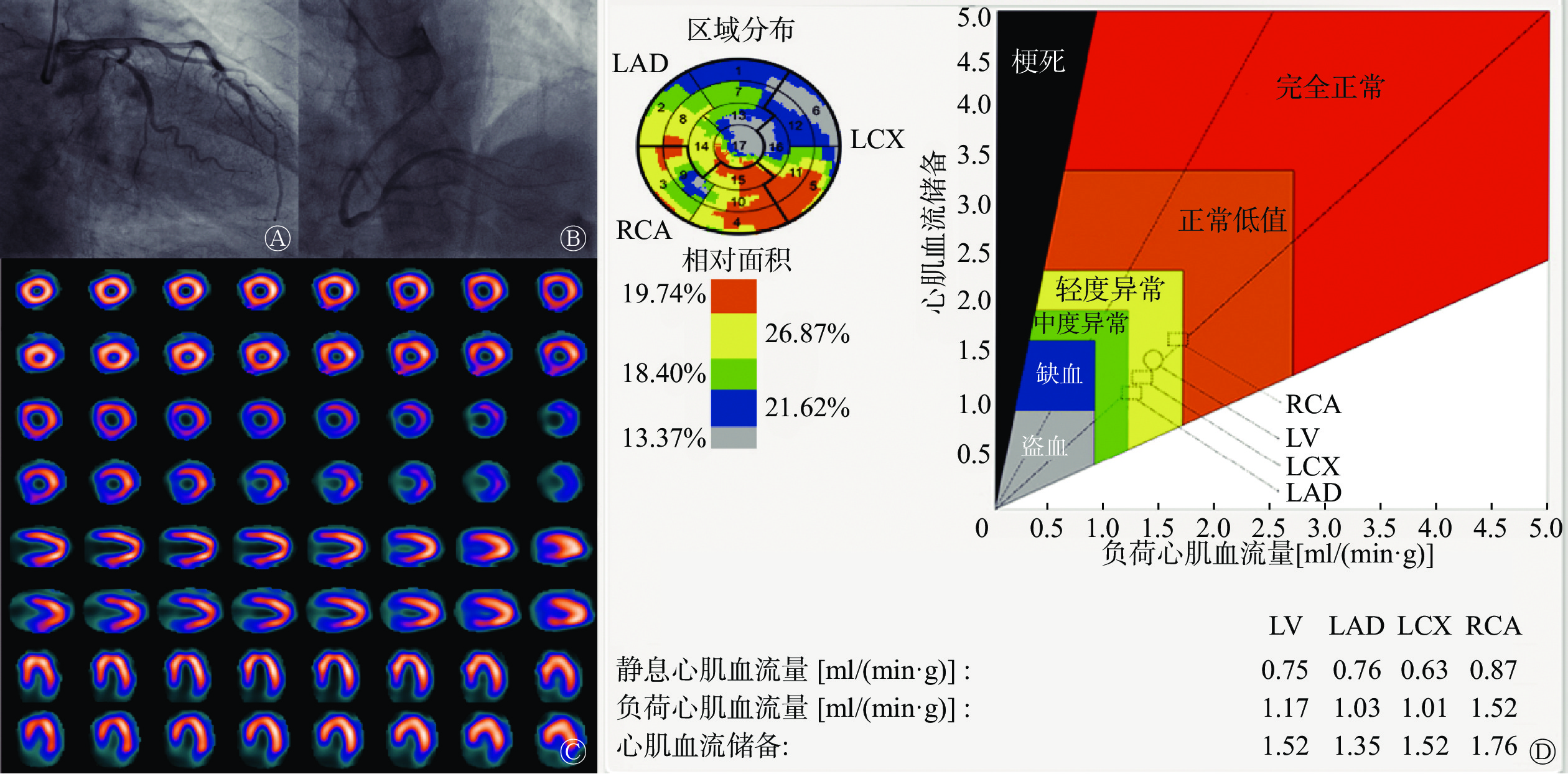
由表1可知,INOCA患者中有MACE组的s-MBF和MFR均显著低于无MACE组[1.27(1.03,1.88)ml/(min·g)对2.25(1.59,3.13)ml/(min·g)、1.65(1.35,2.04)对2.52(1.75,3.39)],差异均有统计学意义(Z=−2.986、−2.859,均P<0.05)。2组的r-MBF及MPI半定量参数[包括SSS、SRS、SDS、负荷TPD(stress TPD, s-TPD)、静息TPD(rest TPD,r-TPD)]的差异均无统计学意义(均P>0.05)。典型病例见图1。
组别 MFR
[M(Q1, Q3)]s-MBF
[ml/(min·g),M(Q1, Q3)]r-MBF
[ml/(min·g),M(Q1, Q3)]MPI半定量参数异常
[例(%)]SSS
[分,M(Q1, Q3)]有MACE组(n=11) 1.65(1.35, 2.04) 1.27(1.03, 1.88) 0.88(0.76, 0.93) 2(18.2) 2.00(1.00, 3.00) 无MACE组(n=89) 2.52(1.75, 3.39) 2.25(1.59, 3.13) 0.91(0.87, 0.93) 13(14.6) 1.00(0.00, 3.00) 检验值 Z=−2.859 Z=−2.986 Z=−1.269 χ2=0.098 Z=−1.013 P值 0.004 0.003 0.204 0.754 0.311 组别 SRS
[分,M(Q1, Q3)]SDS
[分,M(Q1, Q3)]s-TPD
[%,M(Q1, Q3)]r-TPD
[%,M(Q1, Q3)]有MACE组(n=11) 0.00(0.00, 0.00) 1.00(0.00, 3.00) 3.00(1.00, 6.00) 1.00(0.00, 2.00) 无MACE组(n=89) 0.00(0.00, 0.00) 1.00(0.00, 2.00) 1.00(0.50, 3.00) 1.00(0.00, 2.00) 检验值 Z=−0.156 Z=−0.963 Z=−1.543 Z=−0.104 P值 0.876 0.336 0.123 0.917 注: INOCA为缺血伴非阻塞性冠状动脉疾病;MACE为主要不良心血管事件;D-MPI为动态心肌灌注显像;MPI为心肌灌注显像;MFR为心肌血流储备;s-MBF为负荷心肌血流量;r-MBF为静息心肌血流量;SSS为负荷总积分;SRS为静息总积分;SDS为差值总积分;s-TPD为负荷总灌注缺损;r-TPD为静息总灌注缺损;MPI半定量参数异常定义为SSS≥4分且SDS≥2分 表 1 INOCA患者中无MACE组与有MACE组的D-MPI定量参数和MPI半定量参数的比较
Table 1. Comparison of quantitative parameters of dynamic myocardial perfusion imaging (D-MPI) and semi-quantitative parameters of myocardial perfusion imaging (MPI) between non-major adverse cardiovascular events (MACE) group and MACE group in ischaemia and non-obstructive coronary arteries (INOCA) patients
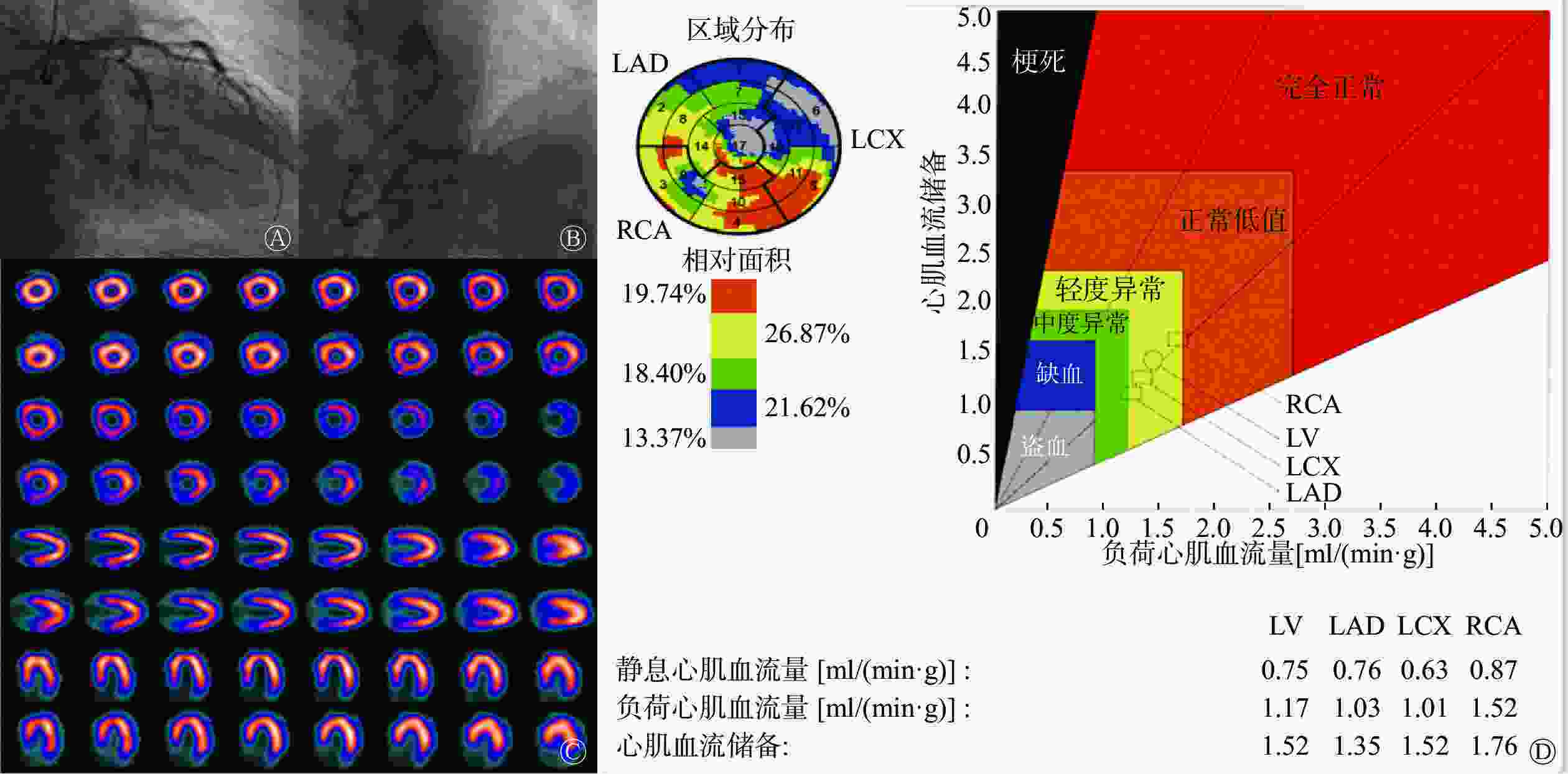
图 1 间断胸骨后疼痛10 d的INOCA患者(男性,58岁)的冠状动脉造影、99Tcm-MIBI心肌灌注显像和心肌血流定量图
Figure 1. Coronary angiography, 99Tcm-sestamibi (MIBI) myocardial perfusion imaging and quantitative myocardial flow images of the ischaemia and non-obstructive coronary arteries (INOCA) patient (male, 58 years old) with intermittent retrosternal pain for 10 days
-
由表2可知,OCAD患者中有MACE组的s-MBF和MFR均显著低于无MACE组[1.21(0.61, 1.51) ml/(min·g) 对1.76(1.14, 2.56) ml/(min·g)、1.51(0.81, 1.91)对2.02(1.50, 2.86)],差异均有统计学意义(Z=−2.891、−2.984,均P<0.05)。而2组间的r-MBF和 MPI半定量参数(包括SSS、SRS、SDS、s-TPD、r-TPD)的差异均无统计学意义(均P>0.05)。
组别 MFR
[M(Q1, Q3)]s-MBF
[ml/(min·g),M(Q1, Q3)]r-MBF
[ml/(min·g),M(Q1, Q3)]MPI半定量参数异常
[例(%)]SSS
[分,M(Q1, Q3)]有MACE组(n=16) 1.51(0.81, 1.91) 1.21(0.61, 1.51) 0.91(0.81, 0.91) 8(50.0) 4.01(2.01, 15.51) 无MACE组(n=187) 2.02(1.50, 2.86) 1.76(1.14, 2.56) 0.89(0.80, 0.93) 75(40.1) 3.00(1.00, 6.00) 检验值 Z=−2.984 Z=−2.891 Z=−1.366 χ2=0.597 Z=−1.777 P值 0.003 0.004 0.172 0.440 0.075 组别 SRS
[分,M(Q1, Q3)]SDS
[分,M(Q1, Q3)]s-TPD
[%,M(Q1, Q3)]r-TPD
[%,M(Q1, Q3)]有MACE组(n=16) 0.01(0.01, 11.01) 2.01(1.31, 5.81) 5.01(2.01, 21.51) 3.51(0.31, 12.81) 无MACE组(n=187) 0.00(0.00, 1.00) 2.00(1.00, 4.00) 3.00(1.00, 8.00) 2.00(1.00, 3.00) 检验值 Z=−1.713 Z=−0.668 Z=−1.297 Z=−1.524 P值 0.087 0.504 0.194 0.127 注: OCAD为阻塞性冠状动脉粥样硬化性心脏病;MACE为主要不良心血管事件;D-MPI为动态心肌灌注显像;MPI为心肌灌注显像;MFR为心肌血流储备;s-MBF为负荷心肌血流量;r-MBF为静息心肌血流量;SSS为负荷总积分;SRS为静息总积分;SDS为差值总积分;s-TPD为负荷总灌注缺损;r-TPD为静息总灌注缺损; MPI半定量参数异常定义为SSS≥4分且SDS≥2分 表 2 OCAD患者中无MACE组与有MACE组的D-MPI定量参数和MPI半定量参数的比较
Table 2. Comparison of quantitative parameters of dynamic myocardial perfusion imaging (D-MPI) and semi-quantitative parameters of myocardial perfusion imaging (MPI) between non-major adverse cardiovascular events (MACE) group and MACE group in obstructive coronary artery disease (OCAD) patients
-
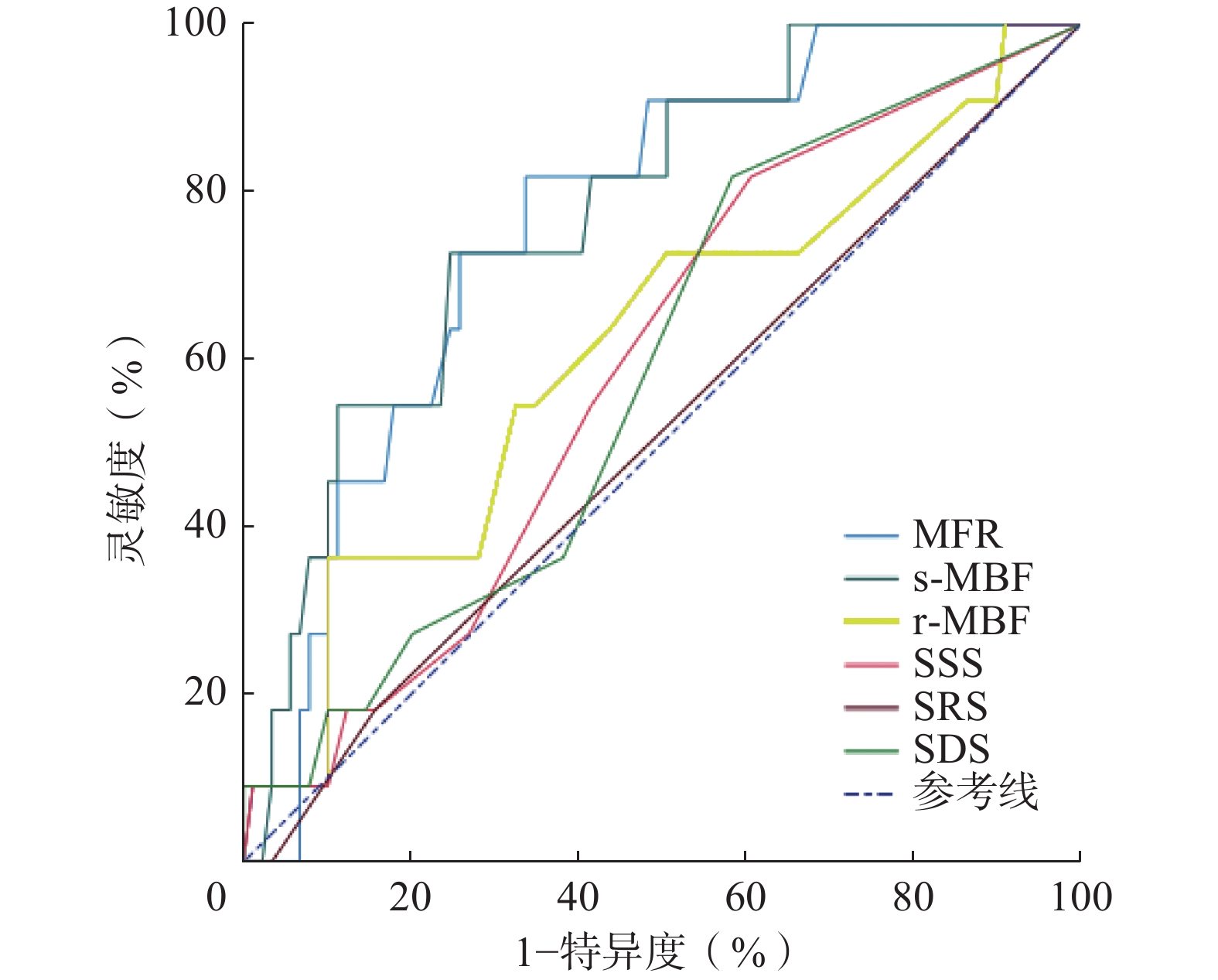
由图2可见,ROC曲线分析结果显示,s-MBF和MFR对于预测INOCA患者发生MACE具有较高的诊断效能(AUC=0.777、0.765,均P<0.001)。由表3可知, 当MFR临界值为2.04时,预测INOCA患者发生MACE的灵敏度为81.8%、特异度为66.3%;当s-MBF临界值为1.57 ml/(min·g)时,预测INOCA患者发生MACE的灵敏度为72.7%、特异度为75.3%。r-MBF和MPI半定量参数( 包括SSS、SRS、SDS、s-TPD、r-TPD)的诊断效能相对较弱(AUC=0.617、0.591、0.509、0.586、0.640、0.509,均P>0.05)。Delong检验结果显示,MFR和s-MBF均较SRS有更好的诊断效能,差异均有统计学意义(Z=3.244,P=0.001;Z=3.122,P=0.002)。其余D-MPI定量参数与 MPI半定量参数(包括SSS、SDS、s-TPD、r-TPD)间的差异均无统计学意义(均P>0.05)。采用NRI进一步验证s-MBF及MFR预测INOCA患者发生MACE的诊断效能,以s-MBF≤1.57 ml/(min·g)及MFR≤2.04对INOCA患者预后进行分类,NRI结果显示,与MPI半定量参数异常(SSS≥4分且SDS≥2分)比较,s-MBF≤1.57 ml/(min·g)对INOCA患者预后进行分类时NRI=0.444,正确分类比例提高了44.4%;MFR≤2.04对INOCA患者预后进行分类时NRI=0.445,正确分类比例提高了44.5%。
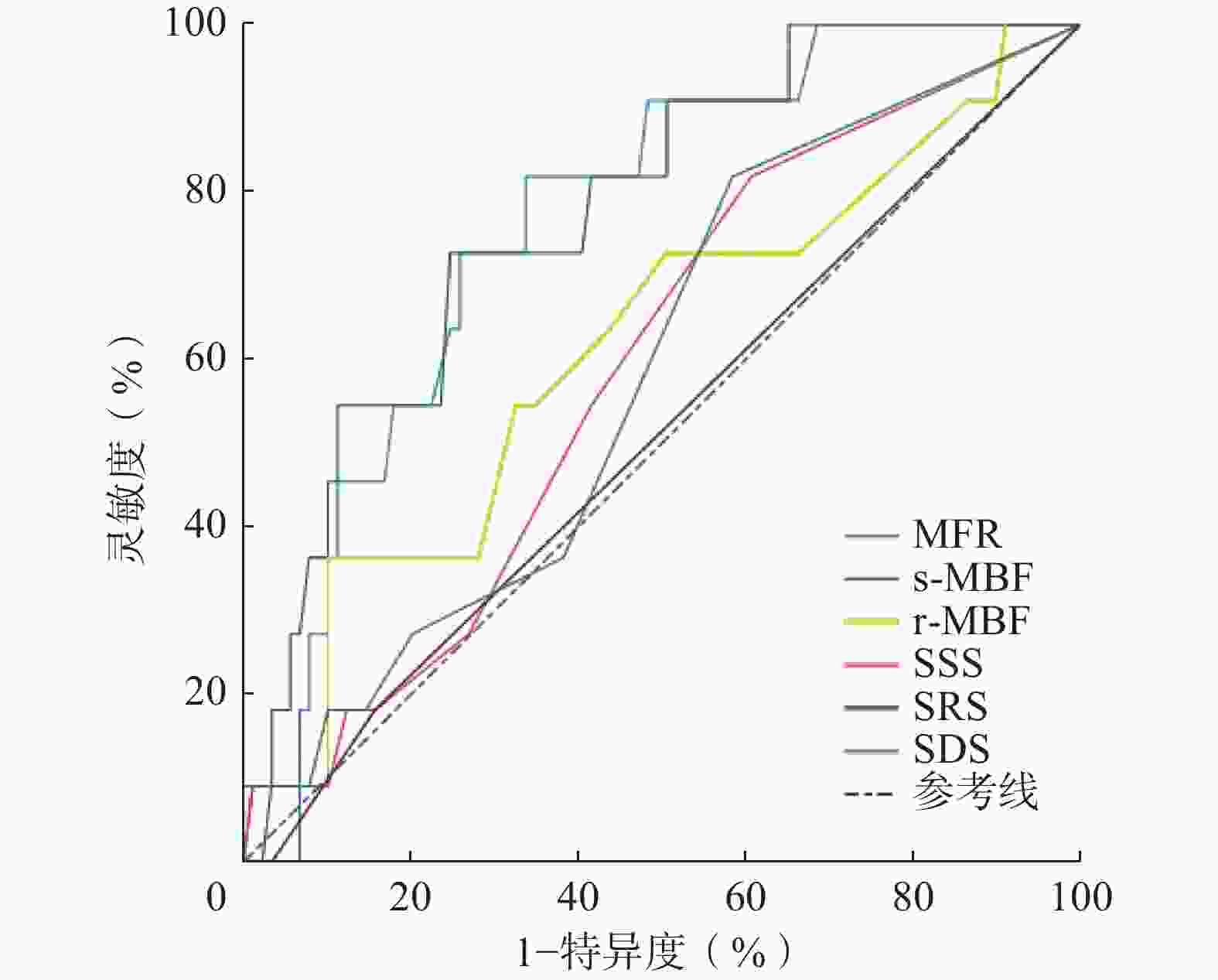
图 2 CZT心脏专用SPECT D-MPI定量参数和MPI半定量参数预测INOCA患者发生MACE的ROC曲线
Figure 2. Receiver operating characteristic (ROC) curves between quantitative parameters of cadmium zinc telluride (CZT) cardiac SPECT dynamic myocardial perfusion imaging (D-MPI) and semi-quantitative parameters of myocardial perfusion imaging (MPI) for predicting major adverse cardiovascular events (MACE) in ischaemia and non-obstructive coronary arteries (INOCA) patients
参数 AUC(95%CI) 临界值 Youden指数 灵敏度(%) 特异度(%) P值 MFR 0.765(0.670~0.844) 2.04 0.481 81.8 66.3 <0.001 s-MBF[ml/(min·g)] 0.777(0.683~0.854) 1.57 0.480 72.7 75.3 <0.001 r-MBF[ml/(min·g)] 0.617(0.514~0.712) 0.76 0.263 36.4 89.9 0.231 SSS(分) 0.591(0.488~0.688) 0.00 0.211 81.8 39.3 0.276 SRS(分) 0.509(0.407~0.611) 1.00 0.034 0.0 96.6 0.883 SDS(分) 0.586(0.483~0.683) 0.00 0.234 81.8 41.6 0.307 s-TPD(%) 0.640(0.538~0.734) 4.00 0.263 36.4 89.9 0.151 r-TPD(%) 0.509(0.407~0.611) 3.00 0.057 90.9 3.4 0.924 注:CZT为碲锌镉;SPECT为单光子发射计算机体层摄影术;D-MPI为动态心肌灌注显像;MPI为心肌灌注显像;INOCA为缺血伴非阻塞性冠状动脉疾病;MACE为主要不良心血管事件;AUC为曲线下面积;CI为置信区间;MFR为心肌血流储备;s-MBF为负荷心肌血流量;r-MBF为静息心肌血流量;SSS为负荷总积分;SRS为静息总积分;SDS为差值总积分;s-TPD为负荷总灌注缺损;r-TPD为静息总灌注缺损 表 3 CZT心脏专用SPECT D-MPI定量参数和MPI半定量参数预测INOCA患者发生MACE的诊断效能
Table 3. Comparison of quantitative parameters of cadmium zinc telluride (CZT) cardiac SPECT dynamic myocardial perfusion imaging (D-MPI) and semi-quantitative parameters of myocardial perfusion imaging (MPI) for predicting major adverse cardiovascular events (MACE) in ischaemia and non-obstructive coronary arteries (INOCA) patients
-
由图3可见,ROC曲线分析结果显示,MFR和s-MBF对于预测INOCA患者发生MACE具有较高的诊断效能(AUC=0.725、0.718,均P<0.001)。由表4可知,当MFR临界值为1.71时,预测OCAD患者发生MACE的灵敏度为75.0%、特异度为63.6%;当s-MBF临界值为1.49 ml/(min·g)时,预测OCAD患者发生MACE的灵敏度为81.3%、特异度为61.5%。r-MBF和MPI半定量参数(包括SSS、SRS、SDS、s-TPD、r-TPD)的诊断效能相对较弱(AUC=0.603、0.633、0.606、0.550、0.597、0.613,均P>0.05)。Delong检验结果显示,MFR和s-MBF均较SDS有更好的诊断效能,差异均有统计学意义(Z=2.639,P=0.008;Z=2.492,P=0.013)。其余D-MPI定量参数与 MPI半定量参数间的差异均无统计学意义(均P>0.05)。采用NRI进一步验证s-MBF及MFR预测OCAD患者发生MACE的诊断效能,以s-MBF≤1.49 ml/(min·g)及MFR≤1.71对OCAD患者预后进行分类,NRI结果显示,与MPI半定量参数异常(SSS≥4分且SDS≥2分)比较,s-MBF≤1.49 ml/(min·g)对OCAD患者预后进行分类时NRI=0.329,正确分类比例提高了32.9%;MFR≤1.71对OCAD患者预后进行分类时NRI=0.287,正确分类比例提高了28.7%。
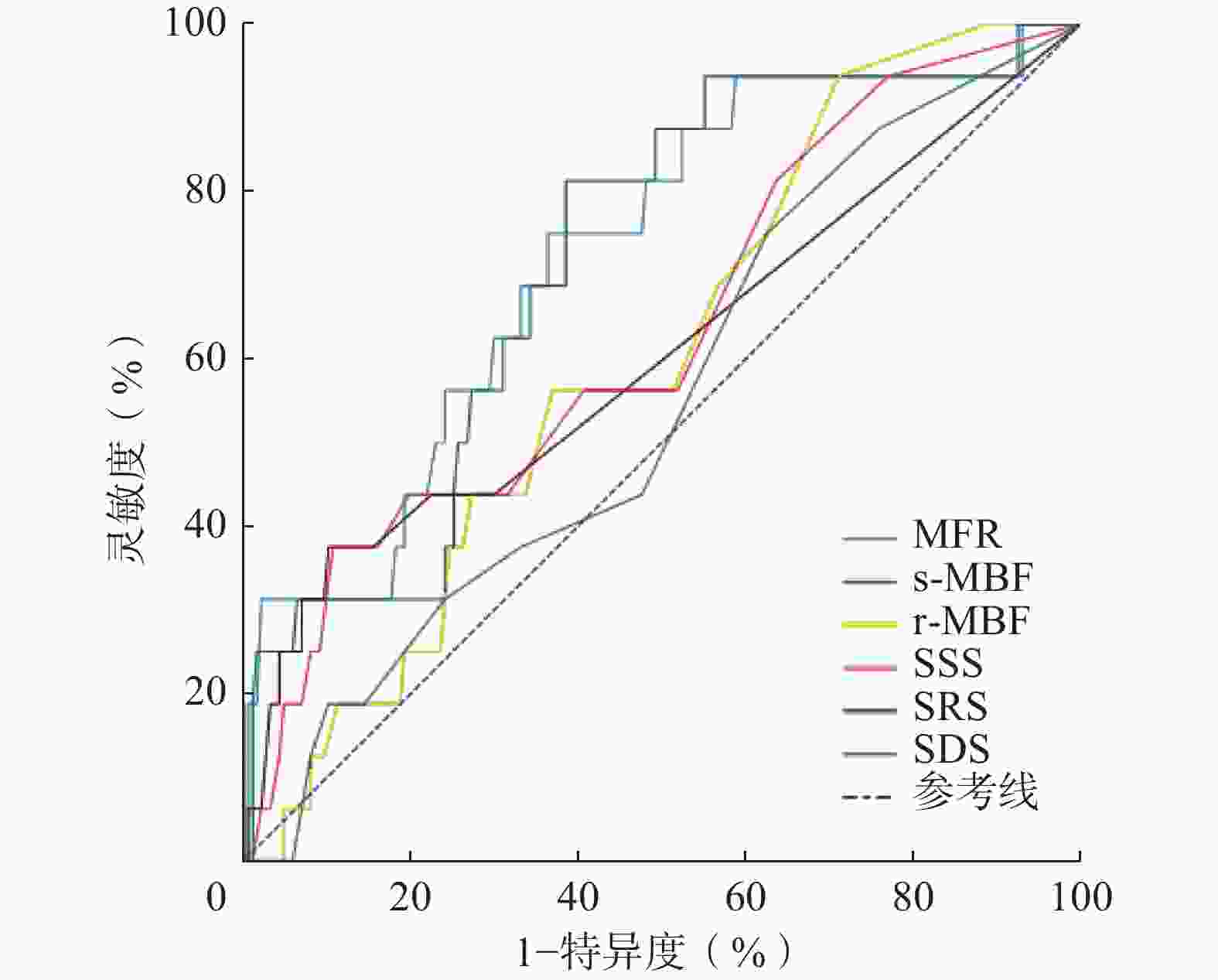
图 3 CZT心脏专用SPECT D-MPI定量参数和MPI半定量参数预测OCAD患者发生MACE的ROC曲线
Figure 3. Receiver operating characteristic (ROC) curves between quantitative parameters of cadmium zinc telluride (CZT) cardiac SPECT dynamic dynamic myocardial perfusion imaging (D-MPI) and semi-quantitative parameters of myocardial perfusion imaging (MPI) for predicting major adverse cardiovascular events (MACE) in obstructive coronary artery disease (OCAD) patients
参数 AUC(95%CI) 临界值 Youden指数 灵敏度(%) 特异度(%) P值 MFR 0.725(0.658~0.785) 1.71 0.386 75.0 63.6 <0.001 s-MBF[ml/(min·g)] 0.718(0.651~0.779) 1.49 0.428 81.3 61.5 <0.001 r-MBF [ml/(min·g)] 0.603(0.532~0.670) 0.92 0.226 93.8 28.9 0.115 SSS(分) 0.633(0.563~0.699) 13.00 0.268 37.5 89.3 0.078 SRS(分) 0.606(0.535~0.673) 4.00 0.273 37.5 89.8 0.168 SDS(分) 0.550(0.479~0.620) 1.00 0.124 75.0 37.4 0.488 s-TPD(%) 0.597(0.526~0.665) 11.00 0.261 43.8 82.4 0.257 r-TPD(%) 0.613(0.542~0.680) 4.00 0.361 50.0 86.1 0.212 注:CZT为碲锌镉;SPECT为单光子发射计算机体层摄影术;D-MPI为动态心肌灌注显像;MPI为心肌灌注显像;OCAD为阻塞性冠状动脉粥样硬化性心脏病;MACE为主要不良心血管事件;AUC为曲线下面积;CI为置信区间;MFR为心肌血流储备;s-MBF为负荷心肌血流量;r-MBF为静息心肌血流量;SSS为负荷总积分;SRS为静息总积分;SDS为差值总积分;s-TPD为负荷总灌注缺损;r-TPD为静息总灌注缺损 表 4 CZT心脏专用SPECT D-MPI定量参数和SPECT MPI半定量参数预测OCAD患者发生MACE的诊断效能
Table 4. Comparison of quantitative parameters of cadmium zinc telluride (CZT) cardiac SPECT dynamic myocardial perfusion imaging (D-MPI) and semi-quantitative parameters of myocardial perfusion imaging (MPI) for predicting major adverse cardiovascular events (MACE) in obstructive coronary artery disease (OCAD) patients
-
近年来的研究结果显示,因心肌缺血症状接受CAG的心绞痛患者中,INOCA的发病率可高达70%[3],多项研究结果表明INOCA患者的预后不良[13, 18]。INOCA的发病机制多样、异质性很高,各种定量方法获得的MFR减低可提示CMD,从而使部分INOCA患者受益于CMD的早期诊断、分层治疗和管理[19]。
SPECT MPI是评估心肌灌注的经典方法,在过去的几十年里,SPECT MPI在冠心病的诊断和预后评估中的作用不断被证实。1998年,Iskander和Iskandrian[20]纳入12 000例患者的Meta分析结果显示,MPI结果正常的患者发生心肌梗死或死亡的风险为0.6%,MPI结果异常的患者为7.4%。但是由于传统MPI是通过专门的软件将患者的心肌核素放射性分布图像与“正常参考段”或“正常数据库”进行比较,从而获得相应的MPI半定量参数(SSS、SDS、SRS和TPD等)用于判断冠心病患者心肌缺血的程度,对于左主干病变、三支病变或CMD造成的多支区域缺血和(或)均衡性缺血等容易出现低估和(或)假阴性结果[21]。随着影像技术的发展,CZT心脏专用SPECT由于能量分辨率、系统灵敏度和空间分辨率等方面的性能大幅提升,能够实现D-MPI,获得心肌血流的定量参数MFR和MBF[22-23]。CZT心脏专用SPECT D-MPI测定的MFR与公认的无创测定“金标准”PET D-MPI测定的MFR的一致性也得到了验证[12],且成本较PET更低。
Panjer等[24]通过将CZT心脏专用SPECT D-MPI与CAG、PET等“金标准”进行对比,证明了其在诊断冠心病方面具有良好的灵敏度和特异度。Liu等[13]对232例INOCA患者和274例OCAD患者的随访研究结果显示,CZT心脏专用SPECT MPI半定量参数在INOCA和OCAD患者中都表现出了较好的预后预测价值。然而,有关CZT心脏专用SPECT D-MPI定量参数对INOCA患者的预后价值评估方面的研究较少,D-MPI定量参数与MPI半定量参数对INOCA患者的预后预测效能比较的研究尚未见报道。Zhang等[15]对118例INOCA患者进行的随访研究结果表明,有MACE组患者的s-MBF和MFR较无MACE组患者显著减低。本研究结果与该文献结果一致。本研究中,ROC曲线分析结果表明,CZT心脏专用SPECT D-MPI定量参数MFR和s-MBF对预测INOCA及OCAD患者的预后均具有较高的诊断效能(AUC为0.7~0.9),而MPI半定量参数的诊断效能相对较低(AUC<0.7)。为了进一步对比D-MPI定量参数和MPI半定量参数的诊断效能,我们通过Delong检验和NRI对INOCA患者发生MACE进行验证,结果显示s-MBF和MFR对于预测INOCA患者发生MACE均较SRS有更高的诊断效能;MFR≤2.04和s-MBF≤1.57 ml/(min·g)较MPI半定量参数异常对于预测INOCA患者发生MACE有更高的诊断效能。通过Delong检验和NRI对OCAD患者发生MACE进行验证,结果显示s-MBF和MFR对于预测OCAD患者发生MACE均较SDS有更高的诊断效能;MFR≤1.71和s-MBF≤1.49 ml/(min·g) 较MPI半定量参数异常对于预测OCAD患者发生MACE有更高的诊断效能。
本研究存在一定的局限性:(1)本研究为单中心研究、样本量有限,需进一步进行多中心研究寻找更为精确的临界值用于INOCA和OCAD患者的预后评估;(2)本研究的中位随访时间为16个月,相对较短,患者的远期预后需要更长的随访时间进行评估。
综上所述, CZT心脏专用SPECT D-MPI提供的定量参数MFR和s-MBF对INOCA和OCAD患者发生MACE均表现出较高的诊断效能,尤其对于INOCA患者而言,MPI半定量参数的预后诊断价值十分有限,难以对患者进行进一步的危险分层,而D-MPI提供的定量参数MFR和s-MBF则表现出更高的增益诊断价值。
利益冲突 所有作者声明无利益冲突
作者贡献声明 李琳琳负责文献的检索、数据的收集与统计分析、论文的撰写与修改;庞泽堃、陈越、汪娇负责数据的收集与分析;李剑明负责命题的提出与设计、论文的修改与审阅
碲锌镉心脏专用SPECT动态心肌灌注显像定量参数在INOCA和OCAD患者预后评估中的诊断价值
Diagnostic value of dynamic myocardial perfusion imaging quantitative parameters of cadmium zinc telluride cardiac SPECT in prognostic assessment of patients with INOCA and OCAD
-
摘要:
目的 探究碲锌镉(CZT)心脏专用SPECT动态心肌灌注显像(D-MPI)定量参数在缺血伴非阻塞性冠状动脉疾病(INOCA)和阻塞性冠状动脉粥样硬化性心脏病(OCAD)患者预后评估中的诊断价值,并与心肌灌注显像(MPI)半定量参数进行比较。 方法 回顾性分析2020年3月至2021年7月于泰达国际心血管病医院行CZT心脏专用SPECT D-MPI、具备显像前后3个月内的冠状动脉造影(CAG)资料并最终完成随访的100例INOCA患者[其中,男性37例、女性63例,年龄62.0(55.3,66.0)岁]和同期诊断为OCAD的203例患者[其中,男性122例、女性81例,年龄63.0(57.0,69.0)岁]的临床资料,随访内容为主要不良心血管事件(MACE)的发生情况。根据随访结果将INOCA和OCAD患者分别分为无MACE组和有MACE组。比较无MACE组与有MACE组患者的D-MPI定量参数[心肌血流储备(MFR)、静息心肌血流量( r-MBF)和负荷心肌血流量(s-MBF)]及MPI半定量参数[负荷总积分(SSS)、静息总积分(SRS)、总积分差(SDS)、负荷总灌注缺损(s-TPD)和静息总灌注缺损(r-TPD)]间的差异。计量资料的组间比较采用两独立样本t检验或Mann-Whitney U检验,计数资料的组间比较采用Pearson卡方检验。采用受试者工作特征(ROC)曲线评估D-MPI定量参数和MPI半定量参数预测INOCA和OCAD患者发生MACE的诊断效能。采用Delong检验和净重新分类指数(NRI)进一步验证D-MPI定量参数和MPI半定量参数的诊断效能的差异。 结果 100例INOCA患者中,有MACE组的s-MBF和MFR均显著低于无MACE组[1.27(1.03,1.88) ml/(min·g)对2.25(1.59,3.13) ml/(min·g)、1.65(1.35,2.04)对2.52(1.75,3.39)],差异均有统计学意义(Z=−2.986、−2.859, 均P<0.05)。ROC曲线分析结果显示,s-MBF和MFR对预测INOCA患者发生MACE具有较高的诊断效能[曲线下面积(AUC)=0.777、0.765,均P<0.001],当s-MBF临界值为1.57 ml/(min·g)时,预测INOCA患者MACE的灵敏度为72.7%、特异度为75.3%;当MFR临界值为2.04时,预测INOCA患者MACE的灵敏度为81.8%、特异度为66.3%。NRI结果显示,s-MBF≤1.57 ml/(min·g)、MFR≤2.04对于INOCA患者预后的正确分类比例较MPI半定量参数异常(SSS≥4分且SDS≥2分)分别提高了44.4%和44.5%。203例OCAD患者中,有MACE组的s-MBF和MFR均显著低于无MACE组[1.21(0.61,1.51) ml/(min·g) 对1.76(1.14,2.56) ml/(min·g)、1.51(0.81,1.91)对2.02(1.50,2.86)],差异均有统计学意义(Z=−2.891、−2.984,均P<0.05)。ROC曲线分析结果显示,MFR和s-MBF对预测OCAD患者发生MACE具有较高的诊断效能(AUC=0.725、0.718,均P<0.001 ),当MFR临界值为1.71时,预测OCAD患者MACE的灵敏度为75.0%、特异度为63.6%;当s-MBF临界值为1.49 ml/(min·g)时,预测OCAD患者MACE的灵敏度为81.3%、特异度为61.5%。NRI结果显示,s-MBF≤1.49 ml/(min·g)、MFR≤1.71对于OCAD患者预后的正确分类比例较MPI半定量参数异常(SSS≥4分且SDS≥2分)分别提高了32.9%和28.7%。 结论 CZT心脏专用SPECT D-MPI获得的MFR和s-MBF均可以作为预测INOCA及OCAD患者发生MACE的诊断指标,并具有较好的预后诊断效能,与MPI半定量参数相比,能为临床提供更准确的预后评估。 Abstract:Objective To investigate the diagnostic value of cadmium zinc telluride (CZT) cardiac SPECT dynamic myocardial perfusion imaging (D-MPI) quantitative parameters in prognostic assessment of patients with ischaemia and non-obstructive coronary arteries (INOCA) and obstructive coronary artery disease (OCAD). These parameters were compared with myocardial perfusion imaging (MPI) semi-quantitative parameters. Methods Retrospective analysis was performed on patients who received CZT cardiac SPECT D-MPI in TEDA International Cardiovascular Hospital from March 2020 to July 2021, had coronary angiography data before and after D-MPI, and completed follow-up. A total of 100 patients with INOCA (37 males and 63 females, aged 62.0(55.3, 66.0) years) and 203 patients with OCAD (122 males and 81 females, aged 63.0(57.0, 69.0) years) were followed for major adverse cardiovascular events (MACE). According to MACE results, patients with INOCA were divided into the MACE and non-MACE groups, similar to patients with OCAD. The D-MPI quantitative parameters (including myocardial flow reserve (MFR), rest myocardial blood flow (r-MBF), and stress myocardial blood flow (s-MBF)) and MPI semi-quantitative parameters (including summed stress score (SSS), summed rest score (SRS), summed different score (SDS), stress total perfusion defect (s-TPD) and rest total perfusion defect (r-TPD)) were compared between the MACE group and the non-MACE group. Two independent sample t-test or the Mann-Whitney U test were used to compare measurement data between groups, and the Pearson′s chi-square test was used to compare counting data between groups. The receiver operating characteristic (ROC) curve was used to evaluate the diagnostic efficacy of quantitative parameters of D-MPI and semi-quantitative parameters of MPI in predicting MACE in patients with INOCA and OCAD. The Delong test and net reclassification index (NRI) were used to verify the differences in diagnostic efficacy between D-MPI quantitative parameters and MPI semi-quantitative parameters. Results Among the 100 patients with INOCA, s-MBF and MFR in the MACE group were significantly lower than those in the non-MACE group (1.27(1.03, 1.88) ml/(min·g) vs. 2.25(1.59, 3.13) ml/(min·g); 1.65(1.35, 2.04) vs. 2.52(1.75, 3.39)), and the differences were statistically significant (Z=−2.986 and −2.859, both P<0.05). ROC curve analysis showed that s-MBF and MFR had high diagnostic efficiency in predicting MACE in patients with INOCA (area under curve (AUC)=0.777 and 0.765, both P<0.001). When the cut-off value of s-MBF was 1.57 mL/(min·g), the sensitivity and specificity of predicting MACE in patients with INOCA were 72.7% and 75.3%, respectively. When the cut-off value of MFR was 2.04, the sensitivity and specificity of predicting MACE in patients with INOCA were 81.8% and 66.3%, respectively. According to NRI results, the proportion of correct classification in prognosis of INOCA patients with s-MBF≤1.57 ml/(min·g) and MFR≤2.04 was 44.4% and 44.5% higher than that of abnormal MPI semi-quantitative parameters (SSS≥4 and SDS≥2). Among 203 patients with OCAD, s-MBF and MFR in the MACE group were significantly lower than those in the non-MACE group (1.21 (0.61, 1.51) ml/(min·g) vs. 1.76 (1.14, 2.56) ml/(min·g); 1.51 (0.81, 1.91) vs. 2.02(1.50, 2.86)), and the differences were statistically significant (Z=−2.891 and −2.984, both P<0.05). ROC curve analysis showed that MFR and s-MBF had high diagnostic efficacy in predicting MACE in patients with OCAD (AUC=0.725 and 0.718, both P<0.001). When the cut-off value of MFR was 1.71, the sensitivity and specificity of predicting MACE in patients with OCAD were 75.0% and 63.6%, respectively. When the cut-off value of s-MBF was 1.49 ml/(min·g), the sensitivity and specificity of predicting MACE in patients with OCAD were 81.3% and 61.5%, respectively. According to NRI results, the proportion of correct classification in prognosis of OCAD patients with s-MBF≤1.49 ml/(min·g) and MFR≤1.71 was 32.9% and 28.7% higher than that of abnormal MPI semi-quantitative parameters (SSS≥4 and SDS≥2). Conclusions MFR and s-MBF obtained by CZT cardiac SPECT D-MPI can be used to indicate the occurence of MACE in patients with INOCA and OCAD and have good predictive diagnostic efficacy. Compared with MPI semi-quantitative parameters, MFR and s-MBF provide more accurate prognostic evaluation for clinical practice. -
图 1 间断胸骨后疼痛10 d的INOCA患者(男性,58岁)的冠状动脉造影、99Tcm-MIBI心肌灌注显像和心肌血流定量图
Figure 1. Coronary angiography, 99Tcm-sestamibi (MIBI) myocardial perfusion imaging and quantitative myocardial flow images of the ischaemia and non-obstructive coronary arteries (INOCA) patient (male, 58 years old) with intermittent retrosternal pain for 10 days
图 2 CZT心脏专用SPECT D-MPI定量参数和MPI半定量参数预测INOCA患者发生MACE的ROC曲线
Figure 2. Receiver operating characteristic (ROC) curves between quantitative parameters of cadmium zinc telluride (CZT) cardiac SPECT dynamic myocardial perfusion imaging (D-MPI) and semi-quantitative parameters of myocardial perfusion imaging (MPI) for predicting major adverse cardiovascular events (MACE) in ischaemia and non-obstructive coronary arteries (INOCA) patients
图 3 CZT心脏专用SPECT D-MPI定量参数和MPI半定量参数预测OCAD患者发生MACE的ROC曲线
Figure 3. Receiver operating characteristic (ROC) curves between quantitative parameters of cadmium zinc telluride (CZT) cardiac SPECT dynamic dynamic myocardial perfusion imaging (D-MPI) and semi-quantitative parameters of myocardial perfusion imaging (MPI) for predicting major adverse cardiovascular events (MACE) in obstructive coronary artery disease (OCAD) patients
表 1 INOCA患者中无MACE组与有MACE组的D-MPI定量参数和MPI半定量参数的比较
Table 1. Comparison of quantitative parameters of dynamic myocardial perfusion imaging (D-MPI) and semi-quantitative parameters of myocardial perfusion imaging (MPI) between non-major adverse cardiovascular events (MACE) group and MACE group in ischaemia and non-obstructive coronary arteries (INOCA) patients
组别 MFR
[M(Q1, Q3)]s-MBF
[ml/(min·g),M(Q1, Q3)]r-MBF
[ml/(min·g),M(Q1, Q3)]MPI半定量参数异常
[例(%)]SSS
[分,M(Q1, Q3)]有MACE组(n=11) 1.65(1.35, 2.04) 1.27(1.03, 1.88) 0.88(0.76, 0.93) 2(18.2) 2.00(1.00, 3.00) 无MACE组(n=89) 2.52(1.75, 3.39) 2.25(1.59, 3.13) 0.91(0.87, 0.93) 13(14.6) 1.00(0.00, 3.00) 检验值 Z=−2.859 Z=−2.986 Z=−1.269 χ2=0.098 Z=−1.013 P值 0.004 0.003 0.204 0.754 0.311 组别 SRS
[分,M(Q1, Q3)]SDS
[分,M(Q1, Q3)]s-TPD
[%,M(Q1, Q3)]r-TPD
[%,M(Q1, Q3)]有MACE组(n=11) 0.00(0.00, 0.00) 1.00(0.00, 3.00) 3.00(1.00, 6.00) 1.00(0.00, 2.00) 无MACE组(n=89) 0.00(0.00, 0.00) 1.00(0.00, 2.00) 1.00(0.50, 3.00) 1.00(0.00, 2.00) 检验值 Z=−0.156 Z=−0.963 Z=−1.543 Z=−0.104 P值 0.876 0.336 0.123 0.917 注: INOCA为缺血伴非阻塞性冠状动脉疾病;MACE为主要不良心血管事件;D-MPI为动态心肌灌注显像;MPI为心肌灌注显像;MFR为心肌血流储备;s-MBF为负荷心肌血流量;r-MBF为静息心肌血流量;SSS为负荷总积分;SRS为静息总积分;SDS为差值总积分;s-TPD为负荷总灌注缺损;r-TPD为静息总灌注缺损;MPI半定量参数异常定义为SSS≥4分且SDS≥2分  下载: 导出CSV
下载: 导出CSV
表 2 OCAD患者中无MACE组与有MACE组的D-MPI定量参数和MPI半定量参数的比较
Table 2. Comparison of quantitative parameters of dynamic myocardial perfusion imaging (D-MPI) and semi-quantitative parameters of myocardial perfusion imaging (MPI) between non-major adverse cardiovascular events (MACE) group and MACE group in obstructive coronary artery disease (OCAD) patients
组别 MFR
[M(Q1, Q3)]s-MBF
[ml/(min·g),M(Q1, Q3)]r-MBF
[ml/(min·g),M(Q1, Q3)]MPI半定量参数异常
[例(%)]SSS
[分,M(Q1, Q3)]有MACE组(n=16) 1.51(0.81, 1.91) 1.21(0.61, 1.51) 0.91(0.81, 0.91) 8(50.0) 4.01(2.01, 15.51) 无MACE组(n=187) 2.02(1.50, 2.86) 1.76(1.14, 2.56) 0.89(0.80, 0.93) 75(40.1) 3.00(1.00, 6.00) 检验值 Z=−2.984 Z=−2.891 Z=−1.366 χ2=0.597 Z=−1.777 P值 0.003 0.004 0.172 0.440 0.075 组别 SRS
[分,M(Q1, Q3)]SDS
[分,M(Q1, Q3)]s-TPD
[%,M(Q1, Q3)]r-TPD
[%,M(Q1, Q3)]有MACE组(n=16) 0.01(0.01, 11.01) 2.01(1.31, 5.81) 5.01(2.01, 21.51) 3.51(0.31, 12.81) 无MACE组(n=187) 0.00(0.00, 1.00) 2.00(1.00, 4.00) 3.00(1.00, 8.00) 2.00(1.00, 3.00) 检验值 Z=−1.713 Z=−0.668 Z=−1.297 Z=−1.524 P值 0.087 0.504 0.194 0.127 注: OCAD为阻塞性冠状动脉粥样硬化性心脏病;MACE为主要不良心血管事件;D-MPI为动态心肌灌注显像;MPI为心肌灌注显像;MFR为心肌血流储备;s-MBF为负荷心肌血流量;r-MBF为静息心肌血流量;SSS为负荷总积分;SRS为静息总积分;SDS为差值总积分;s-TPD为负荷总灌注缺损;r-TPD为静息总灌注缺损; MPI半定量参数异常定义为SSS≥4分且SDS≥2分
下载: 导出CSV
表 3 CZT心脏专用SPECT D-MPI定量参数和MPI半定量参数预测INOCA患者发生MACE的诊断效能
Table 3. Comparison of quantitative parameters of cadmium zinc telluride (CZT) cardiac SPECT dynamic myocardial perfusion imaging (D-MPI) and semi-quantitative parameters of myocardial perfusion imaging (MPI) for predicting major adverse cardiovascular events (MACE) in ischaemia and non-obstructive coronary arteries (INOCA) patients
参数 AUC(95%CI) 临界值 Youden指数 灵敏度(%) 特异度(%) P值 MFR 0.765(0.670~0.844) 2.04 0.481 81.8 66.3 <0.001 s-MBF[ml/(min·g)] 0.777(0.683~0.854) 1.57 0.480 72.7 75.3 <0.001 r-MBF[ml/(min·g)] 0.617(0.514~0.712) 0.76 0.263 36.4 89.9 0.231 SSS(分) 0.591(0.488~0.688) 0.00 0.211 81.8 39.3 0.276 SRS(分) 0.509(0.407~0.611) 1.00 0.034 0.0 96.6 0.883 SDS(分) 0.586(0.483~0.683) 0.00 0.234 81.8 41.6 0.307 s-TPD(%) 0.640(0.538~0.734) 4.00 0.263 36.4 89.9 0.151 r-TPD(%) 0.509(0.407~0.611) 3.00 0.057 90.9 3.4 0.924 注:CZT为碲锌镉;SPECT为单光子发射计算机体层摄影术;D-MPI为动态心肌灌注显像;MPI为心肌灌注显像;INOCA为缺血伴非阻塞性冠状动脉疾病;MACE为主要不良心血管事件;AUC为曲线下面积;CI为置信区间;MFR为心肌血流储备;s-MBF为负荷心肌血流量;r-MBF为静息心肌血流量;SSS为负荷总积分;SRS为静息总积分;SDS为差值总积分;s-TPD为负荷总灌注缺损;r-TPD为静息总灌注缺损
下载: 导出CSV
表 4 CZT心脏专用SPECT D-MPI定量参数和SPECT MPI半定量参数预测OCAD患者发生MACE的诊断效能
Table 4. Comparison of quantitative parameters of cadmium zinc telluride (CZT) cardiac SPECT dynamic myocardial perfusion imaging (D-MPI) and semi-quantitative parameters of myocardial perfusion imaging (MPI) for predicting major adverse cardiovascular events (MACE) in obstructive coronary artery disease (OCAD) patients
参数 AUC(95%CI) 临界值 Youden指数 灵敏度(%) 特异度(%) P值 MFR 0.725(0.658~0.785) 1.71 0.386 75.0 63.6 <0.001 s-MBF[ml/(min·g)] 0.718(0.651~0.779) 1.49 0.428 81.3 61.5 <0.001 r-MBF [ml/(min·g)] 0.603(0.532~0.670) 0.92 0.226 93.8 28.9 0.115 SSS(分) 0.633(0.563~0.699) 13.00 0.268 37.5 89.3 0.078 SRS(分) 0.606(0.535~0.673) 4.00 0.273 37.5 89.8 0.168 SDS(分) 0.550(0.479~0.620) 1.00 0.124 75.0 37.4 0.488 s-TPD(%) 0.597(0.526~0.665) 11.00 0.261 43.8 82.4 0.257 r-TPD(%) 0.613(0.542~0.680) 4.00 0.361 50.0 86.1 0.212 注:CZT为碲锌镉;SPECT为单光子发射计算机体层摄影术;D-MPI为动态心肌灌注显像;MPI为心肌灌注显像;OCAD为阻塞性冠状动脉粥样硬化性心脏病;MACE为主要不良心血管事件;AUC为曲线下面积;CI为置信区间;MFR为心肌血流储备;s-MBF为负荷心肌血流量;r-MBF为静息心肌血流量;SSS为负荷总积分;SRS为静息总积分;SDS为差值总积分;s-TPD为负荷总灌注缺损;r-TPD为静息总灌注缺损
下载: 导出CSV
-
[1] GBD 2015 Mortality and Causes of Death Collaborators. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980-2015: a systematic analysis for the Global Burden of Disease Study 2015[J]. Lancet, 2016, 388(10053): 1459−1544. DOI: 10.1016/S0140-6736(16)31012-1. [2] Schwartz CJ, Valente AJ, Kelley JL, et al. Thrombosis and the development of atherosclerosis: rokitansky revisited[J]. Semin Thromb Hemost, 1988, 14(2): 189−195. DOI: 10.1055/s-2007-1002775. [3] Kunadian V, Chieffo A, Camici PG, et al. An EAPCI expert consensus document on ischaemia with non-obstructive coronary arteries in collaboration with European society of cardiology working group on coronary pathophysiology & microcirculation endorsed by coronary vasomotor disorders international study group[J]. Eur Heart J, 2020, 41(37): 3504−3520. DOI: 10.1093/eurheartj/ehaa503. [4] Del Buono MG, Montone RA, Camilli M, et al. Coronary microvascular dysfunction across the spectrum of cardiovascular diseases: JACC state-of-the-art review[J]. J Am Coll Cardiol, 2021, 78(13): 1352−1371. DOI: 10.1016/j.jacc.2021.07.042. [5] Hansen B, Holtzman JN, Juszczynski C, et al. Ischemia with no obstructive arteries (INOCA): a review of the prevalence, diagnosis and management[J]. Curr Probl Cardiol, 2023, 48(1): 101420. DOI: 10.1016/j.cpcardiol.2022.101420. [6] Lyon AR, Citro R, Schneider B, et al. Pathophysiology of takotsubo syndrome: JACC state-of-the-art review[J]. J Am Coll Cardiol, 2021, 77(7): 902−921. DOI: 10.1016/j.jacc.2020.10.060. [7] Deussen A, Ohanyan V, Jannasch A, et al. Mechanisms of metabolic coronary flow regulation[J]. J Mol Cell Cardiol, 2012, 52(4): 794−801. DOI: 10.1016/j.yjmcc.2011.10.001. [8] Guo R, Weingärtner S, Šiurytė P, et al. Emerging techniques in cardiac magnetic resonance imaging[J]. J Magn Reson Imaging, 2022, 55(4): 1043−1059. DOI: 10.1002/jmri.27848. [9] Rush CJ, Berry C, Oldroyd KG, et al. Prevalence of coronary artery disease and coronary microvascular dysfunction in patients with heart failure with preserved ejection fraction[J/OL]. JAMA Cardiol, 2021, 6(10): 1130−1143[2023-07-06].https://jamanetwork.com/journals/jamacardiology/fullarticle/2781078. DOI: 10.1001/jamacardio.2021.1825. [10] Sharir T, Slomka PJ, Berman DS. Solid-state SPECT technology: fast and furious[J]. J Nucl Cardiol, 2010, 17(5): 890−896. DOI: 10.1007/s12350-010-9284-5. [11] Wells RG, Timmins R, Klein R, et al. Dynamic SPECT measurement of absolute myocardial blood flow in a porcine model[J]. J Nucl Med, 2014, 55(10): 1685−1691. DOI: 10.2967/jnumed.114.139782. [12] Hsu B, Hu LH, Yang BH, et al. SPECT myocardial blood flow quantitation toward clinical use: a comparative study with 13N-Ammonia PET myocardial blood flow quantitation[J]. Eur J Nucl Med Mol Imaging, 2017, 44(1): 117−128. DOI: 10.1007/s00259-016-3491-5. [13] Liu L, Abdu FA, Yin GQ, et al. Prognostic value of myocardial perfusion imaging with D-SPECT camera in patients with ischemia and no obstructive coronary artery disease (INOCA)[J]. J Nucl Cardiol, 2021, 28(6): 3025−3037. DOI: 10.1007/s12350-020-02252-8. [14] Li LL, Pang ZK, Wang J, et al. Prognostic value of myocardial flow reserve measured with CZT cardiac-dedicated SPECT low-dose dynamic myocardial perfusion imaging in patients with INOCA[J]. J Nucl Cardiol, 2023, 30(6): 2578−2592. DOI: 10.1007/s12350-023-03332-1. [15] Zhang H, Caobelli F, Che WL, et al. The prognostic value of CZT SPECT myocardial blood flow (MBF) quantification in patients with ischemia and no obstructive coronary artery disease (INOCA): a pilot study[J]. Eur J Nucl Med Mol Imaging, 2023, 50(7): 1940−1953. DOI: 10.1007/s00259-023-06125-3. [16] Wang J, Li S, Chen WQ, et al. Diagnostic efficiency of quantification of myocardial blood flow and coronary flow reserve with CZT dynamic SPECT imaging for patients with suspected coronary artery disease: a comparative study with traditional semi-quantitative evaluation[J]. Cardiovasc Diagn Ther, 2021, 11(1): 56−67. DOI: 10.21037/cdt-20-728. [17] Cerqueira MD, Weissman NJ, Dilsizian V, et al. Standardized myocardial segmentation and nomenclature for tomographic imaging of the heart. A statement for healthcare professionals from the Cardiac Imaging Committee of the Council on Clinical Cardiology of the American Heart Association[J]. Circulation, 2002, 105(4): 539−542. DOI: 10.1161/hc0402.102975. [18] Bourque JM. ISCHEMIA sheds light on INOCA: understanding population heterogeneity to inform prognosis and guide management[J]. JACC Cardiovasc Imaging, 2023, 16(1): 75−77. DOI: 10.1016/j.jcmg.2022.10.012. [19] Mohammed AA, Zhang HB, Abdu FA, et al. Effect of nonobstructive coronary stenosis on coronary microvascular dysfunction and long-term outcomes in patients with INOCA[J]. Clin Cardiol, 2023, 46(2): 204−213. DOI: 10.1002/clc.23962. [20] Iskander S, Iskandrian AE. Risk assessment using single-photon emission computed tomographic technetium-99m sestamibi imaging[J]. J Am Coll Cardiol, 1998, 32(1): 57−62. DOI: 10.1016/s0735-1097(98)00177-6. [21] Cho SG, Kim J, Song HC. Debates over NICE guideline update: what are the roles of nuclear cardiology in the initial evaluation of stable chest pain?[J]. Nucl Med Mol Imaging, 2019, 53(5): 301−312. DOI: 10.1007/s13139-019-00607-9. [22] Ziadi MC. Myocardial flow reserve (MFR) with positron emission tomography (PET)/computed tomography (CT): clinical impact in diagnosis and prognosis[J]. Cardiovasc Diagn Ther, 2017, 7(2): 206−218. DOI: 10.21037/cdt.2017.04.10. [23] Pang ZK, Wang J, Li S, et al. Diagnostic analysis of new quantitative parameters of low-dose dynamic myocardial perfusion imaging with CZT SPECT in the detection of suspected or known coronary artery disease[J]. Int J Cardiovasc Imaging, 2021, 37(1): 367−378. DOI: 10.1007/s10554-020-01962-x. [24] Panjer M, Dobrolinska M, Wagenaar NRL, et al. Diagnostic accuracy of dynamic CZT-SPECT in coronary artery disease. A systematic review and meta-analysis[J]. J Nucl Cardiol, 2022, 29(4): 1686−1697. DOI: 10.1007/s12350-021-02721-8. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 7394
- HTML全文浏览量: 5579
- PDF下载量: 17
