


 下载:
下载:
-
原发性甲状旁腺功能亢进症(primary hyperparathyroidism,PHPT) 是因甲状旁腺组织的原发病变引起甲状旁腺激素(parathyroid hormone,PTH)分泌过多,继而导致的一系列病变,包括高钙血症、肾钙质沉着症、肾结石、肾钙重吸收、尿磷排泄增加和以皮质骨为主的骨吸收增加等[1]。99Tcm-MIBI SPECT/CT双时相平面显像操作简单,是PHPT的常规影像检查方法[2]。但是,有研究结果显示,当病灶的质量<500 mg时,显像的假阴性率会升高[3]。王静等[4]的研究结果表明,当甲状旁腺质量较小时,其病灶的长径及体积也比较小,99Tcm-MIBI SPECT/CT双时相平面显像检测病灶的灵敏度也相对较低。本文中我们报道了1例初诊99Tcm-MIBI SPECT显像结果阴性、99Tcm-MIBI SPECT/CT跟踪显像结果阳性的不典型甲状旁腺小腺瘤患者,希望能在临床高度怀疑PHPT,但常规影像检查未发现病灶时,充分发挥99Tcm-MIBI SPECT/CT显像的诊断效能,为临床医师的诊断提供参考。
-
患者女性,51 岁,因“平地滑倒致右下肢疼痛、肿胀伴活动受限10 h”入院。行膝关节X线片检查:右胫骨上端骨折;右股骨下段内固定术术后表现;右膝关节明显骨质疏松。以“右胫骨平台骨折、右股骨干骨折术后”收入遵义医科大学附属医院骨科。本例患者3个月前也曾因平地摔倒致右股骨下段骨折于当地医院行手术治疗。47岁绝经。查体:被动卧位,右膝肿胀、压痛,活动受限,余无异常体征。辅助检查:PTH 205.80 pg/ml(正常参考值范围:18.50~88.00 pg/ml);血钙2.73 mmol/L(正常参考值范围:2.20~2.65 mmol/L);血磷0.78 mmol/L(正常参考值范围:0.81~1.45 mmol/L)。初步诊断:(1)右胫骨平台骨折;(2)右股骨干骨折内固定术后;(3)重度骨质疏松;(4)疑甲状旁腺功能亢进症。颈部彩超:未探及占位性病变。
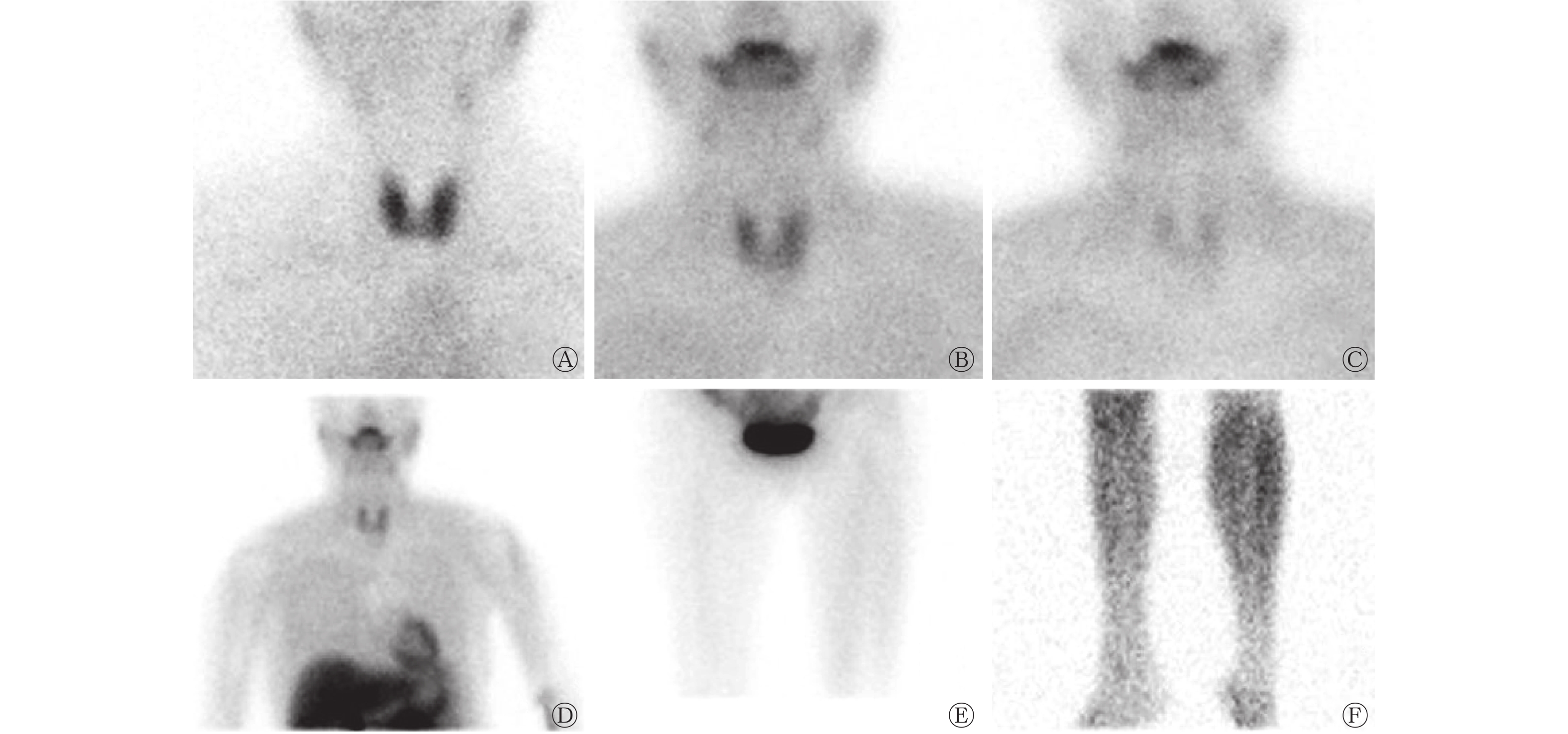
$ ^{{\rm{99}}}{\rm{T}}{{\rm{c}}^{\rm{m}}}{\rm{O}}_4^ - $ SPECT甲状腺显像(美国GE公司Infinia Hawkeye 4型SPECT/CT):双叶甲状腺未见明显异常(图1A)。99Tcm-MIBI SPECT双时相甲状旁腺显像(美国GE公司Infinia Hawkeye 4型SPECT/CT):甲状腺显影均匀消退,未见明显异常放射性浓聚(图1B、1C);大视野及全身扫描未见甲状腺床外明显异常放射性浓聚(图1D~1F)。相关检查未发现引起PTH水平升高的继发性原因。对本例患者予以降钙、水化及外固定等治疗,患者病情好转出院,嘱其定期复诊。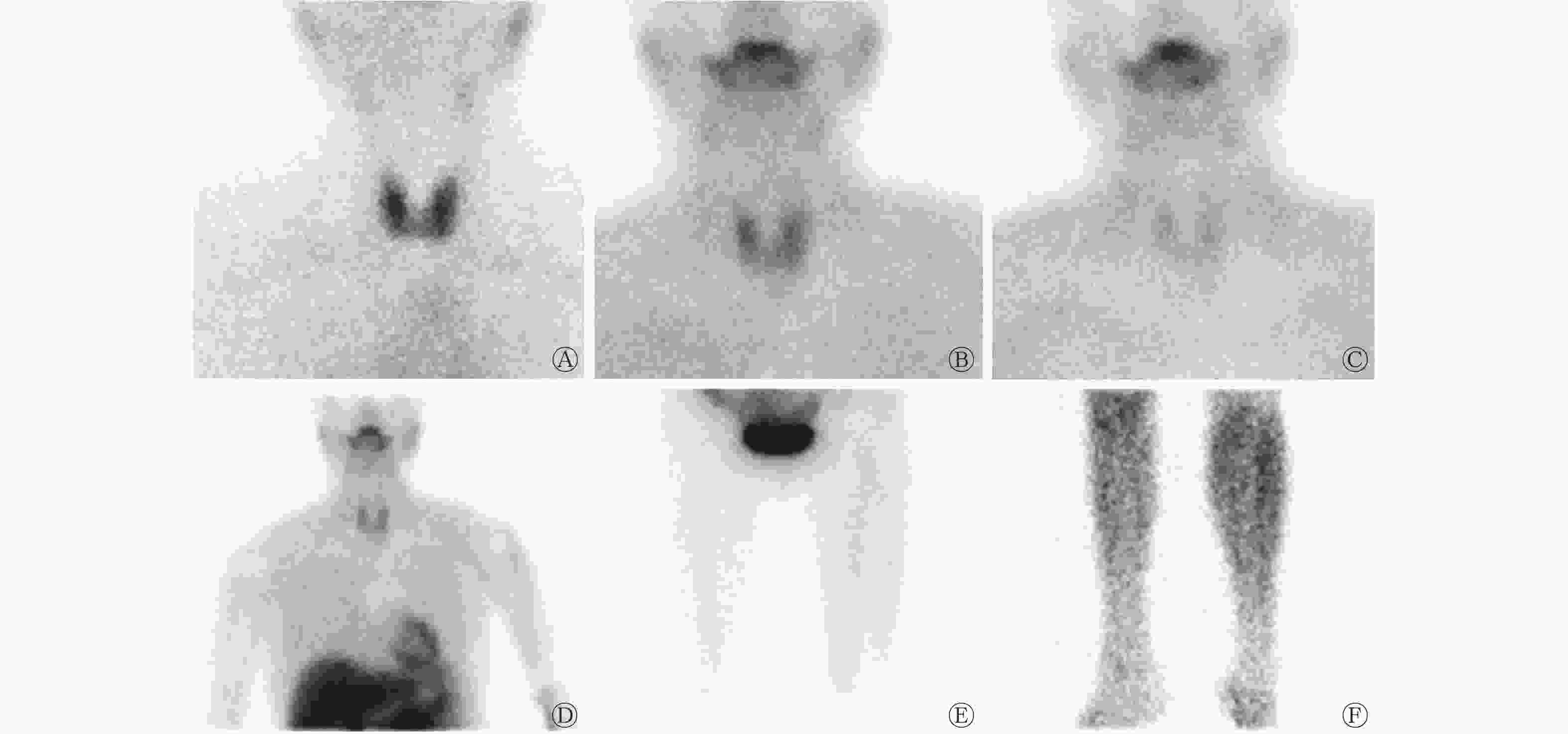
图 1 PHPT患者(女性,51岁)的SPECT静态平面显像图
Figure 1. Images of SPECT static planar imaging of a 51-year-old female primary hyperparathyroidism patient
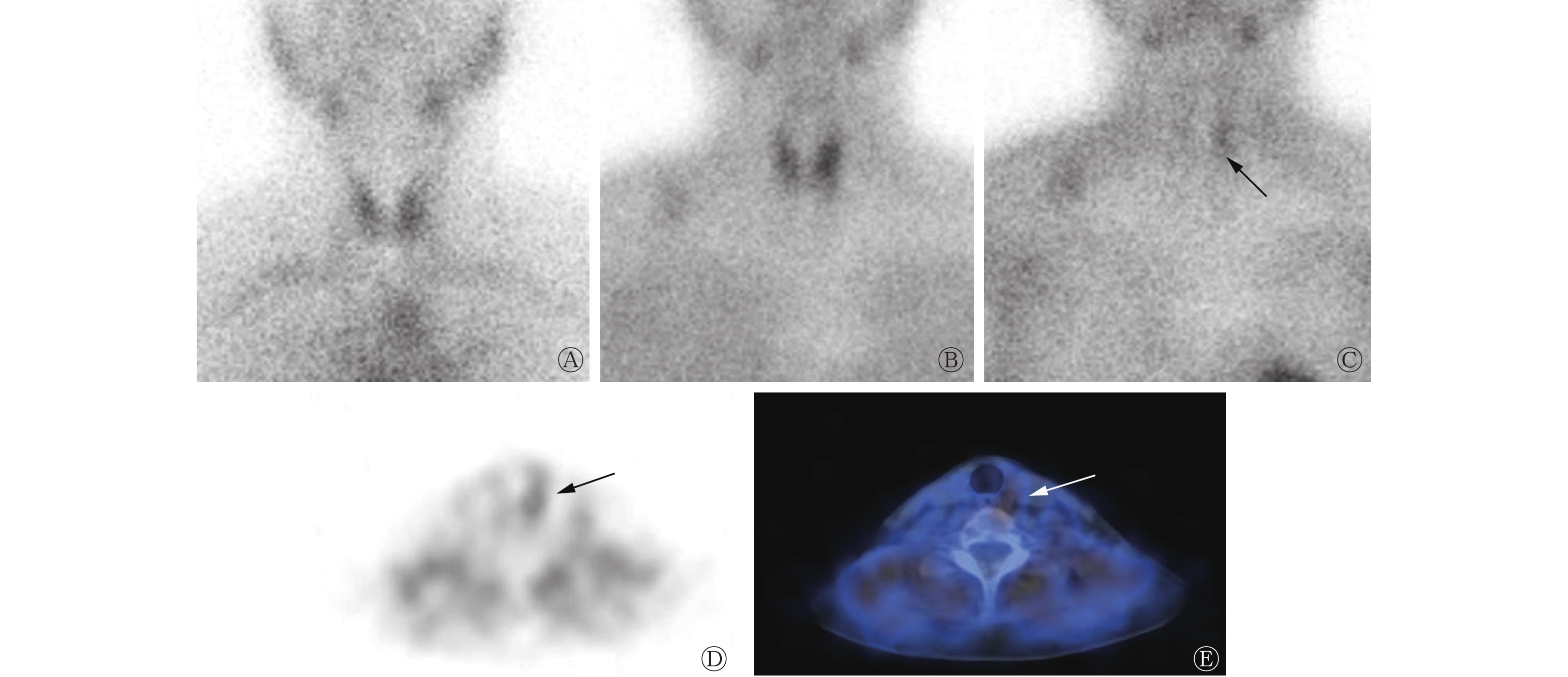
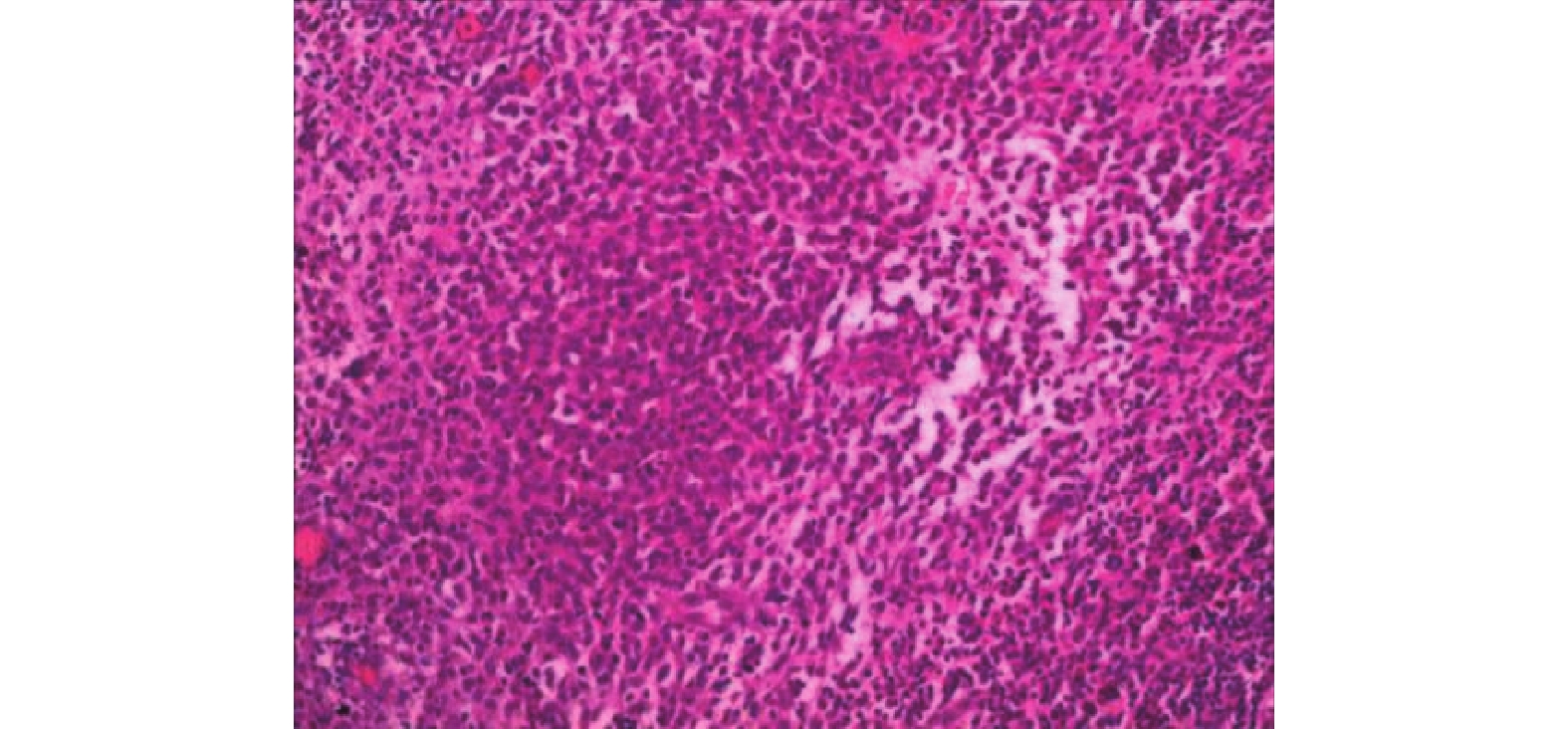
本例患者出院后每2个月复查颈部彩超,均未见异常,血钙和PTH水平均较前轻度升高,血磷水平无异常。出院半年后再次住院评估,结果如下。实验室检查:血钙2.81 mmol/L;血磷1.00 mmol/L;PTH 208.80 pg/ml。颈部彩超及CT检查均未见异常。99Tcm-MIBI SPECT/CT双时相甲状旁腺显像:左叶甲状腺床中下极部分放射性浓聚,结合临床资料考虑存在功能亢进的甲状旁腺组织显影可能性大(图2)。综合评估后行“左下甲状旁腺切除术+左侧喉返神经探查保护术”,术中术者借助SPECT/CT影像引导反复探查发现左下甲状旁腺可疑增生肥大,大小约1.1 cm×0.6 cm×0.3 cm,与周围组织轻度粘连,呈不规则状,予以完整切除后术中冰冻切片行组织病理学检查,结果提示:甲状旁腺良性病变。切除左下甲状旁腺20 min后,实验室检查:血清PTH 23.30 pg/ml;血钙2.48 mmol/L;血磷0.48 mmol/L。术后石蜡切片行组织病理学检查,结果显示:大体所见灰白组织一枚,长径 0.9 cm,质软,提示为甲状旁腺腺瘤(图3)。术后5 d复查:血钙2.13 mmol/L;血磷1.21 mmol/L;PTH 43.60 pg/ml。
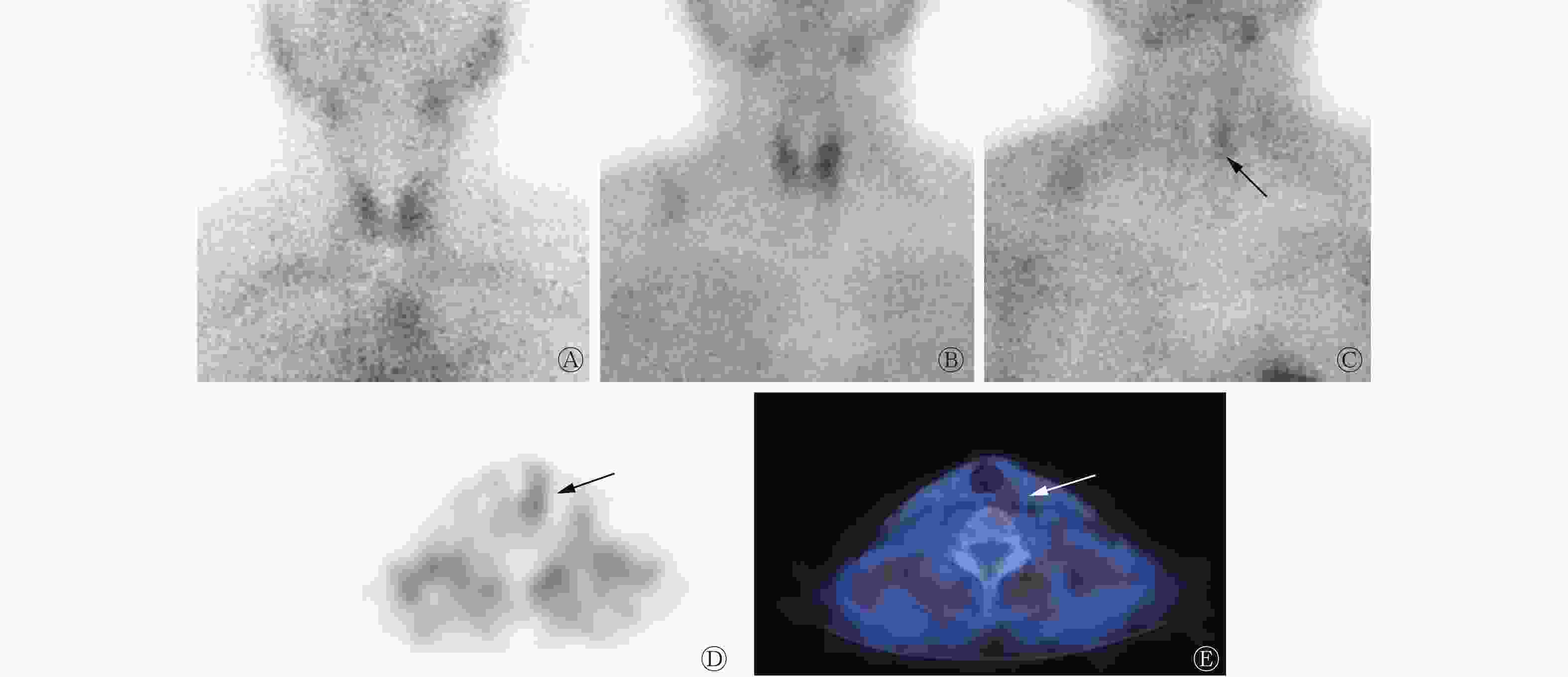
图 2 PHPT患者(女性,51岁)SPECT/CT静态平面显像及断层显像图(第1次显像半年后再次显像)
Figure 2. Images of SPECT/CT static plane imaging and tomography of a 51-year-old female primary hyperparathyroidism patient (re-imaging six months after the first imaging)
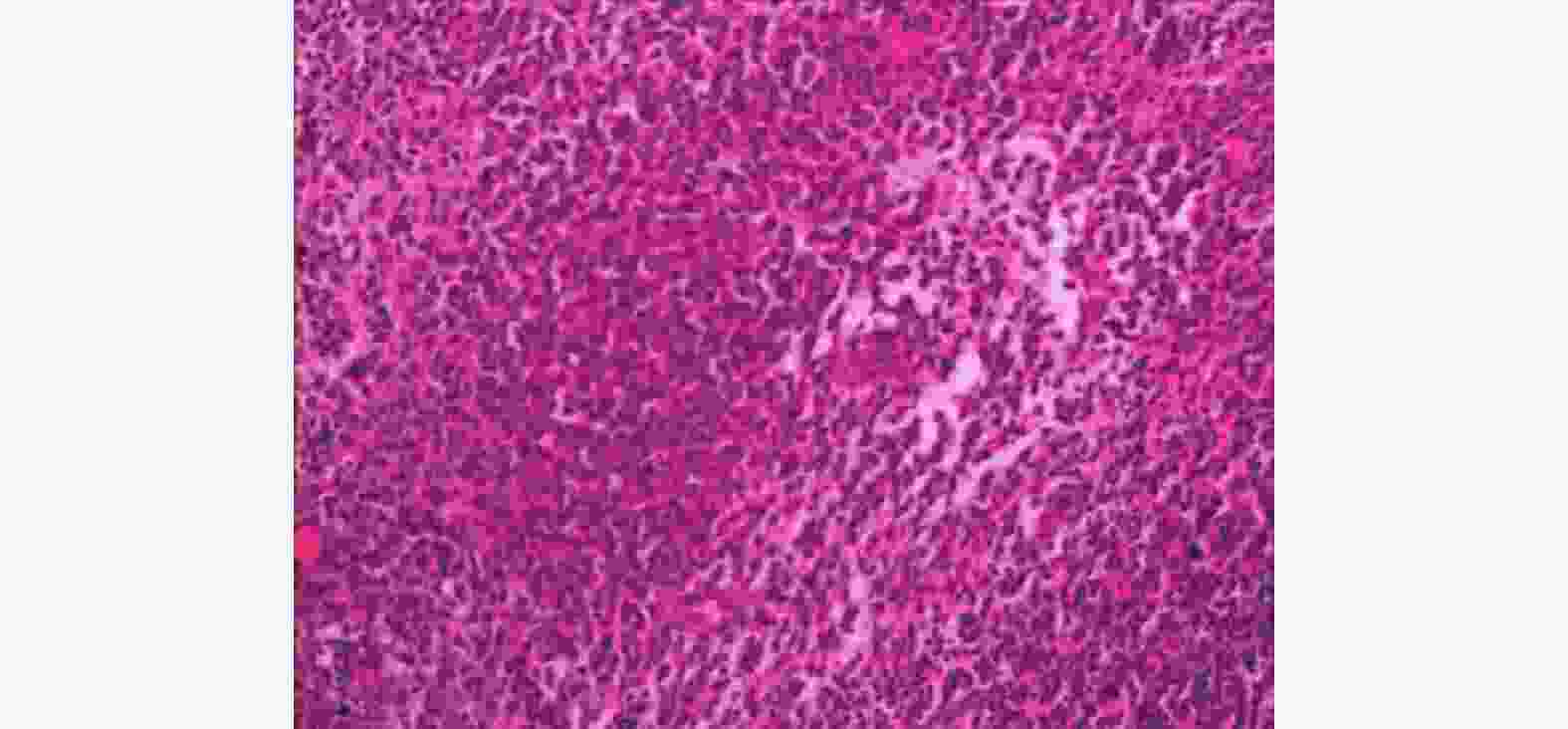
图 3 原发性甲状旁腺功能亢进症患者(女性,51岁)术后组织病理学检查图(苏木精-伊红染色,×100)
Figure 3. Postoperative histopathological examination image of a 51-year-old female primary hyperparathyroidism patient (hematoxylin eosin staining, ×100)
-
PHPT在欧美国家的发病率为0.2%~0.5%,其中,女性的发病率是男性的2~3 倍,而且这种差异随着年龄的增长而增加[5]。PHPT在组织病理学上以单发甲状旁腺腺瘤最多见,多发性腺瘤和甲状旁腺囊肿少见,且甲状旁腺癌也很少见。目前PHPT主要的治疗方法是通过外科手术切除功能亢进的甲状旁腺组织,而手术能否成功的关键是准确的术前定位诊断,术前显像和准确定位对于手术中的操作至关重要。目前定位甲状旁腺的方法有多种,包括超声检查、CT和MRI。与上述解剖学显像方法相比,99Tcm-MIBI SPECT/CT是一种功能性显像,被认为是PHPT患者主要的术前定位方法,该显像可以对病灶进行准确定位,提高手术的成功率、缩小术中探查范围,具有较高的灵敏度[6-7]。但是这也不是绝对的,Seki等[8]报道了1 例典型PHPT患者,在MRI、超声图像上均能发现长径为2 cm的1个病灶,但在99Tcm-MIBI SPECT/CT及18FDG PET上均未能检测到甲状旁腺肿瘤。目前,早期SPECT/CT显像仍然是PHPT患者术前常规评估的一部分[9]。甲状旁腺腺体分泌PTH,PTH水平在调节机体的钙稳态中起着主要作用。正常范围内的PTH水平可以调节细胞外钙浓度在正常的范围[10]。当怀疑存在异位甲状旁腺时,需加做胸部抬高位(包括颈部及上胸部)SPECT显像,若有必要还需行断层 SPECT/CT显像。如早期及延迟相均提示甲状腺、甲状腺旁的颈部或纵隔区见单个或多个异常放射性浓聚区,且浓聚区消退不明显,此则为典型的功能亢进的甲状旁腺组织显影图像[1]。
本例患者有明显的骨质疏松,且已绝经,除骨折外没有任何甲状旁腺功能亢进症的临床症状,易被认为是绝经后骨质疏松症。患者虽有血钙轻度增高、血磷轻度降低、血PTH轻度增高,但多种甲状旁腺影像检查结果均为阴性,此时虽然高度怀疑PHPT,却没有相应的影像证据支持,因此仅能通过监测血电解质及血PTH进行对症治疗。当常用的影像检查结果均为阴性时,可尝试行18F-氟代胆碱PET/CT检查,有相关研究结果显示该检查具有较高的灵敏度及特异度,是定位亢进的甲状旁腺腺瘤的一种准确、有效的显像方法[11]。但是该检查目前并未在临床中广泛应用。对于诊断困难的早期甲状旁腺腺瘤,有研究者报道可通过选择性PTH静脉采血,采集双侧颈部和胸部静脉血中的PTH进行分析,以定位甲状旁腺腺瘤,其相对于99Tcm-MIBI SPECT/CT显像等非侵入性显像方法具有更高的灵敏度,但该方法为有创性检查,且需要由具有丰富采样经验的介入医师进行操作[12]。以上2种检查方法虽然均比99Tcm-MIBI SPECT/CT显像具有更高的灵敏度,但是PET/CT显像费用昂贵,受到检查设备及显像剂的制约,目前开展该项检查的医院相对较少,局限性大;选择性PTH静脉采血为有创性检查,因甲状旁腺旁的静脉血管非常细,采血难度很大,对操作者的依赖性高,能够开展该项检查的医院也非常少。99Tcm-MIBI SPECT/CT显像虽然在灵敏度上不如以上2种检查,但其操作更简单、费用合理,大多数医院都能开展,对操作者的依赖性低,患者也更容易接受[13]。本例患者经彩超检查密切随访虽无阳性发现,但半年后行99Tcm-MIBI SPECT/CT显像结果为可疑阳性,核医学科医师通过综合判断并结合临床经验给予了临床医师可能的影像定位诊断参考。患者最终经手术、组织病理学检查及PTH监测证实为单个甲状旁腺小腺瘤。由此可见,99Tcm-MIBI SPECT/CT显像仍然具有不可替代的优势,我们用最简单、经济的方法帮助临床做出准确诊断,为患者获得了尽早手术治疗的机会。
手术是PHPT的唯一根治方法,对于那些有症状的患者和有进展风险的无症状患者,首选治疗方法是手术切除病灶。但对于本例患者来说,初诊多种影像检查不能准确定位诊断,仅能选择内分泌药物进行治疗,以增加骨密度或降低血钙水平[14]。文献报道99Tcm-MIBI SPECT/CT显像诊断PHPT的灵敏度为41.7%~94.0%[15]。有研究者认为99Tcm-MIBI SPECT/CT显像诊断及定位PHPT的影响因素较多,主要与甲状旁腺的功能亢进病灶的大小、分泌功能、血钙水平、甲状旁腺肿瘤细胞类型、甲状旁腺细胞的活性等有关[16-17]。本例患者2次99Tcm-MIBI SPECT/CT显像时检测的PTH水平相近,但是在初诊时99Tcm-MIBI SPECT显像结果为阴性,复查时(第2次99Tcm-MIBI SPECT/CT显像)发现了可疑病灶,其主要原因可能是由于初诊时甲状旁腺腺瘤较小,分泌功能还不够旺盛,故未明显摄取99Tcm-MIBI。
总之,当临床疑诊PHPT,而超声、CT等影像诊断结果为阴性时,可进行甲状旁腺99Tcm-MIBI SPECT/CT显像,且应将99Tcm-MIBI SPECT/CT显像作为PHPT定位诊断的首选方法,对于不具有典型临床特征的小腺瘤,可采用简便、易行、无创性的99Tcm-MIBI SPECT/CT显像技术动态监测,以期实现尽早诊断。
利益冲突 所有作者声明无利益冲突
作者贡献声明 蔡瑞负责数据的获取、论文的撰写;杨玲、李芳负责临床数据的收集、整理与分析;唐金艳、文瑞、王攀负责图片和数据的整理与核对;黄琦负责命题的设计、论文的修订
以反复骨折为主诉的不典型甲状旁腺腺瘤99Tcm-MIBI SPECT/CT跟踪显像1例
99Tcm-MIBI SPECT/CT tracking imaging of atypical parathyroid adenoma with recurrent fracture as the chief complaint: a case report
-
摘要: 笔者报道了1 例以反复骨折、高甲状旁腺激素水平、初诊99Tcm-甲氧基异丁基异腈(MIBI)SPECT显像结果阴性、99Tcm-MIBI SPECT/CT跟踪显像结果阳性为特点的不典型甲状旁腺腺瘤患者的影像及临床特征,结合相关文献进行回顾分析,探讨当CT、超声定位诊断结果均为阴性,甚至 99Tcm-MIBI SPECT/CT显像结果仍为阴性时的诊断思路,以期提高对不典型甲状旁腺腺瘤的认识及早期诊断水平,避免临床漏诊。Abstract: This paper reports the imaging and clinical features of a patient with an atypical parathyroid adenoma characterized by recurrent fractures, high parathyroid hormone level, negative 99Tcm-methoxyisobutylisonitrile (MIBI) SPECT imaging at initial diagnosis and positive 99Tcm-MIBI SPECT/CT tracking imaging at follow-up. By reviewing and analyzing relevant literature, this paper aims to explore the diagnostic approach when both CT and ultrasound localization diagnostic results are negative, and even when the 99Tcm-MIBI SPECT/CT imaging are still negative, in order to improve the understanding and early diagnosis of atypical parathyroid adenoma and avoid clinical missed diagnosis.
-
Key words:
-
图 1 PHPT患者(女性,51岁)的SPECT静态平面显像图
Figure 1. Images of SPECT static planar imaging of a 51-year-old female primary hyperparathyroidism patient
图 2 PHPT患者(女性,51岁)SPECT/CT静态平面显像及断层显像图(第1次显像半年后再次显像)
Figure 2. Images of SPECT/CT static plane imaging and tomography of a 51-year-old female primary hyperparathyroidism patient (re-imaging six months after the first imaging)
-
[1] 中华医学会骨质疏松和骨矿盐疾病分会, 中华医学会内分泌分会代谢性骨病学组. 原发性甲状旁腺功能亢进症诊疗指南[J]. 中华骨质疏松和骨矿盐疾病杂志, 2014, (3): 187−198. DOI: 10.3969/j.issn.1674-2591.2014.03.002.
Osteoporosis and Bone Mineral Salt Disease Branch, Chinese Medical Association, Metabolic Osteopathology Group, Endocrinology Society, Chinese Medical Association. Guidelines for diagnosis and treatment of primary hyperparathyroidism[J]. Chin J Osteoporosis Bone Miner Res, 2014, (3): 187−198. DOI: 10.3969/j.issn.1674-2591.2014.03.002.[2] Mandal R, Muthukrishnan A, Ferris RL, et al. Accuracy of early-phase versus dual-phase single-photon emission computed tomography/computed tomography in the localization of parathyroid disease[J]. Laryngoscope, 2015, 125(6): 1496−1501. DOI: 10.1002/lary.25020. [3] 张长明, 马欢, 张玉芳. 99Tcm-MIBI断层及同机CT融合显像在继发性甲状旁腺功能亢进症术前定位诊断中的价值[J]. 中华内分泌外科杂志, 2016, 10(1): 23−25. DOI: 10.3760/cma.j.issn.1674-6090.2016.01.006.
Zhang CM, Ma H, Zhang YF. Value of 99Tcm-MIBI tomography and registration with integrated CT in preoperative localization and diagnosis of secondary hyperparathyroidism[J]. Chin J Endocr Surg, 2016, 10(1): 23−25. DOI: 10.3760/cma.j.issn.1674-6090.2016.01.006.[4] 王静, 朱玉春, 蔡国强, 等. 甲状旁腺病灶重量对99Tcm-MIBI显像诊断灵敏度的影响[J]. 国际放射医学核医学杂志, 2020, 44(6): 352−358. DOI: 10.3760/cma.j.cn121381-201903012-00037.
Wang J, Zhu YC, Cai GQ, et al. The influence of parathyroid lesion weight on diagnostic sensitivity of 99Tcm-MIBI imaging[J]. Int J Radiat Med Nucl Med, 2020, 44(6): 352−358. DOI: 10.3760/cma.j.cn121381-201903012-00037.[5] Al Zahrani A, Levine MA. Primary hyperparathyroidism[J]. Lancet, 1997, 349(9060): 1233−1238. DOI: 10.1016/s0140-6736(96)06176-4. [6] Lavely WC, Goetze S, Friedman KP, et al. Comparison of SPECT/CT, SPECT, and planar imaging with single- and dual-phase 99mTc-sestamibi parathyroid scintigraphy[J]. J Nucl Med, 2007, 48(7): 1084−1089. DOI: 10.2967/jnumed.107.040428. [7] 钟箫, 欧晓红, 李林, 等. 99Tcm-MIBI SPECT/CT融合显像在甲状旁腺功能亢进症术前诊断中的应用价值[J]. 中华核医学与分子影像杂志, 2017, 37(7): 395−399. DOI: 10.3760/cma.j.issn.2095-2848.2017.07.004.
Zhong X, Ou XH, Li L, et al. Value of 99Tcm-MIBI SPECT/CT in pre-operative diagnosis of primary and secondary hyperparathyroidism[J]. Chin J Nucl Med Mol Imaging, 2017, 37(7): 395−399. DOI: 10.3760/cma.j.issn.2095-2848.2017.07.004.[8] Seki K, Hashimoto K, Hisada T, et al. A patient with classic severe primary hyperparathyroidism in whom both Tc-99m MIBI scintigraphy and FDG-PET failed to detect the parathyroid tumor[J]. Intern Med, 2004, 43(9): 816−823. DOI: 10.2169/internalmedicine.43.816. [9] Zhang RQ, Zhang ZW, Huang PB, et al. Diagnostic performance of ultrasonography, dual-phase 99mTc-MIBI scintigraphy, early and delayed 99mTc-MIBI SPECT/CT in preoperative parathyroid gland localization in secondary hyperparathyroidism[J/OL]. BMC Med Imaging, 2020, 20(1): 91[2022-02-08]. https://bmcmedimaging.biomedcentral.com/articles/10.1186/s12880-020-00490-3. DOI: 10.1186/s12880-020-00490-3. [10] Taniegra ED. Hyperparathyroidism[J]. Am Fam Physician, 2004, 69(2): 333−339. [11] Lezaic L, Rep S, Sever MJ, et al. 18F-Fluorocholine PET/CT for localization of hyperfunctioning parathyroid tissue in primary hyperparathyroidism: a pilot study[J]. Eur J Nucl Med Mol Imaging, 2014, 41(11): 2083−2089. DOI: 10.1007/s00259-014-2837-0. [12] Sun PY, Thompson SM, Andrews JC, et al. Selective parathyroid hormone venous sampling in patients with persistent or recurrent primary hyperparathyroidism and negative, equivocal or discordant noninvasive imaging[J]. World J Surg, 2016, 40(12): 2956−2963. DOI: 10.1007/s00268-016-3621-z. [13] 段晓晔, 马婉璐, 朱庆莉, 等. 骨痛、高甲状旁腺素血症、99mTc MIBI甲状旁腺显像阴性[J]. 中华骨质疏松和骨矿盐疾病杂志, 2019, 12(2): 172−176. DOI: 10.3969/j.issn.1674-2591.2019.02.011.
Duan XY, Ma WL, Zhu QL, et al. Bone pain, high serum parathyroid hormone, negative 99mTc-sestamibi scanning: a case report[J]. Chin J Osteoporosis Bone Miner Res, 2019, 12(2): 172−176. DOI: 10.3969/j.issn.1674-2591.2019.02.011.[14] Walker MD, Silverberg SJ. Primary hyperparathyroidism[J]. Nat Rev Endocrinol, 2018, 14(2): 115−125. DOI: 10.1038/nrendo.2017.104. [15] Levy JM, Kandil E, Yau LC, et al. Can ultrasound be used as the primary screening modality for the localization of parathyroid disease prior to surgery for primary hyperparathyroidism? A review of 440 cases[J]. ORL J Otorhinolaryngol Relat Spec, 2011, 73(2): 116−120. DOI: 10.1159/000323912. [16] 王军, 张宏, 安宁, 等. 99mTc-MIBI核素显像误诊为甲状旁腺腺瘤1例[J]. 中国医学文摘耳鼻咽喉科学, 2016, 31(6): 325−327. DOI: 10.19617/j.issn1001-1307.2016.06.011.
Wang J, Zhang H, An N, et al. 99mTc-MIBI radionuclide imaging misdiagnosed as parathyroid adenoma: a case report[J]. Chin Med Dig: Otorhinolaryngol, 2016, 31(6): 325−327. DOI: 10.19617/j.issn1001-1307.2016.06.011.[17] 崔梦钊, 刚晓坤, 陈光, 等. 99Tcm-MIBI SPECT/CT扫描阴性的甲状旁腺癌一例[J]. 中华医学杂志, 2017, 97(40): 3187−3188. DOI: 10.3760/cma.j.issn.0376-2491.2017.40.015.
Cui MZ, Gang XK, Chen G, et al. A case of parathyroid carcinoma with 99Tcm-MIBI SPECT/CT scan negative[J]. Natl Med J China, 2017, 97(40): 3187−3188. DOI: 10.3760/cma.j.issn.0376-2491.2017.40.015. -

 点击查看大图
点击查看大图
图(3)
计量
- 文章访问数: 3839
- HTML全文浏览量: 3056
- PDF下载量: 12
