



-
放射性核素平衡法门控心血池显像能够无创性反映左右心室功能参数,对冠心病的心功能评价、异常心电传导和心肌病的辅助诊断等均具有重要价值。该显像方法受人为干扰小、测量方法稳定性好、准确性高。除了心脏疾病,其在肿瘤患者化疗及靶向治疗可能导致的心脏毒性和不良反应引起的心室功能损伤的定期监测中具有重要的临床应用价值[1-2]。此外,该显像方法在左右心室机械收缩同步性评估中的价值也一直受到临床重视[3-4]。NaI-SPECT平衡法门控心血池平面显像(简称NaI-SPECT平面显像)最为经典,但受到房室重叠、本底勾画和低探测计数的制约,其测定心室功能的准确性受到影响[5]。SPECT断层技术在一定程度上克服了这些问题,而且在左心室射血分数(left ventricular ejection fraction, LVEF)及容积测量上与心脏磁共振的一致性和相关性较好[6-7],也成为有金属植入物患者(存在心脏磁共振禁忌)准确评估左、右心室情况的首选替代检查方法[8]。但NaI-SPECT平面显像存在时间和空间分辨率低、探测器放射性计数敏感性低和采集时间长等局限性。
近年来,随着技术的进步和设备的更迭,配置固体常温半导体材料碲锌镉(cadmium zinc telluride,CZT)探测器的SPECT(即CZT-SPECT)被发明和应用,从而实现了上述NaI-SPECT性能的极大提高[9]。高门控帧数、高灵敏度将极大提高心血池断层显像的采集信息量[10-11],并且CZT-SPECT实现了表模式(list model)采集,后期可以对全部采集数据进行任意时间段的截取和重组,实现多种重建模式,如获得多种采集时间、门控帧数和成像角度的重建图像[12]。现有的对其诊断效能及采集方案优化的研究均表明这项新兴技术具有很大的潜在临床价值[13-14],但总体而言,有关CZT-SPECT平衡法门控心血池断层显像(简称CZT-SPECT断层显像)技术方面的研究相对较少,国内尚无相关研究报道。本研究旨在通过对比分析传统NaI-SPECT平面显像与心脏专用CZT-SPECT断层显像及其重建平面显像(简称CZT-SPECT断层重建平面显像)所获得的左、右心室功能参数的相关性及其差异,进行心脏专用CZT-SPECT断层显像测定双心室功能的方法学研究并探讨其优势。
-
回顾性分析2021年8月至2022年11月在泰达国际心血管病医院行放射性核素平衡法门控心血池显像的患者58例,其中,男性38例、女性20例,年龄(60.6±12.3)岁。纳入标准:年龄为18~90岁,同日先后行NaI-SPECT平面显像和CZT-SPECT断层显像。排除标准:因极度心律不齐无法完成门控采集者;未能于同日完成平面和断层显像者。本研究获得泰达国际心血管病医院伦理委员会批准(批准号:2022-0429-4)。因本研究为回顾性临床研究,豁免签署患者知情同意书。
-
注射显像剂为99Tcm标记自体红细胞,采用体内标记法。取亚锡焦磷酸钠(北京欣科思达医药科技有限公司)10 mg,用2 ml生理盐水溶解,摇匀后用注射器抽出并于患者静脉注射。嘱患者休息30 min后再静脉注射1 ml 740~925 MBq 99TcmO4 −(原子高科股份有限公司),10~15 min后开始显像。患者先仰卧于NaI-SPECT(美国GE公司Discovery NM630型)检查床,双手上举,胸部连接心电采集电极。将心脏置于探头中央视野内,将探头调至左前斜位45°,然后微调至使左右心室能分隔清晰的左前斜位角度,遂启动采集。采集条件:准直器为低能高分辨平行孔型准直器,矩阵为64×64,射线能窗为±15%,能峰为140 keV,心电R-R间期被分成32等份,心率窗为±15%;采集时间为15 min或600万计数。采集完成后,患者换至CZT-SPECT(美国GE公司Discovery NM530c型)检查床,体位同前,胸部连接心电采集电极。自动定位心血池影后,将采集焦点设于左心腔几何中心后自动调整采集位置。采集条件:19个固定角度针孔型准直器,矩阵为64×64,能窗、能峰同前,表模式采集时间为10 min。2次检查之间除了患者需要更换检查设备时的上下检查床时间,无其他等候时间。
-
采集完毕后,数据均传输至Xeleris 4 DR工作站(美国GE公司)进行处理。由1名经验丰富的核医学医师分别对2种设备上的采集数据进行回顾性分析,再对结果进行盲法分析。心室功能参数[LVEF和右心室射血分数(right ventricular ejection fraction,RVEF)]的表示方法:NaI-SPECT平面显像用LVEF(P)和RVEF(P)表示,CZT-SPECT断层显像用LVEF(T)和RVEF(T)表示,CZT-SPECT断层重建平面显像用LVEF(re)和RVEF(re)表示。用Alcyone to Multigated Views软件包对CZT-SPECT数据进行左前斜位平面重建(选择能清晰分隔左右心室的角度),NaI-SPECT平面显像数据和CZT-SPECT断层重建平面显像数据用EF analysis软件包分析;用Lister工具对CZT-SPECT的10 min表模式采集数据(即原始数据)重建出采集时间为3、4和5 min的数据[即LVEF(3 min)、LVEF(4 min)、LVEF(5 min)和RVEF(3 min)、RVEF(4 min)、RVEF(5 min)],再由Cedars-Sinai G-BPGs软件包处理。将LVEF(10 min)和RVEF(10 min)按≥20%、≥30%、≥40%和≥50%重新分为各亚组,并与上述重建数据分别进行分析。
-
采用SPSS 26.0软件进行统计学分析。符合正态分布的计量资料以
$\bar x\pm s $ 表示,采用配对t检验和Pearson相关性分析;非正态分布的计量资料以M(Q1,Q3)表示,采用Wilcoxon符号秩检验和Spearman相关性分析。相关性(r值)评价:0.8≤r≤1.0为优秀;0.6≤r<0.8为较好;0.4≤r<0.6为一般;0.2≤r<0.4为较差;<0.2为无相关。P<0.05为差异有统计学意义。 -
本研究共纳入患者58例,患者的一般资料见表1。所有患者均有心脏相关疾病,包含表1中的1种或多种。
一般资料 例(%)或 $ \bar x\pm s $ 

年龄(岁) 60.6±12.3 男性 38(65.5) 女性 20(34.5) 身高(cm) 167.3±8.5 体重(kg) 72.1±15.0 显像剂注射剂量(MBq) 802.9±66.6 LVEF(P)(%) 31.00(22.00,41.00) RVEF(P)(%) 39.78±12.16 危险因素 高血压 33(56.9) 高血脂 1(1.7) 糖尿病 8(13.8) 吸烟 26(44.8) 饮酒 22(37.9) 临床诊断 冠心病 20(34.5) 扩张型心肌病 19(32.8) 心力衰竭 20(34.5) 完全性左束支传导阻滞 20(34.5) 其他类型心律失常 10(17.2) 其他心脏疾病(瓣膜病、风湿性
心脏病、酒精性心肌病等)7(12.1) 注:LVEF(P)为NaI-SPECT平面显像获得的左心室射血分数;RVEF(P)为NaI-SPECT平面显像获得的右心室射血分数 表 1 纳入的58例行放射性核素平衡法门控心血池显像的 患者的一般资料
Table 1. General data on the 58 included patients of gated equilibrium radionuclide cardio angiography
-
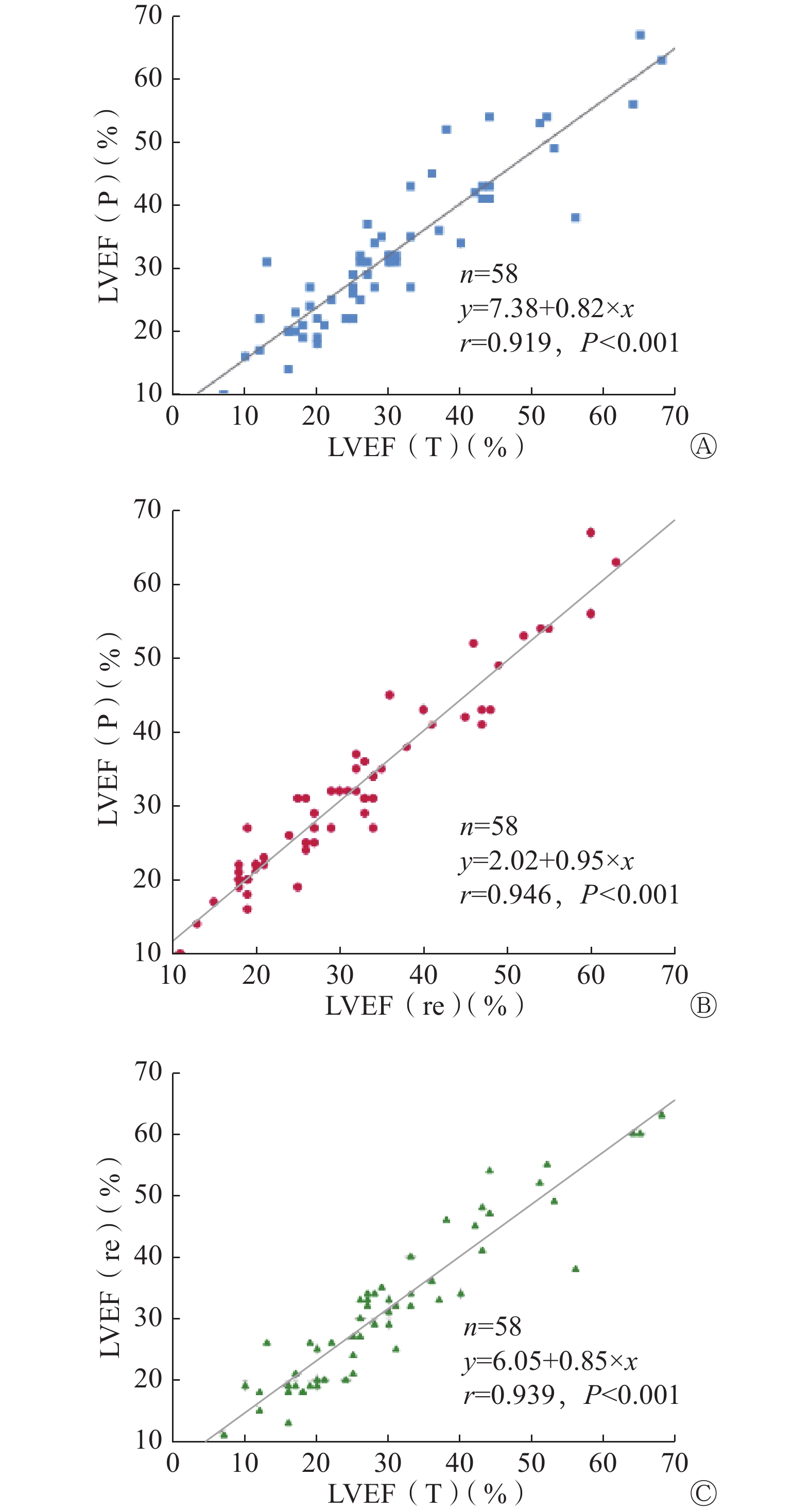
LVEF(P)、LVEF(T)和LVEF(re)分别为31.00%(22.00%,41.00%)、27.00%(19.75%,38.50%)和30.50%(20.00%,38.50%)。LVEF(re)、LVEF(P)与LVEF(T)之间的差异均有统计学意义(Z=−2.645、−3.065,均P<0.05),LVEF(re)与LVEF(P)之间的差异无统计学意义(Z=−1.057,P>0.05);三者间比较,两两之间的相关性均为优秀,相对而言,LVEF(re)与LVEF(P)之间的相关性(r=0.946,P<0.001)稍优于LVEF(T)与LVEF(P)(r=0.919,P<0.001),见图1。

图 1 3种显像方法获得的LVEF之间的相关性散点图
Figure 1. Scatter plots of the correlation between the left ventricular ejection fraction obtained by the 3 imaging methods
-
RVEF(P)、RVEF(T)和RVEF(re)分别为39.78%±12.16%、41.57%±15.18%和40.88%±13.19%。RVEF(P)、RVEF(T)和RVEF(re)两两之间的差异均无统计学意义(t=−1.949、−1.721、0.883,均P>0.05);三者间比较,两两之间的相关性均为优秀,相对而言,RVEF(re)与RVEF(P)之间相关性(r=0.929,P<0.001)优于RVEF(T)与RVEF(P)(r=0.892,P<0.001),见图2。

图 2 3种显像方法获得的RVEF之间的相关性散点图
Figure 2. Scatter plots of the correlation between the right ventricular ejection fraction obtained by the 3 imaging methods
-
LVEF(5 min)、LVEF(4 min)、LVEF(3 min)分别为27.50%(21.00%,39.25%)、28.50%(21.75%,40.00%)和29.50%(23.00%,42.00%),与LVEF(10 min)[27.00%(19.75%,38.50%)]相比,差异均有统计学意义(Z=−2.798、−3.288、−3.995,均P<0.05),且相关性均为优秀(r=0.970、0.938、0.903,均P<0.001)。随着重建时间的缩短,LVEF呈稍升高趋势。
RVEF(5 min)、RVEF(4 min)、RVEF(3 min)分别为42.90%±14.68%、44.55%±16.01%、45.48%±15.24%,与RVEF(10 min)(41.57%±15.18%)之间的差异均有统计学意义(t=−2.187、−3.976、−5.154,均P<0.05),且相关性均为优秀(r=0.953、0.934、0.928,均P<0.001)。随着重建时间的缩短,RVEF呈稍升高趋势。
亚组分析结果显示,除LVEF(10 min)≥20%亚组,其余亚组中LVEF(5 min)与LVEF(10 min)之间的差异均无统计学意义(均P>0.05);LVEF(10 min)≥50%亚组中LVEF(3 min)与LVEF(10 min)之间的差异无统计学意义(P>0.05);在LVEF(10 min)各亚组中,LVEF(4 min)与LVEF(10 min)之间的差异均有统计学意义(均P<0.05)。在RVEF(10 min)各亚组中,RVEF(5 min)与RVEF(10 min)之间的差异均无统计学意义(均P>0.05),而RVEF(4 min)和RVEF(3 min)与RVEF(10 min)之间的差异均有统计学意义(均P<0.05)。见表2、表3。
重建不同采集时间获得的LVEF LVEF(10 min)≥20% LVEF(10 min)≥30% LVEF(10 min)≥40% LVEF(10 min)≥50% (n=44) (n=25) (n=14) (n=7) 检验值 P值 检验值 P值 检验值 P值 检验值 P值 LVEF(3 min) −3.043a 0.002 −2.529a 0.011 −2.456a 0.014 −2.287b 0.062 LVEF(4 min) −2.837a 0.005 −2.513a 0.012 −2.203a 0.028 −2.976b 0.025 LVEF(5 min) 2.837a 0.004 −1.597a 0.110 −1.429a 0.153 −1.804b 0.121 注:CZT为碲锌镉;SPECT为单光子发射计算机体层摄影术;LVEF(3 min)、LVEF(4 min)、LVEF(5 min)分别为由原始数据重建采集时间为3、4、5 min的数据获得的左心室射血分数;LVEF(10 min)为采集时间为10 min的原始数据获得的左心室射血分数;a表示Z值;b表示t值 表 2 CZT-SPECT断层显像患者重建不同采集时间获得的LVEF与原始数据获得的LVEF的各亚组之间的比较
Table 2. Comparison between subgroups of left ventricular ejection fraction obtained at different acquisition times and left ventricular ejection fraction obtained from raw data in patients with CZT-SPECT reconstruction
重建不同采集时间获得的RVEF RVEF(10 min)≥20% RVEF(10 min)≥30% RVEF(10 min)≥40% RVEF(10 min)≥50% (n=56) (n=44) (n=31) (n=16) 检验值 P值 检验值 P值 检验值 P值 检验值 P值 RVEF(3 min) −4.229a <0.001 −3.956a <0.001 −3.659a <0.001 −3.381b 0.004 RVEF(4 min) −3.760a <0.001 −3.327a 0.001 −3.724a <0.001 −4.015b 0.001 RVEF(5 min) −1.853a 0.064 −1.339a 0.180 −1.158a 0.247 −0.132b 0.897 注:CZT为碲锌镉;SPECT为单光子发射计算机体层摄影术;RVEF(3 min)、RVEF(4 min)、RVEF(5 min)分别为由原始数据重建采集时间为3、4、5 min的数据获得的右心室射血分数;RVEF(10 min)为采集时间为10 min的原始数据获得的右心室射血分数;a表示Z值;b表示t值 表 3 CZT-SPECT断层显像患者重建不同采集时间获得的RVEF与原始数据获得的RVEF的各亚组之间的比较
Table 3. Comparison between subgroups of right ventricular ejection fraction obtained at different acquisition times and right ventricular ejection fraction obtained from raw data in patients with CZT-SPECT reconstruction
-
CZT-SPECT由于设备性能较NaI-SPECT有明显的提升,在探测灵敏度、空间分辨率、图像质量和显像时间等方面具有明显的提升和改善,而且只需一次心电门控表模式采集,后期便可通过工作站进行采集时间、采集角度和门控帧数等方面的任意组合重建。本研究结果表明:对于平衡法门控心血池显像,NaI-SPECT平面显像、CZT-SPECT断层显像及其重建平面显像所测得的双心室功能参数(LVEF和RVEF)均具有优秀的相关性,这与国外研究结果基本一致[15-17]。在本研究大多数样本数据中,我们发现CZT-SPECT断层重建平面显像所测得的LVEF和RVEF通常介于NaI-SPECT平面显像和CZT-SPECT断层显像之间,但更接近于NaI-SPECT平面显像,类似于一组“中间缓冲”数据。因此,我们认为,CZT-SPECT可以通过断层显像重建出较为可靠的平面显像数据。在特定原因(如心室过大、重构明显或室壁运动极不协调等)导致断层显像勾画双心室可能不准确的情况下,我们通过重建获得更容易勾画靶区的平面数据,二者可以同时进行分析,以便相互参考和佐证。另外,从图像质量方面来看,由于设备的分辨率和探测效率明显提高,CZT-SPECT断层重建平面图像明显优于NaI-SPECT,而且由于可以同时自由选择最优左右心室分隔的投影角度,因此极大改善了图像处理与分析过程,进一步减少了测量的误差。
本研究还进一步探讨了CZT-SPECT断层显像重建不同采集时间数据处理结果之间的差异。参考国外既往研究[10-11, 16-17]中得出的采集时间缩短过少对于临床应用意义并不大的结论,我们直接将原始采集时间缩短一半(即5 min)进行分析,结果表明,尽管由3、4和5 min的采集时间获得的LVEF和RVEF均与采集10 min的结果具有优秀的相关性,但差异仍有统计学意义。究其原因,我们认为这可能与样本对象的选择有关。国外既往研究中的心脏相关疾病患者较少,而肿瘤化疗导致心脏毒性进行监测的患者占大部分,其中心功能正常者居多,而我们的样本对象全部是心脏相关疾病患者,疾病种类较多且复杂,多伴有心力衰竭,患者的LVEF和RVEF平均水平都相对较低。因此,我们进行了进一步的根据LVEF程度逐级减少来分组的亚组分析,结果表明在LVEF≥50%亚组中,LVEF(3 min)与LVEF(10 min)之间的差异无统计学意义,但由于样本数较少,尚需进一步扩大样本量来研究。结合本研究中LVEF和RVEF的亚组分析结果,我们认为采集时间设定为3 min和4 min 不适合于心脏相关疾病患者的CZT-SPECT断层显像;在LVEF≥30%和RVEF≥20%亚组中,采集时间设定为5 min的方案是适合临床应用的,反之则可能需要在采集前进行预估或采用采集时间>5 min的方案。这一结果表明,CZT-SPECT断层显像在大多数患者群体中可以在常规剂量下有效将心血池显像的采集时间缩短66.7%(CZT-SPECT断层显像的5 min与NaI-SPECT平面显像的15 min的比较)。同理,如果按照常规采集时间,CZT-SPECT断层显像可以采用半剂量注射,这样可以同时缩短一定的采集时间(CZT-SPECT断层显像的10 min与NaI-SPECT平面显像的15 min的比较)和降低辐射剂量。既往研究结果表明,CZT-SPECT断层显像的优化采集方案可将辐射剂量降低至1.80~1.92 mSv[10-11]。
本研究的局限性在于样本量相对少,未能获得不同心脏疾病足够大的样本量进行进一步分析,且受实际临床情况的限制,未能获得心室造影或CMR作为“金标准”来进行对比。
综上所述,CZT-SPECT断层显像一次表模式采集能够获得断层和优选分隔左右心室角度的重建平面2组数据,在常规剂量下,采集时间设定为5 min及>5 min的采集方案能获得可靠的数据用于后期处理,优化采集方案既能提高采集效率和降低辐射剂量,又能保证测量双心室功能参数的准确性。
利益冲突 所有作者声明无利益冲突
作者贡献声明 陈越负责研究方案的设计、数据的处理与统计分析、论文的撰写;杨学文负责设备的维护、硬件的调试、图像采集的协助;梁钰、赵迪、卢如明、王小杰负责设备参数的调节、图像的采集、数据的整理与保存;李剑明负责研究方案的完善与确定、研究过程的总体监督、论文的审阅与修订
碲锌镉SPECT平衡法门控心血池断层显像重建平面及快速显像方案的研究
Study of tomographic gated equilibrium radionuclide angiography on reconstructed-planar imaging and rapid acquisition mode with cadmium zinc telluride SPECT
-
摘要:
目的 通过对比分析传统NaI-SPECT平衡法门控心血池平面显像(简称NaI-SPECT平面显像)与心脏专用碲锌镉(CZT)SPECT(CZT-SPECT)平衡法门控心血池断层显像(简称CZT-SPECT断层显像)及其重建平面显像(简称CZT-SPECT断层重建平面显像)所获得的左、右心室功能参数的相关性及其差异,进行CZT-SPECT断层显像的方法学研究并探讨其优势。 方法 回顾性分析2021年8月至2022年11月在泰达国际心血管病医院行放射性核素平衡法门控心血池显像的患者58例[其中,男性38例、女性20例,年龄(60.6±12.3)岁],所有患者均于同日先后行NaI-SPECT平面显像和CZT-SPECT断层显像,重建CZT-SPECT断层显像数据成平面显像数据,比较和分析NaI-SPECT平面显像(P)、CZT-SPECT断层显像(T)及其重建平面显像(re)获得的左心室射血分数(LVEF)和右心室射血分数(RVEF)。重建3、4和5 min的CZT-SPECT断层显像采集数据,将获得的LVEF(3 min)、LVEF(4 min)、LVEF(5 min)和RVEF(3 min)、RVEF(4 min)、RVEF(5 min)与原始采集数据LVEF(10 min)、RVEF(10 min)进行比较。将LVEF(10 min)和RVEF(10 min)按≥20%、≥30%、≥40%和≥50%重新分为各亚组,并与上述重建数据分别进行分析。计量资料的比较采用配对t检验(或Wilcoxon符号秩检验),相关性采用Pearson(或Spearman)相关性分析。 结果 LVEF(re)[30.50%(20.00%,38.50%)]、LVEF(P)[31.00%(22.00%,41.00%)]与LVEF(T)[27.00%(19.75%,38.50%)]之间的差异均有统计学意义(Z=−2.645、−3.065,均P<0.05),LVEF(re)与LVEF(P)之间的差异无统计学意义(Z=−1.057,P>0.05);RVEF(P)(39.78%±12.16%)、RVEF(T)(41.57%±15.18%)和RVEF(re)(40.88%±13.19%)之间两两比较,差异均无统计学意义(t=−1.949、−1.721、0.883,均P>0.05);3种显像方法获得的LVEF、RVEF比较,两两之间的相关性均为优秀(r=0.892~0.946,均P<0.001);LVEF(3 min)、LVEF(4 min)、LVEF(5 min)和RVEF(3 min)、RVEF(4 min)、RVEF(5 min)分别与LVEF(10 min)和RVEF(10 min)比较,差异均有统计学意义(Z=−2.798、−3.288、−3.995,t=−2.187、−3.976、−5.154,均P<0.05),且相关性均为优秀(r=0.903~0.970,均P<0.001)。亚组分析结果显示,除LVEF≥20%亚组外,其余各亚组中,LVEF(5 min)与LVEF(10 min)、RVEF(5 min)与RVEF(10 min)之间的差异均无统计学意义(Z=−1.853~−1.158,t=−1.804、−0.132,均P>0.05)。 结论 CZT-SPECT断层显像可通过重建获得平面显像数据,结合采集性能优势,可在获得可靠的数据用于后期处理和获得准确的测量结果的同时,进一步降低检查中的辐射剂量或缩短时间。 -
关键词:
- 门控血池显像 /
- 碲锌镉 /
- 体层摄影术,发射型计算机,单光子 /
- 心室射血分数
Abstract:Objective To analyze the correlation and difference of biventricular function from planar gated equilibrium radionuclide angiography with conventional sodium iodide SPECT (NaI-SPECT planar imaging) and tomographic gated equilibrium radionuclide angiography with cadmium zinc telluride SPECT (CZT-SPECT tomographic imaging), and reconstructed-planar imaging from CZT-SPECT tomographic imaging (CZT-SPECT re-planar imaging) to investigate the methodology and advantages of CZT-SPECT tomographic imaging. Methods A retrospective analysis was performed on 58 patients (38 males and 20 females aged (60.6±12.3) years), who underwent gated equilibrium radionuclide angiography in TEDA International Cardiovascular Hospital from August 2021 to November 2022. All patients were subjected to NaI-SPECT planar imaging and CZT-SPECT tomographic imaging on the same day. CZT-SPECT tomographic imaging data were reprocessed in re-planar form and at different acquisition times. The left ventricular ejection fraction (LVEF) and right ventricular ejection fraction (RVEF) of NaI-SPECT planar imaging (P), CZT-SPECT tomographic imaging (T), and CZT-SPECT re-planar imaging (re) were compared and analyzed, and the CZT-SPECT tomographic imaging acquisition data at 3, 4, and 5 min were reconstructed. The LVEF (3 min), LVEF (4 min), LVEF (5 min), and RVEF (3 min), RVEF (4 min), RVEF (5 min) were compared with the original acquisition data LVEF (10 min) and RVEF (10 min), respectively. Divide LVEF (10 min) and RVEF (10 min) into subgroups of ≥20%, ≥30%, ≥40%, and ≥50%, and analyze them separately with the reconstructed data mentioned above. Paired t-test (or Wilcoxon signed rank test) and Pearson (or Spearman) were used in analyzing differences and correlations among the data. Results The differences among LVEF (re) (30.50% (20.00%, 38.50%)), LVEF (P) (31.00% (22.00%, 41.00%)), and LVEF (T) (27.00% (19.75%, 38.50%)) were statistically significant (Z=−2.645, −3.065; both P<0.05), whereas the differences between LVEF (re) and LVEF (P) were not statistically significant (Z=−1.057; P>0.05). No significant difference was found among RVEF (P) (39.78%±12.16%), RVEF (T) (41.57%±15.18%) and RVEF (re) (40.88%±13.19%; t=−1.949, −1.721, 0.883; all P>0.05). The LVEF and RVEF correlations obtained by the three imaging methods were excellent (r=0.892–0.946; all P<0.001). The differences between LVEF (3 min), LVEF (4 min), LVEF (5 min), and LVEF (10 min), and between RVEF (3 min), RVEF (4 min), RVEF (5 min), and RVEF (10 min) were statistically significant (Z=−2.798, −3.288, and −3.995; t=−2.187, −3.976, and −5.154; all P<0.05), and the correlations were excellent (r=0.903–0.970; all P<0.001). Subgroup analysis showed no significant difference between LVEF (5 min) and LVEF (10 min) and between RVEF (5 min) and RVEF (10 min) in all subgroups, except the LVEF≥20% subgroup (Z=−1.853 to −1.158; t=−1.804, −0.132; all P>0.05). Conclusions CZT-SPECT tomographic imaging can obtain planar datasets through reconstruction. Owing to its acquisition performance, CZT-SPECT tomographic imaging can further reduce the radiation dose or time for examination while obtaining reliable data for postprocessing and accurate measurement results. -
图 1 3种显像方法获得的LVEF之间的相关性散点图
Figure 1. Scatter plots of the correlation between the left ventricular ejection fraction obtained by the 3 imaging methods
图 2 3种显像方法获得的RVEF之间的相关性散点图
Figure 2. Scatter plots of the correlation between the right ventricular ejection fraction obtained by the 3 imaging methods
表 1 纳入的58例行放射性核素平衡法门控心血池显像的 患者的一般资料
Table 1. General data on the 58 included patients of gated equilibrium radionuclide cardio angiography
一般资料 例(%)或 $ \bar x\pm s $ 年龄(岁) 60.6±12.3 男性 38(65.5) 女性 20(34.5) 身高(cm) 167.3±8.5 体重(kg) 72.1±15.0 显像剂注射剂量(MBq) 802.9±66.6 LVEF(P)(%) 31.00(22.00,41.00) RVEF(P)(%) 39.78±12.16 危险因素 高血压 33(56.9) 高血脂 1(1.7) 糖尿病 8(13.8) 吸烟 26(44.8) 饮酒 22(37.9) 临床诊断 冠心病 20(34.5) 扩张型心肌病 19(32.8) 心力衰竭 20(34.5) 完全性左束支传导阻滞 20(34.5) 其他类型心律失常 10(17.2) 其他心脏疾病(瓣膜病、风湿性
心脏病、酒精性心肌病等)7(12.1) 注:LVEF(P)为NaI-SPECT平面显像获得的左心室射血分数;RVEF(P)为NaI-SPECT平面显像获得的右心室射血分数  下载: 导出CSV
下载: 导出CSV
表 2 CZT-SPECT断层显像患者重建不同采集时间获得的LVEF与原始数据获得的LVEF的各亚组之间的比较
Table 2. Comparison between subgroups of left ventricular ejection fraction obtained at different acquisition times and left ventricular ejection fraction obtained from raw data in patients with CZT-SPECT reconstruction
重建不同采集时间获得的LVEF LVEF(10 min)≥20% LVEF(10 min)≥30% LVEF(10 min)≥40% LVEF(10 min)≥50% (n=44) (n=25) (n=14) (n=7) 检验值 P值 检验值 P值 检验值 P值 检验值 P值 LVEF(3 min) −3.043a 0.002 −2.529a 0.011 −2.456a 0.014 −2.287b 0.062 LVEF(4 min) −2.837a 0.005 −2.513a 0.012 −2.203a 0.028 −2.976b 0.025 LVEF(5 min) 2.837a 0.004 −1.597a 0.110 −1.429a 0.153 −1.804b 0.121 注:CZT为碲锌镉;SPECT为单光子发射计算机体层摄影术;LVEF(3 min)、LVEF(4 min)、LVEF(5 min)分别为由原始数据重建采集时间为3、4、5 min的数据获得的左心室射血分数;LVEF(10 min)为采集时间为10 min的原始数据获得的左心室射血分数;a表示Z值;b表示t值
下载: 导出CSV
表 3 CZT-SPECT断层显像患者重建不同采集时间获得的RVEF与原始数据获得的RVEF的各亚组之间的比较
Table 3. Comparison between subgroups of right ventricular ejection fraction obtained at different acquisition times and right ventricular ejection fraction obtained from raw data in patients with CZT-SPECT reconstruction
重建不同采集时间获得的RVEF RVEF(10 min)≥20% RVEF(10 min)≥30% RVEF(10 min)≥40% RVEF(10 min)≥50% (n=56) (n=44) (n=31) (n=16) 检验值 P值 检验值 P值 检验值 P值 检验值 P值 RVEF(3 min) −4.229a <0.001 −3.956a <0.001 −3.659a <0.001 −3.381b 0.004 RVEF(4 min) −3.760a <0.001 −3.327a 0.001 −3.724a <0.001 −4.015b 0.001 RVEF(5 min) −1.853a 0.064 −1.339a 0.180 −1.158a 0.247 −0.132b 0.897 注:CZT为碲锌镉;SPECT为单光子发射计算机体层摄影术;RVEF(3 min)、RVEF(4 min)、RVEF(5 min)分别为由原始数据重建采集时间为3、4、5 min的数据获得的右心室射血分数;RVEF(10 min)为采集时间为10 min的原始数据获得的右心室射血分数;a表示Z值;b表示t值
下载: 导出CSV
-
[1] Totzeck M, Aide N, Bauersachs J, et al. Nuclear medicine in the assessment and prevention of cancer therapy-related cardiotoxicity: prospects and proposal of use by the European Association of Nuclear Medicine (EANM)[J]. Eur J Nucl Med Mol Imaging, 2023, 50(3): 792−812. DOI: 10.1007/s00259-022-05991-7. [2] Polomski EAS, Antoni ML, Jukema JW, et al. Nuclear medicine imaging methods of radiation-induced cardiotoxicity[J]. Semin Nucl Med, 2022, 52(5): 597−610. DOI: 10.1053/j.semnuclmed.2022.02.001. [3] Naya M, Manabe O, Koyanagawa K, et al. The role of nuclear medicine in assessments of cardiac dyssynchrony[J]. J Nucl Cardiol, 2018, 25(6): 1980−1987. DOI: 10.1007/s12350-017-1072-z. [4] Steelant B, Stankovic I, Roijakkers I, et al. The impact of infarct location and extent on LV motion patterns: implications for dyssynchrony assessment[J]. JACC Cardiovasc Imaging, 2016, 9(6): 655−664. DOI: 10.1016/j.jcmg.2015.07.021. [5] Tonge CM, Fernandez RC, Harbinson MT. Commentary: current issues in nuclear cardiology[J]. Br J Radiol, 2008, 81(964): 270−274. DOI: 10.1259/bjr/59260451. [6] Apert A, Canu M, Jankowski A, et al. Comparison of cadmium zinc telluride ECG-gated SPECT equilibrium radionuclide angiocardiography to magnetic resonance imaging to measure right ventricular volumes and ejection fraction in patients with cardiomyopathy[J]. J Nucl Cardiol, 2022, 29(4): 1647−1656. DOI: 10.1007/s12350-021-02653-3. [7] Xie BQ, Tian YQ, Zhang J, et al. Evaluation of left and right ventricular ejection fraction and volumes from gated blood-pool SPECT in patients with dilated cardiomyopathy: comparison with cardiac MRI[J]. J Nucl Med, 2012, 53(4): 584−591. DOI: 10.2967/jnumed.111.096057. [8] Lairez O, Delmas C, Fournier P, et al. Feasibility and accuracy of gated blood pool SPECT equilibrium radionuclide ventriculography for the assessment of left and right ventricular volumes and function in patients with left ventricular assist devices[J]. J Nucl Cardiol, 2018, 25(2): 625−634. DOI: 10.1007/s12350-016-0670-5. [9] Einstein AJ, Blankstein R, Andrews H, et al. Comparison of image quality, myocardial perfusion, and left ventricular function between standard imaging and single-injection ultra-low-dose imaging using a high-efficiency SPECT camera: the MILLISIEVERT study[J]. J Nucl Med, 2014, 55(9): 1430−1437. DOI: 10.2967/jnumed.114.138222. [10] Bailly M, Le Rouzic G, Metrard G. Gated tomographic radionuclide angiography using CZT gamma camera in patients receiving cardiotoxic chemotherapy: going faster and less irradiating[J]. Clin Nucl Med, 2019, 44(6): 472−474. DOI: 10.1097/RLU.0000000000002569. [11] Tissot H, Roch V, Morel O, et al. Left ventricular ejection fraction determined with the simulation of a very low-dose CZT-SPECT protocol and an additional count-calibration on planar radionuclide angiographic data[J]. J Nucl Cardiol, 2019, 26(5): 1539−1549. DOI: 10.1007/s12350-019-01619-w. [12] Liu YH, Fazzone-Chettiar R, Sandoval V, et al. New approach for quantification of left ventricular function from low-dose gated bloodpool SPECT: validation and comparison with conventional methods in patients[J]. J Nucl Cardiol, 2021, 28(3): 939−950. DOI: 10.1007/s12350-019-01823-8. [13] Hansen NL, Haarmark C, Zerahn B. Ventricular peak emptying and filling rates measured by gated tomographic radionuclide angiography using a cadmium-zinc-telluride SPECT camera in chemotherapy-naïve cancer patients[J]. J Nucl Cardiol, 2020, 27(4): 1193−1201. DOI: 10.1007/s12350-019-01756-2. [14] Rydberg J, Andersen J, Haarmark C, et al. The influence of anthropometric and basic circulatory variables on count rate in cadmium-zinc-telluride SPECT gated radionuclide angiography[J]. J Nucl Cardiol, 2019, 26(6): 1974−1980. DOI: 10.1007/s12350-018-1402-9. [15] Wells RG, Marvin B, Kovalski G, et al. Planar radionuclide angiography with a dedicated cardiac SPECT camera[J]. J Nucl Cardiol, 2013, 20(3): 358−366. DOI: 10.1007/s12350-013-9674-6. [16] Duvall WL, Guma-Demers KA, George T, et al. Radiation reduction and faster acquisition times with SPECT gated blood pool scans using a high-efficiency cardiac SPECT camera[J]. J Nucl Cardiol, 2016, 23(5): 1128−1138. DOI: 10.1007/s12350-015-0214-4. [17] Chen YC, Ko CL, Yen RF, et al. Comparison of biventricular ejection fractions using cadmium-zinc-telluride SPECT and planar equilibrium radionuclide angiography[J]. J Nucl Cardiol, 2016, 23(3): 348−361. DOI: 10.1007/s12350-015-0367-1. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 2447
- HTML全文浏览量: 2002
- PDF下载量: 17
