


-
儿童卵巢扭转为少见且严重的小儿妇科急症,约占小儿急性腹痛全部病例的2.7%[1]。儿童卵巢扭转缺乏临床特异性,诊断较困难[2]。如延误治疗,后果严重[3]。因此,正确的诊断和治疗对于保留儿童卵巢及附件功能是非常重要的[4]。临床医师可根据患儿病史、体征、辅助检查等结果进行综合判断,目前诊断多依赖于影像学检查,优选超声检查,但其容易受到肠气、操作者经验和手法等诸多因素影响,明确诊断比较困难。MRI检查所需时间长、费用高,且对儿童镇静的条件有较高要求,临床应用相对较少。多层螺旋CT(mutislice spiral CT,MSCT)的优势在于成像速度快,多平面重建等图像后处理技术可清晰显示出解剖结构的细节,是诊断小儿卵巢扭转的重要方法之一。本研究回顾性分析30例卵巢扭转患儿的临床与影像资料,探讨MSCT的特征及其诊断价值,旨在提高小儿卵巢扭转诊断的准确率,最大程度地保留儿童卵巢功能和生育能力[5]。
-
回顾性分析2014年1月至2018年6月于天津市儿童医院经手术免疫组织化学检查确诊为卵巢扭转的30例女患儿的临床资料与影像资料,年龄2~12岁,中位年龄9.3岁。纳入标准:(1)年龄为2~12岁的女童;(2)手术证实为单纯卵巢扭转及卵巢占位合并扭转;(3)有完整腹部MSCT相关影像资料,且图像质量良好。排除标准:(1)术前未进行腹部CT影像检查;(2)存在呼吸伪影,图像模糊。本研究符合《赫尔辛基宣言》的原则。所有患儿家属均于检查前签署了知情同意书。
-
30例患儿均于术前接受腹部MSCT平扫检查。对于6岁以下不配合检查的患儿,口服水合氯醛(0.5 ml/kg)予以镇静。检查均使用美国GE公司Revolution CT扫描仪,扫描范围自膈顶到盆底。扫描参数:管电压 100 kV、Smart mA 自动管电流(60~300 mA),噪声指数 13.0。 CT 剂量指数 1.0~1.8 mGy,中位值 1.43 mGy。对原始图像进行薄层重建,使用多平面重建(MPR)、最大密度投影(MIP)、容积再现(VR)等技术进行后处理。由2名放射科副主任医师阅片,重点观察病灶部位、形态、密度及子宫偏移、盆腔积液等。如果意见不统一,由主任医师审阅、科室内讨论达成一致意见。
-
30例患儿均行腹腔镜探查,卵巢及附件扭转复位后血供恢复的行保守治疗,合并占位的同时祛除病变,若已坏死行卵巢及附件切除术。使用美国Ventanna公司的全自动免疫组织化学染色机(BenchMark ULTRA型)进行免疫组织化学检查,按照说明书步骤进行操作,即脱蜡2 h,热预处理56 min,加抗体后37 ℃孵育36 min,苏木精复染2 min后封片,即可在显微镜下观察。
-
30例患儿按照单纯性卵巢扭转、卵巢囊肿合并扭转、卵巢畸胎瘤合并扭转排序,中位年龄分别为6.8、10.2、5.3岁。21例患儿以腹痛就诊,疼痛持续时间为3 h~15 d不等,12例为持续性腹痛、30例患儿均出现不同程度呕吐。其他具体临床表现见表1。
组别 临床表现 MSCT表现(例) 中位年龄
[M(Q1,Q3),岁]就诊症状 疼痛持续时间
[M(Q1,Q3),d]患侧卵巢肿大 子宫偏位 盆腔积液 合并钙化 混合密度肿物 单纯性卵巢扭转(n=9) 6.8(6.0,7.5) 腹痛、呕吐 4.5(3.0,7.5) 8 6 7 1 7 卵巢占位合并扭转 卵巢囊肿合并扭转(n=15) 10.2(9.2,12.0) 腹痛、呕吐 7.0(3.0,11.0) 13 11 11 1 13 卵巢畸胎瘤合并扭转(n=6) 5.3(2.8,7.0) 腹痛、呕吐 4.0(3.5,5.5) 6 3 5 6 6 注:MSCT为多层螺旋计算机体层摄影术 表 1 30例卵巢扭转患儿的临床表现和MSCT表现
Table 1. Clinical characteristics and multislice spiral CT findings of 30 children with ovarian torsion
-
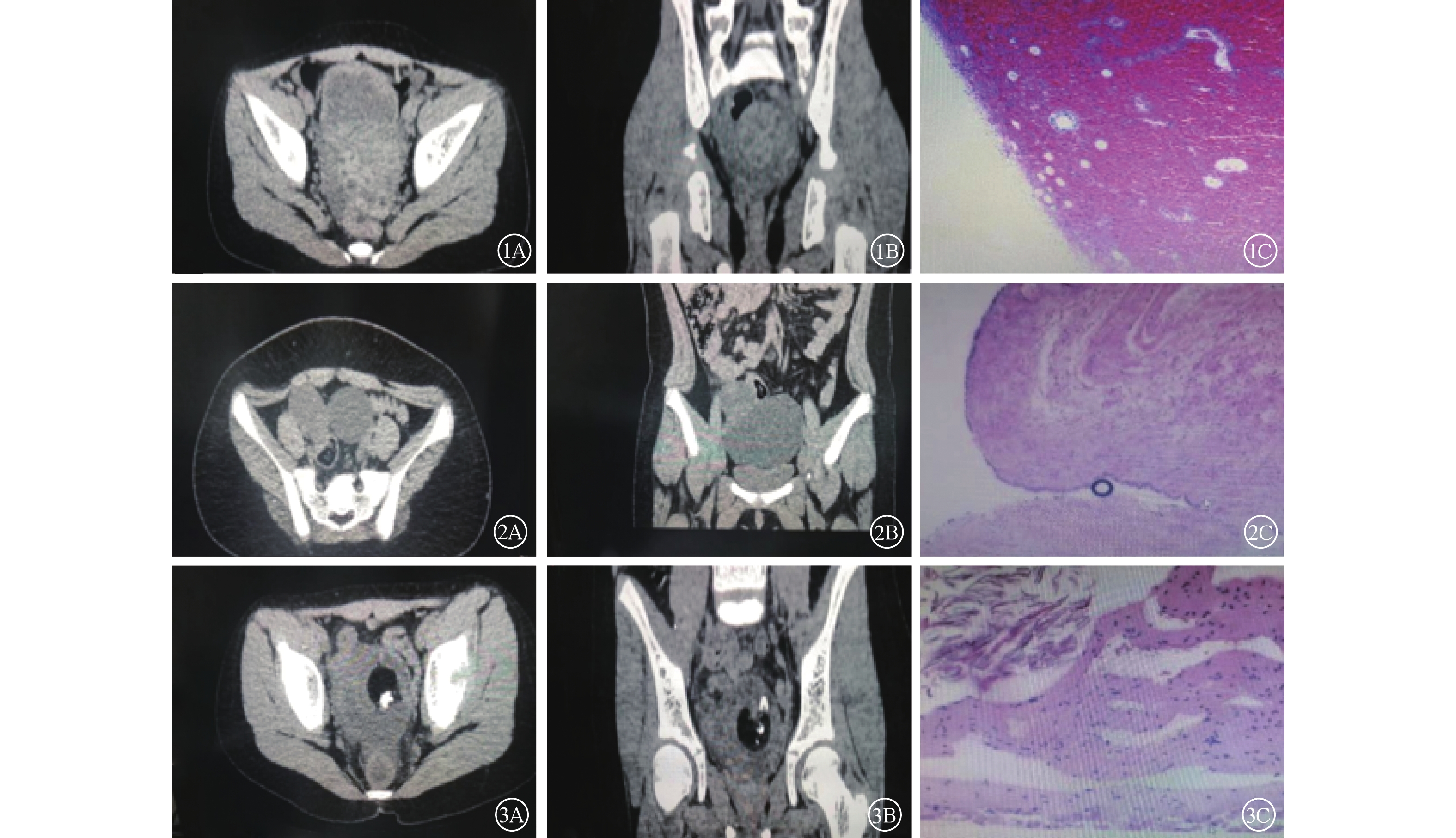
30例患儿经手术和免疫组织化学检查证实为单纯性卵巢扭转9例(图1)、卵巢囊肿合并扭转15例(图2)、卵巢畸胎瘤合并扭转6例(图3)。22例(73.3%,22/30)发生于右侧,8例(26.7%,8/30)发生于左侧。

图 1~3 卵巢扭转患儿的MSCT图及免疫组织化学检查图(Envision法,×100)
Figure 1~3. Multislice spiral CT and immunohistochemistry in children with varian torsion (Envision method, ×100)
-
由表1可见,在30例患儿中,27例(90.0%)患侧卵巢均有不同程度肿大伴密度不均匀增高,8例(26.7%)伴有钙化,13例(43.3%)显示卵巢周边蜂窝状改变的增大滤泡, 12例(40.0%)出现周围脂肪间隙模糊,20例(66.7%)子宫不同程度向患侧卵巢移位,23例(76.7%)伴有盆腔少量积液。
-
卵巢扭转按其病因分为单纯性与继发性2种。单纯性卵巢扭转主要是由于固定卵巢的韧带结构出现扭转,并由此导致卵巢组织大量缺血、坏死。而儿童出现卵巢扭转还与先天性卵巢及输卵管系膜过长以及儿童好动、活动量大有关。青春期由于卵巢受激素的影响而呈生理性增大,失去了子宫支持从而出现扭转。此外,还有一些因素可影响卵巢的发育而导致其扭转。继发性卵巢扭转多继发于卵巢占位,其中以畸胎瘤和卵巢囊肿多见[6]。卵巢扭转以右侧多发,这可能与乙状结肠位于盆腔左侧,以及受盲肠和末端回肠活动度高等因素密切相关[7]。本研究30例患儿中,22例发生于右侧、8例发生于左侧,与以上研究结果相符。
目前国内外研究者认为,可以根据临床和影像特征正确诊断儿童卵巢扭转[8-10]。通过本研究结果,我们发现儿童卵巢扭转除具有相对特异性的MSCT征象外,其表现与卵巢血供受阻时间、范围、程度等也密切相关。主要影像特征包括以下表现。(1)大小形态变化:患侧卵巢体积增大,右侧明显多于左侧。(2)单纯性卵巢扭转较继发性卵巢扭转少见。(3)密度变化:患侧卵巢密度不均匀性增高,扭转初期血流改变是静脉受压、循环回流受阻,且动脉血供恢复正常,导致卵巢充血增大,卵巢周围分布着向外移位的卵泡影,这是由于扭转致静脉回流障碍,卵巢间质内压增高而形成的滤泡样影像。表现为卵巢周围小圆形低密度影,该征象在薄层和多平面重建图像上显示更为清晰,为单纯性卵巢扭转特征性的表现[11]。(4)包膜下积液征:若扭转持续发展,外移之水肿卵泡可发生破裂,形成卵巢包膜下积液,这表明病情较重,提示可能发生卵巢坏死。(5)盆腔积液:卵巢动脉的不断受压和堵塞可能会造成血管断裂,严重者会引起卵巢或者卵巢肿瘤的破裂,进而出现盆腔积液。(6)子宫患侧偏位征:卵巢系膜由于扭转、变短,会牵拉子宫,使子宫位移到患侧,该征象可鉴别卵巢扭转和单纯的附件区占位[12]。 (7)继发性卵巢扭转:儿童期继发性卵巢扭转最常见于卵巢囊肿或卵巢畸胎瘤伴扭转,在MSCT上均可见附件区包块影。前者表现为囊性稍低密度影,部分病例因合并出血使囊内密度有所增高,并形成液-液平面;后者典型的病例可见钙化、脂肪成分,而MSCT对诊断这两种成分非常灵敏。综上所述,MSCT不仅是一种快速有效的方法,还可与其他具有类似临床表现的疾病相鉴别,因此MSCT检查在儿童卵巢扭转中具有重要的辅助诊断价值。
综上所述,MSCT在儿童卵巢扭转中具有一定特征性表现,根据临床和影像特征可以建立正确的诊断[13]。这不仅能明确卵巢扭转的病因及鉴别诊断,还可根据MSCT上卵巢实质的改变进一步评价卵巢扭转和淤血程度。因此,卵巢扭转的影像检查是本研究患儿确诊的重要基础,也是挽救患儿生育能力的关键。另外,在临床工作中,MSCT诊断的准确率与影像科医师的个体诊断水平密切相关,因此,我们应当进一步提高临床医师的阅片水平,结合临床其他资料提高卵巢扭转的诊断率。
利益冲突 所有作者声明无利益冲突
作者贡献声明 杨宏负责研究命题的提出与设计、论文的撰写;王春祥负责论文的审阅与修订;闫喆负责数据的分析;王月负责病历资料的调查
MSCT 在儿童卵巢扭转中的诊断价值
The value of MSCT in diagnosis of ovarian torsion in children
-
摘要:
目的 探究多层螺旋CT(MSCT)检查在儿童卵巢扭转诊断中的应用价值。 方法 回顾性分析2014年1月至2018年6月于天津市儿童医院经术后免疫组织化学检查确诊为卵巢扭转的30例女患儿的临床资料与影像资料,年龄2~12岁,中位年龄9.3岁。所有患儿均于术前行腹部MSCT检查,主要观察卵巢扭转后的大小、形态、密度以及子宫附件是否发生异常变化。术后行免疫组织化学检查。 结果 30例卵巢扭转患儿中,发生于右侧者22例(73.3%,22/30)、左侧者8例(26.7%,8/30);9例(30.0%,9/30)证实为单纯性卵巢扭转、21例(70.0%,21/30)合并占位性病变。MSCT检查结果显示,27例(90.0%,27/30)患侧卵巢均有不同程度肿大伴密度增高,8例(26.7%,8/30)伴有钙化,13例(43.3%,13/30)显示卵巢周边蜂窝状改变的增大滤泡,12例(40.0%,12/30)出现周围脂肪间隙模糊,20例(66.7%,20/30)子宫不同程度向患侧卵巢移位,23例(76.7%,23/30)伴有盆腔少量积液。 结论 MSCT可作为儿童卵巢扭转的重要辅助诊断手段,有助于提高卵巢扭转的检出率,为临床治疗提供参考依据。 -
关键词:
- 卵巢扭转 /
- 儿童 /
- 体层摄影术,螺旋计算机
Abstract:Objective To explore the value of multislice spiral CT (MSCT) in the diagnosis of ovarian torsion in children. Methods The clinical and imaging data of 30 female children with ovarian torsion confirmed by postoperative immunohistochemistry in Tianjin Children's Hospital from January 2014 to June 2018 were retrospectively analyzed. The children's age ranged from 2 years to 12 years, with a median age of 9.3 years. All children were examined via abdominal MSCT before operation to observe the size, shape, density, and abnormal changes in uterine appendages after ovarian torsion. Immunohistochemical examination was performed after operation. Results Among the 30 cases, ovarian torsion occurred on the right side in 22 cases (73.3%, 22/30) and on the left side in 8 cases (26.7%, 8/30). Nine cases (30.0%, 9/30) were confirmed as having simple ovarian torsion, and 21 cases (70.0%, 21/30) were complicated with space-occupying lesions. The MCST results showed that 27 cases (90.0%, 27/30) of the affected ovaries had different degrees of enlargement with increased density, 8 cases (26.7%, 8/30) had calcification, and 13 cases (43.3%, 13/30) showed enlarged follicles with honeycomb changes around the ovaries. Meanwhile, 12 cases (40.0%, 12/30) showed blurred peripheral fat space, 20 cases (66.7%, 20/30) had different degrees of uterine displacement to the affected ovary, and 23 cases (76.7%, 23/30) had a small amount of accumulated pelvic fluid. Conclusions MSCT can be used as an important auxiliary diagnostic tool for ovarian torsion in children. It can help improve the detection rate of ovarian torsion and provide a reference for clinical treatment. -
Key words:
- Ovarian torsion /
- Children /
- Tomography, spiral computed
-
图 1~3 卵巢扭转患儿的MSCT图及免疫组织化学检查图(Envision法,×100)
Figure 1~3. Multislice spiral CT and immunohistochemistry in children with varian torsion (Envision method, ×100)
表 1 30例卵巢扭转患儿的临床表现和MSCT表现
Table 1. Clinical characteristics and multislice spiral CT findings of 30 children with ovarian torsion
组别 临床表现 MSCT表现(例) 中位年龄
[M(Q1,Q3),岁]就诊症状 疼痛持续时间
[M(Q1,Q3),d]患侧卵巢肿大 子宫偏位 盆腔积液 合并钙化 混合密度肿物 单纯性卵巢扭转(n=9) 6.8(6.0,7.5) 腹痛、呕吐 4.5(3.0,7.5) 8 6 7 1 7 卵巢占位合并扭转 卵巢囊肿合并扭转(n=15) 10.2(9.2,12.0) 腹痛、呕吐 7.0(3.0,11.0) 13 11 11 1 13 卵巢畸胎瘤合并扭转(n=6) 5.3(2.8,7.0) 腹痛、呕吐 4.0(3.5,5.5) 6 3 5 6 6 注:MSCT为多层螺旋计算机体层摄影术  下载: 导出CSV
下载: 导出CSV
-
[1] 杨宏, 董亮, 董迎, 等. 儿童卵巢扭转64例诊治体会[J]. 天津医药, 2014, 42(2): 186−187. DOI: 10.3969/j.jssn.0253-9896.2014.02.027.
Yang H, Dong L, Dong Y, et al. The diagnosis and treatment of 64 children with ovarian torsion[J]. Tianjin Med J, 2014, 42(2): 186−187. DOI: 10.3969/j.jssn.0253-9896.2014.02.027.[2] Bolli P, Schädelin S, Holland-Cunz S, et al. Ovarian torsion in children: development of a predictive score[J]. Medicine (Baltimore), 2017, 96(43): e8299. DOI: 10.1097/MD.0000000000008299. [3] 裴广华, 王景福, 郑津生, 等. 超声诊断小儿卵巢扭转的价值[J]. 天津医药, 2005, 33(2): 93−95. DOI: 10.3969/j.issn.0253-9896.2005.02.010.
Pei GH, Wang JF, Zheng JS, et al. Diagnostic value of ultrasonography in children with ovarian torsion[J]. Tianjin Med J, 2005, 33(2): 93−95. DOI: 10.3969/j.issn.0253-9896.2005.02.010.[4] Singh S, Sasmal PK, Nagarajan K. CT imaging in predicting ovarian torsion: report of two cases, with and without infarction[J/OL]. Cureus, 2021, 13(8): e17082[2022-11-22]. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8432481. DOI: 10.7759/cureus.17082. [5] 童成文, 罗小琴, 陈光斌, 等. 多层螺旋CT在儿童卵巢蒂扭转中的诊断价值[J]. 医学影像学杂志, 2019, 29(12): 2095−2097, 2106.
Tong CW, Luo XQ, Chen GB, et al. Diagnostic value of multislice spiral CT in torsion of ovarian pedicle in children[J]. J Med Imaging, 2019, 29(12): 2095−2097, 2106.[6] 熊婧, 路丽, 吕志宝. 儿童卵巢扭转相关危险因素分析[J]. 中华小儿外科杂志, 2020, 41(5): 390−394. DOI: 10.3760/cma.j.cn421158-20200106-00008.
Xiong J, Lu L, Lyu ZB. An analysis of risk factors related with ovarian torsion in children[J]. Chin J Pediatr Surg, 2020, 41(5): 390−394. DOI: 10.3760/cma.j.cn421158-20200106-00008.[7] Dasgupta R, Renaud E, Goldin AB, et al. Ovarian torsion in pediatric and adolescent patients: a systematic review[J]. J Pediatr Surg, 2018, 53(7): 1387−1391. DOI: 10.1016/j.jpedsurg.2017.10.053. [8] Raman Patil A, Nandikoor S, Chaitanya Reddy S. CT in the diagnosis of adnexal torsion: a retrospective study[J]. J Obstet Gynaecol, 2020, 40(3): 388−394. DOI: 10.1080/01443615.2019.1633514. [9] Mentessidou A, Mirilas P. Surgical disorders in pediatric and adolescent gynecology: adnexal abnormalities[J/OL]. Int J Gynaecol Obstet, 2022, 00: 1−9[2022-11-22]. https://obgyn.onlinelibrary.wiley.com/doi/10.1002/ijgo.14574. DOI: 10.1002/ijgo.14574. [10] 鹿连伟, 吴慧莹, 刘强, 等. 儿童附件扭转的CT特征与临床对照分析[J]. 中山大学学报(医学科学版), 2021, 42(1): 124−132. DOI: 10.13471/j.cnki.j.sun.yat-sen.univ(med.sci).2021.0017.
Lu LW, Wu HY, Liu Q, et al. CT feature and clinical analysis of adnexal torsion in children[J]. J Sun Yat-sen Univ: Med Sci, 2021, 42(1): 124−132. DOI: 10.13471/j.cnki.j.sun.yat-sen.univ(med.sci).2021.0017.[11] 丁永刚, 蔡金华, 秦勇, 等. 儿童卵巢扭转的MSCT表现[J]. 中国介入影像与治疗学, 2015, 12(6): 349−352. DOI: 10.13929/j.1672-8475.2015.06.007.
Ding YG, Cai JH, Qin Y, et al. MSCT manifestations of ovarian torsion in children[J]. Chin J Interv Imaging Ther, 2015, 12(6): 349−352. DOI: 10.13929/j.1672-8475.2015.06.007.[12] 王健, 张大江, 杨奇芳, 等. 儿童卵巢扭转的影像学征象及卵巢坏死评估[J]. 放射学实践, 2018, 33(2): 197−201. DOI: 10.13609/j.cnki.1000-0313.2018.02.018.
Wang J, Zhang DJ, Yang QF, et al. The analysis of imaging features of ovarian torsion in children and evaluation of ovarian necrosis[J]. Radiol Pract, 2018, 33(2): 197−201. DOI: 10.13609/j.cnki.1000-0313.2018.02.018.[13] Li DM, Zhang JW, Kiryu S, et al. Clinical and CT features of ovarian torsion in infants, children and adolescents[J]. Int J Gynaecol Obstet, 2022, 156(3): 444−449. DOI: 10.1002/ijgo.13657. -

 点击查看大图
点击查看大图
图(1)表(1)
计量
- 文章访问数: 2453
- HTML全文浏览量: 1853
- PDF下载量: 10