




-
131I治疗是DTC术后患者综合治疗的主要方法之一。在行首次131I治疗后,DTC术后患者唾液腺的摄取及排泌功能会受到不同程度的影响,其发生率为46%~78%[1-2]。国外大量研究结果表明,年龄、性别、131I治疗剂量、唾液腺疾病、TSH水平、身体质量指数(body mass index,BMI)、收缩压、舒张压、肿瘤分期、糖尿病史、淋巴结受累情况、131I全身扫描(whole body scan,WBS)结果、左甲状腺素钠片(levothyroxine sodium,L-T4)停药时间、DTC术后行131I治疗的时间等是DTC患者发生唾液腺损伤的危险因素[3-8]。目前,国内研究DTC患者术后行131I治疗发生唾液腺损伤的预测因素的文献报道非常有限。本研究中,我们回顾性分析107例接受首次131I治疗的DTC术后患者的临床资料,探讨131I治疗对唾液腺功能损伤的影响因素,旨在发现我国DTC术后131I治疗患者唾液腺功能损伤的危险因素。
-
回顾性分析2019年1月至2022年7月于山西医科大学第一医院行131I治疗的107例DTC患者的临床资料,其中男性35例、女性72例,年龄(42.8±1.0)岁。纳入标准:(1)首次行131I清甲治疗;(2)行甲状腺全切手术;(3)组织病理学结果诊断为DTC(包括乳头状甲状腺癌、滤泡状甲状腺癌和混合性甲状腺癌);(4)唾液腺动态显像示双侧腮腺的排泌分数(excretion fraction,EF)≥50%。排除标准:(1)首次131I治疗前长期口干;(2)既往有头颈部放疗史或接受过任何131I 标记的放射性药物治疗;(3)有严重的心脏、肝脏、肾脏功能障碍;(4)唾液腺病变(结石、肿瘤和接受过手术治疗);(5)有甲状腺功能亢进症(毒性结节、毒性多结节性甲状腺肿和Graves病);(6)患者在131I治疗前1天和治疗后1个月未同时行唾液腺动态显像。所有患者均于检查前签署了知情同意书。本研究获得山西医科大学第一临床医学院伦理委员会的批准(批准号:2019伦审字SK003)。
-
收集107例DTC患者的年龄、性别、BMI、收缩压、舒张压、原发肿瘤的组织病理学分型及分期、是否有淋巴结转移、是否有糖尿病、131I治疗前TSH水平、停用L-T4时间、131I治疗剂量、131I WBS结果等资料。年龄、BMI、收缩压、舒张压、TSH水平均为131I治疗前2天的情况。患者服用131I治疗后2~4 d行131I WBS,结果分为阴性(颈部无131I摄取)、阳性(颈部存在131I摄取)和远处转移(颈部和远处器官存在131I摄取)。
-
所有患者分别于131I治疗前1天和治疗后1个月行唾液腺动态显像。嘱患者取仰卧位,使用SYMBIA T16型 SPECT/CT(德国西门子医疗器械有限公司)和ImaginE NET 632 型 SPECT(北京永新医疗设备有限公司)进行显像,显像参数:矩阵64×64,窗宽20%,能峰140 keV,放大1.5倍。经患者静脉注射222~296 MBq 99TcmO4 − (原子高科股份有限公司)后,即刻开始连续采集图像,以每帧60 s的速度(60 s/1 F)采集20 min后,即采集至第20帧时嘱患者保持头颈部静止,给予患者维生素C片(300 mg)含化,继续采集图像,至采集30 min结束。测量99TcmO4 −注射前和注射后注射器内的放射性计数,以计算注入患者体内的显像剂剂量。
-
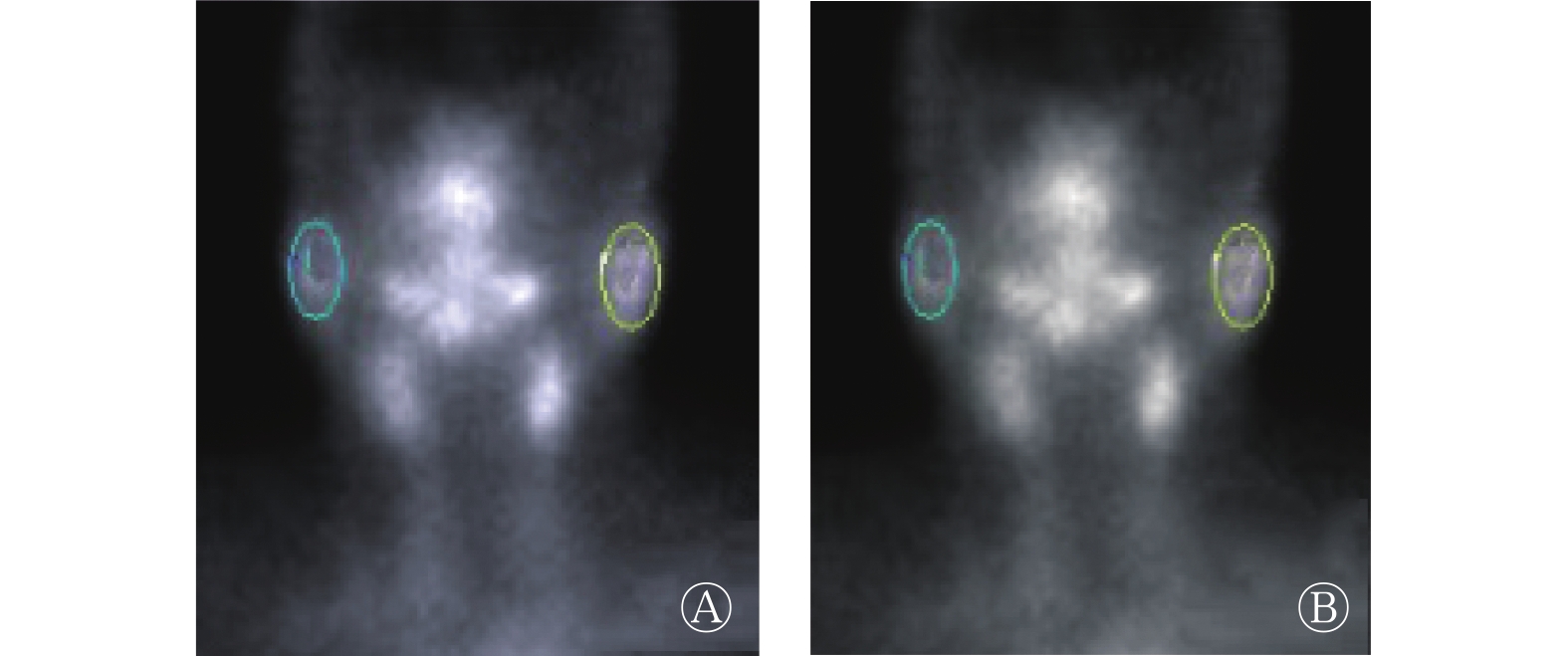
由2名具有3年及以上经验的核医学科医师共同对唾液腺动态显像图像进行分析,通过NMSoft-DIM软件(北京奈米软件科技有限公司)勾画双侧腮腺的ROI及其所对应的本底(图1)。利用腮腺时间-放射性曲线(TAC),计算腮腺的EF(EF可作为评估DTC患者131I治疗后唾液腺功能是否正常的参数),EF=(腺体最大放射性计数−腺体最小放射性计数)/(腺体最大放射性计数−本底放射性计数)×100% 。根据双侧腮腺的EF结果将唾液腺功能分为正常和损伤2种情况[9-10]。唾液腺功能正常:双侧腮腺EF≥50%;唾液腺功能损伤:一侧或双侧腮腺EF<50%。

图 1 接受131I治疗的分化型甲状腺癌患者正常唾液腺(A)和损伤唾液腺(B)感兴趣区勾画的示意图
Figure 1. Schematic diagram of the region of interest outlined of normal salivary glands (A) and injury salivary glands (B) in patients with differentiated thyroid cancer after 131I treatment
-
应用 SPSS 25.0 软件对数据进行统计学分析。符合正态分布的计量资料用
$\bar x \pm s $ 表示,组间比较采用单因素方差分析(ANOVA);计数资料以百分比(%)表示,组间比较采用χ2检验,期望频数<5时采用Fisher确切概率法。采用单因素分析比较唾液腺正常和唾液腺损伤DTC患者的临床资料,将单因素分析有统计学意义的因素采用二分类Logistic回归分析进行多因素分析,确定影响唾液腺损伤的独立危险因素。P<0.05为差异有统计学意义。 -
107例患者均为甲状腺乳头状癌,其中唾液腺正常患者70例,唾液腺损伤患者37例,唾液腺损伤发生率为34.6%(表1)。唾液腺正常患者和唾液腺损伤患者的唾液腺动态显像图分别见图2和图3。
因素 唾液腺损伤(n=37) 唾液腺正常(n=70) 检验值 P值 年龄(岁, $\bar x \pm s $ 

45.84±2.10 41.11±0.97 F=5.457 0.046 BMI( $\bar x \pm s $ 

22.02±1.35 24.71±0.43 F=5.556 0.064 收缩压(mm Hg, $\bar x \pm s $ 

127.59±3.10 119.86±1.84 F=5.210 0.024 舒张压(mm Hg, $\bar x \pm s $ 

83.06±1.82 82.01±1.24 F=0.231 0.632 糖尿病(例,%) − 0.657 有 1(2.7) 4(5.7) 无 36(97.3) 66(94.3) 组织病理学分型 − 1.000 乳头状癌 37(100) 70(100) 肿瘤分期 χ2=0.830 0.362 Ⅰ期 27(73.0) 45(64.3) Ⅱ期 10(27.0) 25(35.7) 淋巴结转移(例,%) − 0.769 有 29(78.4) 61(87.1) 无 8(21.6) 9(12.9) 131I治疗剂量(例,%) − 0.568 <3.7 GBq 0(0) 1(1.4) 3.7~5.6 GBq 34(91.9) 67(95.7) >5.6 GBq 3(8.1) 2(2.9) 131I治疗前TSH水平(mIU/L, $\bar x \pm s $ 

99.82±8.46 122.59±4.03 F=6.288 0.019 L-T4服用情况(例,%) χ2=1.613 0.204 停用1个月 18(48.6) 43(61.4) 未服用 19(51.4) 27(38.6) 术后月数(月, $\bar x \pm s $ 

1.94±0.18 2.25±0.21 F=0.899 0.345 131I WBS结果 − 0.543 阴性 0(0) 2(2.9) 阳性 37(100) 68(97.1) 注:−表示使用Fisher确切概率法,无检验值。BMI为身体质量指数;TSH为促甲状腺激素;L-T4为左甲状腺素钠片;WBS为全身扫描 表 1 107例分化型甲状腺癌患者131I治疗后影响唾液腺功能损伤的单因素分析
Table 1. Univariate analysis of factors affecting salivary gland function injury in 107 patients with differentiated thyroid cancer after 131I treatment

图 2 接受131I治疗的分化型甲状腺癌患者(女性,48岁)的正常唾液腺动态显像图
Figure 2. Dynamic imaging of normal salivary glands in a patient with differentiated thyroid cancer (female, 48 years old) after 131I treatment

图 3 接受131I治疗的分化型甲状腺癌患者(女性,27岁)的损伤唾液腺动态显像图
Figure 3. Dynamic imaging of injured salivary glands in a patient with differentiated thyroid cancer (female, 27 years old) after 131I treatment
-
单因素分析结果显示,患者的年龄、131I治疗前TSH水平、收缩压与DTC患者131I治疗后唾液腺功能损伤有关,唾液腺损伤患者的年龄、收缩压大于唾液腺正常患者,唾液腺损伤患者131I治疗前TSH水平低于唾液腺正常患者,且差异均有统计学意义(均P<0.05)(表1)。
-
多因素Logistic 回归分析结果显示,年龄、131I治疗前TSH水平、收缩压是唾液腺功能损伤的非独立危险因素(均P>0.05)(表2)。
因素 B值 Wald值 OR值 95%CI P值 年龄 0.017 0.443 1.017 0.968~1.068 0.506 131I治疗前TSH水平 −0.011 3.771 0.989 0.979~1.000 0.052 收缩压 0.023 2.592 1.023 0.995~1.051 0.107 注:TSH为促甲状腺激素;OR为比值比;CI为置信区间 表 2 分化型甲状腺癌患者131I治疗后影响唾液腺功能损伤的多因素Logistic 回归分析
Table 2. Multivariate Logistic regression analysis of factors affecting salivary gland function injury in patients with differentiated thyroid cancer after 131I treatment
-
目前, 甲状腺全切、服用131I、甲状腺激素替代治疗是国内外公认的DTC患者的治疗方法,其中131I 治疗的疗效确切且安全有效,目前已被临床广泛应用。131I可通过β射线杀灭残留甲状腺组织和存在于其他组织中的微小甲状腺癌病灶,从而降低甲状腺癌复发和转移的可能。 因唾液腺内具有与甲状腺组织相同的钠碘同向转运体(NIS)[11],所以131I治疗会对唾液腺造成一定的辐射损伤。对于DTC患者来说,早期识别和发现影响唾液腺功能损伤的潜在因素非常重要。
唾液腺的辐射损伤通常表现为放射性唾液腺损伤。Lee等[3]对 164 例在131I治疗6个月后接受甲状腺超声检查的患者进行随访,以患者在131I治疗后6~27个月的主观症状评估其唾液腺的功能状态,结果显示,患者年龄与唾液腺损伤的发生无相关性。但也有研究结果表明,年龄较大可能是甲状腺癌术后患者唾液腺功能障碍的危险因素[6]。一项前瞻性队列研究的结果表明,年龄是甲状腺癌术后患者唾液腺功能障碍最有效的预测因素[12]。本研究中,唾液腺损伤患者的年龄较唾液腺正常者大且差异有统计学意义,这可能与年龄较大者的唾液腺摄取和分泌功能会相对降低有关[12];也可能与年龄较大患者的免疫力、机体损伤修复能力均较差有关[13]。
许多关于131I治疗DTC患者唾液腺损伤的研究未将131I治疗前TSH水平列为发生唾液腺损伤的影响因素[13-16]。有学者对174 例甲状腺乳头状癌患者在131I 治疗后48 h内是否出现唾液腺损伤进行研究,将患者按131I治疗前TSH水平分为<50 mIU/L、50~75 mIU/L、>75 mIU/L 3组,发现TSH水平对唾液腺损伤没有明显的影响[4]。本研究却发现唾液腺正常患者的TSH水平均值高于唾液腺损伤患者,且二者间的差异有统计学意义。DTC患者未使用甲状腺激素导致血清 TSH 水平升高时,可通过激活钠碘同向转运体刺激唾液腺,因此当患者的甲状腺功能减退(简称甲减)时可能会影响唾液腺的功能[16]。但Riachy等[4]的研究结果与上述结果不同,可能与诊断唾液腺损伤的标准不同、观察出现唾液腺损伤的时间不同、研究人群不同、研究的例数较少等有关。
目前,重组人促甲状腺激素(recombinant human thyroid stimulating hormone,rhTSH)已经在欧洲、美国和巴西被批准用于临床。研究结果表明,rhTSH的使用对于DTC患者131I治疗后发生的唾液腺损伤有一定的改善,可能是由于rhTSH对DTC患者术后的甲减有预防和缓解的作用[17],其可使患者在131I 治疗期间保持甲状腺功能正常,并且降低患者的全身辐射剂量。因此使用rhTSH有望减少唾液腺的辐射暴露,减轻唾液腺损伤的症状[7]。目前我国还未批准使用rhTSH,因此rhTSH是否适合我国DTC术后患者131I治疗后预防唾液腺损伤尚需进一步研究。
国外学者对DTC患者术后131I治疗的危险因素进行了广泛的研究,对于131I 治疗导致唾液腺损伤的独立预测因素目前仍无定论 [18-23]。Riachy等[4]对DTC术后131I治疗患者进行分析,发现收缩压高的DTC患者唾液腺损伤的发生率更高。本研究结果也表明,唾液腺损伤患者的收缩压明显高于唾液腺正常患者。众所周知,甲状腺激素在调节人体心脏、血管及其生理代谢过程中起着重要的作用[5]。DTC患者131I治疗前停用L-T4,使机体处于严重的甲减状态,有研究结果表明,甲减患者的血管径向壁的厚度更大、顺应性更强,可启动低血浆肾素活性机制导致收缩压升高[24-25],但收缩压对DTC患者131I治疗后唾液腺损伤的影响及其具体机制仍有待进一步的研究。
本研究尚存在一定的局限性。(1)本研究为回顾性性研究,DTC患者L-T4停药的具体时间以月为单位记录,未以天为单位进行精准的记录;(2)患者的随访时间有限,本研究主要是对DTC患者131I治疗后1个月的唾液腺功能进行研究,而未进行短期(48 h至1周)和更长时间(数月至数年)的研究;(3)研究的样本量有限,因此本研究的结果可能存在一定的偏倚;(4)未对多次行131I治疗的患者进行随访,故结果仍需进一步探讨。
DTC患者行131I 治疗时出现唾液腺损伤可能与年龄、131I治疗前TSH水平及收缩压相关。在临床实际工作中,需重视唾液腺损伤的相关因素,出现损伤时应及时治疗。
利益冲突 所有作者声明无利益冲突
作者贡献声明 李晓倩负责试验的实施、数据的获取与分析、论文的撰写与最终版本的修订;仝慧敏负责试验的实施;黄楠、岳荣丽、方菊、秦卓琦负责数据的获取、提供与分析;陆克义负责最终版本的修订;程艳负责研究命题的提出、设计、最终版本的修订
分化型甲状腺癌患者131I治疗后唾液腺损伤的相关因素分析
Analysis of related factors to salivary gland injury in patients with differentiated thyroid cancer after 131I treatment
-
摘要:
目的 探讨分化型甲状腺癌(DTC)患者131I 治疗后唾液腺损伤的危险因素。 方法 回顾性分析2019年1月至2022年7月于山西医科大学第一医院行131I治疗的107例DTC患者的临床资料,其中男性35例、女性72例,年龄(42.8±1.0)岁。比较唾液腺损伤患者与唾液腺正常患者年龄、身体质量指数、收缩压、舒张压、原发肿瘤的组织病理学分型及分期、是否有淋巴结转移、是否并发糖尿病、131I治疗前促甲状腺素(TSH)水平、停用左甲状腺素钠片(L-T4)时间、131I治疗剂量、131I全身显像(WBS)等临床资料的差异。符合正态分布的计量资料的组间比较采用单因素方差分析(ANOVA),计数资料的组间比较采用χ2检验,期望频数<5时采用Fisher确切概率法。通过单因素分析和多因素Logistic回归分析明确唾液腺损伤的相关因素。 结果 107例DTC患者中,37例患者发生唾液腺损伤,唾液腺损伤的发生率为34.6%。单因素分析结果显示,唾液腺损伤患者的年龄、收缩压大于唾液腺正常患者[(45.84±2.10)岁 对(41.11±0.97)岁,(127.59±3.10) mm Hg对(119.86±1.84) mm Hg],唾液腺损伤患者131I治疗前TSH水平低于唾液腺正常患者[(99.82±8.46) mIU/L对(122.59±4.03) mIU/L],且差异有统计学意义(F=5.457、5.210、6.288,均P<0.05)。多因素Logistic回归分析结果显示,年龄、131I治疗前TSH水平、收缩压是唾液腺功能损伤的非独立危险因素(OR=1.017、0.989、1.023,均P>0.05)。 结论 年龄较大、131I治疗前TSH水平较低及收缩压较高是DTC患者行131I 治疗出现唾液腺损伤的相关因素。 Abstract:Objective To investigate the risk factors of salivary gland injury in patients with differentiated thyroid cancer (DTC) after 131I treatment. Methods The clinical data of 107 patients with DTC who received 131I treatment in the First Hospital of Shanxi Medical University from January 2019 to July 2022 were retrospectively analyzed. The patients included 35 males and 72 females, aged (42.8±1.0) years. The age, body mass index, systolic blood pressure, diastolic blood pressure, histopathological classification and stage of the primary tumor, lymph node metastasis, diabetes, thyroid stimulating hormone (TSH) level before 131I treatment, levothyroxine sodium discontinuation (L-T4) time, 131I treatment dose, 131I whole-body imaging, and other clinical data were compared between patients with salivary gland injury and those with normal salivary gland. Univariate analysis of variance was used to compare the measurement data conforming to normal distribution, and χ2 test was used to compare count data. Fisher's exact probability method was used when the expected frequency is less than 5. Univariate regression analyses and multivariate Logistic regression analyses were conducted to identify factors related to salivary gland injury. Results Among 107 DTC patients, 37 cases had salivary gland injury with an incidence of 34.6%. Univariate regression analysis showed that age and systolic blood pressure of patients with salivary gland injury were higher than those of patients with normal salivary gland ((45.84±2.10) years vs. (41.11±0.97) years, (127.59±3.10) mm Hg vs. (119.86±1.84) mm Hg); the TSH level before 131I treatment of patients with salivary gland injury was lower than that of patients with normal salivary gland ((99.82±8.46) mIU/L vs. (122.59±4.03) mIU/L), and the differences were statistically significant (F=5.457, 5.210, 6.288; all P<0.05). Multivariate Logistic regression analysis showed that age, TSH level before 131I treatment, and systolic blood pressure were independent risk factors for salivary gland injury (OR=1.017, 0.989, 1.023; all P>0.05). Conclusion Old age, low TSH level before 131I treatment, and high systolic blood pressure are related factors to salivary gland injury in patients with DTC after 131I treatment. -
Key words:
- Thyroid neoplasms /
- Iodion radioisotopes /
- Sialadenitis /
- Risk factors
-
图 1 接受131I治疗的分化型甲状腺癌患者正常唾液腺(A)和损伤唾液腺(B)感兴趣区勾画的示意图
Figure 1. Schematic diagram of the region of interest outlined of normal salivary glands (A) and injury salivary glands (B) in patients with differentiated thyroid cancer after 131I treatment
图 2 接受131I治疗的分化型甲状腺癌患者(女性,48岁)的正常唾液腺动态显像图
Figure 2. Dynamic imaging of normal salivary glands in a patient with differentiated thyroid cancer (female, 48 years old) after 131I treatment
图 3 接受131I治疗的分化型甲状腺癌患者(女性,27岁)的损伤唾液腺动态显像图
Figure 3. Dynamic imaging of injured salivary glands in a patient with differentiated thyroid cancer (female, 27 years old) after 131I treatment
表 1 107例分化型甲状腺癌患者131I治疗后影响唾液腺功能损伤的单因素分析
Table 1. Univariate analysis of factors affecting salivary gland function injury in 107 patients with differentiated thyroid cancer after 131I treatment
因素 唾液腺损伤(n=37) 唾液腺正常(n=70) 检验值 P值 年龄(岁, $\bar x \pm s $ 45.84±2.10 41.11±0.97 F=5.457 0.046 BMI( $\bar x \pm s $ 22.02±1.35 24.71±0.43 F=5.556 0.064 收缩压(mm Hg, $\bar x \pm s $ 127.59±3.10 119.86±1.84 F=5.210 0.024 舒张压(mm Hg, $\bar x \pm s $ 83.06±1.82 82.01±1.24 F=0.231 0.632 糖尿病(例,%) − 0.657 有 1(2.7) 4(5.7) 无 36(97.3) 66(94.3) 组织病理学分型 − 1.000 乳头状癌 37(100) 70(100) 肿瘤分期 χ2=0.830 0.362 Ⅰ期 27(73.0) 45(64.3) Ⅱ期 10(27.0) 25(35.7) 淋巴结转移(例,%) − 0.769 有 29(78.4) 61(87.1) 无 8(21.6) 9(12.9) 131I治疗剂量(例,%) − 0.568 <3.7 GBq 0(0) 1(1.4) 3.7~5.6 GBq 34(91.9) 67(95.7) >5.6 GBq 3(8.1) 2(2.9) 131I治疗前TSH水平(mIU/L, $\bar x \pm s $ 99.82±8.46 122.59±4.03 F=6.288 0.019 L-T4服用情况(例,%) χ2=1.613 0.204 停用1个月 18(48.6) 43(61.4) 未服用 19(51.4) 27(38.6) 术后月数(月, $\bar x \pm s $ 1.94±0.18 2.25±0.21 F=0.899 0.345 131I WBS结果 − 0.543 阴性 0(0) 2(2.9) 阳性 37(100) 68(97.1) 注:−表示使用Fisher确切概率法,无检验值。BMI为身体质量指数;TSH为促甲状腺激素;L-T4为左甲状腺素钠片;WBS为全身扫描  下载: 导出CSV
下载: 导出CSV
表 2 分化型甲状腺癌患者131I治疗后影响唾液腺功能损伤的多因素Logistic 回归分析
Table 2. Multivariate Logistic regression analysis of factors affecting salivary gland function injury in patients with differentiated thyroid cancer after 131I treatment
因素 B值 Wald值 OR值 95%CI P值 年龄 0.017 0.443 1.017 0.968~1.068 0.506 131I治疗前TSH水平 −0.011 3.771 0.989 0.979~1.000 0.052 收缩压 0.023 2.592 1.023 0.995~1.051 0.107 注:TSH为促甲状腺激素;OR为比值比;CI为置信区间
下载: 导出CSV
-
[1] Krcalova E, Horacek J, Gabalec F, et al. Salivary gland function in thyroid cancer patients with radioiodine administration history[J]. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub, 2020, 164(3): 277−283. DOI: 10.5507/bp.2019.023. [2] Badam RK, Suram J, Babu DB, et al. Assessment of salivary gland function using salivary scintigraphy in pre and post radioactive iodine therapy in diagnosed thyroid carcinoma patients[J]. J Clin Diagn Res, 2016, 10(1): ZC60−ZC62. DOI: 10.7860/JCDR/2016/16091.7121. [3] Lee HN, An JY, Lee KM, et al. Salivary gland dysfunction after radioactive iodine (I-131) therapy in patients following total thyroidectomy: emphasis on radioactive iodine therapy dose[J]. Clin Imaging, 2015, 39(3): 396−400. DOI: 10.1016/j.clinimag.2014.12.018. [4] Riachy R, Ghazal N, Haidar MB, et al. Early sialadenitis after radioactive iodine therapy for differentiated thyroid cancer: prevalence and predictors[J]. Int J Endocrinol, 2020, 2020: 8649794. DOI: 10.1155/2020/8649794. [5] 梁昌平, 徐颖, 何涛. 131I治疗前不同撤药时间对分化型甲状腺癌患者甲状腺激素、血脂、心血管相关因素的影响及其临床分析[J]. 标记免疫分析与临床, 2022, 29(3): 408−412,437. DOI: 10.11748/bjmy.issn.1006-1703.2022.03.011.
Liang CP, Xu Y, He T. Effects of different withdrawal time points before 131I treatment on thyroid hormones, blood lipids and cardiovascular related factors in patients with differentiated thyroid carcinoma and its clinical analysis[J]. Labeled Immunoassays Clin Med, 2022, 29(3): 408−412,437. DOI: 10.11748/bjmy.issn.1006-1703.2022.03.011.[6] Hollingsworth B, Senter L, Zhang XL, et al. Risk factors of 131I-induced salivary gland damage in thyroid cancer patients[J]. J Clin Endocrinol Metab, 2016, 101(11): 4085−4093. DOI: 10.1210/jc.2016-1605. [7] Iakovou I, Goulis DG, Tsinaslanidou Z, et al. Effect of recombinant human thyroid-stimulating hormone or levothyroxine withdrawal on salivary gland dysfunction after radioactive iodine administration for thyroid remnant ablation[J]. Head Neck, 2016, 38(S1): SE227−E230. DOI: 10.1002/hed.23974. [8] Lee SM, Lee JW, Kim SY, et al. Prediction of risk for symptomatic sialadenitis by post-therapeutic dual 131I scintigraphy in patients with differentiated thyroid cancer[J]. Ann Nucl Med, 2013, 27(8): 700−709. DOI: 10.1007/s12149-013-0735-3. [9] 刘岩, 杨爱民, 欧阳雁, 等. 放射性核素唾液腺显像及抗核抗体联合检查在干燥综合征中的诊断价值[J]. 国际放射医学核医学杂志, 2014, 38(4): 219−222. DOI: 10.3760/cma.j.issn.1673-4114.2014.04.003.
Liu Y, Yang AM, Ouyang Y, et al. The diagnostic value of joint inspection of radionuclide salivary gland scintigraphy and antinuclear antibody examination in Sjögren's syndrome patients[J]. Int J Radiation Med Nucl Med, 2014, 38(4): 219−222. DOI: 10.3760/cma.j.issn.1673-4114.2014.04.003.[10] Byeon HK, Jeong GC, Kim B, et al. Clinical utility of quantitative parameters of salivary gland scintigraphy for diagnosing burning mouth syndrome[J/OL]. Diagnostics (Basel), 2022, 12(9): 2256[2022-10-10]. https://www.mdpi.com/2075-4418/12/9/2256. DOI: 10.3390/diagnostics12092256. [11] Upadhyaya A, Zhou PP, Meng ZW, et al. Radioprotective effect of vitamin E on salivary glands after radioiodine therapy for differentiated thyroid cancer: a randomized-controlled trial[J]. Nucl Med Commun, 2017, 38(11): 891−903. DOI: 10.1097/MNM.0000000000000727. [12] Almeida JP, Sanabria ÁE, Lima ENP, et al. Late side effects of radioactive iodine on salivary gland function in patients with thyroid cancer[J]. Head Neck, 2011, 33(5): 686−690. DOI: 10.1002/hed.21520. [13] 杨静, 郑容. 131I治疗分化型甲状腺癌肺转移患者的疗效及其影响因素[J]. 中国医学影像技术, 2016, 32(10): 1624−1627. DOI: 10.13929/j.1003-3289.2016.10.038.
Yang J, Zheng R. Curative effect and influencing factors of 131I in treatment of differentiated thyroid cancer patients with pulmonary metastases[J]. Chin Med Imaging Technol, 2016, 32(10): 1624−1627. DOI: 10.13929/j.1003-3289.2016.10.038.[14] Adramerinas M, Andreadis D, Vahtsevanos K, et al. Sialadenitis as a complication of radioiodine therapy in patients with thyroid cancer: where do we stand?[J]. Hormones (Athens), 2021, 20(4): 669−678. DOI: 10.1007/s42000-021-00304-3. [15] Dehbi HM, Mallick U, Wadsley J, et al. Recurrence after low-dose radioiodine ablation and recombinant human thyroid-stimulating hormone for differentiated thyroid cancer (HiLo): long-term results of an open-label, non-inferiority randomised controlled trial[J]. Lancet Diabetes Endocrinol, 2019, 7(1): 44−51. DOI: 10.1016/S2213-8587(18)30306-1. [16] Dong P, Qu Y, Yang L, et al. Outcomes after radioiodine ablation in patients with thyroid cancer: long-term follow-up of a Chinese randomized clinicaltrial[J]. Clin Endocrinol (Oxf), 2021, 95(5): 782−789. DOI: 10.1111/cen.14563. [17] Rosário PW, Borges MAR, Purisch S. Preparation with recombinant human thyroid-stimulating hormone for thyroid remnant ablation with 131I is associated with lowered radiotoxicity[J]. J Nucl Med, 2008, 49(11): 1776−1782. DOI: 10.2967/jnumed.108.050591. [18] Shen FC, Hsieh CJ, Huang IC, et al. Dynamic risk estimates of outcome in Chinese patients with well-differentiated thyroid cancer after total thyroidectomy and radioactive iodine remnant ablation[J]. Thyroid, 2017, 27(4): 531−536. DOI: 10.1089/thy.2016.0479. [19] Ahn J, Jin MH, Song EY, et al. Clinical outcomes after early and delayed radioiodine remnant ablation in patients with low-risk papillary thyroid carcinoma: propensity score matching analysis[J]. Endocrinol Metab (Seoul), 2020, 35(4): 830−837. DOI: 10.3803/EnM.2020.747. [20] Cheng F, Xiao J, Huang FY, et al. Delay of initial radioactive iodine therapy beyond 3 months has no effect on clinical responses and overall survival in patients with thyroid carcinoma: a cohort study and a meta-analysis[J/OL]. Cancer Med, 2022, 11(12): 2386−2396[2022-10-10]. https://onlinelibrary.wiley.com/doi/10.1002/cam4.4607. DOI: 10.1002/cam4.4607. [21] Li H, Zhang YQ, Wang C, et al. Delayed initial radioiodine therapy related to incomplete response in low- to intermediate-risk differentiated thyroid cancer[J]. Clin Endocrinol (Oxf), 2018, 88(4): 601−606. DOI: 10.1111/cen.13551. [22] 王鑫, 宋清斌, 徐冬冬, 等. 术后首次放射性碘治疗时机的选择对分化型甲状腺癌早期疗效的影响[J]. 中国医科大学学报, 2019, 48(4): 359−362, 369. DOI: 10.12007/j.issn.0258-4646.2019.04.016.
Wang X, Song QB, Xu DD, et al. Effects of timing of initial postoperative radioactive iodine therapy on the outcome of patients with differentiated thyroid cancer[J]. J China Med Univ, 2019, 48(4): 359−362, 369. DOI: 10.12007/j.issn.0258-4646.2019.04.016.[23] 仝慧敏, 杨素云, 程艳. 131I致分化型甲状腺癌患者唾液腺辐射损伤及其防治的研究进展[J]. 国际放射医学核医学杂志, 2022, 46(7): 425−429. DOI: 10.3760/cma.j.cn121381-202111007-00198.
Tong HM, Yang SY, Cheng Y. Research progress on radiation injury of salivary gland and its prevention and treatment in patients with differentiated thyroid cancer induced by 131I[J]. Int J Radiat Med Nucl Med, 2022, 46(7): 425−429. DOI: 10.3760/cma.j.cn121381-202111007-00198.[24] Giontella A, Lotta LA, Overton JD, et al. Association of thyroid function with blood pressure and cardiovascular disease: a mendelian randomization[J/OL]. J Pers Med, 2021, 11(12): 1306[2022-10-10]. https://www.mdpi.com/2075-4426/11/12/1306. DOI: 10.3390/jpm11121306. [25] Goswami B, Bhattacharjya H, Sengupta S, et al. Hypovitaminosis D, dyslipidemia, and thyroid dysfunction among adolescents and their associations with blood pressure in a northeastern city of India[J]. Indian J Community Med, 2021, 46(3): 484−488. DOI: 10.4103/ijcm.IJCM_907_20. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 2225
- HTML全文浏览量: 1686
- PDF下载量: 15
