


-
瘢痕疙瘩是一种由于皮肤组织过度增生形成的疤痕组织,常常由皮肤损伤或刺激引起。病理性瘢痕组织通常由网状真皮的损伤及其随后的异常愈合引起,其组织病理学特征为持续的局部组织炎症[1],包括新生成的炎症细胞和成纤维细胞以及新形成的血管和胶原蛋白沉积物[2]。瘢痕疙瘩可在皮肤损伤后的几个月至几年内出现,且无限期地增长,没有消退的迹象。因此,瘢痕疙瘩虽然是一种良性皮肤纤维化疾病,但具有与恶性肿瘤相似的特征[3],常给患者带来身体上的痛苦。瘢痕疙瘩和增生性瘢痕在青少年和青年人群中发生的概率更高,可影响患者的生活质量[4]。
瘢痕疙瘩可通过手术切除进行治疗,但手术又会有导致新的瘢痕形成的可能。因此,瘢痕疙瘩的治疗比较困难,手术治疗的复发风险较高,有研究结果显示,大部分手术切除的瘢痕疙瘩会复发[5]。用于治疗瘢痕疙瘩的方法较多,包括硅胶片或硅胶凝胶,压迫疗法,物理疗法,皮下注射皮质类固醇、5-氟尿嘧啶注射液,冷冻疗法,放疗等。这些治疗方法可以单独使用,也可以联合使用[4]。
与手术相比,放疗在降低瘢痕疙瘩的复发率方面有着明显的优势[6];与冷冻治疗相比,放疗的效果更好[7]。一项荟萃分析的结果显示,单纯行放疗治疗瘢痕疙瘩的复发率仅为37%,手术联合放疗的复发率为22%,放疗中近距离放疗的复发率最低[8]。90Sr-90Y敷贴治疗是目前最常用的一种通过近距离放疗治疗瘢痕疙瘩的方法,其通过发射β射线发挥治疗作用。90Sr-90Y敷贴治疗的照射总剂量约为20 Gy,分10次完成,总缓解率接近90%[9]。相较于注射皮质类固醇等药物会使患者发生明显疼痛等并发症,90Sr-90Y敷贴治疗的全身不良反应较小,同时可以有效降低治疗后的复发率[10]。瘢痕疙瘩90Sr-90Y敷贴治疗的主要不良反应为瘢痕疙瘩周围正常皮肤发生放射性皮炎,这种放射性皮炎是影响患者接受足量、足疗程治疗的常见原因。
因此,本研究尝试将硅胶片用于90Sr-90Y敷贴治疗保护瘢痕疙瘩周围的正常皮肤组织,以观察其预防瘢痕疙瘩周围正常皮肤出现放射性皮炎的效果。我们测试了不同厚度硅胶片的保护效果,以期发现最合适的硅胶片。
-
回顾性分析2019年1月至2021年6月于上海交通大学附属第六人民医接受90Sr-90Y敷贴治疗瘢痕疙瘩的175例患者的临床资料,其中男性81 例、女性94 例,年龄(27.2±3.7)岁。纳入标准:90Sr-90Y敷贴治疗疗程≤2个月。排除标准:(1)患有糖尿病或免疫系统疾病;(2)治疗部位有皮肤感染或破损。所有患者均在治疗前签署了知情同意书。本研究符合《赫尔辛基宣言》的原则。
-
使用中国原子能科学研究院生产的方形90Sr-90Y敷贴器(2.274 MeV)对患者的瘢痕疙瘩进行敷贴治疗,敷贴范围为2 cm×2 cm。治疗时将90Sr-90Y敷贴器放平紧贴于瘢痕疙瘩病灶表面,如病灶范围超出90Sr-90Y敷贴器大小则需分野敷贴照射。采用多次小剂量法进行敷贴治疗,每次的治疗剂量为8~10 Gy,每次4~6 min,每周2~3次。每个疗程的总剂量为20~40 Gy,如未治愈,间隔1~2个月可行下个疗程治疗,一般治疗总疗程为2~3个疗程,不超过4个疗程。
-
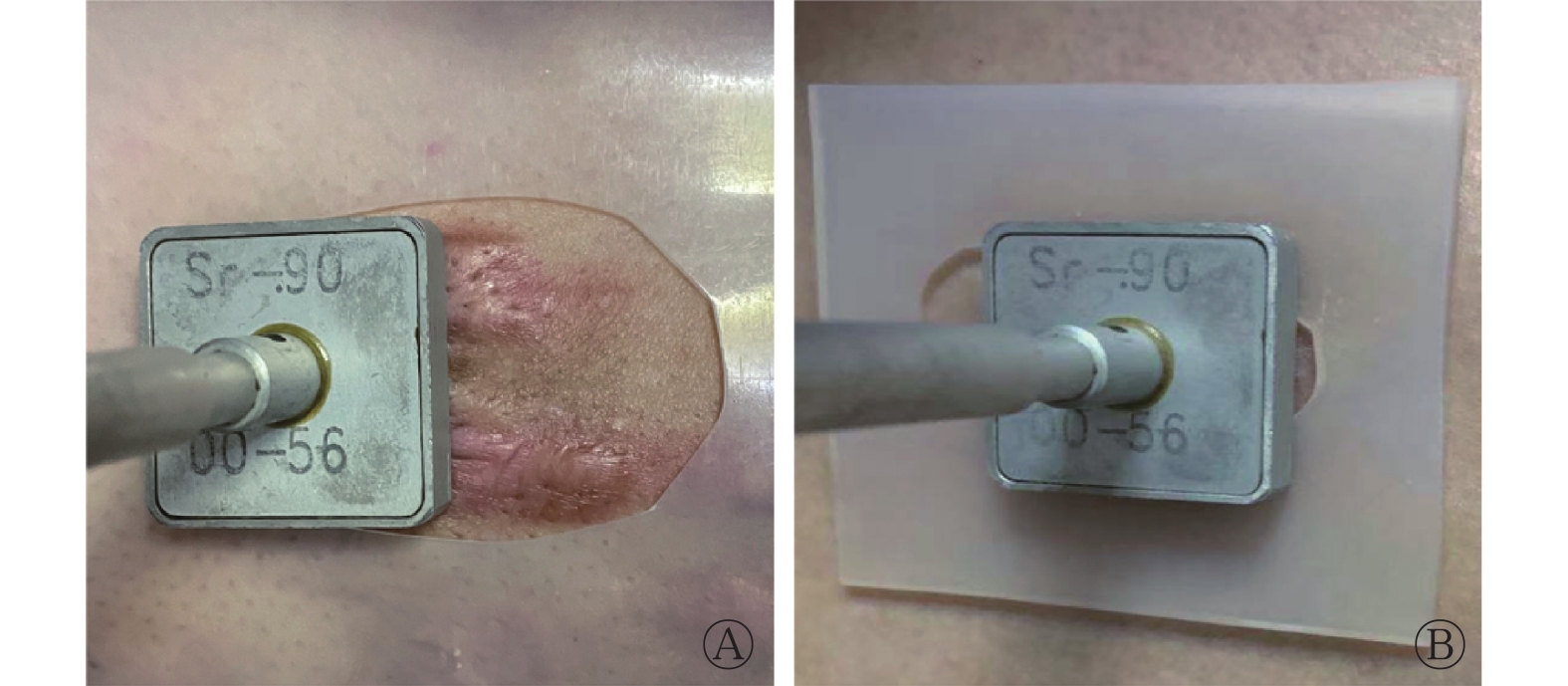
根据瘢痕疙瘩的面积及形状适形剪裁(四周略大于瘢痕疙瘩0.2 cm)1 mm厚硅胶片及2 mm厚硅胶片,对正常皮肤进行保护(图1)。采用信封随机分组法将患者分为对照组(57例)、1 mm厚硅胶片保护组(55例)、2 mm厚硅胶片保护组(63例)。

图 1 90Sr-90Y敷贴治疗瘢痕疙瘩患者中硅胶片保护方法示意图
Figure 1. Schematic diagram of 90Sr-90Y applicator for the protection of silicone in the treatment of patients with keloids
-
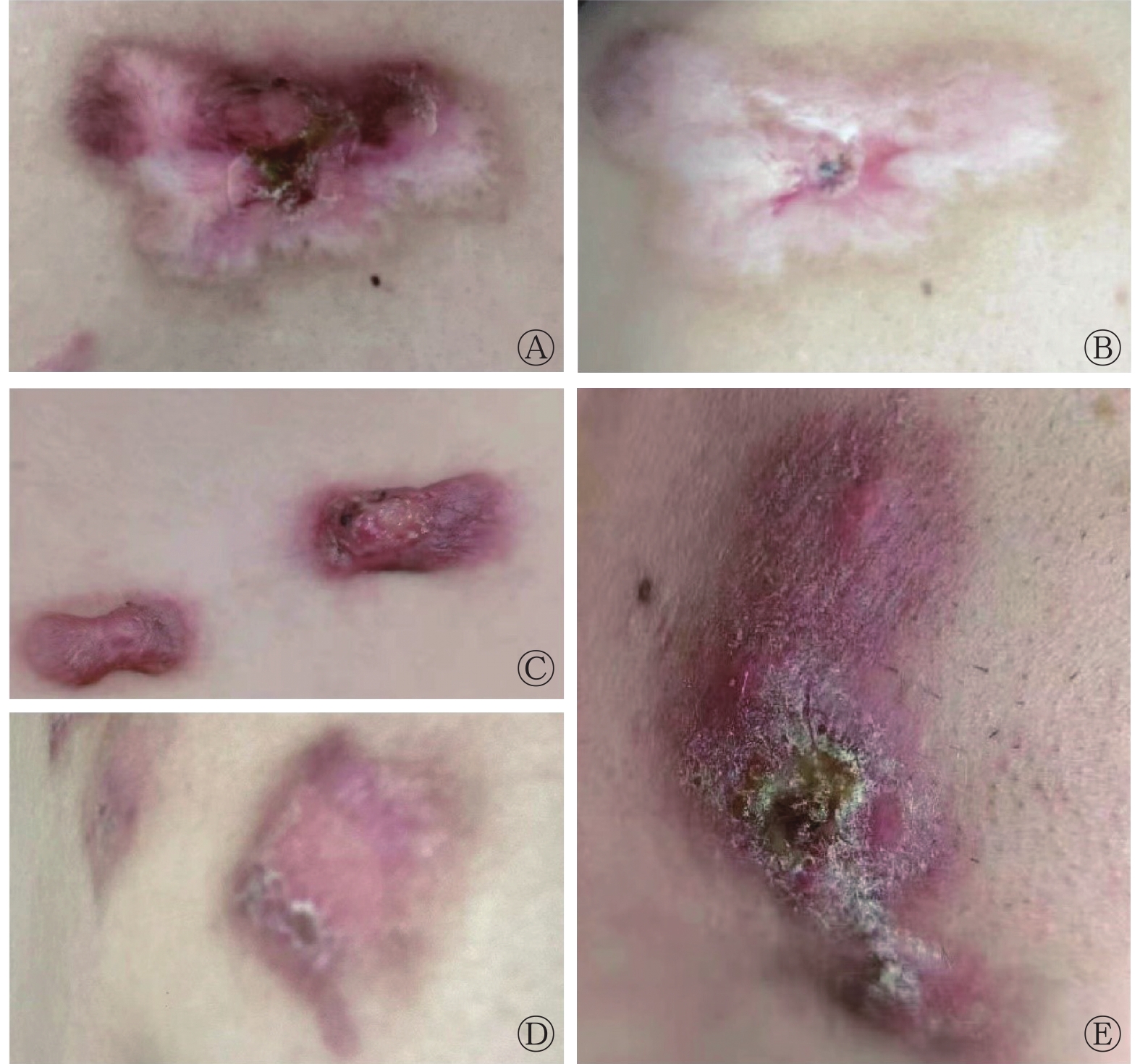
满足以下条件即为治疗有效:90Sr-90Y敷贴治疗后,瘢痕疙瘩的面积比治疗前缩小50%以上,剩余瘢痕组织变平,瘢痕厚度较治疗前变薄(图2A、2B)。

图 2 90Sr-90Y敷贴治疗瘢痕疙瘩患者的效果及放射性皮炎的分级图
Figure 2. The effect of 90Sr-90Y applicator in the treatment of patients with keloids and the grading chart of radi dermatitis
-
急性放射性皮炎一般发生于瘢痕疙瘩患者接受放疗后的2个月内,因此,我们从治疗开始观察2个月内患者急性放射性皮炎的发生情况,按美国肿瘤放疗学会的放射性皮炎分级标准[11],将放射性皮炎分为5级(即总体放射性皮炎等级)。Ⅰ级:水疱性皮损、淡红斑或暗红斑,脱发,干性脱屑,少汗(图2C);Ⅱ级:触痛性红斑或鲜红斑,片状湿性脱屑,局部皮肤中度水肿(图2D);Ⅲ级:皮肤褶皱部位以外融合性湿性脱屑,凹陷性水肿(图2E);Ⅳ级:皮肤溃疡,出血,坏死;Ⅴ级:死亡。将放射性皮炎≥Ⅱ级定义为严重放射性皮炎。排除未发生放射性皮炎的患者,只考虑各组发生放射性皮炎患者的皮炎等级为相对放射性皮炎等级。按相对放射性皮炎的严重等级赋值:未发生放射性皮炎=0,Ⅰ级=1,Ⅱ级=2,Ⅲ级=3,计算各组患者的相对放射性皮炎等级。
-
应用SPSS 25.0软件对数据进行统计学分析。符合正态分布的计量资料以
$ \bar x\pm s $ 表示,计数资料以例和百分比表示。计量资料的2组间比较采用独立样本t检验(方差齐),3组间比较采用单因素方差分析;计数资料的组间比较采用卡方检验;采用单因素Logistics回归分析对影响疗效的因素进行分析。P<0.05为差异有统计学意义。 -
对照组患者57例,年龄(27.8±3.3)岁,其中男性28例(49.1%)、女性29例(50.9%),病程(1.77±0.71)年。1 mm厚硅胶片保护组患者55例,年龄(26.8±3.8)岁,其中男性24例(43.6%)、女性 31例(56.4%),病程(1.83±0.72)年。2 mm厚硅胶片保护组患者63例,年龄(27.2±3.9)岁,其中男性29例(46.0%)、女性 34例(54.0%),病程(1.68±0.62)年。3组患者年龄、性别、病程的差异均无统计学意义(均P>0.05)(表1)。
项目 对照组
(n=57)1 mm 厚硅胶片保护组
(n=55)2 mm厚硅胶片保护组
(n=63)检验值 P值 年龄(岁, $ \bar x\pm s $ 

27.8±3.3 26.8±3.8 27.2±3.9 F=1.047 0.353 性别(男/女) 28/29 24/31 29/34 χ2=0.341 0.843 病程(年, $ \bar x\pm s $ 

1.77±0.71 1.83±0.72 1.68±0.62 F=0.767 0.466 疗程数(个, $ \bar x\pm s $ 

2.26±0.97 2.35±1.00 2.40±1.06 F=0.263 0.769 治疗有效率[例(%)] 54(94.7) 51(92.7) 60(95.2) χ2=0.474 0.848 放射性皮炎发生率[例(%)] 51(89.5) 46(83.6) 34(54.0)ab χ2=23.328 <0.001 总体放射性皮炎等级( $ \bar x\pm s $ 

1.37±0.75 1.05±0.65a 0.63±0.66ab F=17.361 <0.001 相对放射性皮炎等级( $ \bar x\pm s $ 

1.53±0.61 1.26±0.49a 1.18±0.39a F=5.613 0.005 注:a表示与对照组比较,差异均有统计学意义(χ2=18.108,t=−2.409、−2.577、−5.749、−3.780;均P<0.05);b表示与1 mm厚硅胶片保护组比较,差异均有统计学意义(χ2=11.738,t=−3.473;均P<0.05) 表 1 不同厚度硅胶片保护的90Sr-90Y敷贴治疗175例瘢痕疙瘩患者的临床资料、放射性皮炎发生率和严重程度的比较
Table 1. Comparison of clinical data and incidence and severity of radi dermatitis in 175 patients with keloid treated with 90Sr-90Y applicator with different silicone protective thicknesses
-
对照组治疗(2.26±0.97)个疗程,治疗有效率为94.7%(54/57);51例(89.5%)患者发生放射性皮炎,其中Ⅰ级放射性皮炎27例、Ⅱ级21例、Ⅲ级3例。1 mm厚硅胶片保护组治疗(2.35±1.00)个疗程,治疗有效率为92.7%(51/55);46例(83.6%)患者发生放射性皮炎,其中Ⅰ级放射性皮炎35例、Ⅱ级10例、Ⅲ级1例。2 mm厚硅胶片保护组治疗(2.40±1.06)个疗程,治疗有效率为95.2%(60/63);34例(54.0%)患者发生放射性皮炎,其中Ⅰ级放射性皮炎28例、Ⅱ级6例。对照组与1 mm厚硅胶片保护组放射性皮炎发生率间的差异无统计学意义(P>0.05)。与对照组和1 mm厚硅胶片保护组相比,2 mm厚硅胶片保护组的放射性皮炎的发生率明显降低,且差异均有统计学意义(均P<0.05)(表1)。
-
对照组、1 mm厚硅胶片保护组、2 mm厚硅胶片保护组患者的总体放射性皮炎等级的差异有统计学意义(P<0.001)。1 mm厚硅胶片保护组的总体放射性皮炎等级低于对照组,且差异有统计学意义(P<0.05);2 mm厚硅胶片保护组的总体放射性皮炎等级低于对照组和1 mm厚硅胶片保护组,且差异均有统计学意义(均P<0.05)。对照组、1 mm厚硅胶片保护组、2 mm厚硅胶片保护组患者的相对放射性皮炎等级的差异有统计学意义(P<0.01),1 mm厚硅胶片和2 mm厚硅胶片保护组患者的相对放射性皮炎等级均低于对照组,且差异均有统计学意义(均P<0.05),但1 mm厚硅胶片和2 mm厚硅胶片保护组间相对放射性皮炎等级的差异无统计学意义(P>0.05)(表1)。
-
175例患者中,41例(23.4%)出现严重放射性皮炎。考虑到90Sr-90Y敷贴治疗的疗程长短与患者单位皮肤面积接受敷贴照射的总剂量有关,而硅胶片能够降低放射性皮炎的发生率,因此将疗程及硅胶片保护作为自变量,发生严重放射性皮炎作为因变量,进行单因素Logistics回归分析。结果显示,90Sr-90Y敷贴治疗疗程的增加可增加严重放射性皮炎发生的风险(OR=2.348,95%CI:1.524~3.618,P<0.001),不同厚度硅胶片保护均能降低严重放射性皮炎的发生风险(1 mm厚硅胶片:OR=0.273,95%CI为0.109~0.685,P<0.01;2 mm厚硅胶片:OR=0.099,95%CI为0.034~0.293,P<0.001)(表2)。
因素 B值 标准误差 Wald值 OR值 95%CI P值 1 mm厚硅胶片 −1.298 0.469 7.663 0.273 0.109~0.685 0.006 2 mm厚硅胶片 −2.309 0.552 17.491 0.099 0.034~0.293 <0.001 疗程 0.854 0.221 14.967 2.348 1.524~3.618 <0.001 常量 −2.296 0.596 14.855 0.101 − <0.001 注:−表示无此项数据。OR为比值比;CI为置信区间 表 2 90Sr-90Y敷贴治疗疗程及硅胶片保护对瘢痕疙瘩患者 发生严重放射性皮炎影响的单因素Logistics回归分析
Table 2. Univariate Logistic regression analysis of the effect of 90Sr-90Y applicator treatment sessions and silicone protection on the occurrence of severe radiodermatitis in patients with keloids
-
瘢痕疙瘩对治疗的抵抗性强,治疗后的复发率高[12]。放疗对瘢痕疙瘩有较好的治疗效果,其创伤较小,复发率低,是一种较为理想的无创治疗瘢痕疙瘩的方法[6,10]。90Sr-90Y敷贴治疗是临床上常用的治疗瘢痕疙瘩的方法[10],其能够降低成纤维细胞活性,诱导细胞凋亡,因此治疗后的复发率较低。90Sr-90Y敷贴器发射的β射线随距离增加衰减较快,对皮肤下深层组织的损伤较小。但90Sr-90Y敷贴对瘢痕疙瘩周围的正常皮肤仍存在一定的损伤,临床上主要表现为放射性皮炎。目前,相关的研究大多聚焦于90Sr-90Y敷贴治疗的剂量、照射时间和照射次数,但这并不能完全避免周围正常皮肤放射性皮炎的发生。本研究结果显示,使用硅胶片对瘢痕疙瘩周围的正常皮肤进行保护,具有较好的效果。
放射性皮炎是90Sr-90Y敷贴治疗瘢痕疙瘩中常见的并发症。本研究结果表明,在无保护措施的90Sr-90Y敷贴治疗中,尽管使用了小剂量、多次治疗的方案,但放射性皮炎的发生率仍达到89.5%。在使用1 mm厚硅胶片进行保护的患者中,放射性皮炎的发生率为83.6%。在使用2 mm厚硅胶片保护的患者中,放射性皮炎的发生率为54.0%,因此使用2 mm厚硅胶片可以显著降低放射性皮炎的发生率。
本研究结果还显示,采用硅胶片保护还能够降低放射性皮炎的严重程度。虽然使用1 mm厚硅胶片保护的患者放射性皮炎的发生率与对照组患者接近,但其放射性皮炎的严重程度明显下降。使用2 mm厚硅胶片保护的患者放射性皮炎的严重程度较使用1 mm厚硅胶片保护的患者进一步下降。排除3组中未发生放射性皮炎的患者,仅观察发生放射性皮炎的患者的严重等级(相对放射性皮炎等级)时发现,即使出现了放射性皮炎,使用1 mm厚硅胶片保护患者的放射性皮炎的严重程度也明显低于对照组患者,与2 mm厚硅胶片保护的患者相似。国外的相关研究主要关注硅胶制剂在瘢痕疙瘩治疗中的作用[13-15]。在动物实验中,硅胶敷料已经被证实可以降低放射性皮炎的严重程度,这可能与硅胶制剂可抑制皮肤组织中某些细胞因子(如干扰素-γ、白细胞介素-1β、白细胞介素-2 和TNF-α等)的产生有关[16],效果优于氧化锌涂剂。在本研究之前,鲜见使用硅胶制品预防放射性皮炎的研究。本研究结果表明,硅胶片对于放射性皮炎有较好的防护效果。
硅胶片本身较为柔软且无需粘贴于皮肤,使用中及使用后不会使患者的皮肤产生不适。瘢痕疙瘩常高于正常皮肤表面,但硅胶片较薄,因此使用硅胶片对瘢痕疙瘩周围的正常皮肤进行保护不会明显增加放射源与瘢痕疙瘩的距离。本研究中,我们发现对照组与使用1 mm和2 mm厚硅胶片对正常皮肤进行保护的患者90Sr-90Y敷贴治疗的有效率和平均疗程的差异均无统计学意义。因此,使用硅胶片保护正常皮肤不会降低90Sr-90Y敷贴治疗对瘢痕疙瘩治疗的有效性,亦不会延长患者的治疗时间,显示出了较好的安全性。
如果发生轻微的放射性皮炎,通常仅需观察或对症治疗即可[17],而严重的放射性皮炎则常会增加患者的痛苦,甚至使患者无法继续治疗,从而导致治疗效果欠佳或治疗失败。本研究结果显示,严重的放射性皮炎与患者接受90Sr-90Y敷贴治疗的疗程长短和使用硅胶片保护有关,90Sr-90Y敷贴治疗疗程的增加会增加等级较高的放射性皮炎的发生风险。使用硅胶片保护能够降低等级较高的放射性皮炎的发生风险,2 mm厚硅胶片较1 mm厚硅胶片可更好地降低等级较高的放射性皮炎的发生风险。90Sr-90Y发射的β射线在皮肤中的穿透距离为2 mm,且对皮肤组织的影响随距离的增加而衰减。硅胶片的密度为1.02 g/cm3,与人体皮肤的密度相同,故可以起到很好的防护作用。
综上所述,在对瘢痕疙瘩患者行90Sr-90Y敷贴治疗时,使用2 mm厚硅胶片保护周围正常皮肤组织能够明显降低放射性皮炎的发生率和严重程度,有一定的临床价值。本研究也存在着一定的局限性,由于只纳入了疗程≤2个月的患者,因此硅胶片防护对于疗程长、大剂量的放疗导致的放射性皮炎的防护效果无法确定;此外,由于随访时间的限制,硅胶片对于慢性放射性皮炎是否具有防护效果也无法确定,需在后续的研究随访中继续观察。
利益冲突 所有作者声明无利益冲突
作者贡献声明 陈越虹负责论文的撰写与修改;陆勤、黄忆云负责数据的整理与分析;罗全勇负责病例的收集与技术支持;沈晨天负责方法的建立、论文的审阅
硅胶片对90Sr-90Y敷贴治疗瘢痕疙瘩中放射性皮炎预防作用的研究
Study on the prophylactic effect of silicone on radiodermatitis in keloid treated with 90Sr-90Y applicator
-
摘要:
目的 研究90Sr-90Y敷贴治疗瘢痕疙瘩中硅胶片对放射性皮炎的预防作用。 方法 回顾性分析2019年1月至2021年6月于上海交通大学附属第六人民医接受90Sr-90Y敷贴治疗的175例瘢痕疙瘩患者的临床资料,其中男性 81例、女性94例,年龄(27.2±3.7)岁。采用信封随机分组法将患者分为对照组(57例)、1 mm厚硅胶片保护组(55例)、2 mm厚硅胶片保护组(63例)。所有患者均使用90Sr-90Y敷贴器进行多次小剂量治疗,1 mm厚硅胶片保护组患者和2 mm厚硅胶片保护组患者分别使用1 mm、2 mm厚硅胶片对病灶周围皮肤进行保护。采用美国肿瘤放疗学会的放射性皮炎分级标准对3组患者的放射性皮炎进行分级,比较各组患者放射性皮炎的发生率及严重等级。分析90Sr-90Y敷贴治疗疗程及硅胶片保护对发生严重放射性皮炎的影响。符合正态分布的计量资料的2组间比较采用独立样本t检验(方差齐),3组间的比较采用单因素方差分析;计数资料的组间比较采用卡方检验;采用单因素Logistics回归分析对影响疗效的因素进行分析。 结果 1 mm厚硅胶片保护组和对照组患者放射性皮炎发生率(83.6%对89.5%)间的差异无统计学意义(χ2=0.815,P>0.05);与对照组和1 mm厚硅胶片保护组相比,2 mm厚硅胶片保护组的放射性皮炎的发生率显著降低(89.5% 对83.6% 对 54.0%),且差异均有统计学意义(χ2=18.108、11.738,均P<0.05)。1 mm厚硅胶片保护组患者总体放射性皮炎的严重等级低于对照组(1.05±0.65 对 1.37±0.75),且差异有统计学意义(t=−2.409,P<0.05),2 mm厚硅胶片保护组患者放射性皮炎的严重等级(0.63±0.66)低于对照组和1 mm厚硅胶片保护组,且差异均有统计学意义(t=−5.749、−3.473,均P<0.05)。90Sr-90Y敷贴治疗疗程的增加会使瘢痕疙瘩患者严重放射性皮炎发生的风险增加(OR=2.348,95%CI :1.524~3.618,P<0.001),不同厚度硅胶片的使用可降低严重放射性皮炎的发生风险(1 mm厚硅胶片:OR=0.273,95%CI:0.109~0.685,P<0.01;2 mm厚硅胶片:OR=0.099,95%CI:0.034~0.293,P<0.001)。 结论 90Sr-90Y敷贴治疗瘢痕疙瘩患者时,使用2 mm厚硅胶片保护周围正常皮肤组织,能够显著降低放射性皮炎的发生率和严重程度。 -
关键词:
- 瘢痕疙瘩 /
- 放射性皮炎 /
- 硅胶片 /
- 90Sr-90Y敷贴治疗
Abstract:Objective To investigate the prophylactic effect of silicone on radiodermatitis during the treatment of keloid by using 90Sr-90Y applicator. Methods The clinical data of 175 patients who received 90Sr-90Y applicator for keloids at the Shanghai Sixth People's Hospital Affiliated to Shanghai Jiao Tong University School of Medicine from January 2019 to June 2021 were retrospectively analyzed. The patients included 81 males and 94 females, with ages of (27.2±3.7) years. The patients were divided into the control group (57 cases), the 1 mm-thick silicone protection group (55 cases), and the 2 mm-thick silicone protection group (63 cases) by using the envelope random grouping method. All the patients were treated with multiple small-dose radiation therapy by using a 90Sr-90Y applicator. The skin around the lesion was respectively protected with 1 mm- and 2 mm-thick silicone in the 1 mm-thick and 2 mm-thick silicone protection groups. Radidermatitis for the three groups of patients was graded using the radidermatitis grading criteria of the Radiation Therapy Oncology Group. The incidence and severity of radiodermatitis were compared among the groups. The effects of the treatment course and silicone protection on the occurrence of severe radidermatitis were analyzed. Independent sample t-test (equal variances assumed) was used to compare the two groups for the measurement data in accordance with normal distribution. One-way ANOVA was adopted to compare the three groups. The chi-squared test was conducted to compare the count data in the three groups. Lastly, the factors that affected the efficacy of the treatment were analyzed via univariate Logistic regression analysis. Results No statistically significant difference was found in the incidence of radiodermatitis between the 1 mm-thick silicone protection group and the control group (83.6% vs. 89.5%, χ2=0.815, P=0.367). The incidence of radiodermatitis was significantly lower in the 2 mm-thick silicone protection group than in the control group and the 1 mm-thick silicone protection group (89.5% vs. 83.6% vs. 54.0%), and the differences were statistically significant (χ2=18.108, 11.738; both P<0.05). The severity of overall radiodermatitis was lower in the 1-mm thick silicone protection group than in the control group (1.05±0.65 vs. 1.37±0.75), and the difference was statistically significant (t=−2.409, P<0.05). The severity of radiodermatitis in the 2 mm-thick silicone protection group (0.63±0.66) was lower than that in the control group and the 1 mm-thick silicone protection group, and the differences were statistically significant (t=−5.749, −3.473; both P<0.05). The increase in the number of treatment courses augmented the risk of radiodermatitis (OR=2.348, 95%CI: 1.524–3.618, P<0.001). Meanwhile, the use of silicone with different thicknesses can reduce the risk of radiodermatitis (1 mm-thickness silicone: OR=0.273, 95%CI: 0.109–0.685, P<0.01; 2 mm-thickness silicone: OR=0.099, 95%CI: 0.034–0.293, P<0.001). Conclusion During the treatment of keloid with 90Sr-90Y applicator, the use of 2 mm-thick silicone to protect the surrounding normal skin tissue can significantly reduce the incidence and severity of radiodermatitis. -
Key words:
- Keloid /
- Radiodermatitis /
- Silicone /
- 90Sr-90Y brachytherapy
-
图 1 90Sr-90Y敷贴治疗瘢痕疙瘩患者中硅胶片保护方法示意图
Figure 1. Schematic diagram of 90Sr-90Y applicator for the protection of silicone in the treatment of patients with keloids
图 2 90Sr-90Y敷贴治疗瘢痕疙瘩患者的效果及放射性皮炎的分级图
Figure 2. The effect of 90Sr-90Y applicator in the treatment of patients with keloids and the grading chart of radi dermatitis
表 1 不同厚度硅胶片保护的90Sr-90Y敷贴治疗175例瘢痕疙瘩患者的临床资料、放射性皮炎发生率和严重程度的比较
Table 1. Comparison of clinical data and incidence and severity of radi dermatitis in 175 patients with keloid treated with 90Sr-90Y applicator with different silicone protective thicknesses
项目 对照组
(n=57)1 mm 厚硅胶片保护组
(n=55)2 mm厚硅胶片保护组
(n=63)检验值 P值 年龄(岁, $ \bar x\pm s $ 27.8±3.3 26.8±3.8 27.2±3.9 F=1.047 0.353 性别(男/女) 28/29 24/31 29/34 χ2=0.341 0.843 病程(年, $ \bar x\pm s $ 1.77±0.71 1.83±0.72 1.68±0.62 F=0.767 0.466 疗程数(个, $ \bar x\pm s $ 2.26±0.97 2.35±1.00 2.40±1.06 F=0.263 0.769 治疗有效率[例(%)] 54(94.7) 51(92.7) 60(95.2) χ2=0.474 0.848 放射性皮炎发生率[例(%)] 51(89.5) 46(83.6) 34(54.0)ab χ2=23.328 <0.001 总体放射性皮炎等级( $ \bar x\pm s $ 1.37±0.75 1.05±0.65a 0.63±0.66ab F=17.361 <0.001 相对放射性皮炎等级( $ \bar x\pm s $ 1.53±0.61 1.26±0.49a 1.18±0.39a F=5.613 0.005 注:a表示与对照组比较,差异均有统计学意义(χ2=18.108,t=−2.409、−2.577、−5.749、−3.780;均P<0.05);b表示与1 mm厚硅胶片保护组比较,差异均有统计学意义(χ2=11.738,t=−3.473;均P<0.05)  下载: 导出CSV
下载: 导出CSV
表 2 90Sr-90Y敷贴治疗疗程及硅胶片保护对瘢痕疙瘩患者 发生严重放射性皮炎影响的单因素Logistics回归分析
Table 2. Univariate Logistic regression analysis of the effect of 90Sr-90Y applicator treatment sessions and silicone protection on the occurrence of severe radiodermatitis in patients with keloids
因素 B值 标准误差 Wald值 OR值 95%CI P值 1 mm厚硅胶片 −1.298 0.469 7.663 0.273 0.109~0.685 0.006 2 mm厚硅胶片 −2.309 0.552 17.491 0.099 0.034~0.293 <0.001 疗程 0.854 0.221 14.967 2.348 1.524~3.618 <0.001 常量 −2.296 0.596 14.855 0.101 − <0.001 注:−表示无此项数据。OR为比值比;CI为置信区间
下载: 导出CSV
-
[1] Oliveira GV, Metsavaht LD, Kadunc BV, et al. Treatment of keloids and hypertrophic scars. Position statement of the Brazilian expert group GREMCIQ[J]. J Eur Acad Dermatol Venereol, 2021, 35(11): 2128−2142. DOI: 10.1111/jdv.17484. [2] Kang SU, Kim YS, Kim YE, et al. Opposite effects of non-thermal plasma on cell migration and collagen production in keloid and normal fibroblasts[J/OL]. PLoS One, 2017, 12(11): e0187978[2022-09-16]. https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0187978. DOI: 10.1371/journal.pone.0187978. [3] Liu XY, Chen W, Zeng QY, et al. Single-cell RNA-sequencing reveals lineage-specific regulatory changes of fibroblasts and vascular endothelial cells in keloids[J]. J Invest Dermatol, 2022, 142(1): 124−135.e11. DOI: 10.1016/j.jid.2021.06.010. [4] Meaume S, Le Pillouer-Prost A, Richert B, et al. Management of scars: updated practical guidelines and use of silicones[J]. Eur J Dermatol, 2014, 24(4): 435−443. DOI: 10.1684/ejd.2014.2356. [5] Mustoe TA, Cooter RD, Gold MH, et al. International clinical recommendations on scar management[J]. Plast Reconstr Surg, 2002, 110(2): 560−571. DOI: 10.1097/00006534-200208000-00031. [6] Xu J, Yang EL, Yu NZ, et al. Radiation therapy in keloids treatment: history, strategy, effectiveness, and complication[J]. Chin Med J, 2017, 130(14): 1715−1721. DOI: 10.4103/0366-6999.209896. [7] Bijlard E, Timman R, Verduijn GM, et al. Intralesional cryotherapy versus excision with corticosteroid injections or brachytherapy for keloid treatment: randomised controlled trials[J]. J Plast Reconstr Aesthet Surg, 2018, 71(6): 847−856. DOI: 10.1016/j.bjps.2018.01.033. [8] Mankowski P, Kanevsky J, Tomlinson J, et al. Optimizing radiotherapy for keloids: a meta-analysis systematic review comparing recurrence rates between different radiation modalities[J]. Ann Plast Surg, 2017, 78(4): 403−411. DOI: 10.1097/SAP.0000000000000989. [9] Viani GA, Stefano EJ, Afonso SL, et al. Postoperative strontium-90 brachytherapy in the prevention of keloids: results and prognostic factors[J]. Int J Radiat Oncol Biol Phys, 2009, 73(5): 1510−1516. DOI: 10.1016/j.ijrobp.2008.07.065. [10] Deng K, Xiao HT, Liu XX, et al. Strontium-90 brachytherapy following intralesional triamcinolone and 5-fluorouracil injections for keloid treatment: a randomized controlled trial[J/OL]. PLoS One, 2021, 16(3): e0248799[2022-09-16]. https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0248799. DOI: 10.1371/journal.pone.0248799. [11] Chen GY, Huang LQ, Chen YX, et al. Establishment of incontinence-associated dermatitis rat models and assessment of the therapeutic effects of zinc oxide, painless skin protective film and silicone dressing[J]. Exp Ther Med, 2021, 22(4): 1058. DOI: 10.3892/etm.2021.10492. [12] 中华医学会医学美容与美学分会皮肤美容学组. 放射性皮炎诊疗专家共识[J]. 中华医学美学美容杂志, 2021, 27(5): 353−357.
Dermatologic Aesthetics Group of the Chinese Medical Association's Division of Medical Cosmetology and Aesthetics. Expert consensus on the diagnosis and treatment of radiation dermatitis[J]. Chin J Med Aesth Cosmetol, 2021, 27(5): 353−357.[13] Surakunprapha P, Winaikosol K, Chowchuen B, et al. Adding herbal extracts to silicone gel on post-sternotomy scar: a prospective randomised double-blind study[J]. J Wound Care, 2020, 29(Suppl 4): S36−42. DOI: 10.12968/jowc.2020.29.Sup4.S36. [14] Chow L, Yick KL, Sun Y, et al. A novel bespoke hypertrophic scar treatment: actualizing hybrid pressure and silicone therapies with 3D printing and scanning[J]. Int J Bioprint, 2021, 7(1): 327. DOI: 10.18063/ijb.v7i1.327. [15] Del Toro D, Dedhia R, Tollefson TT. Advances in scar management: prevention and management of hypertrophic scars and keloids[J]. Curr Opin Otolaryngol Head Neck Surg, 2016, 24(4): 322−329. DOI: 10.1097/MOO.0000000000000268. [16] Cox JD, Stetz J, Pajak TF. Toxicity criteria of the Radiation Therapy Oncology Group (RTOG) and the European Organization for Research and Treatment of Cancer (EORTC)[J]. Int J Radiat Oncol Biol Phys, 1995, 31(5): 1341−1346. DOI: 10.1016/0360-3016(95)00060-C. [17] 中国整形美容协会瘢痕医学分会常务委员会专家组. 中国瘢痕疙瘩临床治疗推荐指南[J]. 中国美容整形外科杂志, 2018, 29(5):245−256.
Expert Group of Scar Medicine Branch Standing Committee of Chinese Plastic and Aesthetic Association. Recommended guidelines for clinical treatment of keloid in China[J]. Chin J Aesthetic Plastic Surg, 2018, 29(5): 245−256. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 3525
- HTML全文浏览量: 2988
- PDF下载量: 12
